Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
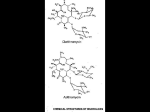
JAC Journal of Antimicrobial Chemotherapy (2000) 46, 255–262 Comparative efficacy of 5 days of dirithromycin and 7 days of erythromycin in skin and soft tissue infections Margaret M. Wasilewski*, Michael G. Wilson, Gregory D. Sides and Jennifer L. Stotka Lilly Research Laboratories, Eli Lilly and Company, Lilly Corporate Center, Indianapolis, IN 46285, USA We investigated the comparative efficacy and safety of dirithromycin and erythromycin in the treatment of skin and soft tissue infections in this double-blind, randomized, multicentre study, in which 439 patients were randomized to treatment with dirithromycin (500 mg daily for 5 days) or erythromycin (250 mg every 6 h for 7 days). All randomized patients were included in the termination analysis, which showed that 187 of 220 (85.0%) dirithromycin recipients and 177 of 219 (80.8%) erythromycin recipients were clinically cured or improved (95% confidence interval (CI) 3.0% to 11.4%). In the termination analysis of the 211 bacteriologically evaluable patients, clinical cure or improvement occurred in 83 of 100 (83%) dirithromycin recipients and in 89 of 111 (80.2%) erythromycin recipients (95% CI 7.8% to 13.4%), and bacteriological eradication occurred in 85 of 100 (85%) and 89 of 111 (80.2%), respectively. Adverse events were similar in incidence and nature between the two groups, except that there was less nausea with dirithromycin (3.6% versus 8.2%; P 0.042). Ten of 220 (4.5%) dirithromycin recipients and 27 of 219 (12.3%) erythromycin recipients returned >20% of their prescribed medication (P 0.033). In the treatment of skin and soft tissue infections, dirithromycin (500 mg daily for 5 days) was comparable in efficacy to, and caused significantly less nausea than, erythromycin (250 mg every 6 h for 7 days). Compliance with the dirithromycin regimen was superior to that with the erythromycin regimen. Introduction Most common skin and soft tissue infections, including impetigo, cellulitis, folliculitis, furuncles and carbuncles, are caused by Staphylococcus aureus and group A streptococci.1–3 The penicillins, first-generation cephalosporins, and macrolides are commonly used to treat uncomplicated community-acquired skin and soft tissue infections because of their historic activity against staphylococci and streptococci. However, resistant strains of staphylococci (β-lactamase-producing and/or non-β-lactamase-producing) are now widespread.4 In the last decade, the fluoroquinolones emerged as alternatives to the β-lactams for the treatment of skin and soft tissue infections. However, factors limiting use of fluoroquinolones include: gastrointestinal and central nervous system toxicity and the potential for arthropathy, which precludes routine use in children and adolescents;5 high cost relative to other orally administered alternatives; and an unnecessarily broad spectrum of activity for most common community-acquired skin and soft tissue infections.6 Traditionally, erythromycin has been both a first-line therapy and an alternative antibacterial agent for the treatment of patients who were sensitive to, or intolerant of, β-lactams. However, adverse gastrointestinal effects, poor absorption resulting in unpredictable serum and tissue concentrations, and clinically significant drug interactions are limiting factors. Dirithromycin is a 14-membered ring macrolide antibacterial agent, which is rapidly converted to its active form, erythromycylamine, by non-enzymatic hydrolysis during absorption. The antimicrobial spectra of dirithromycin and erythromycylamine are similar to that of erythromycin in vitro, with a reported potency ranging from two- to four-fold less active7 to two-fold more active8 against Gram-positive bacteria. Dirithromycin is highly active against streptococci, with an MIC90 of 0.25 mg/L being reported for Streptococcus pyogenes.9 Dirithromycin is also active against S. aureus, with an MIC90 of 4.0 mg/L, and Staphylococcus epidermidis, with an MIC90 of 1.0 mg/L.9 Dirithromycin has more