Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
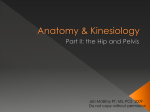
Gynecologic Oncology 116 (2010) 33–37 Contents lists available at ScienceDirect Gynecologic Oncology j o u r n a l h o m e p a g e : w w w. e l s e v i e r. c o m / l o c a t e / y g y n o Pelvic lymphadenectomy in cervical cancer—surgical anatomy and proposal for a new classification system D. Cibula a,⁎, N.R. Abu-Rustum b a b Oncogynecological Centre, Department of Obstetrics and Gynecology, General Faculty Hospital, First Medical Faculty, Charles University, Apolinarska 18 Prague 2, 12000, Czech Republic Gynecology Service, Department of Surgery, Memorial Sloan-Kettering Cancer Center, New York, NY, USA a r t i c l e i n f o Article history: Received 9 July 2009 Available online 17 October 2009 a b s t r a c t Background. Pelvic lymphadenectomy is an integral component of gynecologic cancer surgery, yet there is a lack of standardization in the terminology used, the extent of the procedure, and the definition of anatomic landmarks. This lack of standardization if corrected will likely facilitate a more clear communication and analysis of outcomes from various institutions, and reduce confusion to trainees about the procedure being performed. Methods. We summarize the anatomic data concerning pelvic lymphatic drainage; describe the procedure based on clearly defined anatomic landmarks; and finally propose a new classification system to facilitate standardization, communication, and comparison of results. The accompanying video demonstrates the anatomic landmarks. Results. We list and define four commonly used terms related to pelvic lymph node harvesting: sentinel node mapping, excision of bulky nodes, pelvic lymph node sampling, and systematic pelvic lymphadenectomy. We list the five specific anatomic regions of the pelvic lymphatic basin: external iliac, obturator, internal iliac, common iliac, and presacral. We highlight the important neural structures located in regions of the pelvic lymphadenectomy: genitofemoral nerve, obturator nerve, cranial part of the lumbosacral plexus, hypogastric plexus, and splanchnic nerves. Finally, we propose a new, four-part classification system of types of pelvic lymph node dissection. Conclusion. In this report and video, we demonstrate anatomy and offer a new classification system for pelvic lymphadenectomy. © 2009 Elsevier Inc. All rights reserved. Introduction Surgery is the least standardized treatment modality in gynecologic oncology. This lack of standardization is due to factors such as differences in surgical approach, technology used, patient anatomy, difficulty in measuring and quantitating the extent of procedures, and also imprecise definitions of the extent of some surgical procedures. The technique of pelvic lymphadenectomy has been much discussed in the literature, both in gynecology and urology [1-7]. There are, however, still differences in the terminology used to describe this procedure. Furthermore, anatomic landmarks are not clearly defined in all pelvic regions. The total number of lymph nodes examined in the final pathology report, although highly dependent on the patient and on the quality and accuracy of the pathologic evaluation, still remains one of the few objective criteria in the assessment of the procedure's extent and completeness. With the exception of sentinel node mapping, the larger total lymph node counts are frequently used as a surrogate for radicality and completeness of surgery. The number of lymph nodes examined in the final report varies substantially in the literature, and this variation mirrors a general lack of standardization in pelvic lymphadenectomy. The aim of this paper is to contribute to the standardization of pelvic lymphadenectomy terminology and technique. In particular, we summarize the anatomic landmarks concerning pelvic lymphatic drainage that may serve as the rationale for determining the extent of pelvic lymphadenectomy; describe the procedure in a video based on clearly defined anatomic landmarks; and finally propose a new classification system to facilitate standardization, communication, and comparison of results. Commonly used terminology ⁎ Corresponding author. Oncogynecological Centre, Department of Obstetrics and Gynecology, General Faculty Hospital, First Medical Faculty, Charles University, Apolinarska 18, Prague 2, 120 00, Czech Republic. Fax: +420 224967452. E-mail address: [email protected] (D. Cibula). 