Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Human cytomegalovirus wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Ebola virus disease wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Plasmodium falciparum wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Leptospirosis wikipedia , lookup
Onchocerciasis wikipedia , lookup
Sarcocystis wikipedia , lookup
Cross-species transmission wikipedia , lookup
Marburg virus disease wikipedia , lookup
West Nile fever wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Hepatitis C wikipedia , lookup
Schistosomiasis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Henipavirus wikipedia , lookup
Schistosoma mansoni wikipedia , lookup
Chagas disease wikipedia , lookup
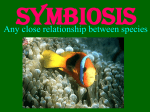
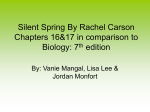
Overview Bedbugs in the 21st Century: The Reemergence of an Old Foe Katelyn Williams, BS,1 Monte S. Willis, MD, PhD2* ABSTRACT Bedbugs are small parasites that feed exclusively on blood from vertebrates, including humans. Attention to these parasites largely disappeared until the past decade, when their incidence grew sharply due to increased international travel, use of less-effective insecticides, and growing insecticide resistance among bedbugs. Bedbugs can be found virtually anywhere, including homes, offices, hotels, and hospitals. They are a severe nuisance and have a real psychological and financial impact on those infested; however, their medical importance is limited. Although more than 40 infectious diseases Insects of the Cimicidae family, more generally known as bedbugs, are small parasites that feed exclusively on blood from vertebrates.1 Attention to these parasites largely disappeared until the past decade, not only in the scientific literature but also in the news media.2 Although more than 40 infectious diseases have been suspected of being transmitted by bedbugs, this transmission has not been proven, to our knowledge. However, bedbugs can cause great psychological stress because of their incorrect association with poor hygiene and poverty. In this review, we discuss the biological characteristics of Cimex lectularius and C. hemipterus, reasons for their increasing prevalence during the past two decades, the public health risks they pose, and countermeasures available to identify and treat infestations. The goal of this article is to put the news-media accounts of bedbugs into the proper context of our current scientific understanding of this notorious pest. DOI: 10.1309/LM1TBJG6S7USSKEN Abbreviations DDT, dichlorodiphenyltrichloroethane; HBV, hepatitis B virus; HIV, human immunodeficiency virus; HCV, hepatitis C virus; PCR, polymerase chain reaction Department of Biological Sciences, Hampton University, Hampton, Virginia, 2 McAllister Heart Institute, Department of Pathology and Laboratory Medicine, University of North Carolina, Chapel Hill, North Carolina 1 *To whom correspondence should be addressed. E-mail: [email protected] www.labmedicine.com may be transmitted by bedbugs, actual transmission of any of those diseases has not been proven to date. This review presents the biological characteristics of Cimex lectularius and C. hemipterus, the public health risks of those parasites, and countermeasures to identify and treat infestations. The goal is to put news-media accounts of bedbugs into the proper context of our current scientific understanding of their characteristics. Keywords: clinical pathology, microbiology, virology, AP infectious disease Background and Appearance Bedbugs are “true bugs” of the order Hemiptera. Insects in this order mostly have wings that are half sclerotic and half membranous (“kissing bugs” of the same order transmit Trypanosoma cruzi [Chagas disease]). Bedbugs are part of the family Cimicidae and are commonly referred to as cimicids. Cimicids can infest not only human households but also the environment of birds (including chickens), bats, and certain domestic animals.3 Cimicids are parasites unique among obligate blood feeders because they do not remain on the host to complete their life cycle. After feeding, they move to local areas and hide in places where their host is resting, such as a bed or a couch. The two species of bedbugs that most commonly affect humans are C. lectularius and C. hemipterus. Their identification is possible only by specialists; both sexes are hematophagous and can live for 12 months without feeding (as long as 1.5-2.0 years in colder environments).4 