favourable pharmacokinetics than erythromycin, and therefore has potential clinical *Corresponding author. Tel: 1-317-276-6291; Fax: 1-317-276-9666; E-mail: [email protected] 255 © 2000 The British Society for Antimicrobial Chemotherapy M. M. Wasilewski et al. advantages.10 Dirithromycin has a terminal half-life of 44 h (range 16–65 h) following a 500 mg oral dose,11 allowing for once-daily administration. The volume of distribution of dirithromycin at steady state is 5 L/kg. Tissue concentrations peak between 5 and 10 h after a dose and gradually redistribute into serum, resulting in a tissue half-life of 20 h. Thus, tissue concentrations are maintained well in the range of the MICs for susceptible organisms for at least 24 h after a single oral dose.12,13 Additionally, dirithromycin is not a competitor of the cytochrome P450 system, and thus has low propensity for drug interactions.14 Dirithromycin for 7 days has been shown to be effective in the treatment of skin and soft tissue infections.10 The objective of this study was to compare the efficacy and safety of dirithromycin 500 mg daily for 5 days with erythromycin 250 mg every 6 h for 7 days in the treatment of skin and soft tissue infections. Patient compliance with the once-daily dirithromycin regimen as compared with the four-times-daily erythromycin regimen was also assessed. Materials and methods Study design This was a double-blind, double-dummy, randomized, multicentre study with two parallel arms. Thirty-one physicians, who specialized in family practice, dermatology and internal medicine, participated in this study. Patients were randomized to receive either dirithromycin or erythromycin. Patients in the dirithromycin treatment group received a total daily dose of 500 mg, given as a single dose of two 250 mg tablets per day for five consecutive days. These patients also received dummy tablets resembling erythromycin, given as one tablet every 6 h for seven consecutive days. Patients in the erythromycin treatment group received a total daily dose of 1000 mg of erythromycin base, given as one 250 mg tablet every 6 h for seven consecutive days. These patients also received dummy tablets resembling dirithromycin, given as a single dose of two tablets per day for five consecutive days. Dirithromycin or its dummy was taken orally with, or immediately after, a meal. Erythromycin or its dummy was taken orally 1 h before meals and at bedtime. Almedica Drug Labeling System (ADLS) labels were used to identify the medication kits and bottles. All bottles with any remaining tablets were returned by the patient at the post-therapy visit, and the remaining tablets were counted. Patients were defined as compliant if they took 80% of tablets dispensed. A complete history, physical examination and culture of the infected site were performed at a pretherapy visit (within 24 h before the first dose of study medication). Patients with abscesses received surgical treatment as deemed necessary by the investigator. Physical examination and follow-up history were performed on days 3–5 of study medication, 3–5 days after the end of study medication (post-therapy visit) to evaluate clinical response to therapy, and 10–14 days after the end of study medication (late post-therapy visit) to evaluate recurrence of infection. Repeat skin or tissue cultures were performed at these visits, if clinically indicated. Patient population Patients aged 12 years, weighing at least 37 kg, and with a culturable bacterial infection of the skin and/or soft tissue were eligible for inclusion. Eligible bacterial infections included subcutaneous abscess, impetigo, pyoderma, skin ulcer (excluding decubitus and venous stasis ulcers, and ulcers below the knees in diabetic patients), post-surgical or traumatic wound infections, cellulitis or erysipelas and lymphangitis. Postpartum, nursing and pregnant women were excluded, and women of childbearing potential must have used a reliable method of birth control during, and for 30 days following completion of therapy. Other exclusion criteria included: the presence of any condition that could