0090-8258/$ – see front matter © 2009 Elsevier Inc. All rights reserved. doi:10.1016/j.ygyno.2009.09.003 Our first step is to identify commonly used terminology relating to the pelvic lymphadenectomy. In the current literature, several types of surgical procedures for pelvic lymph node harvest are recognized. 34 D. Cibula, N.R. Abu-Rustum / Gynecologic Oncology 116 (2010) 33–37 Sentinel lymph node biopsy (SLN) The least extensive lymph node harvesting procedure is the sentinel node (SLN) biopsy. The objective of the SLN is to detect and remove the first draining lymph node(s) on each side of the pelvis. Several authors have reported high rates of detection and sensitivity in cervical cancer (especially small tumors) [8-10]. It is assumed that SLN mapping will become a standard part of the surgical management of cervical cancer. Excision of only bulky nodes Excision of only bulky nodes is a limited lymphadenectomy targeting enlarged nodes only. Nevertheless, there have been repeated reports showing low reliability of palpation of the retroperitonium, and an inadequate sensitivity of current imaging methods in detection of positive nodes [11-12]. Pelvic lymph node sampling Pelvic lymph node sampling is variably defined, either as the removal of a certain minimal number of lymph nodes, or based on anatomic criteria [13]. Irrespective on the definition, lymphatic tissue removal is limited to easily accessible pelvic regions and does not address all nodal groups. The number of lymph nodes obtained during sampling procedures is usually very low. Complete (systematic) pelvic lymphadenectomy Complete pelvic lymphadenectomy should be defined as the removal of all fatty lymphatic tissue from the predicted areas of high incidence of lymph nodes with metastatic involvement. The extent of the procedure should be standardized, and defined by exact anatomic landmarks. The aim of the complete pelvic lymphadenectomy is to remove the majority of lymphatic tissue that drains pelvic organs. The following regions are the most commonly recognized: common iliac, external iliac, internal iliac, obturator, and sacral (or presacral). Some authors further differentiate parametrial and interiliac regions, while others include tissue from the interiliac region to the external iliac and obturator regions and remove the tissue from the parametrial region together with the parametrium during radical hysterectomy. SLN mapping and distribution of positive pelvic nodes in cervical cancer In recent years, there has been a growing interest in SLN mapping owing to an effort to evaluate reliability and accuracy of SLN biopsy in cervical cancer. In the largest studies, 75–88% of SLN were found in two main regions: the obturator fossa and the external iliac region (defined as interiliac by Marnitz et al. [9]) (Fig. 1) [8-10]. About 5% of SLN were reported in the presacral region, and 5% in the common iliac region. Data differ for the internal iliac, paraaortic, and parametrial regions, most likely due to differences in anatomic boundaries of each region [14-15]. Unfortunately, the majority of studies do not allow for more detailed anatomical analysis of SLN localization within the regions described above; such analysis would be beneficial, especially for obturator (supra- or infraobturator) or common iliac (superficial or deep) regions. Not surprisingly, localization of metastatically involved SLN corresponds well with sites of their most frequent detection (Fig. 1) [8-10]. Moreover, the localization of positive pelvic lymph nodes correlates well with data available from SLN mapping (Fig. 1) [16-18]. In larger studies of early stages cervical cancer, positive lymph nodes were most frequently detected in the external iliac, obturator, internal iliac, common iliac, and parametrial regions. Localization in the paraaortic region (1–4.3%) or in the inguinal nodes (1.9%) was rarely Fig. 1. Distribution of sentinel nodes / positive sentinel nodes / positive lymph nodes in % (adopted from [8-10, 16-18]). Regions: CI–common iliac; PS–presacral; EI–external iliac; OBT–obturator; II–internal iliac. reported. Some authors have differentiated deep common iliac and infraobturator (deep obturator) regions, where positive nodes were found in 7% (1/14) [16]. Large variations in the distribution are again likely due to the differing anatomic boundaries