C. lectularius is found in temperate climates including parts of the United States, whereas C. hemipterus is found mainly in tropical climates. However, both can be found in every type of climate due to their easy portability by travelers. Differentiating these species is not simple; further, more than one species may be found in an infestation. C. lectularius ranges in size from 5 to 7 mm; although C. hemipterus is longer, these species can interbreed5 and their sizes may overlap. Before feeding, Summer 2012 | Volume 43, Number 5 Lab Medicine 141 Overview Image 1 Adult bedbug feeding on a human host. Their flat, oval-shaped bodies are reddish brown until they feed, at which point they become reddish and round. Courtesy of http:// www.wikimediacommons.org. bedbugs have flat, reddish brown, oval-shaped bodies; their size is comparable to that of a dog tick. After feeding, the bedbug’s flat body becomes elongated and appears more reddish than brownish (Image 1). Juvenile bedbugs (eg, nymphs) can be as small as 1.5 mm and are yellow to translucent in color before feeding; immediately after feeding, they are bright red. Life Cycle Infestations of bedbugs occur throughout the world. They have long been associated with economically poorer regions; however, they are frequently found in areas to which people travel or in places frequented by many individuals (eg, hotel rooms).6 Institutional facilities and multi-dwelling homes are susceptible because bedbugs may move from one local area to another, affecting many people. Bedbugs do not inhabit the visible surfaces of beds, couches, or chairs. Rather, they move to crevices and cracks, such as the seams of chairs, mattresses, in wallpaper, between couch cushions, and into the folds of curtains. They come out of their hiding places every 5 to 10 days to feed.7 In developing countries, they are commonly found not only in the crevices of mud houses but also in thatched roofs. Infestations are common in refugee camps; for example, 98% of rooms investigated in a refugee camp in Sierra Leone had bedbugs, with 86% of the residents having evidence of bedbug bites.8 Bedbugs can sense and locate warmth and carbon dioxide production, 9,3,10 allowing them to easily 142 Lab Medicine Summer 2012 | Volume 43, Number 5 migrate toward humans.7 They walk at approximately the same rate as ladybugs. Their appearance within a home owes solely to human dispersal. Humans constantly move throughout their homes; therefore, bedbugs can also be found inside personal items, and suitcases.11 Bedbugs feed for approximately 5 minutes per night. Bite marks are typically found on the neck, face, hands, and arms of the host, depending on what parts are exposed during his or her resting period. Bite marks can be found on various parts of the body because some individuals may toss and turn in their sleep, which, in turn, exposes more skin the bedbugs can bite. Most people do not feel the bite marks until several days later; in some cases, an urticarial reaction to the bite can occur.7 When bedbugs feed, they deliver anticoagulant factors, vasodilatory compounds (including the nitric oxide-carrying protein nitrophorin)12 and proteolytic enzymes via their saliva, promoting local hypersensitivity (ie, urticarial) reactions.3 Bedbugs use 2 separate elongated stylets during feeding: one withdraws the blood without clotting and the other injects the saliva that makes their feeding pain-free to the host.13 Male bedbugs direct their sexual activity toward females that have recently fed; each female undergoes approximately 5 traumatic inseminations after each feeding.1 Sperm is deposited by the male’s intromittent organ, bypassing the female genital tract, piercing the cuticle.4 Sperm is injected into the mesospermagele, a female organ that directs the migration of sperm. Female mortality is common during copulation; however, on average, each fertilized adult www.labmedicine.com Overview Life Cycle: The Bedbug Life Cycle 1 Egg 5 Nymph stages (N1-N2-N3-N4-N5) 1 Adult (male or female) Haematophagy for each nymph stages (N1-N5) and male and female adults Adult male Time of a blood meal Time between two blood meals Adult female Traumatic insemination Adult life span Duartion of life cycle (egg to egg): Egg Mating frequency After mating, females stop laying fertilized eggs after Males impose a mating rate on females N1 N5 N2 N4 N3 Time to egg laying after mating Female egg laying rate, always in excess Hatching time Time between