Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
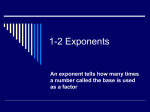
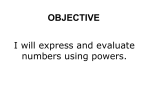
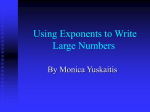
Gzrdiovascular Research ELSEVIER Cardiovascular Research 31 (19%) 410-418 Chaos-related deterministic regulation of heart rate variability in timeand frequency domains: effects of autonomic blockade and exercise Inger Hagerman a** , Margareta Berglund a, Mikael Lorin b, Jacek Nowak ‘, Christer Sylvh a a Departmenr of Cardiology, Karolinska Institute, Huddinge Universily Hospital, S-141 86 Huddinge, Sweden b Department of Technical Assistance, Karolinska Institure, Huddinge Hospital, S-141 86 Huddinge, Sweden ’ Department of Clinical Physiology, Karolinska Institute, Huddinge University Hospital. S-141 86 Huddinge, Sweden Received 27 October 1994; accepted 19 June 1995 Abstract Objectives: To study non-linear complexity or chaotic behaviour of heart rate in short time series and its dependence on autonomic tone. Methods: Ten healthy individuals (5 men, mean age 44 years) were investigated at rest, after intravenous injections of propranolol (0.15 mg/kg), followed by atropine (0.03 mg/kg). On another occasion, investigation was made during exercise on a bicycle ergometer at 40% and at 70% of maximal working capacity. Heart rate variability was assessed by: local sensitive dependence on initial conditions as quantitated by the dominant Lyapunov exponent, coefficient of variation of heart rate, power spectral analysis of high- and low-frequency bands and the l/f-slope of the very-low-frequency band and time domain analysis. Results: The approximate dominant Lyapunov exponent was positive at rest and remained positive during autonomic blockade and during exercise. The exponent decreased significantly with propranolol + atropine and even more soduringexercisebut did not attainzero. At baselineapproximatepredictability was lost after about 30 s whereasafter autonomicblockadeor exerciseit was lost after about60 s. The l/f-slope remainedunaltered around - 1. As expected, power in high- and low-frequency bands as well as time domain index decreased significantly with autonomic blockade. The low-frequency band and time domain index were affected by exercise. Conclusions: Heart rate variability of sinus rhythm in healthy individuals has characteristics suggestive of low-dimensional chaos-like determinism which is modulated but not eliminated by inhibition of autonomic tone or by exercise. The dominant Lyapunov exponent characterises heart rate variability independent or the other investigated measures. Keywords: Heart rate variability; Exercise; Chaos; Non-linear phenomena; Autonomic nervous system 1. Introduction Application of chaos theory to complex biological processesanalysis is based on concepts and models derived from non-linear dynamics. One area of interest in cardiology is to identify and classify electrical instability which may precede arrhythmias [l]. Heart rate response to a change in parasympathetic efferent activity is extremely rapid, occurring usually on a beat-to-beat basis [2]. The change in heart rate in response to changes in efferent sympathetic activity is a slower process [3]. These and other oscillators result in a heart rate variability signal that * Corresponding 7464120. author. Tel.: (+ 46-8) tXO3-6363/%/$15.00 0 1996 Elsevier SSDI 0008-6363(95)00084-4 7464126; fax: is made up of componentswith differing time scalesand corresponding differing frequency components 143. In a mathematical model of vagally driven sinoatrial node, Michaels et al. [S] found that irregular dynamics obeying the rules derived from other chaotic systemswere present during vagal stimulation of the sinus node. Application of the same analytical tools to the analysis of simulation of reflex vagal control of sinus rate suggestedthat chaotic dynamics could be obtained in the physiologically relevant case of the baroreceptor loop. As outlined by Denton [6], the sinusrhythm is constituted by the sinoatrial (SA) node controlled by multiple non-linear mechanisms such as parasympathetictone, sympathetic tone, hormones,preload, (+46-8) Tie Science B.V. All tights reserved for primary review 40 days. I. Hagerman et al./ Cardiovascular afterload, most of which have a long feedback-loop compared with the basic cycle length - “a near perfect substrate for the generation of chaos”. Fast Fourier transformation of heart rate reveals not only high- and lowfrequency peaks. The major spectral density is located in the very-low-frequency band without any distinct peaks. This density may be due to a complexity of oscillators with overlapping time scales. Depressed heart rate variability analysed in time and frequency domains has been shown to predict sudden death in patients with previous myocardial infarction [8]. Techniques derived from non-linear dynamics and chaos theory may be of complementary value in identifying patterns and mechanisms that are not detectable with traditional statistics based on linear models. Deterministic chaos exhibits a number of characteristics that distinguish it from periodic and random behaviour, in particular by sensitive dependence on