of individual regions, mostly including the parametrial or part of the external iliac nodes in the obturator region. Anatomy of the pelvic lymph node drainage Classical anatomical studies on cadavers described very complex lymphatic drainage of the cervix, creating three major lymphatic trunks: lateral, anterior, and posterior. These major trunks terminate in the interiliac, common iliac, obturator, inferior gluteal, superior gluteal, superior rectal, or presacral nodes (regions) [19]. Based on data from surgicopathologic studies on SLN and the distribution of nodal metastasis, it is obvious that clinical importance of the above regions is not equal. Specifically, the superior rectal, superior gluteal, and inferior gluteal regions are rarely involved. For surgical anatomy, it is important to emphasize that the main purpose of major lymphatic trunks in the pelvis is to drain the lymph from lower extremities cranially toward the paracaval and paraaortic lymphatic systems. These trunks receive multiple channels from the midline gynecological organs. Surgical dissection inside these trunks is more difficult; it causes bleeding and inevitably leads to incomplete removal of lymphatic tissue that belongs to highly networked lymphatic trunks. Two major lymphatic trunks can be identified running on the lateral pelvic walls, which are involved in drainage of the cervix, with multiple connections between them. Comprehensive demonstration is available on this paper's accompanying film (supplementary data; film also available at www.esgo-forum.org/videolibrary). A “superficial trunk” enters the pelvis through the femoral canal; it courses on the ventral walls of external iliac vessels, receives lymphatic channels from parametria, and continues on the ventral wall of the common iliac artery cranially to precaval and interaortocaval regions (Figs. 2 and Supplementary Fig. 1). A deep trunk enters the pelvis from the femoral canal as well, medial to external iliac vessels, and surrounds the obturator nerve as a broad bundle of fatty lymphatic tissue, receiving numerous channels from lateral parametria (Fig. 3 and Supplementary Fig. 2). From the obturator fossa it continues cranially to the space between superior gluteal vessels and the psoas muscle, where it divides into two parts (Fig. 3). The first one creates a deep common iliac branch that runs between the psoas muscle and common iliac vein, continuing cranially D. Cibula, N.R. Abu-Rustum / Gynecologic Oncology 116 (2010) 33–37 35 Surgical anatomy of pelvic lymphadenectomy To facilitate orientation, the pelvic lymphatic basin can be divided into five specific anatomic regions. External iliac region (Fig. 4) Tissue is removed cranially, laterally, and medially from both external iliac vessels and between them. The medial border is formed by the opened space of the paravesical fossa, which is bounded cranially by the course of the umbilical ligament. The lateral border is the psoas muscle. The ventral border is commonly indicated as the origin of the deep circumflex iliac vein; however, the origin of this vessel is variable and other lymph nodes are located more ventrally. The ventral border should thus be the superior ramus of the pubic bone and the entry into the femoral canal. Some authors have suggested a greater risk of lymphedema after removal of these distal external iliac nodes. The risk of their metastatic involvement is probably low, but exact data are not available [20]. The dorsal border is the level of the common iliac artery bifurcation, where it continues as the superficial common iliac region. Caudally, it is the level of the caudal margin of the external iliac vein where the tissue proceeds into the obturator region. Fig. 2. Diagram of pelvic lymphatic drainage - superficial lymphatic trunk (right side) EIA–external iliac artery; EIV–external iliac vein; IIV–internal iliac vein; IIA–internal iliac artery; CIA–common iliac artery; CIV–common iliac vein; GN–genitofemoral nerve; PM–psoas muscle; A–aortic bifurcation SLT–superficial lymphatic trunk; EI–external iliac region; SCI–superficial common iliac region. into the paracaval region. The second one, which is often overlooked during lymphadenectomies, runs medially through a tunnel below the common iliac vessels into the medial aspect of common iliac vessels, continuing cranially into the presacral region (Fig. 3 and Supplementary Fig. 3). From