Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
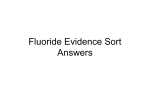
European Journal of Orthodontics 18 (1996) 81-87 O 1996 European Orthodontic Society Enamel fluoride levels after orthodontic band cementation with glass ionomer cement Sevil Akkaya*, Oktay Oner*, Alev Alagam**, and Tuncer Degim*** Departments of 'Orthodontics, and **Pedodontics, Faculty of Dentistry, and ***Department of Pharmaceutical Technology, Faculty of Pharmacy, Gazi University, Ankara, Turkey The aim of this investigation was to examine the fluoride uptake by enamel after application of glass ionomer cement for orthodontic band cementation compared with zinc phosphate cement. The study was conducted on 21 children whose mean age was 14 years. All the children were reared in the Middle Anatolian cities where the water fluoride concentration was below the level of 0.50 ppm. The subjects were randomly divided into three groups. The first experimental group, had seven subjects whose teeth were topically fluoridated with 2 per cent NaF solution, before orthodontic band cementation with zinc phosphate cement. The second experimental group also had seven subjects whose orthodontic bands were cemented with a glass ionomer cement. The third group, consisted of seven control subjects and no dental procedures were performed in this group. All the participants were followed for 3 months and at the end of this period maxillary first premolars, which were in the ninth developmental stage according to Nolla (1960), were extracted for orthodontic purposes. The enamel fluoride concentrations were determined on the left maxillary first premolars at three successive etch depths by means of a fluor ion electrode, whereas the calcium concentrations were determined with an atomic absorption spectrophotometer. The results of this investigation showed that in both cementation groups enamel fluoride concentrations at three successive etch depths were highly increased compared with the control group. However, the difference between the cementation groups was not statistically significant. SUMMARY Introduction Since the inception of fixed orthodontic appliances, discussions about their role on subsequent demineralization, cavitation and caries has continued (Norris et al, 1986; Akkaya and Alacam, 1990; Rezk-Lega et al, 1991). According to Norris et al (1986), in addition to seal breakdown, inadequate structural and bonding strength, the solubility of currently used dental cements in oral fluids, and poor oral hygiene also contribute to the initiation of decalcification. It is clear that oral hygiene and other preventive measures can combat these effects. On the other hand, most recent investigations have concentrated on dental materials. Consequently, the addition of fluorides to zinc phosphate cements, to polycarboxylate cements and to the bonding systems for resulting anticariogenic and antibacterial benefits of fluoride release became popular (Wei and Sierk, 1971; Retief et al, 1984; Tanaka et al, 1987; Temin et al, 1989; Horsted-Bindslev and Larsen, 1990). Fluoride has anticariogenic properties resulting from the formation of less soluble fluoroapatite in the outer enamel layer (Norris et al, 1986). Zinc phosphate cements which have become the standard cement used for cementation of orthodontic bands over the years, have some disadvantages, being brittle, having a relatively high solubility in the mouth and weak adherence to tooth substance. Other dental cements have been developed by researchers to overcome these drawbacks. Polycarboxylate cements reacting chemically with dental enamel and stainless steel were presented as suitable cements for orthodontic treatment. However, short setting time and high viscosity became the main problems affecting 82 the popularity of these cements (Rich et al, 1975; Norris et al, 1986). Glass ionomer cements, which were introduced in 1971, are based on the hardening reaction between an aqueous solution of monomers or copolymers of acrylic acid and powdered calcium aluminosilicate glass (Hotz et al., 1977). Via calcium bridges, hydrogen bonds or other Van der Waal forces and phosphate substitution by which glass ionomers are bound to enamel, glass ionomer cements provide a stronger bond strength (Kopel and Batterman, 1976; Norris et al, 1986; Rezk-Lega et al. 1991). In an in vitro study Retief et al. (1984) showed fluoride uptake of enamel and cementum from a glass ionomer cement. Also, Horsted-Bindslev and Larsen (1990) concluded that the release of fluoride was reduced by time in their investigation, although the fluoride concentrations remained higher than necessary and