initial conditions, which means that small changes in the state variables at one point will create large differences in the behaviour of the system at some future point. This manifests itself graphically as adjacent trajectories that diverge widely from their initial close positions. The Lyapunov exponent is a quantitative measure of the average rate of this separation. A positive Lyapunov exponent indicates sensitive dependence on initial conditions and thus loss of predictability, indicative of deterministic chaos [9]. The aim of this study was to find in healthy volunteers a design applicable to clinical conditions to test heart rate on the one hand for non-linear complexity or chaotic behaviour and on the other hand for its dependence on autonomic tone. Clearly, this requires an approximation of an ideal condition since during clinical conditions the time Research 411 31 11996) 410-418 of recording is limited due to both logistics and the status of the patients. 2. Methods Ten healthy individuals, 5 men and 5 women were, after informed consent, enrolled for investigation. Median age was 44 years (33-51), they were all healthy without a history of cardiovascular disease, normotensive, in sinus rhythm and without any medication. Measurements during rest and with autonomic blockade were made between 9.00 and 11.OO in the morning and measurements during exercise were made between 1.00 and 3.00 in the afternoon. 2.1. Autonomic blockade After a rest in the supine position for 10 min, recording was done of 750 consecutive beats. Recordings were repeated 5 minutes after i.v. administration of propranolol 0.15 mg/kg over 120 s and again after atropine 0.03 mg/kg over 30 s. Thus, the last measurement was performed under dual autonomic inhibition [ 10,111. 2.2. Exercise stress test Exercise test was performed on two separate occasions. Using an ergometer bicycle with an automatic device for continues load increase of 10 W/min (Siemens-Elema, Sweden), the subjects were encouraged to continue work until stopped by fatigue or dyspnoea, in order to determine maximal working capacity. On a second occasion, more than 24 h later, sampling was made at submaximal work Table 1 Effects of varying constants on approximate dominant Lyapunov exponents (bits of information * s- ’ ) of heart rate at baseline and following propranolol and atropine No. Grid Min. Max. Evol. Approximate dominant Lyapunov exponents ANOVA Rest Propranolol P * Rromanolol+ atrooine P * 1 2 3 4 5 6 7 8 9 10 11 12 3 3 3 3 6 6 6 6 10 10 10 10 1 1 3 3 1 1 3 3 1 1 3 3 2 2 2 2 2 2 2 2 2 2 2 2 10 15 10 15 10 15 10 15 10 15 10 15 0.68 f 0.03 0.47 f 0.04 0.56 f 0.02 0.41 f 0.02 0.69 f 0.03 0.46*0.04 0.54 f 0.02 0.40 f 0.02 0.67 f 0.03 0.46 f 0.03 0.53 f 0.02 0.38 f 0.03 0.76 f 0.03 0.52 f 0.03 0.56 f 0.02 0.40*0.02 0.75 f 0.03 0.5 1 f 0.03 0.55 f 0.02 0.40 f 0.03 0.75 f 0.03 0.50 f 0.03 0.54 f 0.02 0.41 *0.02 NS NS NS NS NS NS NS NS NS NS NS NS 0.39 0.24 0.33 0.23 0.39 0.26 0.33 0.23 0.40 0.25 0.33 0.22 f rt f f + f f f f f * * 0.07 0.05 0.05 0.04 0.07 0.05 0.05 0.04 0.07 0.05 0.05 0.04 < < < < < < < < < < < < 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 <: 0.01 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 Nos. 1-12, varying constant combinations. Grid = grid resolution; Evol. = evolution time; Min. = minimum separation of replacement (%); Max. = maximum separation of replacement (a). Compared to rest. P-values from analysis of variance for the 12 combinations are also given. l 412 I. Hagerman et al./ Cardiovuscular Research 31 (1996) 410-418 loads of 40% and at 70% of maximum working capacity. Prior to sampling of time series of 750 consecutive heart beats, the subjects worked 6 min on each level in order to attain steady-state conditions during sampling of the succeeding 750 consecutive heart beats [12,13]. 2.3. Lyapunov exponent measurement of heart rate variability The Lyapunov exponent for time series was calculated according to Wolf [14,15] for 750 consecutive heart beats at a sampling frequency of 20 kHz. Interbeat intervals differing more than 30% from the mean interval of 5 preceding beats were manually edited and excluded from the calculation. Excluded signals were mainly artefacts due to missense of the T-wave. The computer program estimates the dominant Lyapunov exponent in a given time series by averaging the exponential rate of divergence of short segments of the delay reconstructed orbit (trajectory). To minimise a systematic artefact, every time series was evaluated with 12 different combinations of equation constants for grid resolution, evolution time, minimum and maximum separation of time points. Time delay, embedding dimension, time step and orientation error were held constant at 1, 3, 1 and 30, respectively (Table 1). Time delay is the delay with which the return map is constructed and time step the step taken between succeeding return maps. The Lyapunov exponent is positive for chaotic behaviour, zero or negative for periodic behaviour and around zero when noise prevails. 