Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
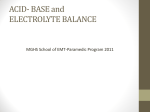
10 Acid–Base Paul W.G. Elbers, Victor A. van Bochove, Pieter Roel Tuinman, and Rainer Gatz Acid–base disturbances are common in critically ill patients and have important physiologic, prognostic, and diagnostic implications. Acidity is determined by the concentration of H+, usually expressed as its negative logarithm, i.e., pH (Table 10.1). Normal [H+] is essential for the function of proteins and hence enzymes, cells, and organ systems. Therefore, it is tightly regulated. The Stewart Approach Traditionally, the bicarbonate-centered and base excess methods have dominated the approach to acid–base disturbances in the United States and Europe, respectively. More recently, the quantitative approach by Stewart has emerged, especially in critical care medicine. Although all approaches are mathematically compatible, this physiochemical approach arguably facilitates better understanding and quantification of complex acid–base disorders. As these occur frequently in critically ill patients, this chapter will primarily focus on the Stewart approach. Important normal values in acid–base physiology including those related to the quantitative approach are given in Table 10.2. One of the fundamental principles of the Stewart approach is that [H+] is governed by a system of chemical equilibrium equations that have to be satisfied simultaneously (see Table 10.3). These can then be mathematically combined and rearranged to yield an expression of [H+] in terms of so-called independent parameters: (( ( ( ¢ éëH + ùû + éëH + ùû ´ ([ K A ] + [SID ]) + éëH + ùû ´ éë K A ùû ´ [SID ] - [ ATOT ] - K C ´ PCO2 + K W 4 3 ( ( 2 ) ) ))) + ¢ éëH + ùû ´ K A ´ K C ´ PCO2 + K W + K 3 ´ KC ´ PCO2 - K A ´ K 3 ´ K C ´ PCO2 = 0 While this may seem intimidating at first glance, these actually demystify the topic completely as there are only three of these independent parameters that determine [H+]. These are: 1. PCO2, the partial pressure of CO2 2. SID, the strong ion difference 3. ATOT, the concentration of nonvolatile weak acids P.W.G. Elbers, MD, PhD (*) • P.R. Tuinman, MD, PhD Department of Intensive Care Medicine, VU University Medical Center, De Boelelaan 1117, Amsterdam 1081 HV, The Netherlands e-mail: [email protected]; [email protected] This implies that all disturbances and corrections occur by changes in one or more of these parameters. In addition, they also ultimately determine other dependent variables such as [HCO3−] and anion gap. In other words, [H+] is a function of the independent parameters: V.A. van Bochove, MSc Department of Anesthesiology, Erasmus University Medical Center, Rotterdam, The Netherlands R. Gatz, MD Department of Anaesthesia and Intensive Care, Herlev Hospital, Herlev, Denmark éëH + ùû = f ( SID, ATOT , PCO2 ) One can think of the independent variables as three forces trying to move [H+] up or down. [H+] will be determined by © Springer International Publishing Switzerland 2016 J.M. O’Donnell, F.E. Nácul (eds.), Surgical Intensive Care Medicine, DOI 10.1007/978-3-319-19668-8_10 109 110 P.W.G. Elbers et al. Table 10.1 Relationship between hydrogen ion concentration and pH [H ] (nanoEq/L) 10 20 40 60 100 pH 8.00 7.70 7.40 7.22 6.70 + Table 10.2 Important acid–base-related parameters and their normal values pH [H+] PCO2 SID SIG AG [HCO3−] 7.35–7.45 35–45 nanoEq/L 38–42 mmHg 38–42 mEq/L 0–2 mEq/L 8–16 mEq/L 22–26 mEq/L SID strong ion difference, SIG strong ion gap, AG anion gap Table 10.3 The Stewart equations Water dissociation equilibrium Weak acid dissociation equilibrium Conservation of mass for “A” Bicarbonate ion formation equilibrium Carbonate ion formation equilibrium Electrical neutrality equation ¢ éëH + ùû ´ éëOH - ùû = K W KA × [HA] = [H+] × [A−] [PCO2] × KC = [H+] × [HCO3−] [K3] × [HCO3−] = [H+] × [CO32−] SID + [H+] − [HCO3−] − [A−] − [CO32−] − [OH−] = 0 All equations reflect chemical equilibriums that need to be satisfied simultaneously. K items represent constants. Units are mEq/L for ions, mM for HA, and ATOT and kPa or mmHg for PCO2. SID strong ion difference. See text for detailed explanation Table 10.4 Classification of acid–base disorders based on the Stewart approach Acidosis High PCO2 Low SID High ATOT Low PCO2 alkalosis Compensation For low SID and/or high ATOT acidosis Central Pain, fear, stress, voluntary, psychogenic Pregnancy (progesterone) Early sepsis (cytokines) Hepatic failure (toxins) Drugs (analeptics, salicylate intoxication) Head injury, stroke Pulmonary Any cause of hypoxemia Pulmonary embolism Pneumonia Asthma Pulmonary edema (all types) Iatrogenic Excessive mechanical ventilation High PCO2 acidosis Compensation For high SID and/or low ATOT alkalosis Central Drugs (opioids, sedatives) Head injury, stroke, tumor, infection Hypoventilation of obesity Neuromuscular Cervical cord lesion <C4 Guillain–Barré syndrome Myasthenia gravis Neuromuscular blocking agents Toxins (organophosphates) Myopathies Lung or chest wall disease Exacerbation of COPD Chest trauma Pneumothorax Diaphragmatic paralysis Pulmonary edema ARDS