Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
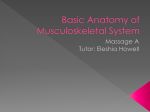
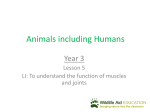
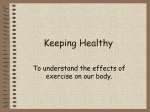
26 Foundations of Exercise Science Skull Cervical Vertebra Clavicle Manubrium Scapula Sternal Body Rib Humerus Xiphoid Process Thoracic Vertebra Lumbar Vertebra Ulna Radius Os Coxae Sacrum Coccyx Carpal Bone Metacarpal Phalanx Femur Patella Tibia Fibula Medial Malleolus Lateral Malleolus Tarsal Bone Metatarsal Phalanx Figure 2.6 The human skeleton anterior view. 28 Foundations of Exercise Science appendicular skeleton is responsible for a large portion of the movements we perform. Axial Skeleton Skull The skull is divided into two major parts. The curved flat bones form the calvaria, or vault that protects the brain and brain stem. The irregular bones of the face give it its individuality, and provide protection for eyes, air passages, chewing, and entry of food into the body (Figure 2.8). Calvaria The calvaria is formed by the frontal, parietal, temporal, occipital, bones. These may be fractured and sphenoid by blows to the skull (Figure 2.8), for example, as a result of being checked or hitting the skull on the ice when playing hockey. The more fragile of the calvaria bones is the temporal bone and it overlies one of the major blood vessels supplying the membranes protecting the brain. If the temporal bone is fractured and displaced internally, it can cut the middle meningeal artery, resulting in an epidural haemorrhage (bleeding between the skull and the meninges, or protective covering of the brain; see Figure 2.8). This is a clinical emergency and bleeding must be stopped as quickly as possible so that blood collecting within the vault of the skull does not compress the brain, which is soft (the consistency of toothpaste) and easily damaged. A good reason for sport helmets, if you ever questioned their necessity. Facial Bones The facial bones (Figure 2.8) include the nasal (nose), lacrimal (for drainage Parietal Bone Frontal Bone Sphenoid Bone Lacrimal Bone Nasal Bone Zygomatic Bone Maxilla Occipital Bone Temporal Bone (mastoid process of) Mandible Anterior View Figure 2.8 Anterior and left lateral view of the skull with epidural haemorrhage. Studying Human Movement and Health Clavicle (superior view) 31 turn articulate with the digits (fingers). All digits except the thumb are made up of three phalanges (singular = phalanx), proximal, middle, and distal. The thumb has only two phalanges, proximal and distal (Figure 2.11). Pelvic Girdle The pelvic girdle is formed from Scapula (anterior view) the paired os coxae or hip bones (comprised of the ilium, pubis, and ischium) which join with the sacrum posteriorly and join each other anteriorly to form a basin-like girdle which supports the bladder and abdominal contents. On the lateral surface of the os coxae is a cup-shaped acetabulum for the head of the femur (Figure 2.12). Humerus (anterior view) Radius Scaphoid Trapezium Capitate Trapezoid Ulna Lunate Triquetral Pisiform Hamate 1st Metacarpal Radius (anterior view) 5th Metacarpal Sesamoid Bone Ulna (anterior view) 5th Digit Proximal Phalanx 2nd Digit Middle Phalanx Carpal Bone (anterior view) Metacarpal (anterior view) Phalanx (anterior view) 3rd Digit Distal Phalanx Figure 2.11 Major bones comprising the upper limb. Studying Human Movement and Health 33 Navicular Talus Intermediate Cuneiform Lateral Cuneiform Femur (anterior view) 1st Metatarsal 1st Digit Proximal Phalanx Cuboid 5th Metatarsal 5th Digit Middle Phalanx Calcaneus Lateral View of Right Foot Patella (anterior view) Calcaneus Talus Tibia (anterior view) Cuboid Navicular Lateral Cuneiform Fibula (anterior view) Intermediate Cuneiform Medial Cuneiform 5th Metatarsal 1st Metatarsal Lateral Malleolus 5th Digit Proximal Phalanx Medial Malleolus Calcaneus (dorsal view) Talus (dorsal view) Navicular (dorsal view) Metatarsal (dorsal view) Phalanx (dorsal view) 1st Digit Distal Phalanx Dorsal View of Right Foot Figure 2.13 Major bones comprising the lower limb. 34 Foundations of Exercise Science Joints may also be classified according to their motion capabilities; some allow for a great deal of movement, while others are severely restricted. The joints which exhibit the least mobility are fibrous and cartilaginous. These joints can absorb shock but permit little movement, if any (e.g., interosseous ligaments). There are also slightly movable joints that are cartilaginous and can also attenuate applied forces (e.g., intervertebral joints and the symphysis pubis). The joints that allow the greatest amount of motion are the synovial joints, which have only slight limitations to movement capability, making possible a wide array of movements. The characteristics of synovial joints are presented in the box on the right. The following discussion will therefore focus on synovial joints. Types of Synovial Joints Hinge (Ginglymus) Joint This type of joint has one articulating surface that is convex, and another that is