Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
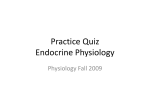
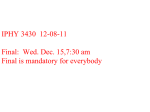
ARTHRITIS & RHEUMATISM Vol. 46, No. 5, May 2002, pp 1344–1350 DOI 10.1002/art.10209 © 2002, American College of Rheumatology Impaired Growth Hormone Secretion in Fibromyalgia Patients Evidence for Augmented Hypothalamic Somatostatin Tone Eduardo S. Paiva, Atul Deodhar, Kim D. Jones, and Robert Bennett Objective. To determine whether female fibromyalgia (FM) patients exhibit a normal growth hormone (GH) response to an acute exercise stressor, and to assess the importance of somatostatin tone in the generation of this GH response. Methods. Twenty female FM patients were compared with 10 healthy female controls. All subjects exercised to volitional exhaustion on a treadmill. A standard metabolic cart was used to monitor pulse, blood pressure, electrocardiography, oxygen uptake, carbon dioxide output, anaerobic threshold, and maximal workload. Blood was drawn for GH and cortisol measurements 1 hour before exercise, immediately before exercise, immediately after exercise, and 1 hour after exercise. One month later, testing that was exactly similar was performed, except all subjects were given pyridostigmine bromide (Mestinon; 30 mg orally) 1 hour before exercise. Results. Compared with controls, FM patients failed to exhibit a GH or cortisol response to acute exercise (P ⴝ 0.003). After administration of pyridostigmine, 1 hour before exercise, the GH levels of FM patients increased 8-fold (P ⴝ 0.001), to a value comparable with that of controls. Pyridostigmine did not increase the cortisol response to exercise in FM patients. Pyridostigmine alone did not stimulate GH secretion in FM patients, nor did it improve exerciseinduced GH secretion in controls. FM patients with normal insulin-like growth factor 1 (IGF-1) levels had an impaired GH response to exercise. Conclusion. Three new findings are reported: 1) FM patients have a reduced GH response to exercise, 2) pyridostigmine reverses this impaired response, and 3) defective GH secretion in FM can occur in patients with normal IGF-1 levels. Because pyridostigmine is known to reduce somatostatin tone, it is surmised that the defective GH response to exercise in FM patients probably results from increased levels of somatostatin, a hypothalamic hormone that inhibits GH secretion. Fibromyalgia (FM) is a common clinical syndrome characterized by widespread musculoskeletal pain, with a high prevalence both in the general population and among patients attending rheumatology clinics (1–4). Increasing evidence implicates a perturbation in the central mechanisms of sensory processing as being relevant to understanding the pain component of FM (5–7). Fibromyalgia is more than a state of chronic musculoskeletal pain, however, because most FM patients also experience fatigue, poor sleep, visceral pain (e.g., irritable bowel or bladder), exercise intolerance, and neurologic symptoms (e.g., dizziness, numbness, tingling) (8). A theoretical model explaining the complexity of FM symptoms has been proposed, which links dysregulation of neuroendocrine/stress/pain mechanisms to disordered sleep–wake physiology (5). This evolving paradigm promotes the notion that FM is a stress-related syndrome, in which a disordered hypothalamic– pituitary–adrenal (HPA) axis acts as a final common pathway linking FM to other stress-related somatic and psychiatric syndromes (7,9,10). The HPA and the HP– growth hormone (GH) axis are closely linked in terms of the opposing influences of corticotropin-releasing hormone and somatostatin on GH secretion (11). Defective GH secretion in FM was initially surmised based on the finding of low levels of insulin-like growth factor 1 (IGF-1; somatomedin C) in a subset of Supported by USPHS grant 5-M01-RR-00334. Eduardo S. Paiva, MD, Atul Deodhar, MD, MRCP, Kim D. Jones, PhD, RN, Robert Bennett, MD, FRCP: Oregon Health Sciences University, Portland. Address correspondence and reprint requests to Robert M. Bennett, MD, Department of Medicine (OP09), Oregon Health Sciences University, Portland, OR 97201. Submitted for publication June 5, 2001; accepted in revised form December 5, 2001. 