two nymph stages (blood meal obligatory) Lifetime total number eggs laid by a female 30-45 days after contamination by a few bedbugs, their number is exponentially multiplied Figure 1 The life cycle of C. lectularius or C. hemipterus. The life cycle of cimicids includes the egg stage, 5 nymph stages (N1, N2, N3, N4, and N5), and the adult stage. From Delaunay P et al., 2011.4 Used with permission ©2011. female yields 200 to 500 eggs in her lifetime. Eggs hatch in 4 to 10 days on average, leading to nymphs 1 to 3 mm long. There are 5 nymph stages (Figure 1), each requiring a blood meal lasting 10 to 20 minutes. These stages are passed every 3 to 7 days until adulthood is reached; this explains how a previously noninfested home may, in a single month, undergo an exponential multiplication of bedbugs. Bedbugs are generally active in the dark and emit a strong, distinct odor resulting from the oils (containing 4-oxoaldehydes, among other chemicals) secreted by their dorsal abdominal glands.14 Clinical Manifestations When a cimicid feeds with its proboscis, it pierces the skin (this behavior is often incorrectly called biting), which may cause skin reactions in individuals responding to cimicid saliva. 3 Because the urticarial reaction is allergic in nature, not all individuals experience it; some individuals do not respond at all. Often, reactions to a bite are minor: the typical skin lesion is a pruritic, erythematous, firm papule (ie, an itchy, red, edematous reaction) 5 to 20 mm in diameter with a central vesicle or hemorrhagic crust at the point where the proboscis had entered.4 These skin reactions may www.labmedicine.com be mistaken for spider bites or mosquito bites, particularly in developed countries in which bedbugs are not common. Many victims of bedbug bites are misdiagnosed by their doctors with hives or scabies.15 Bedbug bites can be identified by their distribution to the uncovered areas of the skin, sometimes appearing in a row (whimsically referred to as “breakfast, lunch, and dinner”).16 Situational cues that support the correct diagnosis include the patient awakening with new lesions and the presence of bedbug fecal smears or blood flecks on bed linen and on the patient’s skin. These clues may prompt an inspection of crevices, the mattress lining, and the box springs to reveal any additional bedbugs. Finally, the pungent odor of the oils released by bedbugs may be identified locally or throughout the residence. The microscopic anatomy of a bedbug bite resembles those of various insect and arthropod hypersensitivity reactions. It involves a perivascular infiltrate within the upper dermis that includes histiocytes, mast cells, eosinophils, and lymphocytes.17 Mast cells release histamine and other substances during an allergic reaction: histamine causes the itchy sensation humans feel after being bitten by a bedbug or a mosquito. Every individual bitten by a bedbug does not have an allergic reaction to the saliva of the bug; however, when a reaction occurs, Summer 2012 | Volume 43, Number 5 Lab Medicine 143 Overview further treatment is needed. For those that have an allergic reaction, itchy, red wheals appear and can become infected through scratching. In most cases, bites will heal after 1 week. If the reaction to the bite is deemed to be severe, antihistamines or a corticosteroid (eg, hydrocortisone) is given to suppress itching; an antibiotic is prescribed only if a secondary infection develops due to excessive scratching.16 Antihistamines are highly effective for reducing itching; however, there is a risk that they will reduce the patient’s ability to detect an ongoing infection. Prevention of Further Bites To prevent bedbugs from taking further blood meals, patients can cover exposed skin, which will prevent bites. Nighttime sleepwear covering as much skin as possible can block the relatively weak skin-piercing apparatus of the bedbug, which cannot penetrate even the thinnest layers of fabric or paper.17 Tape or other tightly woven material placed over crevices known to harbor bedbugs can effectively prevent their mobility.17 Bedbugs are not able to move on surfaces with low-friction covering, so covering bedposts with petroleum jelly or paraffin oil has been suggested.18,19 Treating Infestations Infestations can be identified by small specks of bedbug remnants, including their feces and blood from their hosts and cast skins left behind on bed linens when the bedbugs molt. 20 However, bedbugs are often difficult to locate. Trained detector dogs have been used to identify them based on smell. The services of these dogs are available commercially; the dogs’ detection abilities have a remarkable 97.5% positive indication rate and 0% false positives). 