were maintained for a long time. This investigation aimed to examine the in vivofluorideuptake by enamel at three different depths, before and after band cementation, using a fluoride releasing cement and a zinc phosphate cement, the latter of which was used after the application of topical fluoride, in order to establish the biocompatibility of fluoride for orthodontic cementation. Subjects Clinical phase The study was conducted on 21 male children whose mean age was 14 years. Their maxillary first premolar teeth were in the ninth developmental stage according to Nolla (1960). All the children were reared in Middle Anatolian cities, where the water fluoride concentration was below 0.50 ppm. The children in need of orthodontic treatment and whose healthy maxillary first premolars were to be extracted for orthodontic purposes were randomly divided into three groups. The first experimental group had seven subjects whose teeth were topically fluoridated with 2 per cent sodium fluoride (NaF) solution four times at weekly periods, before orthodontic band cementation with zinc phosphate cement (Adhesor®, Spofa Dental, Czechoslovakia). The second experimental group also had seven subjects whose ortho- S. AKKAYA ET AL. dontic bands were cemented with a glass ionomer cement (Voco Meron®, Voco, Cuxhaven, Germany). The third group consisted of seven control subjects and no dental procedures were performed. The experimental teeth were extracted after 3 months. Following careful removal of the orthodontic bands and cements, the teeth were cleaned of debris with pumice and then rinsed with deionized water. They were then stored in polyethylene tubes containing distilled water at 4°C until the analysis. Laboratory phase Enamel samples of left maxillary first premolar teeth were obtained from the demarcated biopsy sites by means of a modified acid etch microbiopsy procedure (McLean and Wilson, 1977; Vogel et al, 1983; Soyman et al, 1984; Chow etal, 1985; Retief et al, 1985). A 3-mm length of adhesive tape was placed on the vestibular surface of the teeth where the orthodontic bands had previously been applied. The remaining surfaces were covered with Eudgarit s90 (Rohm Pharma GMBH, Darmstadt, Germany) diluted in acetone. The adhesive tape was removed and the teeth were immersed and rinsed in the tubes containing 1 ml 0.5 M perchloric acid. After 60 seconds 4-ml aliquots of 0.5 M Total Ionic Strength Adjustment Buffer (TISAB; Orion Research Inc., Cambridge, MA, USA) was added to perchloric acid and in this way 5 ml of biopsy aliquot was prepared (first layer). This biopsy technique was repeated separately three times for each tooth (second and third layers). Consequently, 25 ml TISAB solution was added to each of the individual etch solutions and fluoride was measured with a fluoride ion electrode (Bilmar model 101 ph mV tempmeter, Russel model 96-6099 combined ion selective electrode). Calcium concentration was measured with an atomic absorption spectrophotometer (Model 603, Perkin-Elmer, Norwalk, CT, USA). The weight and the volume of enamel removed by each acid etch and the corresponding fluoride concentration were calculated by use of the values of 2.95 for human enamel density and 37 per cent for calcium content (Wei and Sierk, 1971; Tanaka et al, 1987; Temin et al, 1989). From the data obtained, the depth of each biopsy was calculated by means of the following equations (Aasenden 83 FLUORIDE UPTAKE FROM GLASS IONOMER CEMENT and Moreno, 1971; Benediktsson et al, 1982; Soyman et al., 1984): mass of enamel=/*g Ca + + x (1 + 1000) x (1 - 1000) x (100 -=- 37)g enamel Depth of etch (cm) = mass of enamel (g) density of enamel x biopsy area (cm2) The result of the equation must be multiplied by 10000 in order to express the depth of etch in fan. Usually, concentrations of trace elements are expressed in parts per million (ppm), so the following formula was used to state the ppm fluoride in the biopsy samples: Fluoride in the aliquot (fig) Fluoride (ppm) = Enamel in the aliquot (g) Because the biopsy depth is an uncontrollable variable, regression analysis was carried out by using the enamel's three different depth levels and the linear ppm fluoride in these depths. Via the regression equation, ppm fluoride concentrations were adjusted to standardized depths of 20, 40, and 60 /an. The evaluation of the biopsy data of the groups for these three successive depths were statistically analysed by Student's f-test and the mean ppm fluoride concentrations of the groups in relation to adjusted enamel depths were compared by paired Mests. Table 1 Fluoride uptake values (ppm) in standardized enamel depths of 20, 40, and 