1344 GH RESPONSE TO EXERCISE IN FEMALE FM PATIENTS FM patients (12–14). It was originally hypothesized that GH production in FM patients would be impaired because such production occurs predominantly during stages 3 and 4 of non–rapid eye movement sleep (12), which is disrupted in many FM patients (15). In the current study, the hypothesis was that an increased level of somatostatin is related to impaired GH secretion in FM patients. To test this hypothesis, the exercisestimulated GH response in female FM patients and healthy controls was evaluated both before and after administration of pyridostigmine (a potent cholinergic agent). The rationale for this pharmacologic manipulation was the observation that increased cholinergic activity stimulates GH release by inhibiting hypothalamic somatostatin tone (16). Thus, an improvement in exercise-stimulated GH secretion after administration of pyridostigmine would suggest that FM patients have increased hypothalamic somatostatin tone. SUBJECTS AND METHODS Twenty women with a diagnosis of FM based on the 1990 American College of Rheumatology criteria (3) were recruited from a database of FM patients at Oregon Health Sciences University (OHSU). All patients were 18–60 years of age and were assessed for the following exclusion criteria: angina, uncontrolled hypertension, chronic obstructive pulmonary disease, hypothyroidism, severe depression, previous pituitary disease or surgery, and pregnancy. Using the same exclusion criteria, 10 healthy women were selected as controls. Other than sex, there were no specific selection criteria for either group. All subjects gave informed consent, and the OHSU review board approved the study. Each subject underwent a treadmill test, using the modified Balke protocol (17). They exercised to the point of volitional exhaustion, which was defined when either of 2 goals was reached: 1) respiratory rate (RR) index (anaerobic threshold) of 1.0, indicative of anaerobic metabolism, or 2) exhaustion (Borg) scale value of 10 (maximum perceived effort). Electrocardiography and blood pressure monitoring were performed every 5 minutes. All testing was performed between 10:00 AM and 2:00 PM. Blood was collected through an indwelling catheter 1 hour before exercise, immediately before exercise (time 0), immediately after exercise, and 1 hour after the end of exercise. GH and cortisol levels were measured at each time point. IGF-1 levels were measured 1 hour before the first treadmill test. Subjects were given a second treadmill test within at least 1 month of the first test. This second test was identical to the first, except all subjects were given 30 mg orally of pyridostigmine bromide (Mestinon) 1 hour before exercise. IGF-1 was measured by immunoradiometric assay (Diagnostic Systems Laboratories, Webster, TX). The sensitivity of this assay is 0.80 ng/ml; the mean intra-assay coefficient of variation (CV) is 2.6%, and the mean inter-assay CV is 4.5%. Human GH was measured by a noncompetitive chemiluminescence assay (Diagnostic Products, Los Angeles, CA). Sensitivity of this assay is 0.01 ng/ml; the mean intra-assay CV 1345 Table 1. Baseline characteristics of the patients and controls* Age, years Weight, kg Body mass index VO2max, ml/kg/minute RER at VO2max Total exercise work, watts IGF-1, ng/ml Resting GH, ng/ml Resting cortisol, ng/ml % pre/postmenopausal % taking HRT Fibromyalgia (n ⫽ 21) Controls (n ⫽ 10) 44.6 ⫾ 8.2 80.8 ⫾ 16† 29.05 ⫾ 5.3 18.6 ⫾ 4.8 1.20 ⫾ 0.11 144 ⫾ 51 189 ⫾ 83 0.66 ⫾ 2.1 7.7 ⫾ 3.3 52/48 30 47.0 ⫾ 47 68.3 ⫾ 13 25.9 ⫾ 4.6 18.7 ⫾ 4.4 1.18 ⫾ 0.06 138 ⫾ 36 170.8 ⫾ 50 0.74 ⫾ 1.49 8.6 ⫾ 3.0 62/38 25 * Unless indicated otherwise, values are the mean ⫾ SD. VO2max ⫽ maximum volume of oxygen utilization; RER ⫽ respiratory exchange ratio; IGF-1 ⫽ insulin-like growth factor 1; GH ⫽ growth hormone; HRT ⫽ hormone replacement therapy. † P ⫽ 0.043 versus controls. is 6.0%, and the mean inter-assay CV is 5.8%. Cortisol was measured by a competitive chemiluminescence assay (Nichols Institute Diagnostics, San Juan Capristano, CA). Sensitivity of this assay is 0.80 ng/ml; the mean intra-assay CV is 4.2%, and the mean inter-assay CV is 7.9%. Statistical analysis was performed with SigmaStat software (1995; Jandel Corporation, San Rafael, CA). Mean changes were compared using a t-test or Mann-Whitney rank sum test. Within-group changes were compared with a paired t-test or Wilcoxon’s signed rank test. Categorical data were analyzed using a 2 ⫻ 2 contingency table with Fisher’s exact test (because some values were ⬍5). All analyses of significance used a 2-tail distribution. RESULTS Baseline characteristics of the FM patients and controls (Table 1) were comparable, except the mean weight of FM patients was 12.5 kg greater than that of controls (P ⫽ 0.043). However, there was no significant difference in body mass index (BMI) between the 2 groups. All participants were able to reach an anaerobic threshold at maximal exertion. There was no difference in the maximal mean values of respiratory exchange ratio, workload, or oxygen uptake (VO2max) between FM patients and controls. The mean IGF-1 and resting GH levels were not significantly different between the 2 groups. After exercising to volitional exhaustion, the healthy controls exhibited an increase in GH, from a mean ⫾ SD of 0.74 ⫾ 1.49 ng/ml before exercise to a mean ⫾ SD of 6.2 ⫾ 6.1 ng/ml after exercise (P ⫽ 0.003). This increase was not influenced by pyridostigmine (P ⫽ 0.21) (Figure 1). Only 1 control subject did not demonstrate an exercise-induced increase in GH. This subject 1346 had a low IGF-1 level (74 ng/ml), and although she did not have FM, she was presumed to have physiologic GH deficiency, because she exhibited a 40-fold increase in GH after administration of pyridostigmine followed by exercise. Eleven of 20 FM patients exhibited no exerciseinduced increase in GH level. Compared with controls, FM patients had a significantly reduced response to exercise (P ⫽ 0.017 by Fisher’s exact test) (Figure 1). On the whole, FM patients had a very modest exerciseinduced change in GH levels, with a mean ⫾ SD increase of 0.66 ⫾ 2.1 ng/ml at time 0 to a mean ⫾ SD of 1.66 ⫾ 2.75 ng/ml (P ⫽ 0.20) 1 hour after exercise (Figure 2). These results cannot be attributed to the greater mean weight of the FM patients, because there was no correlation between GH response and weight or BMI. However, following administration of pyridostigmine, 19 of 20 FM patients exhibited an exerciseinduced increase in GH. Overall, after administration of pyridostigmine, GH in FM patients increased from a mean ⫾ SD of 0.57 ⫾ 0.82 ng/ml to a mean ⫾ SD of 4.7 ⫾ 3.8 ng/ml (P ⫽ 0.001) (Figure 2). This increase in GH was 8-fold higher than that associated with exercise stimulation without pyridostigmine and was similar to the increase seen in healthy controls. This result cannot be explained by the fact that the FM patients exercised to a greater intensity with the pyridostigmine protocol, because their maximal workload was only slightly increased (mean ⫾ Figure 1. Individual peak growth hormone (GH) responses for the 4 study groups. Each pair of symbols connected by a line represents the values for an individual subject from the immediate preexercise time and the immediate postexercise time. PAIVA ET AL Figure 2. Growth hormone (GH) levels in fibromyalgia (FM) patients after exercise. Exercise alone failed to stimulate GH secretion in FM patients, but administration of pyridostigmine bromide (30 mg orally) 1 hour before exercising normalized release of GH in these patients (P ⫽ 0.005). Values are the mean ⫾ SD. SD 44 ⫾ 51 to 155 ⫾ 33 watts; P ⫽ 0.42), and all achieved an RR index ⱖ1.0. Pyridostigmine without exercise did not stimulate GH secretion after 1 hour (Figure 2). Backward stepwise regression analysis showed no relationship between exercise-induced changes in GH level and weight, BMI, VO2max, age, maximal workload at volitional exhaustion, or resting GH level, in either FM patients or controls. The presence of low levels of IGF-1 at baseline did not predict postexercise levels of GH in either group; this was true regardless of whether the cutoff level for IGF-1 deficiency was age-adjusted or predetermined. Resting cortisol levels were not significantly different between FM patients and controls (Table 1). Cortisol secretion was slightly reduced by exercise in FM patients (mean ⫾ SD 7.7 ⫾ 3.3 ng/ml before and 7.4 ⫾ 3.5 ng/ml after exercise; P ⫽ 0.77). Unlike the HP–GH axis, the HPA axis response to exercise was not influenced by prior administration of pyridostigmine in FM patients (1-hour postexercise value 6.2 ⫾ 3.3 ng/ml with pyridostigmine treatment). Cortisol secretion was modestly increased by exercise in healthy controls (mean ⫾ SD 8.6 ⫾ 3.0 ng/ml before and 10.8 ⫾ 3.8 ng/ml after exercise; P ⫽ 0.17). The postexercise cortisol level was significantly higher in controls compared with FM patients (P ⫽ 0.02). There was no correlation between GH RESPONSE TO EXERCISE IN FEMALE FM PATIENTS postexercise GH levels and cortisol levels, either with or without pyridostigmine. DISCUSSION This study provides 3 new pieces of information: FM patients have a reduced GH response to exercise, this impaired response is reversed by administration of pyridostigmine, and defective GH secretion in FM patients can occur in the setting of a normal IGF-1 level. Studies conducted during the past 10 years have demonstrated conflicting results regarding the serum levels of IGF-1 in FM patients compared with those in control subjects. In 4 studies, low levels of IGF-1 were observed in FM patients (12–14,18), and in 4 other studies, no difference between FM patients and controls was demonstrated (19–22). Furthermore, the current study showed no significant difference in IGF-1 levels between FM patients and controls. The reasons for these conflicting results most probably relate to the number of subjects studied. For instance, Buchwald et al studied 27 FM patients and 15 controls; although there was no significant difference between the mean IGF-1 levels of the 2 groups, ⬃20% of the FM patients had low IGF-1 levels (19). In contrast, investigators at our laboratory compared IGF-1 levels in 500 FM patients and 152 controls (both healthy individuals and patients with other rheumatic diseases) and found a very significant (P ⫽ 0.00000000001) reduction of IGF-1 levels in the FM population (14). Many FM patients studied by the latter group had normal IGF-1 levels, however, and it was concluded that about one-third of FM patients have probable GH deficiency. The fact that the FM population in the current study had mean IGF-1 levels similar to those of controls is not, therefore, surprising, given the fact that we studied only 20 FM patients and 10 controls. Other studies have demonstrated low levels of GH in FM patients (23,24), and reduced GH secretion has been shown in various types of stimulation studies (13,14,24– 26). On balance, the literature to date supports the notion that the HP–GH axis is dysfunctional in a subset of FM patients. GH is the only pituitary hormone that is under the influence of both stimulatory and inhibitory hypothalamic hormones. The normal pulsatile secretion of GH depends on the tonic balance of stimulatory growth hormone–releasing hormone (GHRH) and inhibitory somatostatin (27,28). Under normal circumstances, production of GH occurs only when secretion of GHRH 1347 takes place in the setting of low levels of somatostatin tone. Many studies have shown that cholinergic stimulation with pyridostigmine reduces hypothalamic somatostatin tone, with a resultant up-regulation of GH release (16,29,30). Both physiologic and pharmacologic down-regulation of GH secretion is usually the result of increased somatostatin tone (11). For instance, the age-related decline in stimulated GH secretion is reversed by pyridostigmine (31,32). Exercise-induced stimulation of GH release is also blunted with aging and can be reversed by administration of pyridostigmine (31,33). The low levels of GH found in persons who are morbidly obese are increased by pyridostigmine (34). The depressed GH secretion that occurs as a result of excessive endogenous and exogenous corticosteroids is attributable to increased somatostatin tone and can be partially reversed by pyridostigmine (35). Thus, the results of the current study suggest that hypothalamic somatostatin tone in FM patients is increased compared with that in age- and sex-matched controls. The reason for this is not immediately clear, but it is reasonable to hypothesize that there is a link with the perturbations of the HPA axis that have been reported in FM patients (36–38). According to this scenario, the pleiotropic actions of corticotropinreleasing factor (CRF) are thought to play a major controlling role. CRF is the major mediator of the HPA/sympathetic response to both physical and psychological stressors. Some FM patients have reduced HPA axis responsiveness to stressors in terms of cortisol secretion, even though they have enhanced adrenocorticotropic hormone (ACTH) response to CRF (37,39,40). Increased GH secretion is the normal response to an