21 Once bedbugs are identified, patients should launder all their bed linens and vacuum their furniture to reduce the number of bedbugs within the household. 22 Professional exterminators should be consulted, as should management personnel in shared housing, with the understanding that the entire dwelling (and adjacent structures), not just the bed, must be treated. Chemical and nonchemical approaches can then be implemented to rid the area of these insects. The chemical approach 144 Lab Medicine Summer 2012 | Volume 43, Number 5 is a challenge because bedbugs are increasingly resistant to pesticides in current use 4 and there are no effective repellents for these insects, to our knowledge. Dichlorodiphenyltrichloroethane (DDT) was used against bedbugs in the 1970s as less toxic alternatives used at that time were not as effective in eliminating those insects. Mosquito repellent and eucalyptus oils have been suggested; however, their use against bedbugs has not been effective.11 Fumigants do not penetrate deeply enough into the hiding places of bedbugs; further, their use can harm humans. Typical bug sprays that kill cockroaches immediately also kill bedbugs; it is recommended that these chemicals be sprayed directly on infected areas for instant results.4 In spite of these measures, bedbug infestations can continue. Nonchemical solutions such as vacuuming, heat treatments, freezing, and laundering infested articles23 have yielded the best bedbug-eradication results. Vacuuming the infected area with a device that contains a high-efficiency air filter removes bedbug debris and allergens; however, bedbug eggs almost always remain because they are affixed tightly onto surfaces by means of a glue-like substance produced by the mother’s body.17 Heat treatments are used as alternatives to insecticides and should be applied by a professional exterminator. With the proper equipment, it is possible to heat rooms to temperatures lethal to bedbugs: this insect, at all stages of its growth, dies when exposed to temperatures equal to or exceeding 50°C (122°F) for at least 90 minutes. Laundering the affected clothing or linens should be performed on the hottest possible washer and dryer settings and at the highest possible temperature the particular fabrics can withstand. This procedure can easily kill the bedbugs, making it unnecessary to discard clothing and linens; however, it does not prevent further infestations. Freezing the affected items is only effective in cases of limited infestation; items must be frozen for 4 days.17,23 Heating and freezing kits are used by professional exterminators; however, many individuals cannot afford the $500 to $1500 cost to hire such professionals.24 If chemical or nonchemical methods do not work, furniture, clothing, and linen from the affected area must be removed and replaced. For many, this is a last resort due to cost, although it ensures that bedbug clusters are eliminated from the home. www.labmedicine.com Overview Psychological Effects Bedbugs cause more than physical harm to their human victims, who may develop psychological complications from bedbug infestations. These infestations can lead to psychosocial stress affecting daily life and can lead to constant worrying, self-isolation, and management tactics that interrupt daily life.25 Physical marks left by bedbugs can cause individuals to feel insecure and can lower their self-esteem, especially when the bites are located on the face or neck. Because exposed bites are plainly visible, employment performance can also be affected.25 Some individuals may worry constantly about bedbugs even when the insects have been successfully eradicated from the home; some individuals develop delusions that they feel bedbugs crawling on their skin.40 Self-isolation is very common because those with bedbug bites avoid other people and, in turn, they are avoided by the members of their community.25 Harboring a bedbug infestation is seen as a sign of poor hygiene; this stigma is the primary reason for avoidance.25 Also, individuals experience mental trauma from the expense of bedbug eradication: having to pay hundreds, even thousands, of dollars to properly eliminate those insects can be difficult to accept.25 As a