have precluded evaluation of response; any known or anticipated use of systemic or topical antimicrobials (other than as prescribed in the study) from 7 days before enrolment until the post-therapy evaluation; hypersensitivity to macrolide antibiotics; and use of oral or intravenous corticosteroids. Informed consent, approved by the institutional review board, was signed by each patient or their legal guardian. Clinical efficacy analysis All data were collected at the investigational site and analysed by Eli Lilly. Patients were considered clinically evaluable if they met enrolment criteria, had appropriate examinations before and after therapy and met standards for minimum compliance (no minimum compliance was required for a clinical response of relapse or failure, or for safety evaluation). Clinical response was assessed by the investigator based on signs and symptoms. Response definitions were as follows: (i) cure, elimination of all signs and symptoms of infection with no recurrence within the follow-up period; (ii) improvement, significant, but incomplete, resolution of signs or symptoms of infection; (iii) relapse, worsening of signs and symptoms of infection following initial improvement; relapse must have been preceded by at least one clinical assessment (either during or following therapy) of cure or improvement; (iv) failure, signs and symptoms did not subside or improve with therapy; a patient requiring the addition of another antibiotic for the study indication during the expected period of study drug administration was classified as a clinical failure; (v) unable to evaluate, unable to evaluate a clinical response because of premature discontinuation, lack of post-therapy evaluation, poor compliance or other extenuating circumstance; this response disqualified a patient for efficacy analysis but not for safety analysis. 256 Dirithromycin and erythromycin in SSTI Bacteriological efficacy analysis To qualify for the bacteriological evaluation, a patient must have met all qualifications for clinical evaluation, and the patient’s pretherapy culture had to be positive for a pathogen. While susceptibility to the study medication(s) was not a criterion for bacteriological evaluability, sensitivities15,16 were determined. Bacteriological response was assessed by the investigator based on culture results.17 Safety analysis All patients who gave consent to participate and were randomized to a treatment group were included in the safety analysis. At each visit, patients and/or guardians were asked open-ended questions regarding the occurrence and nature of any clinical adverse event and were instructed to contact the investigator should an adverse event occur. Haematology, blood chemistry and urine tests were performed at the visits before and after therapy, and at the late post-therapy visit, if clinically indicated. Adverse events were classified using the US Food and Drug Administration Coding Symbol Thesaurus for Adverse Reaction Terms (COSTART) and categorized by body system. Statistical analysis Statistical analyses were performed at two time points: after therapy and at termination. The termination analysis was based on the results of the late post-therapy visit (10–14 days after the end of study medication). However, if a patient had a clinical response of failure at the posttherapy visit (3–5 days after the end of study medication), or discontinued before the post-therapy visit, a late posttherapy response was not obtained. In this case, the response for that patient at the earlier visit was used in the termination analysis. All eligible patients were included in the clinical and bacteriological analyses. 2 tests and confidence intervals were used to compare clinical and bacteriological response rates between treatment groups. 