here it crosses, cranially, the left common iliac vessels and enters mostly interaortocaval and preaortic regions (Supplementary Fig. 2). This deep trunk receives—on the medial aspect of the common iliac vessels—a lymphatic branch from the internal iliac region, having multiple channels from parametria. Fig. 3. Diagram of pelvic lymphatic drainage–deep lymphatic trunk (right side) EIV– external iliac vein; EIA–external iliac artery; IIV–internal iliac vein; IIA–internal iliac artery; CIA–common iliac artery; CIV–common iliac vein; GN–genitofemoral nerve; PM–psoas muscle; A–lymphatic passage below common iliac vessels DLT–deep lymphatic trunk; OBT–obturator region; II–internal iliac region; DCI–deep common iliac region. Obturator region (Fig. 5) Tissue is removed from the obturator fossa. The cranial border is the caudal wall of the external iliac vein. The dorsal border is the level of the bifurcation of the common iliac vessels, medial the paravesical space, formed by the lateral wall of the urinary bladder. The ventral border is the pubic bone together with the levator ani and obturator muscles, where the obturator nerve leaves the pelvis through the obturator canal. The lateral border is formed by the obturator internal muscle; caudal anatomical landmarks are obturator vessels. Fig. 4. Anatomic landmarks of external iliac (EI), superficial common iliac (SCI), internal iliac (II) and presacral (PS) regions B–deep iliac circumflex vein; ON–obturator nerve; UL–umbilical ligament; PVS–paravesical space; IIA–internal iliac artery; IIV–internal iliac vein; SN–splanchnic nerves; SHP–superior hypogastric plexus; U–ureter; MU– mesoureter; SB–sacral bone; A–aortic bifurcation; EIA–external iliac artery; EIV– external iliac vein; PM–psoas muscle; GN–genitofemoral nerve; CIV–common iliac vein; CIA–common iliac artery; IVC–inferior vena cava. 36 D. Cibula, N.R. Abu-Rustum / Gynecologic Oncology 116 (2010) 33–37 by the course of both common iliac vessels, on the left side partially by the mesoureter [21]. The caudal border is formed by the sacral bone, and the ventral by the level of the right common iliac vessels bifurcation. Anatomic considerations of neural structures encountered during pelvic lymphadenectomy Awareness of anatomic location of nerve structures in all regions of pelvic lymphadenectomy is essential for the safety of procedure. Care must be taken to avoid any harm to nerves, either direct injury or indirect thermal damage caused by electrosurgery. Genitofemoral nerve (Figs. 2 and 4) Runs in the common iliac region on the cranial aspect of the psoas muscle. This nerve often forms two branches in the external iliac region: one branch continues on the psoas muscle, while the second joins the superficial lymphatic trunk on the cranial aspect of external iliac artery, where it can be easily cut or injured. Obturator nerve (Fig. 5) Runs in the middle of obturator fossa, surrounded by fatty lymphatic tissue. It leaves the pelvis ventrally through the obturator canal, and is exposed also in the deep common iliac region between the psoas muscle and common iliac vein, where it runs from below the psoas muscle. Fig. 5. Anatomic landmarks of deep common iliac (DCI) and external iliac (EI) regions PVS–paravesical space; EIA–external iliac artery; EIV–external iliac vein; UL–umbilical ligament; OA–obturator artery; OV–obturator vein; OM–obturator muscle; ON–obturator nerve; SGV–superior gluteal vein; LST–lumbosacral nerve trunk; SB–sacral bone; CIA– common iliac artery; CIV–common iliac vein; ILV–iliolumbal vein; PM–psoas muscle. Internal iliac region (Fig. 4) Tissue is removed medially from the internal iliac vein. The ventral border is the level of the uterine vein origin; medially it is the mesoureter (a thin layer, coursing caudally from the ureter to the sacral bone, forming the boundary between the pararectal fossa medially, and lympho-fatty tissue and large vessels laterally; containing the hypogastric plexus), cranially and laterally it is the course of the internal iliac vessels, caudally it is the sacral bone, and dorsally it is the level of the bifurcation of the common iliac vessels. Common iliac region (Figs. 4 and 5; Supplementary Fig. 5) Tissue is removed ventrally and laterally from both common iliac vessels. The lymphatic tissue can be anatomically divided into two parts: the superficial branch, which continues from the external iliac region, and