60 /on in control group. Tooth no. 20 /an 40 /an 60 /an 1 2 3 4 5 6 7 12888 7614 9116 6959 26386 4531 13866 12421 7633 8828 6337 19831 3031 13571 11971 7653 8549 5769 14905 2028 13283 Table 2 Fluoride uptake values (ppm) in standardized enamel depths of 20, 40, and 60 /an in glass ionomer cementation group. Tooth no. 20 /an 40 /an 60/an 1 2 3 4 5 6 7 55183 19587 47871 46454 18143 64917 19405 41019 18026 39797 41725 16587 62861 17944 30491 16589 33084 37478 15164 60870 16593 Table 3 Fluoride uptake values (ppm) in standardized enamel depths of 20, 40, and 60 /an in zinc phosphate cementation group after topical fluoridation. Results Tooth no. 20 /an 40/an 60/an Mass of enamel (ng), depth of etch (/mi), /mi fluoride in these depths, the disassociation of ppm fluoride and calcium (fig) according to samples after three biopsy applications in the control group, in the group of glass ionomer cementation, and in the topical fluoride applicated group before zinc phosphate cementation were calculated. Fluoride uptake values in standardized enamel depth of 20, 40, and 60 /xm are given in Tables 1, 2, and 3. Mean ppm fluoride values at standardized depths of enamel and the results of statistical significance of the differences in the groups are shown in Table 4 and Fig. 1. Mean ppm fluoride at 20 /an depth was found to be 33 940 in the glass ionomer cementation group, and 23115 in the topically fluoridated group. These fluoride concentrations were found to be statistically significantly different from the control group (P<0.05). However, the mean fluoride values in the glass ionomer cementation group were 1 2 3 4 5 6 7 19019 27258 48482 14667 21331 12404 18644 18099 26197 43953 13162 20170 11753 16562 17224 25177 38848 14812 19072 11136 14712 not statistically significantly different from the topically fluoridated group, although the results were higher. The results of mean ppm fluoride values at the etch depths of 40 and 60 fan were parallel to the results of the first etch depth. It was observed that the mean fluoride concentrations of the application groups were relatively higher than in the control group, whereas the difference between the application groups was not statistically significant. Furthermore, it was noted that the ppm fluoride values decreased according to the increase in depths in all the groups. 84 S. AKKAYA ET AL. Table 4 Mean ppm F values at standardized depths of enamel and the results of statistical importance between the groups of glass ionomer cementation, topical fluoridation before zinc phosphate cementation and control. Glass ionomer cementation Topical F+ZnPO 4 cement Control S.I 20 fan 33940 SD: 22614 23115 SD: 12156 11623 SD: 7291 1-2:* 1-3:" 2-3:" 40/jm 33994 SD: 17280 21414 SD: 11018 10236 SD: 5535 1-2:* 1-3" 2-3" 60 fan 30038 SD: 16321 20283 SD: 9679 9165 SD: 4526 1-2:* 1-3** 2-3** Depth *: not significant. **: significant at/><0.05 level. Discussion The presence of white spot lesions under orthodontic bands represents a serious problem of clinical importance. Recent studies have shown that glass ionomers may inhibit this type of 40 Control lesion development and this outcome is generally attributed to the fluoride released from the cement (Kvam et al, 1983; Valk and Davidson, 1987; Rezk-Lega et al, 1991). The inhibition of enamel demineralization and also the increase in the initial rate of remineralization are generally acknowledged to be the major beneficial effects of fluoride (RezkLega et al, 1991). Kvam et al (1983) showed less enamel demineralization under orthodontic bands attached with a glass ionomer cement than under bands attached with a conventional phosphate cement. The failure rate for bands cemented with glass ionomers was also significantly lower than the rate recorded for bands cemented with a polycarboxylate cement (Mizrahi and Smith, 1969). Because of these characteristics, in one of the experimental groups, orthodontic band cementation was undertaken with a glass ionomer cement. It is suggested that a slight increase in fluoride may be capable of rendering a tooth more resistant to dental caries if the concentration of fluoride in the outer most layer of enamel is the critical factor (Heifetz et al, 1970). Brunn et al (1983) demonstrated that the production of Glass ionomer cementation | Topical fluoridation before zinc phosphate cementation 35 30 25 LL 20 15 10 40 Enamel depth dim) 60 Figure 1 The values of ppm F in 20, 40, and 60 itsa standardized enamel depths of experimental groups. FLUORIDE UPTAKE FROM GLASS IONOMER CEMENT soluble or insoluble products reduced caries attack; thus, the need for removal of the alkali soluble products, which