concave. Examples include the humero-ulnar joint at the elbow and the interphalangeal joints of the fingers. Pivot Joint In these types of joints, one bone rotates around one axis. For example during pronation– supination of the forearm, the radius rotates along its long axis and the ulna remains fixed. (Knuckle) • There is a joint capsule lined with a synovial membrane that secretes the lubrication fluid for the joint. The capsule may or may not have thickenings called intrinsic ligaments that add support. • There is a joint cavity surrounded by the capsule. • There is a capillary layer of synovial fluid to lubricate the joint. • Outside the capsule and not connected to it are extrinsic ligaments that support the joint and connect the articulating bones of the joint. • Some joints have special features such as Synovial joints vary widely in structure and movement capabilities and may be classified in different ways – by the movements possible at the joint or simply by the axes around which the joint can be moved. The more common classification is based on the shape of the joint (Figure 2.14). Condyloid Characteristics of Synovial Joints Joint The joint surfaces are usually oval as in the joint between your third metacarpal (bone of the hand) and the proximal phalanx (bone) of your third digit. One joint surface is an ovular convex shape, and the other is a articular discs, discs fibrocartilaginous labra (singular = labrum) and menisci (singular = meniscus), and intracapsular tendons tendons. reciprocally shaped concave surface. At this joint, flexion–extension, abduction–adduction, and circumduction are all possible. Saddle Joint The bones are set together as in sitting on a horse. This is seen in the carpometacarpal joint of the thumb. Movement capability at this joint is the same as the condyloid joint, but with a greater possible range of motion permitted. Ball and Socket Joint A rounded bone is fitted into a cup-like receptacle. This is the kind of joint found at the shoulder and the hip where rotation in all three planes of movement is possible. Plane (Gliding) Joint This joint permits gliding movements as in the bones of the wrist. The bone surfaces Studying Human Movement and Health 35 Plane (Gliding) Found in bones of the wrist and the acromioclavicular joint of the shoulder. Pivot Found in the atlantoaxial joint of the neck, and in the forearm during pronation– supination. Ball and Socket Found in the hip and shoulder. Hinge (Ginglymus) Found in the elbow. Condyloid (Knuckle) Found in the joints between the metacarpals and phalanges – except at the thumb. Saddle Found in the carpometacarpal joint of the thumb. Figure 2.14 Typical synovial joints of the human body. Studying Human Movement and Health 41 Fibula Tibia Medial Malleolus Lateral Malleolus Calcaneus Talus Talocrural Joint A Transverse Tarsal Joint Talus Calcaneus Navicular Intermediate Cuneiform Lateral Cuneiform B Cuboid Figure 2.20 Ankle and foot joints. A. Dorsal view. B. Lateral view. Ankle Joint Several bones, the medial and lateral malleoli of the tibia and fibula, the head of the talus, and the calcaneus (heel bone), are involved in the ankle (talocrural) joint (Figure 2.20). The talus is wedged into the mortise formed by the medial and lateral malleoli. Because the talus is wider anteriorly than posteriorly, when you dorsiflex at the ankle, you put the ankle into its most stable position. This is the reason for the forward cant in a downhill ski boot. The ankle is least stable in the “en pointe” position in ballet, putting great pressure on dancers’ ligaments and tendons, and increasing the risk of injury. Foot and Toe Joints There are two rows of tarsal bones of the transverse Movement between the proximal and tarsal joint. 44 Foundations of Exercise Science Trapezius (upper fibres) Sternocleidomastoid Deltoid Pectoralis Major Serratus Anterior Pectoralis Minor Biceps Brachii Brachialis External Oblique Brachioradialis Wrist Flexor Group Rectus Abdominis Internal Oblique Pectineus Sartorius Gracilis Vastus Lateralis Tensor Fasciae Latae Adductor Group Rectus Femoris Vastus Medialis Tibialis Anterior Figure 2.24 Anterior muscles of the human body. 46 Foundations of Exercise Science Sternocleidomastoid Deltoid Pectoralis Major Pectoralis Minor Serratus Anterior A Sternocleidomastoid Deltoid Pectoralis Major Serratus Anterior B Figure 2.26 Anterior muscles of the pectoral girdle. A. Anterior view. B. Lateral view. Muscles Connecting the Humerus and Scapula to the Axial Skeleton Anterior and Posterior Groups Muscles acting to hold the pectoral girdle to the chest wall can be divided into anterior and posterior groups as follows. Anterior Group Pectoralis major has two heads. The clavicular head (attached to the clavicle) flexes and medially rotates the shoulder joint; the sternal head (attached to the sternum) extends the shoulder joint from a flexed position and medially rotates the shoulder joint. Pectoralis minor depresses and stabilizes the scapula. Serratus