the deep branch, which runs deeply between the common iliac vein and psoas muscle, continuing from the obturator region. The dorsal border is the level of the aorta bifurcation; medial on the right side is the medial aspect of common iliac vessels (the tissue medial to the vessels is removed together with the presacral nodes), while on the left it is the mesoureter (tissue medial to the vessels should be removed as well). Lateral border is formed by the psoas muscle, ventral by the bifurcation of common iliac vessels. The caudal border is formed by the sacral bone, the cranial part of the lumbosacral trunk (L4 + L5) (medially), and the obturator nerve (laterally), where it enters under the psoas muscle. Presacral region (Fig. 4 and Supplementary Fig. 6) Tissue is removed above the sacral bone below and between both common iliac veins. The cranial and lateral borders are formed Cranial part of the lumbosacral plexus (L 4-5) (Fig. 5 and Supplementary Fig. 5) Exposed together with the obturator nerve (which is lateral) in a deep common iliac region. Hypogastric plexus (Fig. 4) Runs inside of the mesoureter, which forms a thin tissue layer between pararectal fossa and large vessels; it is exposed during dissection of the presacral and internal iliac regions. Splanchnic nerves (Fig. 4) Cross the space between the mesoureter and large vessels; are exposed during dissection of the internal iliac region. Proposal for a new classification system of types of pelvic lymph node dissection We propose a new system to classify types of pelvic lymph node dissection. The four types are listed below. • Type SLN: Only the sentinel lymph nodes detected in the pelvic basin are removed • Type I dissection: External iliac region: removes lymph nodes anterior and medial to the external iliac vessels, ventrally up to the deep circumflex iliac vein. Obturator region: removes obturator nodes above the obturator nerve. Common iliac region: removes nodes anterior (superficial common iliac region) up to the mid common iliac vessels. • Type II dissection: D. Cibula, N.R. Abu-Rustum / Gynecologic Oncology 116 (2010) 33–37 This is a type I dissection which also includes all of the following steps: External iliac region: removes nodes between the external iliac vessels and psoas muscle after vessel mobilization and complete skeletonization; removes distal nodes caudal to deep circumflex iliac vein. Internal iliac region: exposes the internal iliac vein and removes internal iliac nodes. Obturator region: removes nodes below obturator nerve. Presacral region: complete removal of presacral nodes. • Type III dissection: This is a type II dissection which also includes all of the following steps: Common iliac region: removal of superficial common iliac nodes up to the aortic bifurcation; complete medialization of the common iliac vessels and removal of deep common iliac nodes between the lateral aspect of the common iliac vein and the psoas muscle exposing lumbosacral trunk. Conclusion Pelvic lymph node dissection remains an integral component of gynecologic cancer surgery. In modern surgical practice it is essential to standardize terminology and the extent of procedures to facilitate clear communication and analysis of outcomes from various institutions, and to reduce confusion to trainees about the procedure being performed. With our increasing knowledge of the patterns of lymphatic drainage from the emerging SLN mapping data and from anatomic dissections in the living, we are now able to more accurately map and localize the anatomic regions most relevant to the diseases we treat and more precisely target the pelvic regions at risk for nodal metastasis. In spite of continuing debates about the “therapeutic role” of pelvic lymph node dissection in some gynecologic malignancies, a pelvic lymphadenectomy will remain a sentinel procedure in gynecologic oncology training and an important surgical tool for resection of metastatic disease and for staging of select gynecologic tumors. As gynecologic oncologists, we should continue to teach this important procedure to residents and fellows in training and provide them with better anatomic and oncologic rationale for what we practice. We hope that this article and video contributes to standardization and classification of one of the basic procedures in gynecological oncology and improves communication and educational efforts among various training programs. Conflict of interest statement The authors have no conflicts of interest to disclose. Appendix A. Supplementary data Supplementary data associated with this article can be found, in the online version, at doi:10.1016/j.ygyno.2009.09.003. 