2 tests also were used to compare adverse event frequencies between treatment groups. Appropriate continuous data procedures, such as t-tests, were used for the analysis of laboratory-monitoring data to test for significant changes from baseline values both within and between treatment groups. The general association Cochran–Mantel–Haenszel statistic was used to compare differences between treatment groups across investigators. Investigators who enrolled fewer than eight patients were pooled. Results Patient population Two hundred and twenty patients were randomized to the dirithromycin group and 219 to the erythromycin group. Approximately half of all patients had a diagnosis of subcutaneous abscess. The other most frequent diagnoses were traumatic wound infection, cellulitis and pyoderma. The two groups were well matched with respect to demographics and baseline clinical parameters (Table I). Of the 220 dirithromycin recipients, 187 were clinically evaluable; 100 of the latter were also bacteriologically evaluable. Of the 219 erythromycin recipients, 184 were clinically evaluable; 111 of the latter were also bacteriologically evaluable. The main reasons for clinical unevaluability were premature discontinuation because of lack of susceptibility of the pretreatment isolate to the study drug (before a protocol amendment negating this criterion) and loss to follow-up. The main reason for bacteriological unevaluability was failure to identify a pathogen. One hundred and sixty-eight of 220 dirithromycin recipients and 175 of 219 erythromycin recipients completed the protocol. Of patients who did not complete the protocol, 19 of 52 dirithromycin recipients and 15 of 44 erythromycin recipients discontinued because of lack of efficacy. Termination efficacy analyses Termination analysis of all patients. In the termination analysis, a favourable clinical response (cure or improvement) was seen in 187 of 220 (85.0%) dirithromycin recipients and in 177 of 219 (80.8%) erythromycin recipients (95% confidence interval (CI) for the difference between proportions 3.0% to 11.4%) (Table II). A statistically significant advantage for dirithromycin was demonstrated between treatment groups in the distribution of clinical responses (Pearson 2 10.933, four degrees of freedom (DF), P 0.027). A favourable bacteriological response (eradication or presumptive eradication) was seen in 146 of 220 (66.4%) dirithromycin recipients and 139 of 219 (63.5%) erythromycin recipients (95% CI 6.2% to 12.0%). There was no statistically significant difference between the treatment groups in the distribution of bacteriological responses in all patients at termination (Pearson 2 7.593, 4 DF, P 0.108). Termination analysis of bacteriologically evaluable patients. In the termination analysis of bacteriologically evaluable patients, a favourable clinical response (cure or improvement) was seen in 83 of 100 (83.0%) dirithromycin recipients and in 89 of 111 (80.2%) erythromycin recipients (95% CI 7.8% to 13.4% (Table III), but this was not statistically significant (Pearson 2 6.783, 3 DF, P 0.079). A favourable bacteriological response (eradication or presumed eradication) was seen in 85 of 100 (85%) dirithromycin recipients and 89 of 111 (80.2%) erythromycin recipients (95% CI 5.6% to 15.2%), but this difference also was not statistically significant. (Pearson 2 5.511, 3 DF, P 0.138), and results determined for the clinically evaluable population were comparable to those for the bacteriologically evaluable population. 257 M. M. Wasilewski et al. Table I. Demographic and baseline characteristics of the dirithromycin and erythromycin treatment groups Parameter Gender male female Mean age (years) Race Caucasian Black Hispanic Native American Asian other Mean height (cm) Mean weight (kg) Presenting diagnosis subcutaneous abscess traumatic wound infection cellulitis pyoderma impetigo post-operative wound infection infected skin ulcer lymphangitis erysipelas Dirithromycin (n 220) Erythromycin (n 219) 123 (55.9%) 97 (44.1%) 42.2 (range 13–92) 113 (51.6%) 106 (48.4%) 41.5 (range 12–86) 176 (80.0%) 26 (11.8% 16 (7.3%) 1 (0.5%) 1 (0.5%) 0 170.6 78.6 168 (76.7%) 20 (9.1%) 25 (11.4%) 3 (1.4%) 2 (0.9%) 1 (0.5%) 171.0 79.5 110 (50.0%) 24 (10.9%) 28 (12.7%) 30 (13.6%) 11 (5.0%) 14 (6.4%) 2 (0.9%) 1 (0.5%) 0 114 (52.1%) 31 (14.2%) 26 (11.9%) 15 (6.8%) 15 (6.8%) 9 (4.1%) 6 (2.7%) 2 (0.9%) 1.