acute stressor (such as exercise). Thus, it might seem paradoxical that a prolonged stress response could cause impaired GH secretion. However, in his description of the “general adaptation syndrome,” Hans Selye (41) envisaged 3 stages to the stress response: 1) an alarm reaction originates in the brain and spreads to the pituitary, where increased production of ACTH stimulates the adrenal cortex to secrete glucocorticoids and mineralocorticoids; 2) after prolonged exposure to the stressor, a second stage develops during which there is increasing secretion of corticosteroids (this is a regulatory physiologic response promoting survival processes while inhibiting nonessential processes); 3) in the third stage, an “exhaustion” ensues during which there is a progressive decline in the adaptive response and an increasing vulnerability to stress-related pathology. The first 2 stages of the general adaptation syndrome are 1348 mediated by the stress-induced secretion of CRF (42). However, prolonged CRF secretion eventually downregulates the density of CRF-1 receptors in the paraventricular nucleus of hypothalamus (43). Therefore, notwithstanding persistent CRF secretion, the physiologic effects on cortisol secretion ultimately become blunted (42); this is thought to be one mechanism by which the third stage of the general adaptation syndrome is mediated. A second mechanism by which chronic stress is postulated to lead to a dysfunctional endocrine response is up-regulation of somatostatin tone by increased levels of CRF (13). A correlation between defective GH secretion in FM and Selye’s third stage of the general adaptation syndrome is intriguing but speculative. For instance, Neeck and Riedel hypothesized that a stress-induced increase in CRF is the common denominator linking the disturbed HPA axis and reduced GH secretion in FM (36), the critical link being the observation that CRF increases hypothalamic somatostatin tone (44,45). On the other hand, Torpy et al provided some evidence for a chronically reduced hypothalamic CRF tone and hypothesized that low IGF-1 levels in FM are a consequence of reduced GHRH secretion secondary to impaired nonadrenergic input (38). Van Denderen et al reported an impaired adrenergic response to exhaustive exercise in FM patients as well as a deficient cortisol response (as was also shown in this study) (46), thus providing some support for the reduced GHRH hypothesis. The notion that an enhanced hypothalamic somatostatin tone results from increased CRF is not supported by the exaggerated response to CRF that has been reported (37,47). This result would not be expected in the setting of chronic oversecretion of CRF, because, in general, there is a reciprocal relationship between receptor density and the concentration of its cognate ligand. However, the complexity of endocrine regulation in terms of long, short, and ultrashort feedback loops, changes in ligand-binding proteins, induced and inherited changes in receptor density/function, and permissive/ inhibitory effects of interacting hormones (e.g., the potentiation of CRF-induced release of ACTH by vasopressin) does not permit any definitive conclusions to be reached without performance of more sophisticated experiments. There are several examples of human stressrelated disorders other than FM in which patients exhibit evidence of impaired cortisol secretion: chronic pelvic pain syndrome (48), chronic fatigue syndrome (CFS) (49), posttraumatic stress disorder (50), and overtraining syndrome (51). All of these conditions are PAIVA ET AL characterized by an increase in central HPA function with a paradoxical blunting of the adrenal cortisol response. Whether the blunted cortisol response in FM and these other conditions is a manifestation of central changes or a primary adrenal insufficiency is not currently clear, but a preliminary report of a 50% reduction in the size of the adrenal glands in patients with CFS supports the latter explanation (52). Thus, the concept has arisen that FM and some other chronic disorders are characterized by a hypoactive stress response in terms of the HPA axis, GH axis, gonadal axis, and thyroidal axis, together with reduced sympathetic responses (13,36,53–55). This neuroendocrine dysfunction is often considered to be an epiphenomenon in the complex pathophysiology of FM (6,14,36), e.g., a secondary response to the stress of chronic pain and its association with human suffering. This introduces a psycho-physiologic dimension into the understanding of these hormonal perturbations, because environmental and developmental factors interact with genetic susceptibility in modulating an individual’s responses to chronic stressors (39,53,56–58). In the current study, the defective GH secretion in all FM patients, even those with normal IGF-1 levels, was an unexpected finding. However, it is now apparent that although a low level of IGF-1 is usually indicative of adult GH deficiency (59), it is not a very sensitive measure and will miss up to 60% of GH-deficient patients older than age 40 years (60,61). The currently favored test to diagnose adult GH deficiency is the stimulated GH response to a combination of GHRH and an inhibitor of somatostatin tone such as pyridostigmine, arginine, clonidine, or insulin (60). The results of this study indicate that GH deficiency is probably more common in FM patients than was originally reported. Recognition of defective GH secretion in FM patients is of some practical relevance, because GH replacement therapy was shown to benefit FM patients in a 9-month placebo-controlled study (62). It would, therefore, be of interest to determine whether pyridostigmine could be used to provide long-term improvement of growth hormone production in FM patients. REFERENCES 1. Clark P, Burgos-Vargas R, Medina-Palma C, Lavielle P, Marina FF. Prevalence of fibromyalgia in children: a clinical study of Mexican children. J Rheumatol 1998;25:2009–14. 2. White KP, Speechley M, Harth M, Ostbye T. The London Fibromyalgia Epidemiology Study: direct health care costs of fibromyalgia syndrome in London, Canada. J Rheumatol 1999;26: 885–9. GH RESPONSE TO EXERCISE IN FEMALE FM PATIENTS 3. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia: report of the multicenter criteria committee. Arthritis Rheum 1990;33:160–72. 4. Croft P, Rigby AS, Boswell R, Schollum J, Silman A. The prevalence of chronic widespread pain in the general population. J Rheumatol 1993;4:710–3. 5. Pillemer SR, Bradley LA, Crofford LJ, Moldofsky H, Chrousos GP. The neuroscience and endocrinology of fibromyalgia. Arthritis Rheum 1997;40:1928–39. 6. Bennett RM. Emerging concepts in the neurobiology of chronic pain: evidence of abnormal sensory processing in fibromyalgia. Mayo Clin Proc 1999;74:385–98. 7. Weigent DA, Bradley LA, Blalock JE, Alarcon GS. Current concepts in the pathophysiology of abnormal pain perception in fibromyalgia. Am J Med Sci 1998;315:405–12. 8. Clauw DJ. Fibromyalgia: more than just a musculoskeletal disease. Am Fam Physician 1995;52:843–51, 853–4. 9. Crofford LJ. Neuroendocrine abnormalities in fibromyalgia and related disorders. Am J Med Sci 1998;315:359–66. 10. Neeck G. From the fibromyalgia challenge toward a new biopsycho-social model of rheumatic diseases. Z Rheumatol 1998;57 Suppl 2:A13–16. 11. Wehrenberg WB. Neuroendocrine regulation of GH secretion. In: Conn PM, editor. Neuroendocrinology in physiology and medicine. Totowa (NJ): Humana Press; 2000. p. 181–95. 12. Bennett RM, Clark SR, Campbell SM, Burckhardt CS. Low levels of somatomedin C in patients with the fibromyalgia syndrome: a possible link between sleep and muscle pain. Arthritis Rheum 1992;35:1113–6. 13. Riedel W, Layka H, Neeck G. Secretory pattern of GH, TSH, thyroid hormones, ACTH, cortisol, FSH, and LH in patients with fibromyalgia syndrome following systemic injection of the relevant hypothalamic-releasing hormones. Z Rheumatol 1998;57 Suppl 2:81–7. 14. Bennett RM, Cook DM, Clark SR, Burckhardt CS, Campbell SM. Hypothalamic-pituitary-insulin-like growth factor-I axis dysfunction in patients with fibromyalgia. J Rheumatol 1997;24:1384–9. 15. Drewes AM, Gade K, Nielsen KD, Bjerregard K, Taagholt SJ, Svendsen L. Clustering of sleep electroencephalographic patterns in patients with the fibromyalgia syndrome. Br J Rheumatol 1995;34:1151–6. 16. Arvat E, Cappa M, Casanueva FF, Dieguez C, Ghigo E, Nicolosi M, et al. Pyridostigmine potentiates growth hormone (GH)releasing hormone-induced GH release in both men and women. J Clin Endocrinol Metab 1993;76:374–7. 17. Burckhardt CS, Clark SR, Padrick KP. Use of the modified Balke treadmill protocol for determining the aerobic capacity of women with fibromyalgia. Arthritis Care Res 1989;2:165–7. 