result, individuals may experience mild to severe levels of stress, depression, and anxiety, all of which may require treatment.25,26 Bedbugs as Vectors for Infectious Disease: An Unproven (But Warranted) Hypothesis Bedbugs feeding on human blood are exposed to all the pathogens found therein. Arthropod-borne viruses (ie, arboviruses), Lyme disease, and West Nile virus are the most recent examples of diseases that are transmitted by insects between individuals in the United States. However, throughout history, humankind has been plagued by diseases spread by insect vectors, such as malaria (Plasmodium species [spp]), leishmaniasis (Leishmania spp), and Chagas disease (Trypanosoma cruzi). As a result, there has been concern that bedbugs can and do harbor some of the most burdensome infectious diseases known in the developed world. www.labmedicine.com More than 40 pathogens have been suspected of being transmitted via C. lectularius or C. hemipterus.4 However, no reported cases, to our knowledge, display evidence that any of these infectious diseases have been passed to humans.25 The evidence that these pathogens found in the Cimex spp. is incomplete; the causal relationship between vector and disease has not been proven. To prove that an insect transmits disease (ie, that it acts as a vector), it must first be shown that the arthropod can harbor the disease and pass it to another host. To date, no evidence has been reported that any of these 40 or more potential pathogens are passed to humans by bedbugs. The most studied and/or strongest candidates for transmission by bedbugs have recently been reviewed;4 they include Coxiella burnetii (ie, Q fever), Wolbachia spp. (ie, Anaplasmataceae bacteria-obligate bacterial species), Aspergillus spp. (ie, mold) and bacteria (ie, Staphylococcus spp. and Enterobacter spp.),4 Trypanosoma cruzi (ie, Chagas disease), hepatitis B virus (HBV), and human immunodeficiency virus (HIV). C. burnetii has been reported to persist in bedbugs for as long as 250 days without loss of pathogenic potential it is excreted in bedbug feces.27,28 The potential to transmit these pathogens to humans requires further investigation. Wolbachia spp. have been detected in most C. lectularius; transovarial transmission to future generations has been established4 but its ability to spread to humans is unknown. Like most insects, bedbugs can passively transmit mold, such as the Aspergillus spp.; also, 9 bacterial and fungal spp. have been found in the male intromittent organs.1 However, an epidemiologic role in transmission has not been established. When bedbugs were allowed to feed on blood from infected patients with high titers of HBV and hepatitis C virus (HCV), HBV DNA was found in those bedbugs as long as 6 weeks after their feedings. However, HCV RNA was not present in the feces of those bedbugs at any time after feeding, as assayed by polymerase chain reaction (PCR)29; this suggests that HBV has the potential to be passed to humans. Although the HBV pathogen is found in bedbug feces, additional studies must be performed to demonstrate that the bedbug can successfully transmit this virus to its host (ie, to prove its vector competence).11 In a separate study5 conducted in Gambia, spraying insecticide in children’s bedrooms reduced the presence of bedbugs but it had no effect on HBV infection rates, which suggests no correlation between bedbugs and HBV Summer 2012 | Volume 43, Number 5 Lab Medicine 145 Overview A B C Image 2 Locations where bedbugs hide. Being small but visible, bedbugs often hide in furniture (A, B) and luggage (C). From Bedbugs Detroit Extermination and Pest Control Web page. http://www.bedbugsdetroit.com/bed-bugs-news. Accessed June 28, 2011. infections in children. Lastly, HIV has not been identified in bedbugs, although experimental feeding with HIV-tainted blood identified that the virus could survive for 8 days in bodies of these insects.11 Replication and transmission of HIV to laboratory animals has not been possible, despite using high titers of the virus.11 Therefore, HIV is not likely a candidate pathogen for bedbug transmission. So far, bedbugs have not been shown to transmit any of the diseases mentioned in this paragraph to human hosts, despite evidence for their presence in bedbug feces. The Return of Bedbugs to the Developed World In industrialized countries, bedbug infestation decreased throughout the end of the 20th century due to improvements in insecticide effectiveness and in household