Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
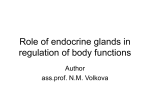
0021-972X/06/$15.00/0 Printed in U.S.A. The Journal of Clinical Endocrinology & Metabolism 91(6):2389 –2395 Copyright © 2006 by The Endocrine Society doi: 10.1210/jc.2005-2480 Treatment with Drugs Able to Reduce Iodine Efflux Significantly Increases the Intracellular Retention Time in Thyroid Cancer Cells Stably Transfected with Sodium Iodide Symporter Complementary Deoxyribonucleic Acid Rossella Elisei, Agnese Vivaldi, Raffaele Ciampi, Pinuccia Faviana, Fulvio Basolo, Ferruccio Santini, Claudio Traino, Furio Pacini, and Aldo Pinchera Department of Endocrinology and Metabolism, Section of Endocrinology (R.E., A.V., R.C., F.S., A.P.); Department of Oncology, Division of Pathology III (P.F., F.B.); and Service of Radiation Safety, South Chiara Hospital (C.T.), University of Pisa, 56124 Pisa, Italy; Department of Internal Medicine, Endocrinology and Metabolism, and Biochemistry, University of Siena (F.P.), 53100 Siena, Italy; and AMBISEN Center, High Technology Center for the Study of the Environmental Damage of the Endocrine and Nervous Systems, University of Pisa (A.P.), 56100 Pisa, Italy Context: One of the major limits of gene therapy with sodium iodide symporter (NIS), which enables cells to be subjected to radioiodine therapy, is that NIS-transfected cells rapidly release the intracellular iodine. Methods: We transfected human anaplastic (FRO) and medullary (TT) thyroid cancer-derived cell lines that were unable to take up iodine with human NIS cDNA. The possibility of increasing the iodine retention time by treating the transfected clones with myricetin, lithium, 17-(allylamino)-17-demethoxygeldanamycin (17-AAG), and 4,4⬘-diisothiocyanatostilbene-2,2⬘-disulfonic acid (DIDS) was explored. Results: We obtained 19 FRO and 16 TT clones stably transfected with NIS. Twelve of 19 FRO and nine of 16 TT clones expressed the full-length NIS mRNA; 11 of 12 FRO and four of nine TT clones were O NE OF THE main functions of the thyroid follicular cell is its ability to take up iodine, which is fundamental for the thyroid hormone synthesis (1). Sodium iodide symporter (NIS) is the plasma membrane protein involved in the uptake and active transportation of iodine from the blood into the follicular cell (2). Because this property may be also retained after malignant transformation, the ability to take up iodine represents the major tool for both diagnosis and treatment of thyroid cancer (3). Two types of well-differentiated thyroid cancer, papillary and follicular [differentiated thyroid cancer (DTC)], arise from follicular cell. Although the overall 5-yr survival rate for DTC is high, about 20% of patients develop an aggressive First Published Online March 14, 2006 Abbreviations: 17-AAG, 17-(Allylamino)-17-demethoxygeldanamycin; AIT, apical iodide transporter; DIDS, 4,4⬘-diisothiocyanatostilbene2,2⬘-disulfonic acid; DTC, differentiated thyroid cancer; FRTL-5, Fisher rat thyroid L-5; h, human; hsp90, 90-kDa heat shock protein; NIS, sodium iodide symporter; PDS, pendrin. JCEM is published monthly by The Endocrine Society (http://www. endo-society.org), the foremost professional society serving the endocrine community. able to take up radioiodine and correctly expressed NIS protein on the plasma membrane. Kinetic analysis of iodide uptake in the two clones (FRO-19 and TT-2) with the highest uptaking activity revealed that the plateau was reached after 30 min by FRO-19 and after 60 min by TT-2. The t1/2 of the iodide efflux was 9 min in FRO-19 and 20 min in TT-2. The treatment of the two cell lines with four different drugs revealed that DIDS and 17-AAG, but not myricetin and lithium, significantly increased the intracellular iodide retention time in FRO19, but not in TT-2. Conclusions: We showed that 17-AAG and DIDS prolong the retention time of 131I in NIS-transfected thyroid tumoral cells, thus reinforcing the hope of using this approach for future clinical application, especially in patients with thyroid carcinoma who are no longer responsive to conventional therapy. (J Clin Endocrinol Metab 91: 2389 –2395, 2006) disease, with local recurrence and distant metastases, as a consequence of their progressive inability to take up radioiodine (4). During the dedifferentiation process, the tumor progressively loses the expression of the differentiation genes, starting with the loss of NIS and continuing with the loss of thyroglobulin, thyroperoxidase, and TSH receptor (5). Follicular cancer, poorly DTC, and undifferentiated or anaplastic thyroid cancer have a much worse prognosis. Intermediate clinical behavior is observed in medullary thyroid cancer originating from parafollicular C cells. Conventional chemotherapy and radiotherapy are poorly effective for the treatment of these advanced and aggressive thyroid tumors (6, 7). NIS gene cloning (8, 9) has raised the possibility of transfecting NIS cDNA in cancer cells with the aim to induce functional NIS expression and, as a consequence, the ability to concentrate iodine. Radioiodine treatment of NIS-transfected cells could thus be reconsidered (10, 11). The major problem of this therapeutic approach is that these cells are deprived of the machinery responsible for iodine organification (12), and intracellular iodine is rapidly released (13–15). 