18. Ferraccioli G, Guerra P, Rizzi V, Baraldo M, Salaffi F, Furlanut M, et al. Somatomedin C (insulin-like growth factor 1) levels decrease during acute changes of stress related hormones: relevance for fibromyalgia. J Rheumatol 1994;21:1332–4. 19. Buchwald D, Umali J, Stene M. Insulin-like growth factor-I (somatomedin C) levels in chronic fatigue syndrome and fibromyalgia. J Rheumatol 1996;23:739–42. 20. Dessein PH, Shipton EA, Joffe BI, Hadebe DP, Stanwix AE, van der Merwe BA. Hyposecretion of adrenal androgens and the relation of serum adrenal steroids, serotonin and insulin-like growth factor-1 to clinical features in women with fibromyalgia. Pain 1999;83:313–9. 21. Jacobsen S, Main K, Danneskiold-Samsoe B, Skakkebaek NE. A controlled study on serum insulin-like growth factor-I and urinary excretion of growth hormone in fibromyalgia. J Rheumatol 1995; 22:1138–40. 22. Landis CA, Lentz MJ, Rothermel J, Riffle SC, Chapman D, Buchwald D, et al. Decreased nocturnal levels of prolactin and 1349 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. growth hormone in women with fibromyalgia. J Clin Endocrinol Metab 2001;86:1672–8. Griep EN, Boersma JW, de Kloet ER. Pituitary release of growth hormone and prolactin in the primary fibromyalgia syndrome. J Rheumatol 1994;21:2125–30. Bagge E, Bengtsson BA, Carlsson L, Carlsson J. Low growth hormone secretion in patients with fibromyalgia: a preliminary report on 10 patients and 10 controls. J Rheumatol 1998;25:145–8. Leal-Cerro A, Povedano J, Astorga R, Gonzalez M, Silva H, Garcia-Pesquera F, et al. The growth hormone (GH)-releasing hormone-GH-insulin-like growth factor-1 axis in patients with fibromyalgia syndrome. J Clin Endocrinol Metab 1999;84: 3378–81. Dinser R, Halama T, Hoffmann A. Stringent endocrinological testing reveals subnormal growth hormone secretion in some patients with fibromyalgia syndrome but rarely severe growth hormone deficiency. J Rheumatol 2000;27:2482–8. Muller EE, Locatelli V, Cocchi D. Neuroendocrine control of growth hormone secretion. Physiol Rev 1999;79:511–607. Hindmarsh PC, Brain CE, Robinson IC, Matthews DR, Brook CG. The interaction of growth hormone releasing hormone and somatostatin in the generation of a GH pulse in man. Clin Endocrinol (Oxf) 1991;35:353–60. Giustina A, Bossoni S, Bodini C, Doga M, Girelli A, Buffoli MG, et al. The role of cholinergic tone in modulating the growth hormone response to growth hormone-releasing hormone in normal man. Metabolism 1991;40:519–23. Ross RJ, Tsagarakis S, Grossman A, Nhagafoong L, Touzel RJ, Rees LH, et al. GH feedback occurs through modulation of hypothalamic somatostatin under cholinergic control: studies with pyridostigmine and GHRH. Clin Endocrinol (Oxf) 1987;27: 727–33. Giusti M, Marini G, Sessarego P, Peluffo F, Valenti S, Caratti C, et al. Growth hormone secretion in aging: effect of pyridostigmine on growth hormone responsiveness to growth hormone-releasing hormone. Recenti Prog Med 1991;82:665–8. Ghigo E, Goffi S, Arvat E, Nicolosi M, Procopio M, Bellone J, et al. Pyridostigmine partially restores the GH responsiveness to GHRH in normal aging. Acta Endocrinol (Copenh) 1990;123: 169–73. Cappa M, Grossi A, Benedetti S, Drago F, Loche S, Ghigo E. Effect of the enhancement of the cholinergic tone by pyridostigmine on the exercise-induced growth hormone release in man. J Endocrinol Invest 1993;16:421–4. Scacchi M, Pincelli AI, Cavagnini F. Growth hormone in obesity. Int J Obes Relat Metab Disord 1999;23:260–71. Trainer PJ, Kirk JM, Savage MO, Grossman AB, Besser GM. Pyridostigmine partially reverses dexamethasone-induced inhibition of the growth hormone response to growth hormone-releasing hormone. J Endocrinol 1992;134:513–17. Neeck G, Riedel W. Hormonal pertubations in fibromyalgia syndrome. Ann N Y Acad Sci 1999;876:325–38. Crofford LJ, Engleberg NC, Demitrack MA. Neurohormonal perturbations in fibromyalgia. Baillieres Clin Rheumatol 1996;10: 365–78. Torpy DJ, Papanicolaou DA, Lotsikas AJ, Wilder RL, Chrousos GP, Pillemer SR. Responses of the sympathetic nervous system and the hypothalamic–pituitary–adrenal axis to interleukin-6: a pilot study in fibromyalgia. Arthritis Rheum 2000;43:872–80. Demitrack MA, Crofford LJ. Evidence for and pathophysiologic implications of hypothalamic-pituitary-adrenal axis dysregulation in fibromyalgia and chronic fatigue syndrome. Ann N Y Acad Sci 1998;840:684–97. Griep EN, Boersma JW, Lentjes EG, Prins AP, van der Korst JK, de Kloet ER. Function of the hypothalamic-pituitary-adrenal axis in patients with fibromyalgia and low back pain. J Rheumatol 1998;25:1374–81. 