and personal hygiene.30-33 However, infestations began to reappear in the late 1990s (ie, approximately 1996) due to the use of less-effective insecticides and increased international travel.31,33-35 Organophosphates, including DDT, were banned in the late 1970s and were followed by the introduction of less-toxic alternatives.36 The limited effectiveness of these insecticides was due to the fact that they did not persist to the degree necessary to kill the insects, especially in the crevices and cracks where bedbugs were most likely to hide.31 Also, bedbugs have been reported to be resistant to new insecticides such as pyrethroids (eg, λ-cyhalothrin and deltamethrin) and chlorfenapyr.35 In Denmark, for example, bedbugs have widespread resistance to permethrin and deltamethrin (ie, pyrethroids) and a reduced sensitivity to 146 Lab Medicine Summer 2012 | Volume 43, Number 5 chlorpyrifos,2 which limits the arsenal against these insects. Resistance to pyrethroids may occur due to mutations in voltage-gated sodium channels, which have been reported in multiple insect species.37,38 Despite the decline in bedbug infestations in the developed world during most of the latter 20th century, bedbug prevalence did not decline in less-developed countries; in fact, bedbug incidence thrived.33 Because bedbugs are particularly adept at hitching rides on humans via luggage or clothing, increased travel has brought bedbugs back to the more inviting environment in developed countries in the 21st century.30-33 It is possible that much of the increase in bedbug infestation we now observe results from the reintroduction of those insects into certain environments and is not necessarily a sign of the fitness of bedbugs over time. Preventing Future Bedbug Infestations With mounting evidence that travel is one of the primary ways in which humans are exposed to bedbugs, some suggestions to help individuals avoid being unintended vehicles for these insects are warranted. Bedbugs attach themselves to clothing during travel and can be found in hotel rooms, among other public areas, allowing them to make their way back to the homes of their hosts (Image 2). It is suggested that when traveling, individuals should inspect their hotel rooms before unpacking and should put their luggage in the bathroom because bedbugs do not frequent that room. An inspection of the mattress and the headboard may help determine the presence of bedbugs. Also, sheets should be turned www.labmedicine.com Overview down to check for bedbug remnants such as blood and feces. Closets and dressers should be inspected thoroughly with a flashlight before storing any clothing within. Luggage should never be placed on the floor of the hotel room; instead, travelers should use the luggage racks provided or use tabletops located away from the walls. On leaving the hotel room, all clothing that requires laundering should be placed in a tightly closed plastic bag, so that any possible bedbugs are contained within. Once travelers return home, they should wash their clothing and thoroughly examine their suitcases. If bedbugs are found on or in suitcases, those items must be scrubbed with boiling hot water.39 Signs of bedbugs, especially fecal stains, can be seen in buses, cars, and taxis. Bags should be kept on one’s lap if possible, avoiding the trunk or storage compartments. Bedbugproof luggage liners and laundry bags may be used by those who travel frequently; it is always a good idea to check one’s clothing and skin for bedbugs and their by-products after exiting a vehicle. bedbugs are here to stay, and the problems they cause will likely get worse. However their threats to people’s health is limited to their ability to be a nuisance not a disease vector. LM Additional Resources 1. Bedbugs. National Geographic Channel. Available at: www.youtube. com/watch?v=WfKCcSPCOQo. 2. Centers for Disease Control. Bedbug resource page. Available at: www.cdc.gov/nceh/ehs/topics/bedbugs.htm. To read this article online, scan the QR code. References 1. Reinhardt K, Siva-Jothy MT. Biology of the bed bugs (Cimicidae). Annu Rev Entomol. 