Restrictive lung disease Airway disorders Iatrogenic Inadequate mechanical ventilation SID strong ion difference. See text for details ATOT = [A−] + [HA] Respiratory Non-respiratory (metabolic) Table 10.5 Causes of PCO2-induced alkalosis and acidosis Alkalosis Low PCO2 High SID Low ATOT their relative strength. A classification of acid–base disturbances based on this approach is given in Table 10.4. PCO2 It follows from the Stewart equations that if PCO2 increases, [H+] must increase as well. Causes of high PCO2 acidosis and low PCO2 alkalosis may be found in Table 10.5. These include the respiratory response to acid– base disturbances, which exert their compensatory effect on [H+] by modulating PCO2. Normally, alveolar ventilation is adjusted to balance cellular CO2 production. The respiratory center controls alveolar ventilation. Normal PCO2 is between 35 and 45 mmHg. In case of hyperventilation or hypoventilation in relation to CO2 production, PCO2 will decrease or increase, respectively. High PCO2 acidosis is commonly encountered in the critically ill patient who cannot maintain adequate ventilation. Specific etiologies include airway obstruction, respiratory center depression, neuromuscular disorders, and pulmonary diseases such as chronic obstructive pulmonary disease (COPD). High PCO2 acidosis is also induced with intentional hypoventilation (permissive hypercapnia) to aid in the treatment of patients with status asthmaticus or acute respiratory distress syndrome. This lung protective ventilatory strategy is well tolerated by the patient and has little impact on hemodynamics. Mismatch in alveolar ventilation and CO2 production can also occur in case of increased CO2 production as seen in sepsis. Of note, alveolar ventilation may markedly differ from ventilation measured as tidal volume times respiratory rate, because of anatomic dead space but more importantly physiological dead space. Low CO2 alkalosis results from increased alveolar ventilation relative to CO2 production. Alveolar ventilation is regulated by several factors: chemoreceptors in the medulla 111 10 Acid–Base and great vessels, voluntary control, and pulmonary chemoreceptors and stretch receptors. Any of these factors alone or in combination may lead to hyperventilation. SID Strong ions are essentially completely dissociated and thus exist in charged form only, even if substantial amounts of some of these ions are non-covalently bound to serum proteins. Important examples are Na+, K+, Ca2+, Mg2+, Cl−, lactate, and keto acids. In contrast, weak ions can exist both in charged and uncharged forms. Examples include HCO3−, albumin, and inorganic phosphate (Pi). The SID is the sum of strong cations minus the sum of strong anions. In plasma, it is mainly determined by [Na+] and [Cl−] and its normal value is about 40 mEq/L. It follows from the Stewart equations that if SID decreases, [H+] must increase and vice versa. Causes of low SID acidosis and high SID alkalosis may be found in Table 10.6. These include the renal response to acid–base disturbances, which exert their compensatory effect on [H+] by modulating SID. Table 10.6 Causes of SID-induced alkalosis and acidosis Low SID acidosis Compensation For low PCO2 and/or low ATOT alkalosis Increased SIG/AGC Lactic acidosis Type A (inadequate O2 delivery) Type B (altered metabolism) Ketoacidosis diabetic Alcohol induced Starvation Acute renal failure Increased osmol gap Salicylates Ethylene glycol Methanol Normal SIG/AGc Infusion of low SID solutions (e.g., NaCl 0.9 %, D5W, H2O) Water retention Positive urine SID Renal tubular acidosis Carbonic anhydrase inhibitors Hypoaldosteronism Acute or chronic kidney disease Negative urine SID Severe diarrhea Pancreatic or biliary drainage Small bowel fistula Ureteroenterostomy High SID alkalosis Compensation For high PCO2 and/or high ATOT acidosis Urine [Cl−] < 10 mM (“hypovolemia”) Use of diuretics Vomiting, gastric drainage Villous adenoma Cl−-rich diarrhea Posthypercapnia Urine [Cl−] > 20 mM (“hypervolemia”) Severe potassium depletion Ongoing diuretic use Steroid administration ACTH excess Primary hypercortisolism Renin-secreting tumor Primary hyperaldosteronism Cushing’s syndrome Bartter’s syndrome Liddle’s syndrome Excessive licorice intake Others Strong cation administration (e.g., NaHCO3, citrate, acetate, lactate) Water loss Milk–alkali syndrome Laxative abuse Exogenous alkali SID strong ion difference, SIG strong ion gap, AGc corrected anion gap. See text for details ATOT Weak acids are molecules that exist in incompletely ionized forms. They are grouped as ATOT, the total amount of weak acids (ATOT), and consist mainly of plasma proteins. From an acid–base perspective, albumin and to a lesser extent phosphate are the most important contributors. It follows from the Stewart equations that if ATOT increases, [H+] must also increase. This implies that hypoalbuminemia of any cause contributes to alkalosis. Similarly, hyperphosphatemia, as seen in renal failure, causes acidosis. While the body actively controls SID and PCO2 to regulate acid–base balance, there is no evidence