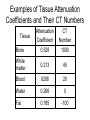
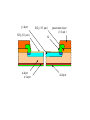
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Computed Tomography in the Diagnostic Radiography Curriculum My Disclaimer • My position on CT in the Diagnostic Curriculum is that it is more beneficial than harmful. • I am not suggesting that students graduate from our Programs as CT techs. • I AM suggesting that they have an understanding of the modality, its basic concepts, and focused clinical opportunities. The Premise • I look at CT within the curriculum as a twofold activity from the student perspective. – One, provides students a basic overview of what CT is, how it works, and why its ‘better’ for some diagnoses. – Two, CT provides an excellent means of review for general radiography principles that may be old hat for some, boring for others, or just offers a different perspective than the original explanations. When to Present CT • CT has to be in the second year or later. There needs to be a foundation of relevance and understanding. • In our Program, CT is officially taught in the Rad T 265 course, first semester second year. • Clinical rotations begin in the middle of the first semester second year. • Unofficially CT is found throughout our second year curriculum. • Radiologic Technology 265 • Principles of Digital Imaging and Computer Applications (2) Prerequisite: Radiologic Technology 165. Introduction to computer aided medical imaging's as used in radiography departments. Applications include computed and digital radiography (CR/DR), CT, MRI, and other modalities. Basic imaging principles are applied, including physics, imaging protocols, and systems electronics. Software and display strategies for varying modalities will be discussed. • • • • • • • • • • • • • • • • • Date Aug 28 Sep 4 Sep 11 Sep 18 Sep 25 Oct 2 Oct 9 Oct 16 Oct 23 Oct 30 Nov 6 Nov 13 Nov 20 Nov 27 Dec 4 Dec 11 Lecture Topic Orientation/Principles of CT HOLIDAY Components of a CT scanner Data Acquisition technology Spiral CT Image reconstruction Image quality Image manipulation MRI physics and equipment MRI image acquisition Computer literacy and its relevance Basic concepts of digital imaging Digital fluoroscopy Digital fluoroscopy Ultrasound and Nuc. Med. Applications FINAL Reading Assignment B. Ch 29, M v3 Ch 33 B. Ch 30 M. Ch 36 M. v. 3 Ch 36 B. Ch 26 B. Ch 27, M v3 Ch 34 M v 3 Ch 35, B. Ch 28 M v3 Ch 37&38 Why the importance of teaching CT? • Provides a break from the regular routine. • Offers ‘new’ technology or info that may be exciting. • Reviews existing (hopefully) knowledge. – For example, Photon/tissue interactions • Great way to review anatomy and pathology as seen clinically. • Provides an excellent opportunity to experience a modality first hand. The Clinical Component • We began a clinical affiliation this year with a free-standing imaging center. • Last year, we had an observational agreement that allowed students to visit and only watch. • This year students have clinical expectations based on the time they spend there. Clinical continued • Students are allowed to pick a three week optional rotation. – We chose this in order to have students doing something that interested them thereby decreasing the possibility of discontent. – Also, students looking for additional education, therapy or nuclear medicine, could get their observational requirements met. The Proposed CT Curriculum • CT Generations • Components, Operations, and Processes • Radiation Protection Practices CT Generations • This is really the only area that has limited value in the diagnostic curriculum. First and Second Generation CT • The first and second generations of CT were very similar. • Both used a scanning technique called translate/rotate in order to move around the patient. • The first generation scanner used a single detector and thin beam. While the second generation scanner use several detectors and a fan beam. – These changes resulted in a significantly faster scanner. Third Generation • The big change here was that the tube was in constant motion throughout the exposure, no more stops and starts. • The detectors were also moving during the exposure and more detectors were added. • As before, we now have an even faster scanner. Fourth Generation • It became obvious that moving detectors introduces noise into the image. • Now the detectors are fixed in a ring around the patient and only the tube moves. • Thousands of detectors are now needed to generate an image. • Faster imaging with increased spatial resolution. Fifth Generation • Electron beam CT – EBCT – Ultrafast Spiral • Slip-ring technology eliminates power cables. • Constant power to moving tube. • Continuous exposure • Patient moves through the beam during exposure • A stream a data is generated (spiral) as opposed to a series of individual slices. • CT scanner generations have limited value outside of understanding CT. However, it does provide a mechanism to see the development of a modality. • Additionally, the advantages of each generation and its evolution illustrates the thought processes that go into learning and adapting. Components, Operations, and Processes • Most of these topics have direct correlation to diagnostic radiography. – Data acquisition – Factors controlling image appearance – Anatomical structures – Post-processing Data Acquisition • Methods – Slice by slice • Contiguous – Volumetric • Spiral/helical Beam Geometry • Parallel • Fan – The