2007;52:351-374. QR code generated on http://qrcode.littleidiot.be Summary Bedbug infestations of human habitats in the United States have become increasingly common during the past decade. The saliva components of these nocturnal blood feeders produce variable skin reaction responses in humans, in much the same manner as the saliva components of mosquitoes. These reactions may manifest as erythematous rashes, urticarial eruptions, or wheals, all accompanied by pruritus (ie, itching). As many as 45 infectious diseases have been suspected of being transmitted by bedbugs (many of which had been found living in those insects for some time); these diseases can be passed via bedbug feces. However, to date, actual transmission of any infection has not been proven. Treatment to counteract bedbug infestation involves symptomatic therapy and elimination of the infestation, the latter of which can be challenging. Because bedbugs can be found almost anywhere humans dwell, including homes, offices, hotels, and hospitals, specific precautions can be taken when traveling to prevent bedbug infestations, including early identification of such infestations and protection of clothing and luggage from potential contact with bedbugs and their by-products. Given increased international travel, the use of inferior pesticides, and the growing resistance of bedbugs to available pesticides, www.labmedicine.com 2. Kilpinen O, Jensen KM, Kristensen M. In: Robinson WH, ed. Proceedings of the Sixth International Conference on Urban Pests. Budapest, Hungary: OOK Press; 2008:395-399. 3. Huntley AC. Cimex lectularius. What is this insect and how does it affect man? Dermatol Online J. 1999;5:6. 4. Delaunay P, Blanc V, Del Giudice P, et al. Bedbugs and infectious diseases. Clin Infect Dis. 2011;52:200-210. 5. Walpole DE, Newberry K. A field study of mating between two species of bedbug in northern KwaZulu, South Africa. Med Vet Entomol. 1988;2:293-296. 6. Kells SA. Bed bugs: A systemic pest within society. Am Entomol. 2006;52:107-108. 7. Bryks S. The bed bug dilemma [letter to the editor]. J Environ Health. 2010;73:48. 8. Gbakima AA, Terry BC, Kanja F, et al. High prevalence of bedbugs Cimex hemipterus and Cimex lectularis in camps for internally displaced persons in Freetown, Sierra Leone: A pilot humanitarian investigation. West Afr J Med. 2002;21:268-271. 9. Ter Poorten MC, Prose NS. The return of the common bedbug. Pediatr Dermatol. 2005;22:183-187. 10.Montes C, Cuadrillero C, Vilella D. Maintenance of a laboratory colony of Cimex lectularius (Hemiptera: Cimicidae) using an artificial feeding technique. J Med Entomol. 2002;39:675-679. 11. Goddard J, deShazo R. Bed bugs (Cimex lectularius) and clinical consequences of their bites. JAMA. 2009;301:1358-1366. 12. Valenzuela JG, Walker FA, Ribeiro JMC. A salivary nitrophorin (nitricoxide-carrying hemoprotein) in the bedbug Cimex lectularius. J Exp Biol. 1995;198(Pt 7):1519-1526. 13.Wilson KM. They only come out at night: Bed bugs and their alarming resurgence. Nursing. 2011;41:54-58. 14. Feldlaufer MF, Domingue MJ, Chauhan KR, et al. 4-Oxo-aldehydes from the dorsal abdominal glands of the bed bug (Hemiptera: Cimicidae). J Med Entomol. 2010;47:140-143. 15.Benac N. Bedbug bites becoming bigger battle. CMAJ. 2010;182:1606. 16.Easing bedbug anxiety. What you need to know about the recent bedbug resurgence. Harv Womens Health Watch. 2011;18:7. 17. Kolb A, Needham GR, Neyman KM, et al. Bedbugs. Dermatol Ther. 2009;22:347-352. Summer 2012 | Volume 43, Number 5 Lab Medicine 147 Overview 18.Thomas I, Kihiczak GG, Schwartz RA. Bedbug bites: A review. Int J Dermatol. 2004;43:430-433. 30.Paul J, Bates J. Is infestation with the common bedbug increasing? BMJ. 2000;320:1141. 19.Crissey JT. Bedbugs: An old problem with a new dimension. Int J Dermatol. 1981;20:411-414. 31. Anderson AL, Leffler K. Bedbug infestations in the news: A picture of an emerging public health problem in the United States. J Environ Health. 2008;70:24-27, 52-23. 20.Cleary CJ, Buchanan D. Diagnosis and management of bedbugs: An emerging U.S. Infestation. Nurse Pract. 2004;29:46-48. 32.Masetti M, Bruschi F. Bedbug infestations recorded in Central Italy. Parasitol Int. 2007;56:81-83. 21. Pfiester M, Koehler PG, Pereira RM. Ability of bed bug-detecting canines to locate live bed bugs and viable bed bug eggs. J Econ Entomol. 2008;101:1389-1396. 33.Boase C. Bed bugs: Back from the brink. Pestic Outlook. 2001;12:159-162. 22.Leininger-Hogan S. Bedbugs in the intensive care unit. A risk you cannot afford. Crit Care Nurs Q. 2011;34:150-153. 34.Romero A, Potter MF, Potter DA, et al. Insecticide resistance in the bed bug: A factor in the pest’s sudden resurgence? J Med Entomol. 2007;44:175-178. 23.Elston DM, Kells S. Bedbugs. UpToDate 2011 Web site. Available at http://www.uptodate.com/contents/bedbugs. Accessed May 27, 2011. 