2.4. Frequency domain measurements of heart rate variability Frequency domain analysis was performed on 750 consecutive beats using a Holter ECG device (Daltec Biomedical). If extrasystoles appear, the preceding and succeeding intervals are substituted through linear interpolation with the following normal R-R. Two or more extrasystoles generate a new calculation period. From the time series of equidistant R-R values the power spectrum is calculated through Fast Fourier transformation [16] within 2 frequency bands: high-frequency power (HF) 0.40-0.15 Hz 0 250 500 750 Heart Beat Fig. 2. Example of approximate dominant Lyapunov exponent calculation (bits of information * s- ‘1 derived from 750 heart beats. and low-frequency power (LF) 0.15-0.04 Hz. As HF is suggested as an index of cardiac parasympathetic activity while LF reflects sympathetic activity with vagal modulation [4,17], these parameters were chosen to describe the influence of autonomic blockade on heart rate variability. Spectral data are expressed as a percentage of total power and as the LF/HF ratio, which has been shown to be a marker of changes in the sympatho-vagal balance [17]. 2.5. I /f measurements of heart rate variability For all time series a regression line relating the log of spectral amplitude to the log of frequency was constructed. This regression line is called a l/f X plot because of the inverse relation between amplitude (or power) and frequency that character& spectra for heart rate variability and other fractal processes [9,27]. The slope of the regression line equals the exponent x in the l/f” plot. This exponent can be used to characterise the overall distribution of frequencies and their amplitudes and has been suggested to indicate the complexity of a process [ 18-201. 2.6. Time domain measurement of heart rate variability Time domain analysis was performed on 750 consecutive beats using a Holter ECG device (Daltec Biomedical). The heart rate variability is displayed as an interval histogram, with the interval on the horizontal axis and the number of beats in each time increment on the vertical axis. A triangular index is calculated as described by Cripps and colleagues [21]. An index < 25 ms has been associated with increased risk for sudden cardiac death in patients with previous myocardial infarction [22]. 2.7. Statistics and ethics Fig. 1. ‘Three-dimensional representation of 750 R-R intervals (ms) from one subject at baseline. The x-axis shows the R-R interval X, tbe y-axis and z-axis the R-R intervals x - 1 and x - 2, respectively. The study was approved by the local Ethics Committee. All data are presented as mean f s.e.m. The data were subjected to one-way analysis of variance (ANOVA) for I. Hagerman ef ul./Cardiovascular Research 31 (1996) 413 410-418 Table 2 Effects of propranolol and atropine on heart rate variability Propranolol Rest P’ Rropranolol + atropine P’ ANOVA < 0.01 NS 86 +4 2.4 to.7 < 0.001 < 0.001 < 0.01 NS NS < 0.05 0.30*0.05 0.94 + 0.04 2.0 rt0.6 3 rto.7 2.0 *0.07 70 +7 < 0.01 NS < 0.001 HR (beats/min) HR (var.%) Approximate Lyapunov l/f I-F (o/o) LF (%) LF/HF Tl h-d 60 +3 2.4 f 1.8 71 +3 1.8 f 0.2 0.52f 0.03 -0.99f 0.04 7.0 rt 1.0 23 2 4.0 3.06* 0.06 200 *19 OSf -0.73f 4.0 12 3.0 218 0.03 0.19 f 1.0 + 2.0 * 0.06 f26 < 0.001 NS NS < 0.01 < 0.001 < 0.01 < 0.001 < 0.001 NS < 0.001 < 0.0001 < 0.01 < 0.001 * Compared to rest. HR = heart rate; Lyapunov exponent (bits of information * s-l), mean from 12 combinations of constants for 10 subjects; l/f= distribution; HF = high frequency; LF = low frequency; TI = time domain index. Values are given as mean f s.e.m. P-value or non-significance (NS) for ANOVA is given. repeated measurements with identification of group differences by Fisher’s protected least significance test. Differences from zero was tested according to the normality distribution. Statistical significance was accepted at P-values below 0.05. similar discriminative capacity for changes in Lyapunov exponents during autonomic blockade (Table 1). Small variations in the magnitude of information due to the selection of constants as made in this study were therefore considered to be of minor importance. Consequently, all 12 constat combinations were used when computing mean approximate Lyapunov exponents. Further, for each constant combination, the mean Lyapunov exponent was divided by the standard deviation. All ratios were statistically different from zero with mean values of 5.7 f 0.7, 9.6 + 2.8 and 3.9 f 0.7 for rest, propranolol and atropine. 3. Results 3.1. Lyapunov exponent - role of constant selections Fig. 1 shows a representative 3-dimensional representation of the cigar-shaped attractor generated by 750 beats of one subject at baseline. The quantity of 750 beats was found to generate a steady-state level of the dominant Lyapunov exponent (Fig. 2). This was further evaluated by calculating the Lyapunov exponent at baseline after 500, 625 and 750 beats, n = 10. ANOVA did not show any non-homogeneity, thus further suggesting that a steady state was obtained. ‘All 12 combinations of constants had 3.2. Autonomic blockade (Table 2) Following propranolol and atropine heart rate, as expected, decreased and increased. The variability coefficient, however did not change for propranolol but for atropine. The mean Lyapunov exponent that was about + 0.5 