(0.5%) Correlation of clinical and bacteriological responses revealed that 82 of 100 (82%) dirithromycin recipients and 89 of 111 (80.2%) erythromycin recipients had both a favourable clinical and a favourable bacteriological response. Fourteen of 17 dirithromycin recipients and all 22 erythromycin recipients who had unfavourable clinical responses also had persistence or presumed persistence of the pathogen. Post-therapy efficacy analyses Results of efficacy analyses of data from the post-therapy evaluations (performed 3–5 days after the end of study medication) were similar to those for the termination analyses. There was no statistically significant difference between the treatment groups in the distribution of clinical responses (Pearson 2 3.171, 4 DF, P 0.530) or bacteriological responses (Pearson 2 4.807, 6 DF, P 0.569) for all patients at the post-therapy visit. In addition, the general association Cochran–Mantel– Haenszel statistic across investigators showed no statistically significant difference between treatment groups in the distribution of clinical responses (2 3.554, 4 DF, P 0.470) or bacteriological responses (2 5.847, 6 DF, P 0.441) for all patients at the post-therapy visit. Post-therapy analysis of bacteriologically evaluable patients by diagnostic subgroup. Post-therapy clinical and bacteriological results were analysed by diagnostic subgroup and were broadly similar between the two treatment groups. Of the patients with subcutaneous abscesses, who accounted for more than half of all bacteriologically evaluable patients, 48 of 54 (88.9%) dirithromycin recipients and 57 of 61 (93.4%) erythromycin recipients had a favourable clinical outcome. Thirty-nine of 54 dirithromycin recipients and 47 of 61 erythromycin recipients with abscesses underwent incision and drainage. There was no statistically significant difference in the proportions of favourable clinical responses between treatment groups after controlling for the effects of incision and drainage of subcutaneous abscess (Cochran– Mantel–Haenszel general association 2 0.536, 1 DF, P 0.464). Bacteriological eradication S. aureus was isolated from most infections before treatment and was eradicated or presumed eradicated from 44 of 56 (78.6%) dirithromycin recipients and from 48 of 59 258 Dirithromycin and erythromycin in SSTI Table II. Termination analysis: clinical and bacteriological responses in all patients Number of patients (%) Response Clinical favourable cure improvement total unfavourable relapse failure total Bacteriological favourable eradication presumed eradication total unfavourable presumed persistent persistence total dirithromycin (n 220) erythromycin (n 219) 95% CIa 141 (64.1%) 46 (20.9%) 187 (85.0%) 151 (68.9%) 26 (11.9%) 177 (80.8%) 13.9% to 4.1% 3.0% to 11.4% 13 (5.9%) 16 (7.3%) 29 (13.2%) 23 (10.5%) 11 (5.0%) 34 (15.5%) 2.3% to 6.8% 9.0% to 4.4% 5 (2.3% 141 (64.1%) 146 (66.4%) 0 139 (63.5%) 139 (63.5%) 6.2% to 12.0% 14 (6.4%) 8 (3.6%) 22 (10.0%) 17 (7.8%) 15 (6.8%) 32 (14.6%) a These are the lower and upper bounds for the 95% CIs for the true differences between treatment groups, percentage of dirithromycintreated patients minus percentage of erythromycin-treated patients. Since these confidence intervals contain 0, there are no statistically significant differences. Table III. Termination analysis: clinical and bacteriological responses in bacteriologically evaluable patients Number of patients (%) Response Clinical favourable cure improvement total unfavourable relapse failure total Bacteriological favourable eradication presumed eradication total unfavourable presumed persistent persistence total dirithromycin (n 100) erythromycin (n 111) 95% CIa 74 (74.0%) 9 (9.0%) 83 (83.0%) 86 (77.5%) 3 (2.7%) 89 (80.2%) 15.3% to 8.3% 7 (7.0%) 10 (10.0%) 17 (17.0%) 15 (13.5%) 7 (6.3%) 22 (19.8%) 3.9% to 11.3% 13.40% to 7.8% 4 (4.0%) 81 (81.0%) 85 (85.0%) 0 89 (80.2%) 89 (80.2%) 5.6% to 15.2% 11 (11.0%) 4 (4.0%) 15 (15.0%) 14 (12.6%) 8 (7.2%) 22 (19.8%) a 7.8% to 13.4% These are the lower and upper bounds for the 95% CIs for the true differences between treatment groups, percentage of dirithromycin recipients minus percentage of erythromycin recipients. Since these confidence intervals contain 0, there are no statistically significant differences. 