35.Moore DJ, Miller DM. Laboratory evaluations of insecticide product efficacy for control of Cimex lectularius. J Econ Entomol. 2006;99:2080-2086. 24.Manuel J. Invasion of the bedbugs. Environ Health Perspect. 2010;118:A429. 25.Doggett SL, Russell R. Bed bugs: What the GP needs to know. Aust Fam Physician. 2009;38:880-884. 36.Gubler DJ. Vector-borne diseases. Rev Sci Tech. 2009;28:583-588. 26.Jacobs A. Just try to sleep tight: the bedbugs are back. The New York Times. November 27, 2005:A1. 37. Burton MJ, Mellor IR, Duce IR, et al. Differential resistance of insect sodium channels with kdr mutations to deltamethrin, permethrin and DDT. Insect Biochem Mol Biol. 2011;41:723-732. 27. Daiter AB. Experimental infection of arthropods with human Q fever [in Russian]. Tr Leningr Inst Epidemiol Mikrobiol. 1963;25:92-100. 38.Soderlund DM. Pyrethroids, knockdown resistance and sodium channels. Pest Manag Sci. 2008;64:610-616. 28.Daiter AB. The bedbug as a possible reservoir of Rickettsia bumetii (experimental and epidemiological data) [in Russian]. Vopr Virusol. 1960;6:591-598. 39.Chalupka S. Preventing bedbug infestation. AAOHN J. 2010;58:500. 40.Vandam J. Sleep tight, and don’t let...Oh, just forget about it. New York Times. 2003. Available at: www.nytimes.com/2003/11/02/ nyregion/neighborhood-report-greenpoint-sleep-tight-and-don-t-letoh-just-forget-about-it.html. 29.Silverman AL, Qu LH, Blow J, et al. Assessment of hepatitis B virus DNA and hepatitis C virus RNA in the common bedbug (Cimex lectularius L.) and kissing bug (Rodnius prolixus). Am J Gastroenterol. 2001;96:2194-2198. CELEBRATING OUR DIAMOND ANNIVERSARY Earn up to 52 CME/CMLE/SAM credits REGISTER EARLY AND SAVE NOVEMBER 2-6, 2012 ◆ BALLY’S LAS VEGAS Plus, ASC members save up to 60% more! cytopathologymeeting.org American Society of Cytopathology 100 West 10th Street, Suite 605 ■ Wilmington, DE 19801 Phone: (302) 543-6583 ■ Fax: (302) 543-6597 Email: [email protected] Experience everything this meeting has to offer. Education. Credits. Perspective. Interaction. Fun. With a combination of returning favorites and new additions, this will be the best meeting experience to date — you don’t want to miss it! New this year… ■ ■ ■ ■ ■ ■ ■ Hot Topic: ASC Workload Recommendations Half-day Thyroid Ultrasound Guided FNA Career Planning and Growth Cytohistology Workshops 60th Anniversary Celebration ■ ■ ■ ■ ■ Plus more events… Scientific Sessions include… ■ ■ ■ ■ 148 Platform and Poster Presentations State of the Society Address Papanicolaou Address Current Issues in Cytology Guest Lecture State of the Art Symposium Innovation & Trends in Medicine Leopold Koss Lectureship Diagnostic Cytology Seminar Gathering for 1st Time Attendees ASC President’s Welcome Reception Lab Medicine Summer 2012 | Volume 43, Number 5 ■ ■ ■ ■ ■ ■ ■ ■ ■ ■ Strategies in Cytology Education Lunch with the Presidents Challenges in Diagnostic Cytomorphology Video Microscopy Tutorials Workshops Panel Luncheon Seminars Roundtable Discussions Presidents’ Rounds Award Presentations Scientific and Technical Exhibits Continuing Medical Education (CME): The American Society of Cytopathology is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. AMA Physician’s Recognition Award: The American Society of Cytopathology designates this educational activity for a maximum of 52 AMA PRA Category 1 credits.™ Physicians should only claim credit commensurate with the extent of their participation in the activity. Continuing Medical Laboratory Education (CMLE): The ASC designates these activities for a maximum of 52 Continuing Medical Laboratory Education (CMLE) credit hours. The CMLE credit hours meet the continuing education requirements for the ASCP Board of Registry Certification Maintenance Program. This program is also approved for continuing education credits in the State of Florida and the State of California. American Board of Pathology Maintenance of Certification (MOC): The 60th Annual Scientific Meeting will have up to 90 courses available to help fulfill the CME requirements mandated by the American Board of Pathology Maintenance of Certification (MOC) process. Self-Assessment Modules (SAMs): The 60th Annual Scientific Meeting will offer 52 additional sessions (maximum of 36.75 credits) requiring completion of (SAM) to test knowledge. The two “Challenges in Diagnostic Cytomorphology” sessions, all Video Microscopy Tutorials, Workshops, Panel Luncheon Seminars and select Scientific Sessions qualify for SAMs. 12-0691 www.labmedicine.com