bits of information * s- ’ at baseline, increased after Table 3 Effects of submaximal exercise at 40 and 70% of symptom-limited work load on heart rate variability Rest Exercise 40% P’ Exercise 70% HR (beats/min) HR (WI%) Lyapunov l/f HF (%) LF (o/o) LF/HF TI (ms) 67 109 k4 1.8 f 0.2 0.56f -0.90* 4.0 f 0.04 0.04 0.7 17.4 f 3 4.9 f 0.7 204 *I9 *4 2.3 dcO.4 0.45 f 0.05 -0.95*0.01 4.4 3 2 93 slope of l/f < 0.001 146 NS NS 3.2 f0.7 0.24kO.l - 1.02 f 0.05 5.7 *3 3 +2 NS f 1.5 NS *1 l 0.01 < 0.001 < 0.001 +7 < 0.001 *4 I.1 f0.1 74 k6 P’ ANOVA < 0.001 < 0.001 NS NS < 0.01 < 0.001 NS NS NS NS < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 * Compared to rest. HR = heart rate; Lyapunov exponent (bits of information * s- ’ ), mean from 12 combinations of constants for 10 subjects; 1/f = slope of l/f distribution; HF = high frequency; LF = low frequency; Tl = time domain index. Values are given as mean f s.e.m. P-value or non-significance (NS) for ANOVA is given. 414 I. Hagerman et al./Cardiovascular Research 31 (1996) 410-418 Table 4 Heart rate (beats/min) calculated for the first, middle and last 30 beats of the 750 beats for the different interventions 05 0,5 - Baseline Propranolol Propranolol + atropine O-40,3 - Baseline 40% exercise 70% exercise 0 20 Workload, 40 60 80 100 Begin 71*3.5 59 f 2.4 88 f 3.6 Middle 70*3.2 59rt2.3 87f-3.6 End 70&-3.4 59k2.3 86k3.5 ANOVA NS NS 0.0005 72 i- 2.9 llOf3.3 149f4.2 7ljI3.07 113f3.3 152 f 4.2 70+3.1 114*3.1 155rt4.4 NS 0.002 O.OGQl Values are given as mean f s.e.m. f-value or non-significance (NS) for ANOVA is given. Watts Fig. 3. Approximate dominant Lyapunov exponent (bits of information* SC’) at rest and at 40 and 70% of symptom-limited ergometer exercise load. Values are given as mean f s.e.m. propranolol whereas following propranolol + atropine it decreased to almost half the value at baseline. With a registration accuracy of 20 kHz corresponding to 14 bits, this means that predictability is lost after about 30 and 60 s at baseline and after propranolol + atropine, respectively. I-IF% and LF% decreased similarly following propranolol and with a further decrease following addition of atropine. This means that the major spectral power after autonomic blockade resides in the very-low-frequency band. The l/f exponent, however, did not change and was around - 1 for the 3 measurements. The TI index did not change with propranolol whereas it decreased substantially after atropine. 3.3. Submaximal exercise stress test (Table 3) Mean work loads at 40 and 70% submaximal exercise were 74 f 7 and 132 Ifr 12 W/min, respectively. As expected, mean heart rate increased with increasing work load. The variability coefficient was unchanged with increasing work load. The Lyapunov exponent decreased curvilinearily (Fig. 3) but remained at 70% work load different from zero (P < 0.01). The decrease was compa- rable to that following autonomic blockade with propranolo1 + atropine. Contrary to following autonomic blockade the spectral HF% did not change from baseline whereas the LF% decreased to a similar degree as after autonomic blockade. The l/f exponent did not change with exercise. Incidentally, the Lyapunov exponent and TI index during both autonomic blockade and exercise showed similar patterns of relative changes as opposed to the other indices of heart rate variability. 3.4. Stationary of time series For calculation of the Lyapunov exponent it is essential that non-stationarity of the heart rate is kept to a minimum. Table 4 shows that while at baseline no differences in heart rate were observed, during the interventions heart rate for the first 30, middle 30 and last 30 beats of the 750 beats showed minimal differences. The dominant Lyapunov exponent based on the first 375, the last 375 and the total 750 beats for the different interventions did not differ (Table 5). Also no difference was seen in the behaviour at baseline and during the interventions. From Table 5 it is also evident that the relative change of the Lyapunov exponent following autonomic blockade and with exercise was the same when calculations were based on only the first 375, on only the last 375 or on the total 750 beats. Table 5 Approximate dominant Lyapunov exponents (bits of information * s- ’ ) based on the first and last 375 beats and the total of 750 beats for the different interventions Begin-Middle Middle-End Total ANOVA Baseline Propranolol Propranolol + a&opine 0.574 f 0.04 0.564 f 0.03 0.419 f 0.06 0.535 f 0.04 0.626 f 0.04 0.410 It 0.05 0.521 f 0.03 0.552 f 0.03 0.299 f 0.05 NS NS NS Baseline 40% exercise 70% exercise 0.614kO.05 0.500*0.06 0.329 f 0.05 0.585 f 0.04 0.513fO.08 0.336 f 0.07 0.555 f 0.04 0.445 f 0.07 0.243 f 0.05 NS NS NS Values are given as mean f s.e.m. P-value or non-significance (NS) for ANOVA is given. I. Hagerman et al./Cardiovascular 4. Discussion In healthy individuals, heart rate variability of sinus rhythm has characteristics of chaos-like determinism, with a positive Lyapunov exponent and l/f-like broad-band spectrum with an exponent of approximately - 1. This conclusion is at variance with Kanters et al. [23] who suggested a lack of evidence for low-dimensional chaos in heart rate