that the control of albumin or phosphate levels is used to control for acid–base disturbances. This, ATOT may rather be thought of as a set point that modifies the balance between SID and PCO2 to set [H+]. This is of paramount importance in the critically ill as hypoalbuminemia and dysphosphatemia are often present. Strong Ion Gap According to the principle of electrical neutrality, blood plasma cannot be charged, so SID must be balanced by negative charges. These mostly stem from CO2 (as HCO3−) and the weak acids (mainly the anionic forms of albumin and phosphate expressed as [A−]). We can calculate SID based on the negative charges of the weak acids. This is called effective SID or SIDE: SID E = ëéHCO3 - ùû + éë A - ùû where [A−] represents mainly [Albumin−] and [Pi−]. Their contribution may be quantified by calculating their anionic fraction. For physiological pH ranges, the following simplified formulas have good accuracy: éë Albumin - ùû = 0.25 ´ éë Albumin ( g / L ) ùû éë Pi - ùû = 1.5 ´ éë Pi - ( mmol / L ) ùû We can also calculate SID on the basis of the amounts of routinely measured strong ions. This is called the “apparent SID” or SIDA: ( ) SID A = éë Na + ùû + éëK + ùû + 2 ´ éë Mg 2 + ùû + éë Ca 2 + ùû - éëCl - ùû For practical purposes a simplified formula is recommended: SIDA = [Na+] + [K+] – [Cl–]. The strong ion gap (SIG) may now be calculated from the difference between apparent and effective SID: SIG = SID A – SID E The normal value for SIG is 0–2 mEq/L. However, normal values for gaps should be verified locally as they may P.W.G. Elbers et al. 112 Fig. 10.1 Graphical representations of AG (a) and SIG (b). Not to scale. Adapted from: Mizock BA. Lactic acidosis. In: Kellum JA, Elbers PW, editor. Stewart’s textbook of acid-base. 2nd ed. Amsterdam: AcidBase.org; 2009 (copyright: Paul Elbers) a b Other+ 2+ – 2+ Ca Mg Other La– Cations differ between hospitals as they depend on the individual components in the formula and their local normal values. A graphical representation of SIG may be found in Fig. 10.1. An increased SIG is virtually always caused by lactate or unmeasured anions. Lactic acidosis is the most commonly encountered cause of an SIG acidosis in the critically ill. It can occur as a result of either excessive lactate formation or decreased lactate clearance and can be divided into type A, or hypoxic lactic acidosis, and type B, or nonhypoxic lactic acidosis. Type A lactic acidosis is caused primarily by an increase in lactate formation as a consequence of tissue hypoxia, resulting, for example, from hemorrhagic shock. Type B lactic acidosis occurs during normal oxygen delivery and often occurs secondary to a variety of medications (epinephrine, biguanides, nitroprusside, AZT), metabolic diseases (glucose 6-phosphatase deficiency), and severe liver failure. The pathogenesis of lactic acidosis in sepsis is multifactorial and may include the development of anaerobic glycolysis within tissues, the inhibition of pyruvate dehydrogenase (an enzyme that converts pyruvate into acetyl coenzyme A), and a defective oxygen use at the mitochondrial level. Another common cause of high SIG acidosis is diabetic ketoacidosis. In typical severe cases SIG levels are 10–20 mEq/L. Other causes of an elevated AG acidosis may be diagnosed with appropriate laboratory evaluation. To further differentiate between causes of SIG, the osmol gap may be calculated. The osmol gap is equal to the difference between the measured serum osmolarity (OsmM) and the calculated serum osmolarity. A high plasma osmol gap (>10–15 mOsm/L) reflects the presence of an unmeasured Ca2+Mg2+ Other– La– A– A– HCO3– HCO3– Na+ K+ Other+ Na+ CI– Anions K+ Cations CI– Anions non-ionized compound. It can be mathematically represented as follows: æ 2 ´ é Na + ( mmol / L ) ù ö û ÷ ç ë Osmol gap = Osm M – ç + éë Urea ( mmol / L ) ùû ÷ ç ÷ ç + éëGlucose ( mmol / L ) ùû ÷ è ø To convert urea and glucose from mg/dL to mmol/L, divide by 18 and 2.8, respectively. The most frequent causes of an increased osmol gap are alcohol, mannitol, and ketones. Toxic alcohols also increase SIG as they are metabolized to organic acids such as glycolic acid. Thus, as a general rule, a high SIG metabolic acidosis together with an elevated osmol gap is probably due to intoxication with a toxic alcohol if lactic acidosis and diabetic ketoacidosis are not present and mannitol has not been administered. It should be noted that glycol intoxication may lead to falsely high lactate levels due to interference with its measurement. A low SID without an elevated SIG implies that this must be caused by changes in the measured strong ions. This is sometimes referred to as hyperchloremic acidosis. However, this may be a misnomer, as this type of acidosis can also exist without high chloride concentrations, provided that strong cations (mainly Na+) are more decreased than [Cl−]. It is useful to first assess any water excess, detected by abnormal Na+, and determine its cause. Water excess will cause a direct reduction in the normally positive SID because strong cations and strong anions are equally