traditional beam geometry, it is opened along the width of the patient. • Spiral – The beam is continuously on allowing for more anatomical coverage in a shorter time. Data Acquisition system (DAS) Components • • • • • Tube Detectors Filters Collimators ADC CT Tubes • Much higher heat loading than conventional tubes – 8MHU and up • Generally have two focal spots Filters • Again CT filtration is similar to diagnostic radiography • All tubes are required to have minimum filtration – Primary purpose is patient protection – Also, in CT the filter is used to harden the beam; thereby, decreasing absoption • Compensating filters – ‘Bow-tie’ – Uniform beam intensity at the detectors • Think ‘wedge ‘ filter in diagnostic radiography. CT Collimators • CT consists of both pre and post-patient collimation • Pre-patient collimation is analogous to the collimation we already know. – Controls beam coverage or amount of anatomy exposed. Post-patient Collimation • Controls slice thickness. • Additionally, it serves to define the slice profile which provides a sort of grid effect. – Scatter rejection Analog-to-Digital Convertor (ADC) • Converts the analog signal from the detectors to a digital signal for processing. • Rated by bits – Most scanners today are 16-bit systems – Produce 4096 data points • The more data points, the better the gray scale (contrast) resolution. Measurement of the Transmitted Beam • A ray – Basically, the detected value of a single photon • Several rays combine to form a view. – The data from multiple photons hitting the detector during a single translation. • Profile – The electrical signal produced by the detector. Encoding into Binary Data • The data from the views is converted into attenuation coefficients using the formula: = 1 ___ lnI /I o x • The attenuation coefficients are then sent to the ADC. Data Transmission to the Computer • Data processing begins – The raw (detector) data is preprocessed to remove bad data sectors. • The reformatted raw data is now sent to the array processors. – The array processors are using filter algorithms to produce the desire image appearance, i.e. soft tissue, bone, high-res. • After the array processors, the data is then subjected to a reconstruction algorithm that produces the cross-sectional image we see. • The most common reconstruction algorithm today is the filtered back projection. • The data is now image data and available for image manipulation. The CT Image • Any digital image, including CT, is comprised of picture elements (pixels). • The pixels are 2-dimensional elements that represent volume elements (voxels). • Pixels are displayed in a matrix. • The brightness of each pixel is determined by the CT number it represents. CT Numbers • CT numbers are calculated by comparing the attenuation coefficients of water and tissue. • The formula is: __ CT # = t w __________ . w K • The CT number of water is ‘0’. • Now, if you look at the formula you can see that tissues attenuate more than water will have a positive CT number. • Conversely, tissues less attenuate less have negative CT numbers. Examples of Tissue Attenuation Coefficients and Their CT Numbers Attenuation Coefficient CT Number Bone 0.528 1000 White matter 0.213 45 Blood 0208 20 Water 0.206 0 Fat 0.185 -100 Tissue Factors Affecting Attenuation • Photon energy – Selected kVp – Filtration • Tissue effective atomic number • Tissue mass density Selectable Scan Factors • Field of View – Scan – Display • • • • Matrix size Slice thickness Algorithm Scan time and rotational arc • Tube output – mAs • Region of Interest (ROI) • Magnification • FSS and Tube geometry Scan FoV • The total area from which raw data is acquired Display FoV • Determines how much raw data is used in displaying the acquired image. Matrix Size • Basically, the number of pixels displayed. • Affects spatial resolution – The bigger the matrix the more pixels. – Given that image size stays the same the pixels have to be smaller; therefore, spatial resolution increases. • Generally, the larger the image matrix the higher the patient dose. Algorithm • Mathematical formula applied to the raw data in order to produce a specific image outcome. Scan time and Rotational Arc Radiographic Tube Output • mAs ROI • Allows the technologist to select a specific area of interest for image reconstruction. • Uses the raw data for the reconstruction instead of using image data – The result is a better quality image. Magnification • Defined as a post-processing activity. – Magnification uses image data not raw data, so the final product has less spatial resolution than when using ROI. FSS and Tube Geometry • FSS – In CT, FSS selection has the same connotations it has in diagnostic radiography. • A smaller FSS has more detail (resolution) than a larger one. However, due to digital imaging issues (monitor and matrices) the effects of a small versus large FSS are not as apparent. Factors Affecting Image Quality • • • • • Spatial resolution Contrast resolution Noise Radiation dose Artifacts Spatial Resolution • The degree of blurring within the image • Ability to discriminate objects of varying density a small distance apart. • CT spatial resolution is affected by – Geometric factors – Reconstruction algorithm Geometric Factors • • • • • • FSS Detector aperture width Slice thickness SID SOD – distance to isocenter Sampling distance – Number of projections Reconstruction algorithms • Several different types of convolution algorithms are