variability. They, however, did not calculate the Lyapunov exponent. Lyapunov exponents have proven to be the most useful dynamic diagnostic for chaos-like systems [14] and any system containing at least one positive exponent is defined as being chaotic, with the magnitude of the exponent reflecting the time scale on which system dynamics being deterministic yet become unpredictable. A non-linear deterministic low-dimensional chaotic behaviour describes that the process is deterministically and homeostatically constrained within a certain range whereby it cannot wander off into infinity like a random process [6]. These results are in keeping with Osaka et al. [24] who calculated the correlation dimension on heart rate registered for 150 s before and after autonomic blockade. Deterministic non-linear estimates of heart rate variability can thus be determined with sufficient and meaningful accuracy under clinical conditions. This is of considerable interest as Skinner et al. [25] reported that a reduction in correlation dimension precedes lethal arrhythmias by hours. Development of diagnostic deterministic tools for the prediction of electrical instability and lethal arrhythmias may therefore become a new field of exploration. Do the Lyapunov exponent and the correlation dimension give different information as regards the complexity of a process? The correlation dimension describes the complex structure of the attractor approximating the fractal dimension and thereby indicating the number of oscillators on which the attractor is dependent. The Lyapunov exponent is a dynamic measure and describes the sensitive dependence on initial conditions - the hallmark of a deterministic chaotic process. Thus with the dominant Lyapunov exponent as the analytical tool, information on the importance of underlying oscillators has to be obtained through experimental interventions. For example, in the present experiments vagal withdrawal was shown to be a more important determinant of the dominant Lyapunov exponent than sympathetic tone. The method for calculating dominant Lyapunov exponents in this study is developed for experimental data, typically consisting of discrete measurements of a single variable [ 141. The computer program creates a database of delay-reconstructed data in a grid of a dimension defined by the parameter “embedding dimension”, which was held constant at 3, considered sufficient with regard to the amount of data available [14,15]. If the embedding dimension chosen is too large, one can expect that noise in the data will tend to decrease the density of points defining the attractor. Noise is an infinite dimensional process which, Research 31 (1996) 410-418 415 unlike the deterministic component of the data, fills each available phase space dimension in a reconstructed attractor. By varying “grid resolution”, the data are stored in different numbers of boxes. Typical values of grid resolution are in the range of 6 to 12 and, within reasonable bounds, the choice of grid resolution affects the efficiency, but not the accuracy of the exponent. In systems where the mechanism for chaos is unknown, exponent stability should be checked over different evolution times, affecting propagation times and replacement steps in the calculations. The value should be kept small enough that orbital divergence is monitored at least a few times per orbit, and sensitive dependence does not pull the measuring points too far apart. We chose evolution time to be 1 or 3 and obtained exponent stability. Minimum separation at replacement is the smallest length scale on which orbital divergence is monitored. To reduce the effect of error bar at the location of each phase space point, this parameter was held relatively small, not exceeding 2%. Minimum separation of time points, if chosen incorrectly, could affect the exponent estimate, as could maximum separation of time points, which defines the largest length scale on which orbital divergence is being monitored. Wolf [14], has for 3- and 4-dimensional reconstructions found a value of lo-15% of the range of time series values to be optimal. We tried both, with some variation in exponent stability but with maintained magnitude of positivity. The effects of noise in the algorithm of Wolf, as in any physical system, could partly be measurement noise. Samples obtained from different time series recorded at 20 kHz were therefore analyzed with a resolution of 5 digits (10-5), 3 digits (10m3> or 2 digits (lo-*), respectively, giving a positive Lyapunov exponent of comparable size. The algorithm was also tested with periodic data, derived with both high and low resolution from the Verhulst equation [6], giving a negative and stable Lyapunov exponent. Thus it appears that with the conditions used measurement noise is kept to a minimum and that the algorithm calculates both negative and positive values. A matter of concern is whether the number of data points is sufficient for this type of analysis. Correlation dimension analysis suggests that heart rate in the basal state has a fractal dimension between 2 and 3 [25]. This and the use of an embedding dimension of 3 suggest the use of least 1000 