include calcium fluoride (potassium hydroxide) according to the method described by Caslavska et al. (1975) should be re-evaluated. McLean and Wilson (1977) concluded that while the cement becomes attached via ionic and polar bonds to the enamel, the intimate molecular contact facilitates fluoride ion exchanges with the hydroxyl ions, whereas a luting agent that does not adhere by molecular interactions would leave gaps between the cement and the tooth. Therefore, even if such a luting agent were to release fluoride, ion exchange would be inhibited. On the other hand, in their in vivo investigation of two glass ionomer cements, Rezk-Lega et al. (1991) have concluded that although the cements had cariostatic properties, fluoride protection against lesion development beneath orthodontic bands could be weak, because the fluoride released from the cement did not cover the enamel crystallites completely. They pointed out that another possible reason for poor response was the magnitude of the cariogenic challenge beneath the bands being so intense, as it is known that below a pH of 4.5 fluoride would have a limited effect. Because of this, topical fluoride application before cementation with a zinc phosphate cement was preferred as an alternative in this investigation. The reaction of topical fluoridation is known to be in two phases. Calcium fluoride which is a soluble first reaction product can change into tightly bound fluoride after repeated applications (Cebe, 1973; Clarkson, 1991). In many investigations it has been observed that the fluoride concentration on the surface enamel showed individual differences according to the area of its application and enamel fluoride acquired from topical fluoride treatment is inversely related to the enamel fluoride content prior to its application (Heifetz et al, 1970; RytSmaa et al, 1974; Benediktsson et al., 1982). So, in comparative studies in which fluoride acquired from topical fluoride agents were evaluated, it would be preferable if teeth with similar fluoride concentrations were used. This investigation was conducted on children reared in Middle Anatolian cities where the water fluoride concentrations were below 0.50 ppm (Erkan et al, 1991). On the other 85 hand, analysis of fluoride in the micro-samples of the enamel spectrophotometrically or by means of fluoride ion electrode, gas chromatography and sensitive physical methods have shown that there were three biologically important variables affecting the values; the origin of the tooth, the particular tooth surface measured and the position of the point analysed on a single surface (Rytomaa et al, 1974). The standardization of the donors' ages in addition to the developmental stage of the teeth was necessary as the fluoride acquisition of young teeth was different from older ones and enamel fluoride acquired was based upon maturation (Nolla, 1960). Since the enamel fluoride concentration of boys was 10 per cent higher than girls, and the fluoride concentrations of different teeth were found to vary, the determination of tooth type and sex of donor were also required (Jenkins, 1978). In this study all the biological variables discussed were standardized as far as possible by conducting the clinical phase on male children whose mean age was 14 and the developmental stage of their maxillary first premolars was the same. Also the enamel samples of experimental teeth were obtained from demarcated biopsy sites on the vestibular surfaces by means of the window technique. Although initial and final enamel fluoride concentrations at specific points of homologous teeth or at similar surfaces of dissected teeth could be determined in vitro (Guo et al, 1989; Fischer-Brandies et al, 1991; Us, 1991), the results are questionable when these conditions are provided in vivo (Eliades et al, 1992; Seppa et al, 1992). •On the other hand, it is concluded that caries activity of the donor increases according to the count of Lactobaccillus in the saliva due to hygienic difficulties derived from orthodontic treatment (Zachrisson and Brobakken, 1978; Mizrahi, 1982; O'Reilly and Featherstone, 1987). Because of this, bilateral teeth were not used as controls in this study. Consequently, the results of this investigation should not be compared with the results of similar in vitro investigations. The fluoride acquired by the enamel and cementum from a glass ionomer cement in the in vitro studies may largely be due to the topical effect of the released fluoride in the synthetic saliva. In the clinical situation a tooth is constantly bathed in saliva which is replenished by 86 the salivary flow. So, in vivo experimentally