2389 2390 J Clin Endocrinol Metab, June 2006, 91(6):2389 –2395 A way to overcome this problem might be to increase radioiodine retention time within the cell by blocking iodine efflux. Several drugs have been previously shown to be able to reduce iodine efflux in normal or malignant transformed thyroid cells (16 –19). In this study we tested four of these drugs [myricetin (20), lithium chloride (21), 17-(allylamino)17-demethoxygeldanamycin (17-AAG) (22), and 4,4⬘-diisothiocyanatostilbene-2,2⬘-disulfonic acid (DIDS) (23)] for their ability to reduce the iodine efflux in both normal and tumoral follicular cells. To this purpose, we transfected two human thyroid cancer-derived cell lines, anaplastic (FRO) and medullary (TT), with human NIS cDNA. After selecting the clones with the highest iodine uptake, the possibility of increasing the iodine retention time by treating the cells with myricetin, lithium, 17-AAG, and DIDS was explored. Materials and Methods Human (h) NIS-FL cDNA stable transfection FRO and TT cell lines were used for transfection experiments. Cell culture conditions were described previously (12). For transfection, cells were plated at the density of 1 ⫻ 105 in six-well plates and stably transfected with full-length hNIS cDNA in pcDNA3 vector (gift from Dr. S. Jhiang, Departments of Physiology and Internal Medicine, Ohio State University, Columbus, OH) and with the empty vector as a control. Transfection was performed with a lipid mixture, Lipofectamine (Invitrogen Life Technologies, Inc., Milan, Italy). After selection with 400 g/ml neomycin for 15 d, well-isolated clones were picked up by the cylinder technique, isolated, then cultured for additional experiments. Stably transfected cell culture was continued in 400 g/ml neomycin (Invitrogen Life Technologies, Inc.)-supplemented medium. RNA extraction, RT-PCR, and NIS real-time quantitative RT-PCR Total RNA was isolated and reverse transcribed in cDNA as previously described (12). cDNA was then amplified by PCR using specific primers for a ubiquitous gene (a portion of n-Ras) as a control and for NIS gene. The primers and conditions used for PCR are reported in Table 1. PCR products were electrophoresed in a 2% agarose gel, then transferred to a nylon membrane. Each filter was hybridized with internal probes (Table 1) specific for each amplified fragment and revealed using a chemiluminescent method (ECL-CDP star detection, Amersham Biosciences, Milan, Italy). To perform quantitative RT-PCR for NIS-mRNA, we used Real-Time Sequence Detection System 7700 (Applied Biosystems, Foster City, CA) (24). A serial dilution of an NIS-containing plasmid was used as the standard curve. Two primer pairs were used, one specific for the amino and one specific for the carboxyl terminus of NIS protein to ensure that the full-length mRNA was present. The ubiquitous gene glyceraldehyde-3-phosphate dehydrogenase was also amplified for normalization of the samples. Primers for glyceraldehyde-3-phosphate dehydrogenase were obtained from Applied Biosystems; the NIS primers are reported in Table 1. Samples omitting reverse transcriptase and cDNA were Elisei et al. • Iodine Uptake in NIS-Transfected Thyroid Cells included in each run as controls of potential laboratory and/or assay contamination. NIS immunocytochemistry Cells were detached by trypsin, centrifuged, fixed by formalin, and included by paraffin in blocks. Sections (5 m) were cut, deparaffined, and rehydrated. All slides were subjected to antigen retrieval using 10% citrate buffer. Washes were performed with PBS for 5 min. Endogenous peroxide activity was blocked with 5% H2O2 for 15 min. Sections were incubated with the purified hNIS antibody (gift from Brahms Diagnostica GmbH, Berlin, Germany) at a 1:1000 dilution at room temperature for 1 h, then subjected to avidin and biotin block for 20 min each, to streptavidin peroxidase for 10 min, and to 3,3⬘-diaminobenzidine substrate chromogen for 5 min. The sections were counterstained with hematoxylin. Iodine uptake and efflux All transfected clones positive for NIS mRNA expression and negative controls were analyzed for their ability to take up iodine according to a method currently used in the laboratory (12). Radioactivity in each sample was counted in a ␥-counter as counts per minute. Cell number was also determined, and iodine uptake was expressed as picomoles of I⫺ per 106 cells. Clones able to take up iodine were then studied to monitor both the kinetics and the specificity of iodine uptake by repeating the iodine uptake experiments at different times (0, 2, 5, 10, 15, 30, 45, and 60 min) and in the presence