available. – Edge enhancement – Smoothing – Soft tissue – Bone • Matrix size is also going to play a role in spatial resolution Potential Spatial Resolution Algorithm Spatial Resolution Ultrahigh 15 Brain soft tissue 9.5 Abdomen soft tissue Abdomen low detail 10 6 • Can easily be demonstrated on CR/DR as well as CT – Examples here Spatial resolution • FoV – Amount of anatomy displayed – Also an issue with fluoroscopy – Affects on patient dose • Matrix – Affects on spatial resolution and patient dose • Pixel • Voxel • Slice thickness – Opportunity to demonstrate partial voluming and superimposition Contrast Resolution • Affected by several factors – Photon flux – Slice thickness – Patient size – Detector sensitivity – Reconstruction algorithm – Image display – noise Photon flux • Basically, the number of photons available – kVp – mAs – Beam filtration • Patient size also affects photon flux – Larger patients attenuate more photons Slice Thickness • Slice thickness is controlled by postpatient collimation • Tight collimation decreases the number of scattered photons that can strike the detectors – Fewer scatter photons, more contrast • Essentially, post-patient collimation works like a grid. Detector Sensitivity • The more sensitive the detector the more variation in photon energy it will resolve Reconstruction Algorithm • Smooth algorithms improve contrast resolution – A rule of thumb • Increase spatial resolution decrease contrast resolution Grayscale Manipulation Distortion Noise Spatial Resolution Post-Processing • • • • Image Reformation Image smoothing Edge enhancement Grayscale manipulation Radiation Dose • • • • Technical factor selection Adjustments for children Scanner dosimetry survey Reducing scatter to the technologist Data Acquisition • In CT data is acquired from either scintillation or gas-filled detectors. Scintillation or Solid-state detectors • Various materials are coupled to photodiodes to record photon activity. – Examples of materials include: • Cadmium tungstate • Ceramics doped with gadolinium or yttrium Indirect Digital Radiography The intensifying screen is made up of cesium-iodide crystals and the photodetector is made up of amorphous silicon. p--layer SiO2 (0.1 μm ) n-layer n+-layer SiO2 ( 0.5 μm ) passivation layer ( 1.0 μm ) Al Al-layer Another Positive in the CT Debate • During the past several years there has been an ongoing discussion about how do we get people interested in being faculty. • Adding CT brings another group of potential faculty members to the table. – Certainly, we increase the probability of adjunct faculty to teach the CT component. • Also, we increase the exposure of our students to potential employers. http://w4.siemens.de/FuI/en/archiv/zeitschrift/heft1_97/artikel03/inde x.html http://www.impactscan.org/rsna2001.htm Contrast Media Photon Tissue Interactions • PE • CE Scatter Control Filtration • Compensating • Required • Effects on beam energy Anode Heel Effect • Line focus principle Exposure Creep • Look for article about pediatric overexposure in CT Sensitivity of Image Receptor • Differences providing the ability to visualize different structures Quantum Mottle • Along for fluoroscopy an excellent modality to demonstrate the effects of it. • Now possible with CR/DR Cross-sectional anatomy • Provides further review for students • Allows them to learn about something they frequently see in the department and hospital. • Certainly helps with positioning and pathology review. Equipment • • • • • Detectors Tubes FSS Filtration Collimation Concepts • • • • Spatial resolution Contrast resolution Image matrix FoV Patient Care • Contrast Media – Patient prep – Reactions – Dose rates – Venipuncture – Ionic v. non-ionic – Atomic number • Concentration • Barium versus iodine Tubes • Anode heel effect • Line focus principle Collimation • Total • Compensating • Pre and post – grid and patient dose Tissue Interactions • Photoelectric effect – Absorption • Compton effect – Scatter – Attenuation PE • Absorption • High contrast • Plain film radiography CE • Low contrast • Scatter • High energy photons – More likely forward scatter • High energy photons – Less absorption (charts/graphs here) Contrast resolution • This will be new – Gray scale – Dynamic range – High and low contrast – Count anatomical structures Radiation Protection • Dose versus Image Quality Quantum Mottle • Easily demonstrated – CR/DR applicable • Particularly when using appropriate techniques – Fluoroscopy applicable Technique selection • No penalty for overexposure – Similar to CR/DR • Too little exposure is trouble – Quantum mottle • Exposure creep Anatomy and Pathology • Opportunity to review diseases again Spine • CSP • LSP – Intervertebral foramen – Zygo joints • Myelograms • Discograms – In some facilities this may be the only opportunity to see these exams Stomach • • • • • Location Position Structures Pathology contrast Kidney • Mention in last years student bowl • Position and angulation Colon • Flexures and their position • Pathology • Appendicitis Skull • Skull types – Angles – Visibility of structures Extremities • Positional relationships between structures • Angles • Non-linear reconstructions Patient Prep • Contrast • Instructions • Post-procedural care – Biopsies – Myelograms – Etc. Review of Lab Values • • • • • • • Vital Signs Hemoglobin RBC Platelets O2 Prothrombin Partial thromboplastin time Several labs will only be done in CT Consents Postural hypotension