diluted. As a second step, a review of recent infusions is warranted. As explained below, these can directly influence SID. If no obvious cause is apparent, urine SID may be helpful to 113 10 Acid–Base d ifferentiate between gut and renal causes of SID acidosis. The urine SID is the difference between the routinely measured urinary cations and anions: Table 10.7 Ionic composition of common intravenous fluids NS Lactated Ringer’sa D 5W ½NS Gelatin 4 % NaHCO3 1.4 % NaHCO3 8.4 % Urine SID = éë Na + ùû + éëK + ùû – éëCl - ùû u u u The presence of a positive urine SID in an individual with low SID acidosis without SIG suggests that the disorder is due to an impaired acid–base handling by the kidneys (e.g., distal renal tubular acidosis). Conversely, the presence of a negative urine SID suggests that the metabolic acidosis is due to gastrointestinal causes (e.g., diarrhea). In patients with renal insufficiency or in those being treated with diuretics, urinary values need to be interpreted with caution. Finally serum potassium may be helpful in distinguishing causes of low SID acidosis. Hypokalemia (<3.5 mmol/L) is associated with ureteral diversion, diarrhea, proximal colostomy, ileostomy, proximal renal tubular acidosis (RTA), type I distal RTA, and parenteral nutrition. Hyperkalemia (>4.5 mmol/L) can be found in hypoaldosterone states, ammonium chloride administration, and type IV distal RTA. An increased strong ion difference is alkalinizing. A common cause is aggressive diuresis with loop diuretics resulting in a low intravascular volume. Other etiologies are noted in Table 10.6 and are grouped into those that are associated with hypovolemia or hypervolemia, although significant overlap may exist. Measurement of [Cl−]u is usually more helpful in distinguishing the two categories, provided that renal compensatory capacity is not severely impaired. In non-respiratory alkalosis, the [Cl−]u is a more accurate reflection of intravascular volume than urine sodium. Fluid Therapy Infusion fluids can directly influence SID. This happens when the SID of the infusion fluid itself differs from that of plasma. For example, NaCl 0.9 % contains 154 mM Na+ and 154 mM Cl−; hence its SID is zero. Adding NaCl 0.9 % to plasma with SID of 40 mM will directly lower its SID. Thus overzealous infusion of low SID solution will cause acidosis. As fluid SID determines its effect, the pH of an infusion fluid is not of any importance. Balanced infusion fluids usually contain strong anions such as lactate or acetate. Immediately upon infusion, their SID will also be 0 mM. However, the anions are normally rapidly metabolized, effectively increasing the SID of these solutions. An overview of the constitution and SID of commonly used infusion fluids is given in Table 10.7. Finally it should be remembered that in clinical practice, kidney handling of strong ions and dilution of ATOT will partially offset the effect on plasma SID of infusion fluids. Na+ 154 131 0 77 154 167 1000 K+/Ca2+ 5/2 Cl− 154 111 HCO3− Lactate− 0 0 0 29 SID 0 29 0 0 0 0 0 0 77 120 0 0 0 0 0 167 1000 0 0 34 167 1000 0 0 0 0 0 Lactated Ringer’s is made by a number of different manufacturers and may have slight variations in formula a Table 10.8 Potential complications of bicarbonate administration Volume overload Paradoxical cerebrospinal fluid/intracellular acidosis Respiratory acidosis Impaired O2 delivery (tissue hypoxia) Hypokalemia Hypocalcemia Hypernatremia Hyperosmolality Overshoot alkalemia Classic buffer fluids include sodium bicarbonate and tromethamine. Although studies have not shown consistent benefit, it is reasonable to administrate these fluids in severe acidosis as a temporizing measure. Sodium bicarbonate directly increases SID and is thus alkalinizing. However, bicarbonate ions combine with hydrogen ions to form carbonic acid, which in turn dissociates into water and CO2. Thus, potential complications of bicarbonate administration may outweigh possible benefits (Table 10.8). Tromethamine (THAM) is a weak alkali that increases arterial pH without producing CO2. THAM has potentially serious side effects, including hypoglycemia and hyperkalemia. Bedside Stewart Approach Using the Stewart approach at the bedside may be perceived as cumbersome because of the calculations involved. However, the widespread introduction of computers in clinical medicine has solved this problem. The online clinical module at www.acidbase.org gives a complete description and in-depth analysis of any acid–base problem. However, for rapid clinical assessment, we suggest the following simplified approach. It introduces a simplified version of SIG by focusing only on [Na+], [Cl−], and SIDE: 1.Determine the problem and its severity by assessing pH. Remember that acidosis and alkalosis refer to P.W.G. Elbers et al. 114 rocesses that influence [H+] or pH. A normal pH does not p rule out acid–base pathology. 2. Assess the relative contribution of the three independent variables that influence [H+]. (a) Assess PCO2. A high PCO2 is acidifying. A low PCO2 is alkalinizing. (b) Assess ATOT and calculate its anionic charge A− = 0.25 × [Albumin (g/L)] + 1.5 × [Pi (mmol/L)]. A high ATOT is acidifying. A low ATOT is alkalinizing. (c) Assess SID by calculating SIDE = HCO3− + A−. A high SID is alkalinizing. A low SID is acidifying. 