of 10 m sodium perchlorate. Iodine efflux was studied by incubating cells for 45 min at 37 C in Hanks’ balanced salt solution incubation buffer plus 0.1 Ci Na125I and 1 m sodium iodide. After the incubation, radioactive buffer was replaced with nonradioactive buffer every 3 min for 30 min, and all supernatants were collected. Cells were lysed after the last supernatant removal. Radioactivity was counted in both supernatants and lysed cells. Total radioactivity at the beginning of efflux (100%) was calculated by adding the counts per minute found in each supernatant to those found in the lysed cells. Iodine efflux was measured both before and after treatment with myricetin, lithium, 17-AAG, and DIDS in two of the positive FRO and TT clones transfected with NIS and able to take up iodine. Myricetin (10 mm stock solution), lithium chloride (1 m stock solution), 17-AAG (3 mm stock solution), and DIDS (100 mm stock solution; all from SigmaAldrich Corp., Milan, Italy) were dissolved in 20 l dimethylsulfoxide/ 800 l absolute ethanol, in distilled water, in dimethylsulfoxide, and in 0.1 potassium bicarbonate, respectively. Cells were treated with myricetin 50 m for 96 h, with 10 mm lithium chloride for 24 h, 17-AAG 3 m for 24 h, and with 1 mm DIDS for 1 h. The Fisher rat thyroid L-5 (FRTL-5) cell line was used as a control in all efflux experiments. FRTL-5 cells were cultured following standard conditions (25). All experiments were performed in triplicate and repeated three times. Dosimetry Because the in vivo therapy is usually performed by administrating I, we calculated the transfected cell-absorbed dose per unit of administered activity (Gy/MBq) for 131I based on the evidence that the physic half-life of radioiodine has no influence on radioiodine kinetics at cellular levels. 131 TABLE 1. PCR primers and probes used for the qualitative RT-PCR of N-ras and NIS mRNA (rows 1 and 2) and for quantitative realtime RT-PCR of both amino-terminal (row 3) and carboxyl-terminal (tow 4) portions of NIS mRNA Gene Primer forward Primer reverse Probe N-ras ATGACTGAGTACAAACTG AGGAAGCCTTCGCCTGTCCT CCTCATCCTGAACCAAGTGACC NIS CTTCTGAACTCGGTCCTCAC TCCAGAATGTATAGCGGCTC CCTCATCCTGAACCAAGTGACC NIS-NH2 GCTCTTCATGCCCGTCTTCT GGCTGAAGCGCATCTCCA FAM-TGGGCCTCACCAGCACCTACGAGTACTAMRA NIS-COOH CCATCCTGGATGACAACTTGG AAAAACAGACGATCCTCATTG FAM-AGAACTCCCCACTGGAAACAAGAAGCCCTAMRA a Conditions Annealing temperature, 55 C; 1.5 mM MgCl2 Annealing temperature, 56 C; 1 mM MgCl2 a a Quantitative real-time PCR following standard conditions. FAM, 6-Carboxyfluorescein; TAMRA, tetramethylrhodamine. Elisei et al. • Iodine Uptake in NIS-Transfected Thyroid Cells The calculation of the cell absorbed dose per unit of administered activity, DC(Gy/MBq), was made using the equation: DC ⫽ SC4C, where SC-C are the S-factors for 7 m diameter cells (26). was calculated taking into account that the radioiodine kinetics in the cells can be considered monoexponential, according to the following equation: A(t) ⫽ A0 exp(t/), where A(t) is the radioiodine activity in the cell, A0 is the administered activity, t is time, and is the cumulated activity per unit of administered activity. It is worth noting that the calculation of DC(Gy/MBq) was based on the following hypotheses: 1) radioiodine activity is homogeneously distributed in the cell culture; 2) dose is calculated taking into account only the self-irradiation of the cell, neglecting the effect of the surrounding radioactivity; and 3) radioiodine activity is considered uniformly distributed into the cell, i.e. the different distributions of the activity in nucleus, cytoplasm, and cell surface are neglected. Statistical analysis Statistical analysis was performed by ANOVA for repeated measures test and Student’s t test with Bonferroni correction using StatView 4.5 software (Abacus Concepts, Inc., Berkeley, CA). Results were considered statistically significant at P ⬍ 0.05. Results Nineteen FRO and 16 TT clones transfected with hNIS and two FRO and six TT clones transfected with the empty vector were isolated after NIS stable transfection and neomycin selection. Qualitative and quantitative RT-PCR of the transfected clones, performed with specific primers for the amino and carboxyl termini of the NIS gene, revealed that 12 of 19 FRO and nine of 16 TT clones expressed the full-length NIS mRNA. As expected, hNIS mRNA was not detected in clones transfected with the empty vector. All hNIS mRNA-expressing clones and clones transfected with the empty vector were then subjected to radioiodine uptake analysis; 11 of 12 FRO and four of nine TT clones showed the ability to take up iodide (FRO clones from 2,800 to 56,000 cpm/106 cells and TT clones from 7,200 and 55,000 cpm/106 cells; Fig. 1). As a control, iodine uptake of the FRTL-5 cell line was also measured (⬃10,000 cpm/106 cells). As expected, none of the clones transfected with the empty vector showed iodine uptake. The clones FRO-19 and TT-2, J Clin Endocrinol Metab, June 2006, 