beats. Convergence of the dominant Lyapunov exponent, however, was demonstrated within 750 data points and was still obtained, and to the same numerical value, when changing embedding dimension and time delay to 4 and 3, respectively. Goldberger [19] achieved a broad-band l/f-like spectrum when sampling heart rate for 600 beats. Osaka et al. [24] used 140 to 240 beats when calculating the correlation dimension. Thus, from an empirical point of view 750 beats appear to be sufficient to calculate an approximate but informative dominant Lyapunov exponent. A minimum for a reliable estimate should be 50 to 100 orbits of the attractor with at 416 I. Hagerman et al./Cardiouascular least a few points per orbit. By eye-balling we found at baseline that the average orbit was about 4 beats, roughly corresponding to the respiratory cycle. Thus we have studied about 180 orbits with an approximate loss of about 2 bits of information*s-‘. Another concern is the degree on non-stationarity of the data [26]. Our registrations were made during stationarity or near stationarity. Although ANOVA shows that during the interventions there were small degrees of non-stationarity, it was minimal. It is difficult to see how such nonstationarity could have been avoided. For example, following propranolol + atropine, the average heart rate was 2 beats/min lower at the end of the registration period than at the start of the registration period. Thus the propranolol + atropine effect appears to be slowly eliminated towards the end of the registration period. To make a more accurate design would involve infusion of propranolol + atropine over longer periods of time. Such an approach would certainly become a major development of the method as the amount of propranolol + atropine needs to be individualised. Probably the whole experiment would have been difficult to pursue even in healthy subjects. From this observation it is also apparent that a longer period of registration after administration of propranolol + atropine would involve a larger degree of artefact as the propranolo1 + atropine effect becomes less apparent with time. The same kind of observation and reasoning holds for the approximate stationarity observed during submaximal exercise. We thus conclude that we have studied the approximate steady state with a degree of accuracy that is attainable during clinical conditions. The next question is whether our results are not the result of non-stationarities. We certainly agree that this is a significant problem. Especially when the degree of complexity or chaos is estimated as a static property like the fractal dimension or correlation dimension. With such a method a changing time series is likely to alter the clustering of data. A dynamic estimate such as the Lyapunov exponent that with frequent resettings estimates the average rate of orbital divergence should be less sensitive to non-stationarity and thus perhaps be more suitable for clinical time series. In any case the positive dominant Lyapunov exponents that we obtained could not have been due to the slight non-stationarity we had in our time series. As the non-stationarity has a trend, such a trend should decrease the Lyapunov exponent or result in a Lyapunov exponent not different from zero or a negative Lyapunov exponent. Following propranolol + atropine, however, the non-stationarity was a fading propranolol + atropine effect which if anything should have increased the Lyapunov exponent. In the heart, the self-similar fractal branching pattern has been observed in the right atria1 musculature, in the cordae tendinae and in the His-Purkinje conduction network [27]. The fractal nature of the His-Purkinje cells results in a frequency spectrum of the QRS complex, Research 31 (1996) 410-418 which takes on the form of an inverse power law. This predicted inverse power law relationship is borne out by Fourier analysis of the normal QRS waveform. Goldberger also examined in healthy subjects the variations in heart rate intervals [27,28] which were found to be substantial. This variability exhibits an inverse power-law relationship qualitatively similar to that in the QRS waveform. In a number of physiological parameters the slope of the line is believed to be a useful index of spectral reserve, and therefore healthiness [20]. The exponent in the case of heart rate variability is reported to be approximately - 1 [27], and this was also obtained in our study. The dominant Lyapunov exponent decreased with atropine. During exercise the dominant Lyapunov exponent approached but did not attain zero or a negative value. Also the l/f exponent remained unaltered around - 1, describing unaltered high spectral power in the very-low-frequency band. If random noise had influenced the dominant Lyapunov exponent to be close to zero, the l/f dimension would probably not have been stable around - 1. Although we did not observe any reactivity in the l/f slope, it can be modulated. Wagner and Persson reported that in a canine model the l/f slope of arterial blood pressure sure time series changed after baroreceptor denervation and blockade of the autonomic nervous system [29]. Thus even during physical