3. Calculate simplified SIG = [Na+] – [Cl−] – SIDE to assess the effect of unmeasured ions. If necessary, use osmol gap, urine SID, and/or urine chloride to improve discrimination between causes of acid–base disturbances. Clinical Features of Acid–Base Disorders Clinical features of acid–base disorders depend largely on the underlying disorder, although abnormal pH itself may impair cardiopulmonary physiology and the immune system. Alkalosis impairs oxygen delivery to tissues and causes neuromuscular hyperexcitability likely because of induced hypocalcemia (seizures, arrhythmias, paresthesias, carpopedal spasms). In respiratory alkalosis, acute hypocapnia induces cerebral vasoconstriction and syncope and seizures may occur. Cardiovascular changes may include an increase in heart rate, arrhythmias, and angina. Typical signs of acidosis are mostly related to the respiratory system. For example, the rapid, deep respirations of Kussmaul breathing occur as a compensatory response for non-respiratory acidosis. Impressive examples include cases of diabetic ketoacidosis, as these typically occur in young patients with large capacity for respiratory compensation. Other clinical features associated with acidosis are arrhythmias, insulin resistance, hyperkalemia, and coagulopathies. In severe acidosis, cardiovascular collapse may be seen. In respiratory acidosis, severe elevations of PCO2 may cause asterixis, myoclonus, and seizures. Papilledema may be found during the examination. Conjunctival and superficial facial blood vessels also may be dilated. Management of Acid–Base Disorders Treatments should always primarily address the underlying causes of acid–base disorders. This implies that other measures, such as fluid therapy to influence SID or changing the settings of the mechanical ventilator to influence PCO2, should only be used to gain time in extreme acid– base disturbances. Mechanical ventilator settings have a profound effect on acid–base status and require appropriate management with adjustments based on pH and not only PCO2. Treatment of respiratory acidosis may require supportive invasive or noninvasive mechanical ventilation. A therapeutic pitfall to avoid in the treatment of respiratory acidosis is the creation of a posthypercapnic metabolic alkalosis. This condition most commonly occurs when a patient with compensated chronic respiratory acidosis is ventilated to a normal or near-normal PCO2. Fluid therapy using high SID solutions such as sodium bicarbonate may have a role in extreme acidosis, especially if at least partially caused by a low SID, as indicated by a low sodium-chloride difference, but such buffering should be used with caution as outlined previously. Fluid therapy for metabolic alkalosis, especially if [Cl−]u is low, includes low SID solutions (Table 10.7) such as normal saline or even HCl. For other causes of metabolic alkalosis, acetazolamide should be considered, especially if diuresis is necessary. Acetazolamide is a carbonic anhydrase inhibitor that produces diuresis and increases the renal excretion ratio of sodium to chloride. However, judicious use is paramount as acidemia may result, associated with worsening hypokalemia because of kaliuresis. Refractory or severe alkalemia (pH > 7.6) can be treated with isotonic HCl (150 mEq/L) via a central vein over 8–24 h. Potassium deficiencies should be corrected. The Bicarbonate-Based Approach The classic methods for assessing acid–base disturbances remain popular and are based on the Henderson–Hasselbalch equation, which is the logarithmic form of the Henderson equation: éëH + ùû = 24 ´ PCO2 / éëHCO3 - ùû This equation is actually one of the Stewart equations (Table 10.3). Singling out, this fixed relationship is attractive as it allows addressing acid–base disorders in terms of changes in PCO2 and [HCO3−]. However, caution should be exerted, as [HCO3−] itself is a dependent variable. Thus, PCO2 and [HCO3−] are interdependent, which may lead to circular reasoning. Table 10.9 shows the four main acid–base disorders that can be distinguished using the Henderson–Hasselbalch equation. Respiratory disturbances are related to excess or a deficiency of carbon dioxide (respiratory). Non-respiratory or metabolic disturbances are associated with changes in [HCO3−]. 