91(6):2389 –2395 2391 which showed the highest levels of iodine uptake (56,000 and 55,000, respectively) and coincided with clones with the highest copy number of NIS mRNA, were selected for additional experiments after performing a perchlorate inhibition test, demonstrating that the iodine uptake was NIS mediated. The immunocytochemistry with anti-NIS antibody showed strong positive staining on the plasma membrane of FRO and TT clones positive for both NIS mRNA expression and iodine uptake (Fig. 2, A and D). Weak cytoplasmic staining was detected in clones that were positive for NIS mRNA expression but unable to take up iodine (Fig. 2, B and E). Negative results were obtained in negative controls (wildtype FRO and TT cells; Fig. 2, C and F). Iodine uptake reached the steady-state level (plateau) after about 30 and 60 min in FRO-19 and TT-2 cells, respectively (Fig. 3A). A rapid efflux of iodine was observed in FRO-19 cells, because about 50% of the cellular radioactivity was released into the medium in about 9 min (t1/2 ⫽ 9 min), whereas a slower efflux was detected in TT-2 cells (t1/2 ⫽ 20 min; Fig. 3B). As shown in Table 2, treatment with 17-AAG and DIDS caused a significant increase in iodine uptake at a plateau in FRTL-5 (1.5- and 1.5-fold increases, respectively; P ⬍ 0.05). In FRO-19 cells, the same effect was observed after treatment with DIDS (1.2-fold increase). Total iodine uptake was not affected by treatment with any of the four drugs in TT-2 cells. As shown in Table 3, myricetin, lithium, 17-AAG, and DIDS significantly reduced iodine efflux in FRTL-5 cells (P ⫽ 0.003 to P ⬍ 0.0001). Thirty minutes after removal of 125I, intracellular radioactivity was increased 20% when cells were treated with lithium and 17-AAG, 25% when cells were treated with DIDS, and 51% when cells were treated with myricetin (compared with untreated cells). When drugs were tested for their ability to affect iodine efflux in cell lines transfected with NIS cDNA, iodine retention was significantly (P ⬍ 0.0001) increased by both DIDS and 17-AAG in FRO-19 cells (Fig. 4). The intracellular iodine content was significantly higher as early as 15 min after FIG. 1. Iodide uptake in wild-type and transfected FRO and TT clones. Eleven of 12 FRO and four of nine TT clones showed the ability to take up iodide (FRO clones from 2,800 to 56,000 cpm/106 cells and TT clones from 7,200 and 55,000 cpm/106 cells). As a control, iodine uptake of the FRTL-5 cell line was also measured. Clones FRO-19 (A) and TT-2 (B) were chosen for additional experiments. 2392 J Clin Endocrinol Metab, June 2006, 91(6):2389 –2395 Elisei et al. • Iodine Uptake in NIS-Transfected Thyroid Cells FIG. 2. Immunocytochemistry with anti-NIS antibody of FRO-19 and TT-2 clones stably transfected with fulllength NIS cDNA. Clones able to express NIS mRNA and take up iodide (A and D) showed correct localization of NIS protein on the plasma membrane; clones able to express NIS mRNA, but not to take up iodide (B and E), showed weak cytoplasmic staining; nontransfected clones (C and F) did not show any staining. removal of radioiodine from the medium compared with that in untreated cells (⫹29% and ⫹23% in DIDS- and 17-AAGtreated cells, respectively), and it was almost doubled at 30 min (⫹103% and ⫹69%, respectively; Table 3). No significant effect on iodine retention was produced by myricetin or lithium in FRO-19 cells. No effect was produced by any drug in the TT-2 cell line. As shown in Table 4, calculation of the administered activity in the FRO-19 cell line (control vs. cells treated with FIG. 3. Iodide kinetics of FRO-19 and TT-2 clones. A, Time course of iodide uptake, showing a plateau at 30 min for FRO-19 and at 60 min for TT-2. B, Iodide efflux, showing a rapid efflux of iodine in FRO-19 cells (t1/2 ⫽ 9 min) and a slower efflux in TT-2 cells (t1/2 ⫽ 20 min). Values are the means of three replicate determinations. 17-AAG and DIDS) showed a significantly higher dose of radioiodine in treated cells vs. controls (P ⬍ 0.01). Discussion Although NIS gene therapy is an attractive approach for the treatment of dedifferentiated and/or undifferentiated thyroid carcinomas, there are two major limits that reduce the possibility of using radioiodine as a therapeutic agent (13, Elisei et al. • Iodine Uptake in NIS-Transfected Thyroid Cells J Clin Endocrinol Metab, June 2006, 91(6):2389 –2395 2393 TABLE 2. Increase in iodine uptake, expressed as picomoles per 106 cells, in cells treated with four different drugs FRTL-5 FRO-19 TT-2 Untreated Myricetin 17-AAG Lithium DIDS 48.7 ⫾ 9.3 325.5 ⫾ 3.3 909.6 ⫾ 80.8 60.0 ⫾ 5.4 (1.2) 263.3 ⫾ 13.2 (0.8) 1045.3 ⫾ 53.3 (1.1) 72.7 ⫾ 5.3 (1.5)a 281.3 ⫾ 12.0 (0.8) 1059.3 ⫾ 219.9 (1.1) 42.3 ⫾ 1.2 (0.9) 343.2 ⫾ 14.6 (1.0) 661.5 ⫾ 5.4 (0.7) 70.9 ⫾ 7.1 (1.5)a 401.3 ⫾ 16.1 (1.2)a 754.6 ⫾ 61.9 (0.8) The fold increases are given in parentheses. All experiments were performed in triplicate; the results of one of the three experiments are reported. a P ⬍ 0.05. 