observed enamel fluoride concentrations will be less than the in vitro studies (Retief et al, 1984; Horsted-Bindslev and Larsen, 1990). It is considered that 1000 ppm enamel fluoride concentration through 30 /an depth seems sufficient for a considerable preventive effect (Cebe, 1973). This depth may be minimally more or less. Fluoride concentration at superficial enamel level, in addition to 60 /an depth, was observed to be greater than necessary for a preventive effect in this study. The findings of reduced fluoride level with an increase in depth were in agreement with previous studies, although statistically insignificant. The results of this investigation showed that fluoride concentration at three etch depths was higher in the glass ionomer cementation group than in the topical application group, although there was no statistically significant difference. On the other hand, it must be pointed out that the increase in the number of the experimental teeth might have affected the statistical significance. Both in vivo and in vitro studies have supported the finding that the release, of fluoride was reduced by time for all; glass ionomer cements (Olsen et al, 1989; (Hx>rsted-Bindslev and Larsen, 1990; Koch' and HatibovicKofman, 1990; Hatibovic-Kofman and Koch, 1991). Therefore, it may be postulated that the higher the release of fluoride, the higher the caries inhibitory effect. The results of the present study also confirm this hypothesis. However, considering 1-3 ppm fluoride in solution was sufficient for a preventive effect, the fluoride concentrations were found to be adequate even after 3 months in an investigation by Horsted-Bindslev and Larsen (1990). On the other hand Norris et al. (1986) concluded that the glass ionomer cements were most effective in adhering to the tooth surface in their experimental study, where the retention of orthodontic bands with zinc phosphate, polycarboxylate, and glass ionomer cements were evaluated. The investigators suggested that even under loose bands, the glass ionomer cement adhered to the enamel and, therefore, may offer clinical protection against decalcification. Supporting this idea, Koch and HatibovicKofman (1990) also showed that the prevalence of S. mutans in saliva decreased after placement of a glass ionomer cement restoration. S. AKKAYA ET AL. So, evaluating all these findings it is concluded that, glass ionomer cement is an alternative to topical fluoride application before cementation with zinc phosphate cement. It has a popular clinical application because of high adhesion capacity to the tooth enamel and also provides an increment in enamel fluoride content. Address for correspondence Associate Professor Dr Sevil Akkaya Gazi University Faculty of Dentistry Department of Orthodontics 06510 Emek Ankara, Turkey References Aasenden R, Moreno E C 1971 Evaluation of biopsy data in human enamel fluoride studies. Archives of Oral Biology 16: 1413-1426 Akkaya S, Alacam A 1990 Cavitation after orthodontic bonding: a case report. Turkish Journal of Orthodontics 3: 123-128 Benediktsson S, Retief D H, Bradley E L, Switzer P 1982 The effect of contact time of acidulated phosphate fluoride on fluoride concentration in human enamel. Archives of Oral Biology 27: 567-572 Brunn C, Thylstrup A, Uribe E 1983 Loosely bound fluoride extracted from natural carious lesions after topical application of APF in vitro. Caries Research 17: 458-460 Caslavska V, Moreno E C, Brudevold F 1975 Determination of the calcium fluoride formed from in vitro exposure of human enamel to fluoride solutions. Archives of Oral Biology 20: 333-339 Cebe K G 1973 Fluor-Lack method for the prophylaxis of child teeth. Thesis, University of Istanbul, Turkey Chow L C, Beaudreau G M, Brown W E 1985 Enamel fluoride profile construction from biopsy data. Caries Research 19: 103-112 Clarkson B H 1991 Caries prevention-fluoride. Advanced Dental Research 5: 41-45 Eliades T, Viazis A D, Eliades G 1992 Enamel fluoride uptake from an experimental fluoride-releasing orthodontic adhesive. American Journal of Orthodontics and Dentofacial Orthopedics 101: 420-424 Erkan Z, Akbulut E, Harputluoglu S, Cokpekin F 1991 Investigation of relationship between fluor concentration of drinking water and DMFT index for 5620 individual in 12-18 year age group. Journal of the Dental Faculty of Ankara University 18: 339-344 Fischer-Brandies H, Kluge G, Theusner J, Hausler K 1991 Fluorine distribution in the enamel in the use of glass ionomer cements as bonding materials. Deutsche zahnarztliche Mund und Kieferheilkunde mit Zentralblatt 79: 349-355 FLUORIDE UPTAKE FROM GLASS IONOMER CEMENT Guo M K, Chow L