anterior steadies and holds the scapula forward (protracts it) against the chest wall (Figure Studying Human Movement and Health 47 Scapula–Humeral Region 2.26). This frees the upper limb for actions such as rope climbing. These muscles as a group would also be required to perform the butterfly stroke in swimming. The following muscles from the scapula to the humerus act across the shoulder joint. Their primary role is to stabilize the shoulder joint to allow full use of the upper limb. Posterior Group Trapezius has three groups of fibres reflecting their relative positions. The upper fibres elevate the scapula, middle fibres retract the scapula, and lower fibres depress the scapula. Latissimus dorsi medially rotates, adducts, and extends the humerus, and teres major medially rotates the humerus (Figure 2.27). Anterior Group Subscapularis adducts and medially rotates the upper limb. (Figure 2.27 C). Superior and Posterior Group Supraspinatus initiates abduction of the upper limb at the shoulder joint. Infraspinatus and teres minor adduct and Trapezius (upper fibres) Supraspinatus Trapezius (middle fibres) Infraspinatus Trapezius (lower fibres) Deltoid Teres Minor Teres Major Subscapularis Erector Spinae Latissimus Dorsi A B C Figure 2.27 Muscles of the back and scapula–humeral region. A. Superficial posterior muscles of the back. B. Posterior muscles of the scapula–humeral region, deep and lateral to latissimus dorsi. C. Anterior subscapularis muscle of the scapula–humeral region. Studying Human Movement and Health Posterior Compartment Triceps brachii has three heads. The medial and lateral heads are attached to the humerus. They join with the long head from the scapula to attach distally to the olecranon process of the ulna. It is the powerful extensor of the elbow (Figure 2.29 B). Muscles of the Forearm The distal end of the humerus widens into lateral and medial epicondyles which provide attachments for muscle groups that act on the forearm and wrist. The forearm muscles act on the elbow, wrist, and digits (fingers and thumb). Muscles attached to the medial epicondyle of the humerus are the flexor–pronator group (Figure 2.29 A) while those 49 attached to the lateral epicondyle of the humerus are the extensor–supinator group (Figure 2.29 B). One muscle attached above the lateral epicondyle of the humerus is the brachioradialis muscle. It is on the extensor side of the humerus but, because it is positioned anterior to the elbow joint, it acts as an elbow flexor, especially when the forearm is partially pronated. You use this muscle when you shake hands with someone. Muscles of the Hand These muscles are divided into groups. The thenar (palm) group acts on the thumb and its metacarpal to abduct, flex, and oppose the thumb tip to the four remaining digits. The Deltoid Deltoid Biceps Brachii Triceps Brachii Brachioradialis Brachialis Brachioradialis Flexors of the Wrist and Digits Extensors of the Wrist and Digits A B Figure 2.29 Muscles of the right arm and forearm. A. Anterior view. B. Posterior view. 50 Foundations of Exercise Science acts on the little finger and its metacarpal. Together the thenar and hypothenar muscles permit you to cup your hand as in holding a baseball. Between these two groups lie the interossei (between bones) and the lumbrical (earthworm) muscles that are referred to collectively as the intrinsic (within) muscles of the hand. Together they flex, extend, abduct, and adduct the fingers, positioning the digits for fine movements. hypothenar (little palm) group Muscles of the Pelvic Girdle From the bony pelvis, muscles are attached that permit a wide range of movement in the lower limb; but here, stability and transfer of weight for walking are the prime focus, not the fine discriminatory movements that are necessary with the hands and fingers. Some of the muscles acting at the hip joint come from the abdomen; others come from the sacrum and external surface of the hip bone (os coxae). Because the hip joint is a ball and socket joint, flexion–extension, abduction–adduction, medial and lateral rotation, as well as circumduction can all occur here. Try it yourself. Notice, however, that the movement here is more limited than at the shoulder joint. Anterior Group Psoas major (from the abdomen) and iliacus (from the iliac fossa of the pelvis) unite to form the iliopsoas muscle that crosses the anterior aspect of the joint and is the primary flexor of the hip, allowing you to bring your thighs up to your chest or your chest to your knees (Figure 2.30). Posterior and Lateral Group Large gluteal muscles cover the hip posteriorly. Put your hand on your hip and extend the joint. Feel the large muscle mass as it contracts. These are the three gluteals. The largest and most superficial posterior muscle, gluteus maximus, is the principal power extensor of the hip. Gluteus medius and minimus lie deep and lateral to maximus and in that order, Psoas Major Iliopsoas Iliacus Sacrum Femur Figure 2.30 Anterior muscles of the pelvic girdle.