27): 1) the poor efficiency of NIS transfection and incorrect localization of the encoded protein; and 2) the short time of iodide retention within the cell. Indeed, in vivo studies have shown that radioiodine treatment does not significantly change the volume of tumors induced in mice after sc injection of NIS-transfected thyroid cells (14). Regarding the problem of transfection efficiency, we observed a quite important difference in the two cell lines, FRO and TT. This phenomenon is likely to be dependent on the different cell types and suggests that the cell system to be transfected should be accurately chosen for clinical applications. In this regard, literature data are limited. However, a transfection efficiency of about 16% has been reported in the transfection of both prostate and thyroid cancer cell lines (28, 29), which is much lower than those obtained by us in FRO (11 of 19; 58%) and TT (four of 16; 25%) cells. It is likely that a different delivery system of the transfected gene (e.g. adenovirus or retrovirus) might be more efficient (15). Furthermore, we observed that in several NIS mRNA-expressing clones, the NIS protein was not on the plasma membrane and was not functional. We can speculate that clones expressing NIS mRNA but unable to take up iodide were subjected to posttranscriptional gene silencing. This phenomenon is very common in transgenic plants and is due to a mechanism also present in animal cells that has the final aim of defending the cell from foreign DNA (30, 31). Although we think that these technical problems should be taken into account and considered as possible limiting factors of this approach, several promising data on NIS gene transfer from various groups have been reported in different tumor cell lines (13, 32, 33). Regarding the problem of the short retention time of iodine in transfected cells, we demonstrated for the first time that treatment with 17-AAG and DIDS of FRO cells, derived from a human anaplastic thyroid carcinoma and transfected with NIS cDNA, is able to significantly reduce iodide efflux, producing an increase in the iodide retention time that improves the killing potential of radioiodine treatment. The same drugs were not able to increase iodide retention in TT cells derived from a human medullary thyroid carcinoma and transfected with NIS cDNA. The reason for this discrepancy may be that FRO and TT cell lines derive from different thyroid tumor histotypes. The mechanism of iodide efflux is still not fully understood, and several unknown proteins are likely to be involved (34). At present, only pendrin (PDS) and the recently characterized protein apical iodide transporter (AIT) have TABLE 3. Effect of treatment of FRTL-5 and FRO-19 cells with the four drugs on radioiodide efflux Time (min) FRTL-5 cells 3 6 9 12 15 18 21 24 27 30 P value FRO-19 cells 3 6 9 12 15 18 21 24 27 30 P value % Intracellular radioactivity Untreated Myricetin Lithium 17-AAG DIDS 49.7 ⫾ 3.5 31.6 ⫾ 0.3 23.5 ⫾ 2.3 19.0 ⫾ 3.6 14.3 ⫾ 2.2 11.7 ⫾ 2.4 9.5 ⫾ 2.3 7.9 ⫾ 2.3 6.0 ⫾ 2.1 4.4 ⫾ 2.1 55.7 ⫾ 3.3 (12) 36.1 ⫾ 2.6 (14) 27.5 ⫾ 2.7 (17) 22.5 ⫾ 4.8 (18) 18.9 ⫾ 5.2 (32) 15.8 ⫾ 5.0 (34) 13.5 ⫾ 4.9 (41) 10.8 ⫾ 4.5 (37) 8.7 ⫾ 4.6 (45) 6.6 ⫾ 4.0 (51) ⬍0.0001 55.0 ⫾ 4.1 (10) 36.8 ⫾ 1.7 (16) 27.6 ⫾ 1.7 (17) 22.1 ⫾ 3.4 (16) 17.9 ⫾ 3.9 (25) 15.2 ⫾ 4.5 (30) 12.5 ⫾ 4.4 (31) 10.3 ⫾ 4.3 (31) 7.1 ⫾ 1.4 (18) 5.3 ⫾ 1.6 (20) ⬍0.0001 54.2 ⫾ 6.3 (9) 37.1 ⫾ 4.2 (17) 28.2 ⫾ 2.9 (20) 22.7 ⫾ 3.0 (19) 19.0 ⫾ 3.5 (32) 14.1 ⫾ 1.4 (20) 11.8 ⫾ 1.9 (24) 9.4 ⫾ 2.1 (20) 7.6 ⫾ 2.2 (27) 5.3 ⫾ 2.1 (20) 0.0004 54.2 ⫾ 5.5 (9) 35.4 ⫾ 2.5 (12) 25.0 ⫾ 1.6 (6) 19.9 ⫾ 0.5 (5) 16.2 ⫾ 1.7 (13) 13.4 ⫾ 2.4 (15) 11.3 ⫾ 2.4 (18) 9.3 ⫾ 2.7 (18) 7.3 ⫾ 2.8 (21) 5.8 ⫾ 3.0 (25) 0.0033 80.0 ⫾ 1.4 62.7 ⫾ 1.9 48.7 ⫾ 2.8 38.2 ⫾ 2.3 29.7 ⫾ 2.1 23.2 ⫾ 1.7 17.9 ⫾ 1.9 13.9 ⫾ 1.9 10.5 ⫾ 1.8 7.5 ⫾ 1.7 76.1 ⫾ 4.7 (⫺5) 58.9 ⫾ 5.9 (⫺6) 45.4 ⫾ 6.2 (⫺6) 35.0 ⫾ 5.2 (⫺8) 27.1 ⫾ 4.5 (⫺9) 20.7 ⫾ 4.1 (⫺10) 15.6 ⫾ 3.2 (⫺13) 11.9 ⫾ 2.6 (⫺14) 8.9 ⫾ 2.5 (⫺15) 6.6 ⫾ 2.3 (⫺13) 77.3 ⫾ 3.4 (⫺3) 61.1 ⫾ 4.7 (⫺2) 48.1 ⫾ 5.1 (⫺1) 37.7 ⫾ 3.1 (⫺1) 30.0 ⫾ 2.4 (0) 23.6 ⫾ 2.1 (1) 18.3 ⫾ 1.8 (2) 14.3 ⫾ 1.3 (3) 11.0 ⫾ 1.2 (4) 8.1 ⫾ 1.4 (7) 79.7 ⫾ 4.3 (0) 65.4 ⫾ 5.3 (4) 54.0 ⫾ 5.4 (11) 44.9 ⫾ 4.0 (17) 36.7 ⫾ 3.9 (23)a 30.3 ⫾ 3.1 (30) 24.9 ⫾ 2.7 (39) 20.2 ⫾ 2.4 (45) 16.1 ⫾ 2.5 (53) 12.7 ⫾ 2.6 (69) ⬍0.0001 82.3 ⫾ 2.0 (3) 67.9 ⫾ 4.6 (8) 56.3 ⫾ 5.3 (16) 46.6 ⫾ 4.7 (22) 38.6 ⫾ 4.5 (29)a 32.1 ⫾ 4.7 (38) 26.8 ⫾ 4.9 (50) 22.2 ⫾ 4.9 (60) 18.5 ⫾ 4.8 (76) 15.3 ⫾ 4.8 (103) ⬍0.0001 The values are the mean ⫾ SD of three experiments, each performed in triplicate. The increase (%) in intracellular radioactivity in treated vs. untreated cells is shown in parentheses. a The intracellular iodine content became significantly higher in treated vs. untreated cells as early as 15 min. 2394 J Clin Endocrinol Metab, June 2006, 91(6):2389 –2395 Elisei et al. • Iodine Uptake in NIS-Transfected Thyroid Cells FIG. 4. Iodide efflux of FRO-19 cells under basal conditions (red line) and after treatment with 17-AAG (green line) and DIDS (blue line). Iodine retention was significantly increased by both DIDS and 17AAG. The values are the means of three experiments, each performed in triplicate (SD are indicated by bars). been recognized as passive iodide transporters (35, 36). It has been shown that DIDS directly inhibits iodide efflux by interfering with the iodide-specific channel located at the apical pole of thyroid cells (19). Unfortunately, that study was performed before cloning of the genes coding for the two above-mentioned proteins (PDS and AIT), and we cannot exclude or confirm that, generally speaking, DIDS might act through the inhibition of PDS and/or AIT. However, on the basis of our previous demonstration that the FRO cell line does not express the PDS gene (12), we can exclude an involvement of this gene. Because DIDS is a well-known inhibitor of anionic channels, we can also speculate that the iodide efflux of FRO-19 cells might be mediated by other anionic channels, not specific, but permeable to iodide, which have been demonstrated to be expressed in thyroid cells (37, 38). 17-AAG treatment has recently been demonstrated to decrease the iodide efflux in normal rat thyroid cells, PCCL3 (18). This action seems to be specific for thyroid cells, because it was not observed in other cell lines. We obtained similar results in a cell line derived from normal rat thyroid cells (FRTL-5) and in FRO-19 cells, derived from a human anaplastic thyroid carcinoma and transfected with NIS cDNA. The negative result obtained with the TT-2 cell line treated with 17-AAG confirms a certain specificity of 17-AAG action in decreasing iodide efflux in follicular cells. 17-AAG is also a known inhibitor of the 90-kDa heat shock protein (hsp90), and it is likely that through the inhibition of hsp90, it acts as TABLE 4. Cumulative activity and dose per unit of administered activity of radioiodine (131I) in FRO-19 cells untreated (C) and treated with 17-AAG and DIDS FRO-19 cells C 17-AAG DIDS (min) ⫾ SD a 12.4 ⫾ 0.3 14.9 ⫾ 0.4 15.8 ⫾ 0.7 D (Gy/MBq) ⫾ SD b 0.232 ⫾ 0.006 0.279 ⫾ 0.007c 0.300 ⫾ 0.01c c a values for the three experiences were obtained by fitting the experimental data using the following equation: A(t) ⫽ A0关exp(⫺1/ )t兴. b D(Gy/MBq) ⫽ SC-C . c P ⬍ 0.01 an antineoplastic agent, both by reducing cellular proliferation and by inducing apoptosis. hsp90 is a chaperone for a group of proteins, several of which are involved in cancer proliferation (22). Recently, one of the most important oncogenes for papillary thyroid cancer (RET/PTC1) has been demonstrated to be a client protein of hsp90 (18). The combination of antineoplastic activity with the ability to reduce iodide efflux, as shown by our data, makes 17-AAG a good candidate for the treatment of thyroid cancer, especially when patients are losing the ability to take up iodine. 17-AAG and DIDS were effective in reducing iodide efflux in FRO-19 as well as in FRTL-5 cells. The same approach does not seem to be applicable in the TT cell line, because none of the tested drugs was able to interfere with iodide transport in this cell line. However, by analyzing the efflux kinetics, it appears evident that iodide transport is different in the two cell systems; in fact, FRO-19 cells release half the iodide after 9 min, whereas TT-2 cells release it after about 20 min. This finding is in agreement with our previous report of the expression of the thyroperoxidase gene in TT cells (12) and the recent observation of iodide organification in NIS-transfected TT cells (39). Although we did not evaluate the organification of iodide in the cells, it is conceivable to hypothesize that iodide efflux in TT-2 cells is slower than that in FRO-19 cells because of a partial iodide organification in the first cell type, but not in the latter. As a consequence, in this cell system, it is more conceivable to improve the rate of iodine organification, as previously suggested (40), than to reduce iodine efflux. Nevertheless, other drugs might be explored in the future. As far as the in vivo therapeutic effect is concerned, it could be of interest to determine the lowest absorbed dose per administered activity able to induce cell death and/or damage. To our knowledge, this information is still unknown. However, there are a few studies clearly demonstrating that 131I treatment of mice with xenografted tumors, obtained using NIS-transfected cells, reduced the growth rate and volume of the tumor (13, 32) and/or increased the survival rate of the animal models (33) despite the rapid iodide efflux. Based on these results, we may assume that in our case also a therapeutic effect of 131I treatment could be obtained in an experimental model and could be improved by the simultaneous treatment with 17-AAG or DIDS, as demonstrated by the statistically significant increase in the absorbed dose of 131I. However, because the iodide efflux in vivo might be significantly different from that in vitro, our data have to be