115 10 Acid–Base Table 10.9 Acid–base disorders according to the Henderson– Hasselbalch-based approach Condition Metabolic acidosis Metabolic alkalosis Respiratory acidosis Respiratory alkalosis pH ↓ ↑ ↓ ↑ PCO2 ↓ ↑ ↑ ↓ HCO3– ↓ ↑ ↑ ↓ Table 10.10 Expected compensatory mechanisms according to the Henderson–Hasselbalch-based approach Disorder Metabolic acidosis Primary change ↓ [HCO3–] Metabolic alkalosis ↑ [HCO3–] Respiratory acidosis ↑ PCO2 Respiratory alkalosis ↓ PCO2 Compensatory mechanism Alveolar hyperventilation to ↓ PCO2 Alveolar hypoventilation to ↑ PCO2 ↑ renal compensation resulting in ↑ [HCO3−] ↓ renal compensation leading to ↓ [HCO3–] metabolic acidosis and measured [HCO3−] of 12 mEql/L, the expected PCO2 would be (1.5 × 12) + 8 = 26 mmHg ± 2. If the actual PCO2 is above 28 mmHg, this indicates the presence of an associated respiratory acidosis (e.g., ketoacidosis and severe pneumonia). Conversely, if the actual PCO2 is below 24 mmHg, this indicates the presence of an associated respiratory alkalosis (e.g., septic shock and inappropriate mechanical ventilation). The Henderson–Hasselbalch-based approach to respiratory acidosis is the same as that of the Stewart approach as discussed previously. However, its approach to non- respiratory acid–base disturbances is different and relies on the determination of anion gap and the delta gap. Anion Gap and the Corrected Anion Gap The anion gap is the difference between the concentration of determined cations and measured anions in plasma (Fig. 10.1). The AG can be estimated by the following formula: ( Table 10.11 Expected compensation according to the Henderson– Hasselbalch-based approach Acid–base disorder Metabolic acidosis Metabolic alkalosis Acute respiratory acidosis Chronic respiratory acidosis Acute respiratory alkalosis Chronic respiratory alkalosis Expected compensation ↓PCO2 = 1.2 × ↓ HCO3– or PaCO2 = 1.5 × [HCO3–] + 8 ± 2 ↑ PCO2 = 0.6 × ↑ HCO3– ↑ HCO3– = 0.1 × ↑ PCO2 ↑ HCO3– = 0.35 × ↑ PCO2 ↓ HCO3– = 0.2 × ↓ PCO2 ↓ HCO3– = 0.5 × ↓ PCO2 A positive or negative change represents an increase or decrease, respectively, from the normal value of 40 mmHg for PCO2 or 24 mEq/L for HCO3– Respiratory and metabolic acid–base disorders initiate predictable compensatory mechanisms that aim to return the pH to normal. These can be classified as follows in Table 10.10. Respiratory compensation occurs rapidly. Metabolic compensation takes hours to days. However, some immediate metabolic compensation will occur because of a shift in the dissociation of the weak acids, mainly albumin, with corresponding rises or falls in bicarbonate concentrations. Still, acute and chronic metabolic compensation may be distinguished. Reasonably healthy individuals exposed to a single acid–base disturbance will show a predictable compensatory response. This has been studied and empirical calculations of the expected response have been derived, commonly known as Winters’ formulae (Table 10.11). If compensation is different from expected, multiple acid–base disorders coexist. For example, in a patient with ) AG = éë Na + ùû - éëCl - ùû + éëHCO3 - ùû The normal AG is 12 ± 4 mEq/L. However, normal values for gaps should be verified locally as they may differ between hospitals as they depend on the individual components in the formula and their local normal values. The unmeasured ions include proteins, phosphates, sulfates, and organic acids. These can be markedly changed in critically ill patients, especially albumin and phosphate. Thus the measured anion gap needs to be corrected for both. The following formula gives a fair estimate of the corrected anion gap: AG C = AG + 0.25 ´ ( 40 - Albumin ( g / L ) ) +1.5 ´ (1 - Pi ( mM ) ) Although the concepts of AG and SIG have markedly different theoretical backgrounds, they both result from the need for electroneutrality in plasma. Thus, the potential causes of high SIG acidosis are the same as those for an elevated AG, provided that the latter be corrected for albumin and/or phosphate levels. These causes are listed in Table 10.6. Delta Gap In an uncomplicated high AG metabolic acidosis, every increase of 1 mEq/L in the AG should result in a concomitant decrease of 1 mEq/L in [HCO3–]. Deviation from this relation suggests a mixed acid–base disorder. The difference between these two values has been termed the delta gap (Δgap) and can be expressed as 116 P.W.G. Elbers et al. Dgap = deviation of AG C from normal – deviation of éë HCO3 - ùû from normal If the normal (corrected) AG is assumed to be 12 mEq/L and the normal [HCO3–] is 24 mEql/L, then the following equation results: ( ) Dgap = ( AG C – 12 ) – 24 – éëHCO3 - ùû A pure AG metabolic acidosis will yield a Δgap of zero; however, variance in measurements and the changing physiology of the patient can result in a Δgap of 0 ± 6. If the Δgap is significantly positive, i.e., greater than +6, then a simultaneous metabolic alkalosis exists because the rise in AG is more than the fall in HCO3. Conversely, if the Δgap is significantly negative, i.e., less than −6, then a concomitant normal AG metabolic acidosis is present because the rise in AG is less than the fall in HCO3. The urine anion gap is the same as the urine strong ion difference. Together with the osmol gap and serum potassium, these can be used to differentiate between causes of metabolic acidosis as discussed previously. Metabolic alkalosis is also treated similarly as the Stewart approach. Bedside Bicarbonate-Based Approach The following is a clinical approach based on the Henderson– Hasselbalch framework that can be utilized at the bedside: 1. Determine the overall acid–base condition by measuring pH. Is acidemia or alkalemia present? 