stress with twice as high a heart rate as during rest, heart rate is determined by deterministic chaos and a strange attractor. From rest the dominant Lyapunov exponent decreased curvilinearily and by extrapolation it was hypothesised to attain zero and thus a stable periodic behaviour around 90% of symptom-limited exercise capacity. Therefore, in three of the volunteers an attempt was made to reach steady-state conditions at this level of exercise capacity but appeared not to be attainable. These results are in keeping with Nakamura [30], who in healthy individuals performed prolonged exercise under quasisteady-state conditions until exhaustion and showed changes in l/f” slope and derived fractal dimensions indicative of less complexity in the system, a change towards stable, periodic behaviour although such behaviour was not attained. The dimension of the dominant Lyapunov exponent was affected by pharmacological autonomic blockade, and during exercise probably due to release of vagal withdrawal. As described by Goldberger [31], the fluctuations in the normal heart beat on short and longer time scales are related to the competing influence of the two branches of the autonomic nervous system, which appear to interact in a non-linear manner, under healthy conditions [32]. The decrease in spectral power of both HF and LF bands with autonomic blockade, and particularly when cardiac vagal activity was reduced, is consistent with studies by Akselrod and others [4,17,33] as is the decrease in the time domain index [33]. Montano et al. [34] have recently evaluated LF and I-IF components in absolute units and in normalized units, indicating that normalized values of both I. Hagerman et al./Cardiovascular LF and HF components may have the highest degree of correlation to changes in sympathovagal balance, although LF and I-IF expressed as percent values of total power also did correlate significantly. The effect of propranolol was more pronounced in the LF band, which reflects that both the sympathetic and the parasympathetic systems mediate low-frequency fluctuations, while parasympathetic activity dominates at higher frequencies. The parallel shift in frequency and time domain indexes and Lyapunov exponent supports a major autonomic influence over non-linear behaviour of heart rate variability, as previously suggested both from a theoretical [S] and an empirical standpoint [6,31]. Parasympathetic activity, however, seems to be a more important determinant than sympathetic activity. During moderate exercise the power in the LF band decreased and remained at the same level during submaximal exercise, despite increased sympathetic drive, reflected by the marked increase in heart rate. This might be due to the fact that spectral power in the LF band depends not only on the activity of the sympathetic nervous system but also on the baroreceptor cardiac reflex. It has been reported that in moderate to severe exercise, the sympathetic activity is elevated [35] but that the baroreceptor control of the heart is inhibited [36] and the LF oscillations decrease [37,38]. Somewhat conflicting, the power in the HF band did not change significantly during exercise as one might expect, at least during moderate exercise with reduced vagal activity. However, similar results were reported by Perini et al. [38] when expressing the power of each component as a percentage of the total spectral power. We have demonstrated that autonomic blockade and exercise modulates chaos-like determinism of heart rate regulation and variability, but does not, at least under the present experimental conditions, transfer heart rate regulation to a stable periodic attractor. Two major determinants appear to be parasympathetic activity and to a lesser degree sympathetic activity. The reactivity of the Lyapunov exponent to the two investigated interventions was similar to that of the TI index, but different from the other established measures of heart rate variability such as the coefficient of variation, high- and low-frequency spectral power, the low-frequency to high-frequency ratio and the I/f exponent. Therefore the Lyapunov exponent might be an independent and deterministic characteristic of heart rate regulation and its integrity. Acknowledgements This study was supported by grants from the Karolinska Institute, ELFA Research Foundation and the Swedish Heart and Lung Foundation. References [l] Chialvo DR. Low dimensional chaos in cardiac tissue. Nature 1990;343:653. Research 31 (19%) 410-418 417 [2] Rosenblueth A, Simeone FA. The interrelations of vagal and accelerator effects on the cardiac rate. Am J Phvsiol 1934;l l&42-55. [31 Appel ML, Berger RD. Saul JP, Smith SM, Cohen R. Beat to beat variability in cardiovascular variables: noise or music? J Am Coil Cardiol 1989;14:1139-1148. t41 Akselrod S, Gordon D, Ubel FA, Shannon DC, Barger AC, Cohen RJ. Power spectrum analysis of heart rate fluctuations: a quantitative probe of beat-to-beat cardiovascular control. Science 1981;213:220222. El Michaels DC, Chialvo DR. Matyas EP, Jahfe J. Chaotic activity in a mathematical model of the vagally driven sinoatrial node. Circ Res 1989;65:1350-1360. b1 Denton TA, Diamond GA, Helfant RH, Khan S, Karagueuzian H. Fascinating rhythm: a primer on chaos theory and its application to cardiology. Am Heart J 1990,120:1419-1440. [71 Kobayashi M, Musha T. l/f fluctuations of heart beat period. IEEE Trans Biomed Eng 1982;29:456. 