259 M. M. Wasilewski et al. Table IV. Bacteriological eradication rates (proven or presumed) Number eradicated/total isolated Pathogens dirithromycin erythromycin 44/56 8/8 5/5 3/3 2/2 1/1 1/1 5/6 16/18b 48/59 12/13 5/5 2/3 1/1 2/2 – 0/1 19/27c Staphylococcus aureus Staphylococcus epidermidis Streptococcus group A Enterococcus Streptococcus group G Streptococcus group B Streptococcus group C Gram-negative organismsa Multiple organisms a Pseudomonas aeruginosa, Enterobacter agglomerans, Klebsiella pneumoniae, Proteus mirabilis, Serratia marcescens, Haemophilus influenzae. b Multiple pathogens persisted or were presumed to have persisted in two patients: S. aureus, K. pneumoniae and Morganella morganii in one patient, and S. aureus and Citrobacter sp. in the other patient. Both patients were clinical failures. c Multiple pathogens persisted or were presumed to have persisted in six patients, all of whom had unfavourable clinical responses: S. aureus and streptococcus group G; S. aureus and S. epidermidis; S. epidermidis and Enterobacter cloacae; S. aureus and streptococcus group B; S. aureus and streptococcus group A; and streptococcus group B and enterococcus, plus P. mirabilis. In two patients, one of two pathogens was eradicated while the other (S. aureus and P. mirabilis, respectively) persisted; both patients had unfavourable clinical responses. Table V. Adverse events reported by at least 2% of patients during the period of study drug administration, regardless of relationship to treatment (81.3%) erythromycin recipients infected with a single pathogen (Table IV). Safety analysis A total of 167 adverse events were reported by 92 of 220 (41.8%) dirithromycin recipients, and 182 events were reported by 96 of 219 (43.8%) erythromycin recipients (P 0.669). The events reported most frequently in both groups were headache and symptoms associated with the digestive system (abdominal pain, diarrhoea, dyspepsia and nausea). Nausea was reported by a significantly lower proportion of dirithromycin recipients (3.6%) than of erythromycin recipients (8.2%) (P 0.042). Adverse events reported in at least 2% of patients, regardless of relationship to study drug, are listed in Table V. No deaths were reported during the course of the study. Four serious adverse events occurred, none of which was related to study drug administration. In dirithromycin recipients, one case each of cellulitis and apnoea secondary to congestive heart failure occurred, and in erythromycin recipients, one case each of cellulitis and myocardial infarction occurred. Four patients in each treatment group discontinued treatment early because of adverse events considered to be related to the study drug. In the dirithromycin group, these events were diarrhoea, stomach pain, nausea and rash. In the erythromycin group, these events were vomiting, nausea (two patients) and gastrointestinal discomfort. Number of patients (%) Event Abdominal pain Diarrhoea Headache Dyspepsia Nausea Pain dirithromycin (n 220) 18 (8.2%) 14 (6.4%) 12 (5.5%) 11 (5.0%) 8 (3.6%) 4 (1.8%) erythromycin (n 219) 17 (7.8%) 20 (9.1%) 13 (5.9%) 4 (1.8%) 18 (8.2%) 9 (4.1%) P 0.871 0.278 0.828 0.067 0.042 0.157 Analysis of clinical laboratory data revealed no statistically significant differences between the treatment populations in mean values and no clinically significant alterations in laboratory parameters that were attributed to study drug. Compliance Ten of 220 patients (4.5%) in the dirithromycin group and 27 of 219 (12.3%) patients in the erythromycin group returned 20% of their prescribed medication. Comparison 260 Dirithromycin and erythromycin in SSTI of treatment groups, using active therapy as the denominator, revealed a statistically significant difference in the distribution of percentage of drug returned (Pearson 2 12.12, 5 DF, P 0.033). However, when treatment groups were compared with respect to percentage of drug returned using total number of tablets (active and placebo) dispensed as the denominator, similar results were seen between groups. Discussion In this double-blind, randomized, multicentre study, dirithromycin (500 mg daily for 5 days) was as effective as erythromycin (250 mg q 6h for 7 days) for skin and soft tissue infections. Thus, a shorter course of once-daily therapy with dirithromycin demonstrated efficacy similar to conventional therapy with erythromycin. These results support the findings of Derriennic & Escande,18 who reported no statistically significant differences in clinical or bacteriological efficacy between dirithromycin 500 mg daily for 7 days and erythromycin 250 mg q 6h for 7 days in two large double-blind, randomized, multicentre studies of skin and soft tissue infections. The first study, conducted in North America, evaluated 156 patients treated with dirithromycin and 127 patients treated with erythromycin. Post-therapy responses were identical between the two treatment groups, with 94% of patients clinically cured or improved and 87% of infecting pathogens eradicated. At the late post-therapy evaluation, 132 of 135 (97.8%) dirithromycin recipients and 104 of 114 (91.2%) erythromycin recipients were clinically cured or improved, while the pathogen was eradicated from 126 (93.3%) and 99 (86.8%) patients, respectively. The second study, conducted in Europe, evaluated a total of 100 dirithromycin recipients and 99 erythromycin recipients. More than 95% of patients in each group had a favourable clinical response at both the post-therapy and late posttherapy evaluations. Favourable bacteriological responses were achieved by 87 of 100 (87%) dirithromycin recipients and 88 of 99 (89%) erythromycin recipients post-therapy, and by 87 of 91 (95.6%) and 84 of 92 (91.3%) recipients, respectively, at the late post-therapy evaluation. In the present study, headache and gastrointestinal symptoms were reported by a lower proportion of dirithromycin recipients (3.6%) than erythromycin recipients (8.2%) (P 0.042). In the two studies reported by Derriennic & Escande,18 nausea was also less common with dirithromycin therapy (1.6% and 5.6%) than with erythromycin therapy (2.0% and 7.3%), although this difference was not statistically significant. Failure to comply with the prescribed treatment regimen is a common cause of treatment failure and represents a significant cost to healthcare systems by leading to recurrence of illness, additional physician and pharmacy visits, and hospital admission.19 The present study shows an improvement in patient compliance with dirithromycin. Studies have reported that compliance decreases with increased frequency of administration and that as many as 60% of patients do not comply with four-times-daily administration regimens.20,21 To improve patient compliance, Feldman & DeTullio19 recommend selecting treatments that have the least likelihood of causing adverse effects and that can be administered once daily. Thus, the less frequent dosing of dirithromycin may explain some of the increased compliance in dirithromycin recipients. In this study, in which the patients took the same number of pills over a 7 day period, dirithromycin recipients had a higher compliance than erythromycin recipients. Also, the higher compliance in dirithromycin recipients may be explained by the lower incidence of nausea (3.6% versus 8.2%; P 0.042). For patients with skin and soft tissue infections not requiring hospitalization, cephalosporins, macrolides and β-lactam penicillins provide coverage for the usual pathogens, S. aureus and S. pyogenes. When clinical and bacteriological efficacy are equivalent, few side effects and ease of administration are attractive to physicians and patients because they should enhance compliance and diminish adverse events. Thus, in the treatment of skin and soft tissue infections, dirithromycin 500 mg daily for 5 days is at least therapeutically equivalent in efficacy to, and causes significantly less nausea than, erythromycin 250 mg every 6 h for 7 days. In addition, dirithromycin’s once-daily dosing may enhance patient compliance. Acknowledgements The authors wish to thank Karen Burkey, Sarah Nehrt and Michael Benton, PhD for preparation of the manuscript. This work was supported by Eli Lilly and Company, Indianapolis, IN, USA. References 1. Bass, J. W. (1992). Treatment of skin and skin structure infections. Pediatric Infectious Disease Journal 11, 152–5. 