C, Schreiber C T, Brown W E 1989 Comparison of fluoride uptake produced by tray and flossing methods in vitro. Journal of Dental Research 68: 496-498 Hatibovic-Kofman S, Koch G 1991 Fluoride release from glass ionomer cement in vivo and in vitro. Swedish Dental Journal 15: 253-258 Heifetz S B, Mellberg J R, Winter S J, Doyle J 1970 In vivo fluoride uptake by enamel of teeth of human adults from various topical fluoride procedures. Archives of Oral Biology 15: 1171-1181 H6rsted-Bindslev P, Larsen M J 1990 Release of fluoride from conventional and metal reinforced glass ionomer cements. Scandinavian Journal of Dental Research 98: 451-455 Hotz P, McLean J W, Seed I, Wilson A D 1977 The bonding of glass ionomer cements to metal and tooth substrates. British Dental Journal 142: 41-47 Koch G, Hatibovic-Kofman S 1990 Glass ionomer cements asfluoriderelease system in vivo. Swedish Dental Journal 14: 267-273 Kopel M H, Batterman C S 1976 The retentive ability of various cementing agents for polycarbonate crowns. Journal of Dentistry for Children 43: 37-43 Kvam E, Brosch J, Nissen-Meyer I H 1983 Comparison between a zinc phosphate cement and a glass ionomer cement for cementation of orthodontic bands. European Journal of Orthodontics 5: 307-313 Jenkins G N 1978 The physiology and biochemistry of the mouth. 4th edition Blackwell Scientific Publications, Oxford, pp. 473-481 McLean J W, Wilson A D 1977 The clinical development of glass ionomer cements-formulations and properties. Australian Dental Journal 22: 31-36 Mizrahi E 1982 Enamel demineralization following orthodontic treatment. American Journal of Orthodontics 82: 62-67 Mizrahi E, Smith D C 1969 The bond strength of a zinc polycarboxylate cement. British Dental Journal 4: 410-414 Nolla C M 1960 The development of the permanent teeth. Journal of Dentistry for Children 27: 254-266 Norris S D, Mclnnes-Leduox P, Schwaninger B, Weinberg R 1986 Retention of orthodontic bands with a new fluoride releasing cements. American Journal of Orthodontics 89: 206-211 Olsen B T, Garcia-Godoy F, Marshall T D, Barnwell G M 1989 Fluoride release from glass ionomer-lined amalgam restorations. American Journal of Dentistry 2: 89-91 O'Reilly M M, Featherstone J D B 1987 Demineralization and remineralization around orthodontic appliances: an 87 in vivo study. American Journal of Orthodontics and Dentofacial Orthopedics 92: 33-40 Retief D H, Bradley E L, Denton J C, Switzer D 1984 Enamel and cementum fluoride uptake from a glass ionomer cement. Caries Research 18: 250-257 Retief D H, Summerlin D J, Harris B E, Bradley E L 1985 An evaluation of three procedures for fluoride analysis. Caries Research 19: 248-254 Rezk-Lega F, 0gaard B, Arends J 1991 An in vivo study on the merits of two glass ionomers for the cementation of orthodontic bands. American Journal of Orthodontics and Dentofacial Orthopedics 99: 162-167 Rich J M, Leinfelder K F, Hershey H G 1975 An in vitro study of cement retention as related to orthodontics. Angle Orthodontist 45: 219-225 Rytdmaa I, Keinonen J, Anttila A 1974 Sensitive physical method for determination of fluorine distribution in human surface enamel. Archives of Oral Biology 19: 553-556 Seppa L, Salmenkivi S, Forss H 1992 Enamel and plaque fluoride following glass ionomer application in vivo. Caries Research 26: 340-344 Soyman M, §irin §, Akinci T 1984 Determination of enamel fluoride concentration by mathematical calculations of demineralized tooth enamel. Journal of Marmara University Dental Faculty 1: 17-27 Tanaka M, Ono H, Kadoma Y, Imai Y 1987 Incorporation into human enamel of fluoride slowly released from a sealant in vivo. Journal of Dental Research 66: 1591-1593 Temin S C, Csuros Z, Mellberg J R 1989 Fluoride uptake from a composite restorative by enamel. Dental Materials 5:64-65 Us Z 1991 In vitro investigation of fluoride uptake of primary teeth enamel after the application of APF (acidulated phosphatefluoride)with dentalflossto approximal surfaces. Thesis, Gazi University, Ankara, Turkey Valk J W P, Davidson C L 1987 The relevance of controlled fluoride release with bonded orthodontic appliances. Journal of Dentistry 15: 257-260 Vogel G L, Chow L C, Brown W E 1983 A microanalytical procedure for the determination of calcium, phosphate and fluoride in enamel biopsy samples. Caries Research 17: 23-31 Wei S H Y , Sierk D L 1971 Fluoride uptake by enamel from zinc phosphate cement containing stannous fluoride. Journal of the American Dental Association 83: 621-624 Zachrisson B U, Brobakken BO 1978 Clinical comparison of direct versus indirect bonding with different bracket types and adhesives. American Journal of Orthodontics 74: 62-78