181Bigger JT, Fleiss JL, Steinman R, Rolnitzky LM, Kleiger RE, Rottman JN. Frequency domain measures of heart period variability and mortality after myocardial infarction. Circulation 1992;85: 164171. I91 Ruelle D. Sensitive dependence on initial condition and turbulent behavior of dynamical systems. Ann NY Acad Sci 1979;316:408416. [lOI Jose AD. Effect of combined sympathetic and pamsympathetic blockade on heart rate and cardiac function in man. Am J Cardiol 1%6:18:476. [III Jose AD, Collision D. Autonomic blockade by propranolol and atropine to study intrinsic myocardial function in man. J Clin Invest 1%9;48:219. t121 Jose AD, Stitt F, Collison D. The effects of exercise and changes in body temperature on the intrinsic heart rate in man. Am Heart J 1970;79:488. [I31 &.trom H, Jonsson B. Design of exercise test, with special reference to heart patients. Br Heart J 1976.38289. [141 Wolf A, Swift JB, Swinney HL, Vastano JA. Determining Lyapunov exponent from a time series. Physica 1985;16D:285-317. iI51 Wolf A. Quantifying chaos with Lyapunov exponents. In: Holden AV, ed. Chaos. Princeton: Princeton University Press, 1986;273290. [I61 Cain ME, Ambros D, Witkowski FX, Sobel BE. Fast-Fourier transform analysis of signal-averaged electrocardiograms for the identiflcation of patients prone to sustained ventricular tachycardia. Circulation 1984;69:71 l-720. [I71 Pagani M, Lombardi F, Guzzetti S, et al. Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ Res 1986;59:178-193. b31 Lipsitz LA, Mietus J, Moody GB, Goldberger AL. Spectral characteristics of heart rate variability before and during postural tilt. Circulation 1990,81(6):1803-1810. t191 Goldberger AL, Rigney DR. Nonlinear dynamics at the bedside. In: Glass L, Hunter P, McCulloch A, eds. Theory of Heart. Biomechanits, Biophysics and Nonlinear Dynamics of Cardiac Function. New York Springer Verlag, 1991;583-605. DO1Eberhart RC. Chaos theory for the biomedical engineer. IEEE Eng Med Biol Mag 1989;8:41-45. Dll Cripps TR. Malik M. Fare11 TG, Camm AJ. Prognostic value of reduced heart rate variability after myocardial infarction: clinical evaluation of a new analysis method. Br Heart J 1991;65:14-19. [221 Kleiger RE, Miller JP, Bigger JT, Jr, Moss A. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am J Cardiol 1987;59:256-262. t231Kanters JK, Holstein-Rathlou N-H, Agner E. Lack of evidence for low-dimensional chaos in heart rate variability. J Cardiovasc Electrophysiol 1994;5:591-601. [%I Osaka M, Saitoh H, Atarashi H, Hayakawa H. Correlation dimen- 418 [25] [26] [27] [28] [29] [30] [31] I. Hagennan et al./Cardiovascular sion of heart rate variability: a new index of human autonomic function. Front Med Biol Eng 1991;5:289-300. Skinner JE, Pratt CM, Vybiral T. A reduction in the correlation dimension of heartbeat intervals precedes imminent ventricular tibrillation in human subjects. Am Heart J 1992.125731-743. Elbert T, Ray WJ, Kowalik ZJ, Skinner JE, Graf KE, Birbaumer N. Chaos and physiology: deterministic chaos in excitable cell assemblies. Am Physiol Sot 199474: l-47. Goldberger AL, West BJ. Fractals in physiology and medicine. Yale J Biol Med 1987;60:421-43.5. Goldberger AL, Fmdley LJ, Blackbum MR. Mandell AI. Nonlinear dynamics in heart failure: implications of long-wavelength cardiopulmonary oscillations. Am Heart J 1984; 107:612-615. Wagner CD, Persson PB. Two ranges in blood pressure power spectrum with different l/f characteristics. Am J Physiol 1994;267:H449-H454. Nakamura Y, Yamamoto Y, Muraoka I. Autonomic control of heart rate during physical exercise and fractal dimension of heart rate variability. J Appl Physiol 1993;74:875-881. Goldberger AL. Fractal electrodynamics of the heartbeat. Ann NY Acad Sci 1990,591:402-409. Research 31 (19%) 410-418 [32] Goldberger AL. Is the normal heart beat chaotic or homeostatic? News Physiol Sci Am Physiol Sot 1991;6:87-91. [33] Hayano J, Sakakibara Y, Yamada A, et al. Accuracy of assessment of cardiac vagal tone by heart rate variability in normal subjects. Am J Cardiol 1991;67:199-204. [34] Montana N, Ruscone T, Porta A, Lombardi F, Pagani M, Malliani A. Power spectrum analysis of heart rate variability to assess the changes in sympathovagal balance during graded orthostatic tilt. Circulation 199490: 1826- 183 1. 1351 Ekblom B, Goldbarg A, Kilbom A, ,&strand P-O. Effect of atropine and propranolol on the oxygen transport system during exercise in man. Sand J Clin Lab Invest 1972;30:35-42. [361 Bristow JD, Brown EB, Cunningham DJC, et al. Effect of bicycling on the baroreflex regulation of pulse interval. Circ Res 1971;28:582-591. [371 Arai Y, Saul JP, Albrecht P, et al. Modulation of cardiac autonomic activity during and immediately after exercise. Am J Physiol 1989;256:H13233141. [38] Perini R, Grixio C, Baselli G, Cerutti S, Veicsteinas A. The influence of exercise intensity on the power spectrum of heart rate variability. Eur J Appl Physiol 1990,61:143-148.