2. Kahn, R. M. & Goldstein, E. J. (1993). Common bacterial skin infections. Diagnostic clues and therapeutic options. Postgraduate Medicine 92, 175–82. 3. Parish, L. C. & Witkowski, J. A. (1991). Systemic management of cutaneous bacterial infections. American Journal of Medicine 91, Suppl. 6A, 106S–10S. 4. Waldvogel, F. (1995). Staphylococcus aureus. In Principles and Practices of Infectious Diseases, 4th edn, (Bennet, J. E., Dolin, R. & Mandell, G. L., Eds), pp. 1754–76, Churchill Livingstone, New York. 5. Hooper, D. C. & Wolfson, J. S. (1993). Adverse effects. In Quinolone Antimicrobial Agents, 2nd edn, (Hooper, D. C. & Wolfson, J. S., Eds), pp. 489–512. American Society for Microbiology, Washington, DC. 6. Gentry, L. O. (1993). Treatment of skin and soft tissue infections with quinolone antimicrobial agents. In Quinolone Antimicrobial 261 M. M. Wasilewski et al. Agents, 2nd edn, (Hooper, D. C. & Wolfson, J. S., Eds) pp. 413–22. American Society for Microbiology, Washington, DC. 7. Hardy, D. J., Hensey, D. M., Beyer, J. M., Vojtko, C., McDonald, E. J. & Fernandes, P. B. (1988). Comparative in vitro activities of new 14-, 15-, and 16-membered macrolides. Antimicrobial Agents and Chemotherapy 32, 1710–9. 8. Yu, K. W. & Neu, H. C. (1990). In vitro activity of dirithromycin (LY 237216) compared with activities of other macrolide antibiotics. Antimicrobial Agents and Chemotherapy 34, 1839–42. 9. Bauernfeind, A. (1993). In-vitro activity of dirithromycin in comparison with other new and established macrolides. Journal of Antimicrobial Chemotherapy 31, Suppl. C, 39–49. 10. Kirst, H. A. & Sides, G. D. (1989). New directions for macrolide antibiotics: pharmacokinetics and clinical efficacy. Antimicrobial Agents and Chemotherapy 33, 1419–22. 11. Sides, G. D., Cerimele, B. J., Black, H. R., Busch, U. & DeSante, K. A. (1993). Pharmacokinetics of dirithromycin. Journal of Antimicrobial Chemotherapy 31, Suppl. C, 65–75. 12. Kirst, H. A. & Sides, G. D. (1989). New directions for macrolide antibiotics: structural modifications and in vitro activity. Antimicrobial Agents and Chemotherapy 33, 1413–8. 13. Bergogne-Bérézin, E. (1993). Tissue distribution of dirithromycin: comparison with erythromycin. Journal of Antimicrobial Chemotherapy 31, Suppl. C, 77–87. 14. Watkins, V. S., Polk, R. E. & Stotka, J. L. (1997). Drug interactions of macrolides: emphasis on dirithromycin. Annals of Pharmacotherapy 31, 349–56. 15. National Committee for Clinical Laboratory Standards. (1993). Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically, Third Edition: Approved Standard M7-A3. NCCLS, Villanova, PA. 16. National Committee for Clinical Laboratory Standards. (1993). Performance Standards for Antimicrobial Disk Susceptibility Tests— Fifth Edition: Approved Standard M2-A5. NCCLS, Villanova, PA. 17. Beam, T. R., Gilbert, D. N. & Kunin, C. M. (1992). General guidelines for the clinical evaluation of anti-infective drug products. Infectious Diseases Society of America and the Food and Drug Administration. Clinical Infectious Diseases 15, Suppl. 1, S5–32. 18. Derriennic, M. & Escande, J. P. (1993). Dirithromycin in the treatment of skin and skin structure infections. Journal of Antimicrobial Chemotherapy 31, Suppl. C, 159–68. 19. Feldman, J. A. & DeTullio, P. L. (1994). Medication noncompliance: an issue to consider in the drug selection process. Hospital Formulary 29, 204–11. 20. Ayd, F. J. (1974). Single daily dose of antidepressants. Journal of the American Medical Association 230, 263–4. 21. Grob, P. R. (1992). Antibiotic prescribing practices and patient compliance in the community. Scandinavian Journal of Infectious Diseases Supplementum 83, 7–14. Received 13 August 1999; returned 22 October 1999; revised 28 February 2000; accepted 20 March 2000 262