confirmed in xenografted animals before hypothesizing about any human therapeutic protocol. In conclusion, in this study we showed that NIS gene therapy, although very promising, may have some technical limitations to be considered before its in vivo application. However, our results indicated that once these limitations have been overcome, certain drugs (i.e. 17-AAG and DIDS) could be used to prolong the retention time of 131I in thyroid tumoral cells transfected with the NIS gene. Thus, our data reinforce the hope of using this approach for future clinical application, especially in those patients with DTC who are no longer responsive to conventional therapy. Elisei et al. • Iodine Uptake in NIS-Transfected Thyroid Cells Acknowledgments We thank Dr. Sissy Jhiang, codirector of the Department of Physiology and Department of Internal Medicine, Ohio State University (Columbus, OH), for the kind gift of NIS full-length cDNA; Dr. Jennifer Cummings for revising the language of the manuscript; and Dr. Lucio Masserini for revising statistics. Received November 14, 2005. Accepted March 3, 2006. Address all correspondence and requests for reprints to: Dr. Rossella Elisei, Department of Endocrinology and Metabolism, Via Paradisa 2, University of Pisa, 56124 Pisa, Italy. E-mail: [email protected]. This work was supported in part by grants from Ministero dell’Istruzione Universitaria e Ricerca Scientifica and Associazione Italiana per la Ricerca sul Cancro. R.E., A.V., R.C., P.F., F.B., F.S., C.T., F.P., and A.P. have nothing to declare. References 1. Braverman, LE, Utiger DL 2000 Werner and Ingbar’s the thyroid: a fundamental and clinical text, 8th Ed. Philadelphia: Lippincott Williams & Wilkins 2. Jhiang SM 2000 Regulation of sodium iodine symporter. Rev Endocr Metab Disord 1:205–215 3. Schlumberger M, Pacini F 1999 Thyroid tumors. Paris: Nucleon Editions; 117–129 4. Arturi F, Russo D, Schlumberger M, Du Villard JA, Caillou B, Vigneri P 1998 Iodine symporter gene expression in human thyroid tumors. J Clin Endocrinol Metab 83:2193–2196 5. Elisei R, Pinchera A, Romei C, Gryczynska M, Pohl V, Maenhaut C, Fugazzola L, Pacini F 1994 Expression of thyrotropin receptor (TSH-R), thyroglobulin, thyroperoxidase and calcitonin messenger ribonucleic acid in thyroid carcinoma: evidence of TSH-R gene transcript in medullary histotype. J Clin Endocrinol Metab 78:867 6. Haugen BR 1999 Management of the patient with progressive radioiodine non-responsive disease. Semin Surg Oncol 16:34 – 41 7. Santini F, Bottici V, Elisei R, Montanelli L, Mazzeo S, Basolo F, Pinchera A, Pacini F 2002 Cytotoxic effects of carboplatinum and epirubicin in the setting of an elevated serum thyrotropin for advanced poorly differentiated thyroid cancer. J Clin Endocrinol Metab 87:4160 – 4165 8. Smanik PA, Liu Q, Furminger TL, Ryu K, Xing S, Mazzaferri EL, Jhiang SM 1996 Cloning of the human sodium iodide symporter. Biochem Biophys Res Commun 226:339 –345 9. Dai G, Levy O, Carrasco N 1996 Cloning and characterization of the thyroid iodide transporter. Nature 379:458 – 460 10. Spitzweg C, Harrington KJ, Pinke LA, Vile RG, Morris JC 2001 The sodium iodide symporter and its potential role in cancer therapy. J Clin Endocrinol Metab 86:3327–3335 11. Chung JK 2002 Sodium iodide symporter: its role in nuclear medicine. J Nucl Med 43:1188 –1200 12. Elisei R, Vivaldi A, Agate L, Ciampi R, Molinaro E, Piampiani P, Romei C, Faviana P, Basolo F, Miccoli P, Capodanno A, Collecchi P, Pacini F, Pinchera A 2005 All-trans retinoic acid treatment inhibits the growth of retinoic acid receptor  messenger ribonucleic acid expressing thyroid cancer cell lines but does not reinduce the expression of thyroid specific genes. J Clin Endocrinol Metab 90:2403–2411 13. Smit JW, Schroder-van der Elst JP, Karperien M, Que I, Stokkel M, van der Heide D, Romijn JA 2002 Iodide kinetics and experimental 131I therapy in a xenotransplanted human sodium iodide symporter transfected human follicular thyroid carcinoma cell line. J Clin Endocrinol Metab 87:1247–1253 14. Shimura H, Haraguchi K, Miyazaki A, Endo T, Onaya T 1997 Iodide uptake and experimental 131I therapy in transplanted undifferentiated thyroid cancer cells expressing the Na⫹/I⫺ symporter gene. Endocrinology 138:4493– 4496 15. Haberkorn U, Henze M, Altmann A, Jiang S, Morr I, Mahmut M, Peschke P, Kubler W, Debus J, Eisenhut M 2001 Transfer of the human NaI symporter gene enhances iodide uptake in hepatoma cells. J Nucl Med 42:317–325 16. Schroder-van der Elst JP, van der Heide D, Romijin JA, Smit JA 2004 Differential effects of natural flavonoids on growth and iodine content in a human Na⫹/I⫺ symporter-transfected follicular thyroid carcinoma cell line. Eur J Endocrinol 150:557–564 17. Koong SS, Reynolds JC, Movius EG, Keenan AM, Ain KB, Lakshman MC, Robbins J 1999 Lithium as a potential adjuvant to 131I therapy of metastatic, well differentiated thyroid carcinoma. J Clin Endocrinol Metab 84:912–916 J Clin Endocrinol Metab, June 2006, 91(6):2389 –2395 2395 18. Marsee DK, Venkateswaran A, Tao H, Vadysirisack D, Zhang Z, Vandre DD, Jhiang SM 2004 Inhibition of heat shock protein 90, a novel RET/PTC1associated protein, increases radioiodine accumulation in thyroid cells. J Biol Chem 279:43990 – 43997 19. Amphoux-Fazekas T, Samih N, Hovsepian S, Aouani A, Beauwens R, Fayet G 1998 DIDS (4,4⬘-diisothiocyanatostilbene-2,2⬘-disulfonic acid) increases iodine trapping, inhibits thyroperoxydase and antagonizes the TSH-induced apical iodine efflux in porcine thyroid cells. Mol Cell Endocrinol 141:129 –140 20. Ong KC, Khoo HE 1997 Biological effects of myricetin. Gen Pharmacol 29: 121–126 21. Urabe M, Hershman JM, Pang XP, Murakami S, Sugawara M 1991 Effect of lithium on function and growth of thyroid cells in vitro. Endocrinology 129: 807– 814 22. Bagatell R, Whitesell L 2004 Altered Hsp90 function in cancer: a unique therapeutic opportunity. Mol Cancer Ther 3:1021–1030 23. Cabantchik ZI, Greger R 1992 Chemical probes for anion transporters of mammalian cell membranes. Am J Physiol 262:C803–C827 24. Elisei R, Vivaldi A, Agate L, Molinaro E, Nencetti C, Grasso L, Pinchera A, Pacini F 2004 Low specificity of blood thyroglobulin messenger ribonucleic acid assay prevents its use in the follow-up of differentiated thyroid cancer patients. J Clin Endocrinol Metab 891:33–39 25. Ambesi Impiombato FS, Parks LAM, Coons HG 1980 Culture of hormonedependent epithelial cells from rat thyroids. Proc Natl Acad Sci USA 77:3455 26. Goddu SM, Rao DV, Howell RW 1994 Multicellular dosimetry for micrometastases: dependence of self-dose versus cross-dose to cell nuclei on type and energy of radiation and subcellular distribution of radionuclides. J Nucl Med 35:521–530 27. Lee WW, Lee B, Kim SJ, Jin J, Moon DH, Lee H 2003 Kinetics of iodide uptake and efflux in various human thyroid cancer cells by expressing sodium iodide symporter gene via a recombinant adenovirus. Oncol Rep 10:845– 849 28. Spitzweg C, Zhang S, Bergert ER, Castro MR, McIver B, Heufelder AE, Tindall DJ, Young CYF, Morris JC 1999 Prostate-specific antigen (PSA) promoter-driven androgen-inducible expression of sodium iodide symporter in prostate cancer cell lines. Cancer Res 59:2136 –2141 29. Smith JWA, Schroder-van der Elst JP, Karperien M, Que I, van der Pluijm G, Goslings B, Romijn JA, van der Heide D 2000 Reestablishment of in vitro and in vivo iodide uptake by transfection of the human sodium iodide symporter (hNIS) in a hNIS defective human thyroid carcinoma cell line. Thyroid 10:939 –943 30. Almeida R, Allshire RC 2005 RNA silencing and genome regulation. Trends Cell Biol 15:251–258 31. Fagard M, Vaucheret H 2000 (Trans)gene silencing in plants: how many mechanisms? Annu Rev Plant Physiol Plant Mol Biol 51:167–194 32. Spitweg C, O’Connor MK, Bergert ER, Tindall DJ, Young CYF, Morris JC 2000 Treatment of prostate cancer by radioiodine therapy after tissue-specific expression of the sodium iodide symporter. Cancer Res 60:6526 – 6530 33. Cho JY, Shen DHY, Yang W, Williams B, Buckwalter TLF, La Perle KMD, Hinkle G, Pozderac R, Kloos R, Nagaraja HN, Barth RF, Jhiang SM 2002 In vivo imaging and radioiodine therapy following sodium iodide symporter gene transfer in animal model of intracerebral gliomas. Gene Ther 9:1139 –1145 34. Rousset BA, Dunn JT 2004 Thyroid hormone synthesis and secretion. In: The thyroid and its diseases, Chap 2. http://www.thyroidmanager.org 35. Royaux IE, Suzuki K, Mori A, Katoh R, Everett LA, Kohn LD, Green ED 2000 Pendrin, the protein encoded by the Pendred syndrome gene (PDS), is an apical porter of iodide in the thyroid and is regulated by thyroglobulin in FRTL-5 cells. Endocrinology 141:839 – 845 36. Rodriguez AM, Perron B, Lacroix L, Caillou B, Leblanc G, Schlumberger M, Bidart JM, Pourcher T 2002 Identification and characterization of a putative human iodide transporter located at the apical membrane of thyrocytes. J Clin Endocrinol Metab 87:3500 –3503 37. Armstrong JW, Cragoe Jr EJ, Bourke JR, Huxham GJ, Manley SW 1992 Chloride conductance of apical membrane in cultured porcine thyroid cells activated by cyclic AMP. Mol Cell Endocrinol 88:105–110 38. Devuyst O, Golstein PE, Sanches MV, Piontek K, Wilson PD, Guggino WB, Dumont JE, Beauwens R 1997 Expression of CFTR in human and bovine thyroid epithelium. Am J Physiol 272:C1299 –C308 39. Cengic N, Baker CH, Schutz M, Goke B, Morris JC, Spitzweg C 2005 A novel therapeutic strategy for medullary thyroid cancer based on radioiodine therapy following tissue-specific sodium iodide symporter gene expression. J Clin Endocrinol Metab 90:4457– 4464 40. Huang M, Batra RK, Kogai T, Lin YQ, Hershman JM, Lichtenstein A, Sharma S, Zhu LX, Brent GA, Dubinett SM 2001 Ectopic expression of the thyroperoxidase gene augments radioiodide uptake and retention mediated by the sodium iodide symporter in non-small cell lung cancer. Cancer Gene Ther 8:612– 618 JCEM is published monthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving the endocrine community.