37 References [1] Kolbenstvedt A, Kolstad P. The difficulties of complete pelvic lymph node dissection in radical hysterectomy for carcinoma of the cervix. Gynecol Oncol 1976;4:244–54. [2] Pilleron JP, Durand JC, Hamelin JP. Location of lymph node invasion in cancer of the uterine cervix: study of 140 cases treated at the Curie Foundation. Am J Obstet Gynecol 1974;15:453–7. [3] Burghardt E, Pickel H. Local spread and lymph node involvement in cervical cancer. Obstet Gynecol 1978;52:138–45. [4] Mangan CE, Rubin SC, Rabin DS, Mikuta JJ. Lymph node nomenclature in gynecologic oncology. Gynecol Oncol 1986;23:222–6. [5] Benedetti-Panici P, Scambia G, Biaocchi G, Greggi S, Mancuso S. Technique and feasibility of radical para-aortic and pelvic lymphadenectomy for gynecologic malignancies: a prospective study. Int J Gynecol Cancer 1991;1: 133–40. [6] Benedetti-Panici P, Scambia G, Baiocchi G, Matonti G, Capelli A, Mancuso S. Anatomical study of para-aortic and pelvic lymph nodes in gynecologic malignancies. Obstet Gynecol 1992;79:498–502. [7] Herrel SD, Trachtenberg J, Theodorescu D. Staging pelvic lymphadenectomy for localized carcinoma of the prostate: a comparison of 3 surgical techniques. J Urol 1997;157:1337–9. [8] Wydra D, Sawicki S, Wojtylak S, Bandurski T, Emerich J. Sentinel node identification in cervical cancer patients undergoing transperitoneal radical hysterectomy: a study of 100 cases. Int J Gynecol Cancer 2006;16:649–54. [9] Marnitz S, Köhler C, Bongardt S, Braig U, Hertel H, Schneider A. Topographic distribution of sentinel lymph nodes in patients with cervical cancer. Gynecol Oncol 2006;103:35–44. [10] Rob L, Strnad P, Robova H, Charvat M, Pluta M, Schlegerova D, et al. Study of lymphatic mapping and sentinel node identification in early stage cervical cancer. Gynecol Oncol 2005;98:281–8. [11] Hricak H, Gatsonis C, Chi DS, Amendola MA, Brandt K, Schwartz LH, et al. Role of imaging in pretreatment evaluation of early invasive cervical cancer: results of the intergroup study American College of Radiology Imaging Network 6651–Gynecologic Oncology Group 183. J Clin Oncol 2005;23: 9329–37. [12] Mitchell DG, Snyder B, Coakley F, Reinhold C, Thomas G, Amendola MA, et al. Early invasive cervical cancer: MRI and CT predictors of lymphatic metastasis in the ACRIN 6651/GOG 183 intergroup study. Gynecol Oncol 2009;112: 95–103. [13] Gynecologic Oncology Group: Surgical Procedures Manual. Revised July 2005. [14] Darai E, Lavoué V, Rouzier R, Coutant C, Barranger E, Bats AS. Contribution of the sentinel node procedure to tailoring the radicality of hysterectomy for cervical cancer. Gynecol Oncol 2007;106:251–6. [15] Coutant C, Morel O, Delpech Y, Uzan S, Darai E, Barranger E. Laparoscopic sentinel node biopsy in cervical cancer using a combined detection: 5-year experience. Ann Surg Oncol 2007;14:2392–9. [16] Benedetti-Panici P, Maneschi F, Scambia G, Greggi S, Cutillo G, D'Andrea G, et al. Lymphatic spread of cervical cancer: an anatomical and pathological study based on 225 radical hysterectomies with systematic pelvic and aortic lymphadenectomy. Gynecol Oncol 1996;62:19–24. [17] Sakuragi N, Satoh C, Takeda N, Hareyama H, Takeda M, Yamamoto R, et al. Incidence and distribution pattern of pelvic and paraaortic lymph node metastasis in patients with stages IB, IIA, and IIB cervical carcinoma treated with radical hysterectomy. Cancer 1999;85:1547–54. [18] Bader AA, Winter R, Haas J, Tamussino KF. Where to look for the sentinel node in cervical cancer. Am J Obstet Gynecol 2007;197:678. [19] Coleman R, Levenback C. Lymphatics of the cervix. In: Levenback C, van der Zee AGJ, Coleman RL, editors. Clinical lymphatic mapping in gynecologic cancers. London and New York: Taylor and Francis; 2004. [20] Abu-Rustum NR, Barakat RR. Observations on the role of circumflex iliac node resection and the etiology of lower extremity lymphedema following pelvic lymphadenectomy for gynecologic malignancy. Gynecol Oncol 2007; 106:4–5. [21] Querleu D, Ferron G, Rafii A, Bouissou E, Delannes M, Mery E, et al. Pelvic lymph node dissection via a lateral extraperitoneal approach: description of a technique. Gynecol Oncol 2008;109:81–5.