1350 41. Selye H. A syndrome produced by diverse nocuous agents. J Neuropsychiatry Clin Neuroscience 1936;10:230–1. 42. Hauger RL. Regulation of the stress response by corticotropinreleasing factor receptors. In: Conn PM, editor. Neuroendocrinology in physiology and medicine. Totowa (NJ): Humana Press; 2000. p. 261–86. 43. Bonaz B, Rivest S. Effect of a chronic stress on CRF neuronal activity and expression of its type 1 receptor in the rat brain. Am J Physiol 1998;275(5 Pt 2):R1438–R1449. 44. Katakami H, Arimura A, Frohman LA. Involvement of hypothalamic somatostatin in the suppression of growth hormone secretion by central corticotropin-releasing factor in conscious male rats. Neuroendocrinology 1985;41:390–3. 45. Rivier C, Vale W. Involvement of corticotropin-releasing factor and somatostatin in stress-induced inhibition of growth hormone secretion in the rat. Endocrinology 1985;117:2478–82. 46. Van Denderen JC, Boersma JW, Zeinstra P, Hollander AP, van Neerbos BR. Physiological effects of exhaustive physical exercise in primary fibromyalgia syndrome (PFS): is PFS a disorder of neuroendocrine reactivity? Scand J Rheumatol 1992;21:35–7. 47. Griep EN, Boersma JW, de Kloet ER. Altered reactivity of the hypothalamic-pituitary-adrenal axis in the primary fibromyalgia syndrome. J Rheumatol 1993;20:469–74. 48. Heim C, Ehlert U, Hanker JP, Hellhammer DH. Abuse-related posttraumatic stress disorder and alterations of the hypothalamicpituitary-adrenal axis in women with chronic pelvic pain. Psychosom Med 1998;60:309–18. 49. Demitrack MA, Dale JK, Straus SE, Laue L, Listwak SJ, Kruesi MJP, et al. Evidence for impaired activation of the hypothalamicpituitary-adrenal axis in patients with chronic fatigue syndrome. J Clin Endocrinol Metab 1991;73:1224–34. 50. Heim C, Ehlert U, Hanker JP, Hellhammer DH. Psychological and endocrine correlates of chronic pelvic pain associated with adhesions. J Psychosom Obstet Gynaecol 1999;20:11–20. 51. Wittert GA, Livesey JH, Espiner EA, Donald RA. Adaptation of the hypothalamopituitary adrenal axis to chronic exercise stress in humans. Med Sci Sports Exerc 1996;28:1015–9. PAIVA ET AL 52. Scott LV, Teh J, Reznek R, Martin A, Sohaib A, Dinan TG. Small adrenal glands in chronic fatigue syndrome: a preliminary computer tomography study. Psychoneuroendocrinology 1999;24: 759–68. 53. Clauw DJ, Chrousos GP. Chronic pain and fatigue syndromes: overlapping clinical and neuroendocrine features and potential pathogenic mechanisms. Neuroimmunomodulation 1997;4: 134–53. 54. Dessein PH, Shipton EA, Stanwix AE, Joffe BI. Neuroendocrine deficiency-mediated development and persistence of pain in fibromyalgia: a promising paradigm? Pain 2000;86:213–15. 55. Neeck G, Riedel W. Thyroid function in patients with fibromyalgia syndrome. J Rheumatol 1992;19:1120–2. 56. Winfield JB. Pain in fibromyalgia. Rheum Dis Clin North Am 1999;25:55–79. 57. Dorn LD, Chrousos GP. The neurobiology of stress: understanding regulation of affect during female biological transitions. Semin Reprod Endocrinol 1997;15:19–35. 58. Clauw DJ. The pathogenesis of chronic pain and fatigue syndromes, with special reference to fibromyalgia. Med Hypotheses 1995;44:369–78. 59. Aimaretti G, Corneli G, Razzore P, Bellone S, Baffoni C, Bellone J, et al. Usefulness of IGF-I assay for the diagnosis of GH deficiency in adults. J Endocrinol Invest 1998;21:506–11. 60. Hoeck HC, Vestergaard P, Jakobsen PE, Falhof J, Laurberg P. Diagnosis of growth hormone (GH) deficiency in adults with hypothalamic-pituitary disorders: comparison of test results using pyridostigmine plus GH-releasing hormone (GHRH), clonidine plus GHRH, and insulin-induced hypoglycemia as GH secretagogues. J Clin Endocrinol Metab 2000;85:1467–72. 61. Ghigo E, Aimaretti G, Gianotti L, Bellone J, Arvat E, Camanni F. New approach to the diagnosis of growth hormone deficiency in adults. Eur J Endocrinol 1996;134:352–6. 62. Bennett RM, Clark SR, Walczyk J. A randomized, double-blind, placebo-controlled study of growth hormone in the treatment of fibromyalgia. Am J Med 1998;104:227–31.