2. Determine if the primary process is metabolic ([HCO3–] deviation) or respiratory (PCO2 deviation). 3. If a respiratory disturbance is present, determine if it is acute or chronic. 4. Determine if the expected compensation is adequate. 5. Calculate the AGC. 6. In case of high AGC metabolic acidosis, calculate the Δgap. 7.In case of normal AGC metabolic acidosis, calculate the UAG. blood pressure, 110/68 mmHg; heart rate, 80/min; respiratory rate, 8/min; and temperature, 97°F (36.1°C). The patient is obtunded and only weakly withdraws to painful stimuli. He is noted to have small pupils. Laboratory: Na+ 142 mEq/L, K+ 4.0 mEq/L, Cl– 104 mEq/L, albumin 40 g/L, and ABG (pH 7.24, PCO2 60 mmHg, PO2 64 mmHg, [HCO3–] 27 mEq/L). What are the acid–base disorder(s) and the likely etiology? Bedside Henderson–Hasselbalch Approach 1. What is the acid–base condition? Acidemia as evidenced by pH 7.24. 2. What is the primary process? Respiratory, because PCO2 is increased and [HCO3–] is not decreased as would be expected for a metabolic acidosis. 3. Is the respiratory process acute or chronic? Acute, as determined by expected bicarbonate change. In acute respiratory acidosis, an increase of 20 mmHg in the PCO2 corresponds to an increase in bicarbonate of around 2 mEq/L. 4. Determine if the expected compensation is adequate. The expected compensation for acute respiratory acidosis would yield [HCO3–] of 26 mmHg. 5. Determine AGC = [Na+] − [Cl−] − [HCO3−] + 0.25 × [40- Albumin] + 1.5 × [1 − Pi] = 142 − 104 − 27 − 0 − 0 (assumed) = 11 mEq/L. This is within the normal range. Note that AGC is equal to AG here because of normal albumin and phosphate concentrations. Bedside Stewart Approach 1.Determine the problem and its severity by assessing pH. Moderate acidemia as evidenced by pH 7.24. 2. Assess PCO2; 60 mmHg means an acidifying factor. 3. Assess SID. SIDE = [HCO3−] + [A−] = [HCO3−] + 0.25 × [Albumin] + 1.5 × [Pi] = 27 + 0.25 × 40 + 1.5 × 1 (assumed) = 38.5 mEq/L. This is 1.5 mEq/L different from normal. Slight acidifying factor. 4. Assess ATOT: normal albumin, normal phosphate (assumed). No significant acid–base influence. 5. S I G = [ N a + ] − [ C l − ] − S I D E = 1 4 2 − 1 0 4 − 3 8 . 5 = −0.5 mEq/L. No significant acid–base influence. Case Examples The following cases show the use of both the Stewart approach and the Henderson–Hasselbalch-based approach for the bedside evaluation of acid–base disorders. Answer: The acid–base condition is acute respiratory acidosis with a likely etiology of respiratory center depression from acute narcotic and/or alcohol intoxication or head trauma. Case 8-A Case 8-B A 24-year-old male is brought to the emergency center with head trauma after a fall at a party. On arrival, vital signs are A 68-year-old female with chronic renal failure presents with fever, severe right lower quadrant pain, and diarrhea for 10 Acid–Base 2 days. Laboratory: electrolytes (Na+ 135 mEq/L, K+ 3.4 mEq/L, Cl– 106 mEq/L) and albumin 35 g/L. Arterial blood gas results: pH 7.44, PCO2 12 mmHg, PO2 74 mmHg, [HCO3–] 8 mEq/L. What are the acid–base disorder(s) and the likely etiology? 117 etabolic acidosis. The respiratory alkalosis and the anion m gap acidosis are likely due to sepsis from an intra-abdominal source. The additional process of the normal anion/low SID acidosis may be related to the diarrhea. Pain and anxiety could contribute to the respiratory alkalosis, whereas possible renal insufficiency may contribute to high SIG metabolic acidosis. Bedside Henderson–Hasselbalch Approach 1. What is the acid–base condition? The pH is at the alkalemic end of the normal range; thus, a primary alkalosis is likely present. 2. What is the primary process? Respiratory because PCO2 is decreased and [HCO3–] is not increased as would be expected for a metabolic alkalosis. 3.Is the respiratory alkalosis acute or chronic? In acute respiratory alkalosis, the reduction of 28 mmHg in PaCO2 would correspond to a decrease in bicarbonate of around 2.8 mEq/L. The expected bicarbonate would be around 21 mEq/L. In chronic respiratory alkalosis, the decrease of 28 mmHg in PaCO2 would correspond to a reduction in bicarbonate of around 9.8 mEq/L. 4. Is the metabolic compensation adequate? The expected bicarbonate would be around 14 mEq/L. The bicarbonate concentration of the patient is lower than expected for either acute or chronic alkalosis. Thus, there is an associated metabolic acidosis. 5. Calculate the corrected anion gap. AGC = [Na+] − [Cl−] − [HCO3−] + 0.25 × [40-Albumin] + 1.5 × [1 − Pi] = 135 − 106 − 8 + 1.25 + 0 (assumed) = 22.25 mEq/L, which is elevated. Thus, an anion gap metabolic acidosis also exists. 6. Calculate the Δgap. Δgap = (AGC − 12) − (24 − [HCO3–]) = (22.25 − 12) − (24 − 8) = −5.75 mEq/L. Thus, this is a borderline low value, close to indicating a coexisting normal anion gap acidosis. Bedside Stewart Approach 1.Determine the problem and its severity by assessing pH. The pH is in the alkalemic range of normal. 2. Assess PCO2; 12 mmHg means an alkalinizing factor. 3. Assess SID. SIDE = [HCO3−] + [A−] = [HCO3−] + 0.25 × [ A l bu m i n ] + 1 . 5 × [ P i ] = 8 + 0 . 2 5 × 3 5 + 1 . 5 × 1 (assumed) = 18.25 mEq/L. This is 21.75 mEq/L different from the normal value of 40 mEq/L. Acidifying factor. 4. Assess ATOT: Slightly decreased albumin, normal phosphate (assumed). Slight alkalinizing influence of albumin. 5. SIG = [Na+] − [Cl−] − SIDE = 135 − 106 − 18.25 = 10.75 mEq/L. Thus, the SIG explains about half the deviation of SID from its normal value, the rest being due to relative hyperchloremia. Answer: The coexisting acid–base disorders are (1) primary respiratory alkalosis, (2) anion gap/SIG metabolic acidosis, and (3) hyperchloremic (normal anion gap) or low SID Case 8-C A 56-year-old female is brought to the emergency center after a fall. She seems to have broken her right femur. She is somnolent and her vital signs are blood pressure, 140/70 mmHg; heart rate, 90/min; and respiratory rate, 21/min. Laboratory: Na+ 130 mEq/L, K+ 3.5 mEq/L, Ca2+ 4.0 mEq/L, Mg2+ 1.6 mEq/L, Cl− 90 mEq/L, Pi 0.9 mmol/L, albumin 20 g/L, pH 7.50, PCO2 30 mmHg, HCO3− 23.5 mmHg. What are the acid–base disorder(s) and the likely etiology? Bedside Henderson–Hasselbalch Approach 1.What is the acid–base condition? The pH is alkalemic. Thus, a primary alkalosis is likely present. 2. What is the primary process? Respiratory because PaCO2 is decreased and [HCO3–] is not increased as would be expected for a metabolic alkalosis. 3.Is the respiratory alkalosis acute or chronic? In acute respiratory alkalosis, the reduction of 10 mmHg in PaCO2 would correspond to a decrease in bicarbonate of around 2 mEq/L. The expected bicarbonate would be around 22 mEq/L. In chronic respiratory alkalosis, the decrease of 10 mmHg in PaCO2 would correspond to a reduction in bicarbonate of around 5 mEq/L, yielding an expected bicarbonate of 19 mEq/L. 4. Is the metabolic compensation adequate? The bicarbonate concentration of the patient is slightly higher than expected for acute respiratory alkalosis, although this is typically judged as being in the expected range. 5. Calculate the corrected anion gap. AGC = [Na+] − [Cl−] − [HCO3−] + 0.25 × [40-Albumin] + 1.5 × [1 − Pi] = 130 − 90 − 23.5 + 5 + 0.15 = 21.65 mEq/L, which is elevated. Thus, an anion gap metabolic acidosis also exists. 6. Calculate the Δgap. Δgap = (AGC − 12) − (24 − [HCO3–]) = (21.35 − 12) − (24 − 23.5) = 8.85 mEq/L. This indicates the existence of a coexisting metabolic alkalosis. Bedside Stewart Approach 1.Determine the problem and its severity by assessing pH. Alkalemia as evidenced by a pH of 7.50. 2. Assess PCO2; 30 mmHg means an alkalinizing factor. 3. Assess SID. SIDE = [HCO3−] + [A−] = [HCO3−] + 0.25 × [Albumin] + 1.5 × [Pi] = 23.5 + 0.25 × 20 + 1.5 × 0.9 = 118 29.85 mEq/L. This is 10.15 mEq/L different from the normal value of 40 mEq/L. Acidifying factor. 4 . Assess ATOT. There is a severely decreased albumin concentration. This implies a strong alkalinizing factor. 5. SIG = [Na +] − [Cl −] − [HCO 3−] − SID E[A −] = 130 − 90 − 29.85 = 10.15 mEq/L. Thus, the high SIG completely explains the low SIDE. Answer: The metabolic acidosis is almost exactly balanced by alkalosis of hypoalbuminemia, so that [HCO3−] is within normal limits; AGC and SIG are high. It would be easy to miss this and interpret the data as a simple respiratory alkalosis, with no metabolic abnormalities. In this case, the AGC and SIG were found to be caused by ketoacidosis, despite this patient’s alkalemia. Further Reading 1.Adrogue HJ, Madias NE. Management of life-threatening acid– base disorders. First of two parts. N Engl J Med. 1998;338:26–34. 2. Adrogue HJ, Madias NE. Management of life-threatening acid–base disorders. Second of two parts. N Engl J Med. 1998;338:107–11. P.W.G. Elbers et al. 3.Fencl V, Jabor A, Kazda A, Figge J. Diagnosis of metabolic acid–base disturbances in critically ill patients. Am J Respir Crit Care Med. 2000;162:2246–51. 4.Figge J, Jabor A, Kazda A, Fencl V. Anion gap and hypoalbuminemia. Crit Care Med. 1998;26:1807–10. 5.Gunnerson KJ, Kellum JA. Acid–base and electrolyte analysis in the critically ill patients: are we ready for the new millennium? Curr Opin Crit Care. 2003;9:468–73. 6.Kellum JA, Elbers PW, editors. Stewart’s textbook of acid-base. Amsterdam: AcidBase.org; 2009. 7.Kellum JA. Clinical review: reunification of acid-base physiology. Crit Care. 2005;9:500–7. 8.Levraut J, Grimaud D. Treatment of metabolic acidosis. Curr Opin Crit Care. 2003;9:260–5. 9. Rose BD, Post TW, editors. Clinical physiology of acid–base and electrolyte disorders. New York: McGraw-Hill; 2001. 10. Story DA, Bellomo R. The acid–base physiology of crystalloid solutions. Curr Opin Crit Care. 1999;5:436–9. 11. Story DA, Morimatsu H, Bellomo R. Strong ions, weak acids and base excess: a simplified Fencl-Stewart approach to clinical acid- base disorders. Br J Anaesth. 2004;92:54–60. 12.Stewart PA. Modern quantitative acid–base chemistry. Can J Physiol Pharmacol. 1983;1:1444–61. 13. Worthley LI. Strong ion difference: a new paradigm or new clothes for the acid–base emperor. Crit Care Resusc. 1999;1:214. 14.Wrenn K. The delta (delta) gap: an approach to mixed acid–base disorders. Ann Emerg Med. 1990;19:1310–3.