Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
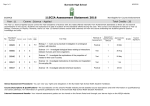
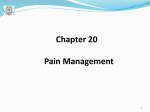
New Patient Health History Please print clearly and answer questions as completely as possible Patient Name: ____________________ Male Female Single Height: ______________ D.O.B:___/____/____ Age: _____ Date: ___/____/____ Married Other Weight: _________________ Occupation: ___________________ 1. What are your main areas of complaint? ____________________________________________ __________________________________________________________________________________ 2. How and when did your problem begin? __________________________________________________________________________________ __________________________________________________________________________________ 3. How often do you experience symptoms? Constantly (76-100% of the time) Occasionally (26-50% of the time) Frequently (51-75% of the time) Intermittently (0-25% of the time) 4. How are your symptoms changing with time? Getting Worse Staying the Same Getting Better 5. Using a pain scale from 0-10 (10 being the worst), how would you rate your problem? 0 1 2 3 4 5 6 7 8 9 10 (Please circle) 6. Has this codition interfered with your work, social activities or sleep?____________________ 7. Who else have you seen for this condition? _________________________________________ _________________________________________________________________________________ 8. What makes your symptoms better?_________________________________________________ 9. Does anything make your symptoms worse? ___________________________________________ 10. What type of exercise do you do? Strenuous Moderate Light None 11. List all medications and supplements you are currently taking or have taken for extended periods:___________________________________________________________________________ __________________________________________________________________________________ 12. List all surgical procedures, serious illnesses and hospitalizations you have had and approximate dates:_________________________________________________________________ __________________________________________________________________________________ __________________________________________________________________________________ 13. Have you had significant past injuries/accidents? Yes No If yes, please explain: _________________________________________________________________________________________ __________________________________________________________________________________ 14. Do you have any health problems? ________________________________________________ Evolve Wellness, LLC, Kelly Barrett, DC 3125 E. Burnside St. Portland, OR 97214 (503)758-9760 For each of the conditions listed below, place a check in the “PAST” column if you have had the condition in the past. If you presently have a condition listed below, place a check in the “PRESENT” column. Past Present Past Present Past Present Headaches Neck Pain Upper/Mid Back Pain Scoliosis Low Back Pain Shoulder Pain Elbow/Upper Arm Pain Wrist/Hand Pain Hip Pain Knee/Leg Pain Ankle/Foot Pain Jaw Pain Herniated Disc Concussion/Head Injury Arthritis Autoimmune Disease Slow Healing Liver/Gallbladder Disorder Nerve Damage High Blood Pressure Heart Disease High Cholesterol Stroke/Aneurysm Kidney Disorders Osteoporosis Bleeding Disorder Anticoagulant Therapy Corticosteroid Therapy Bladder Control Loss Prostate Problems Ulcer Infection/Fever Mental Health Issues Dizziness/Fainting Cancer/Tumor Blood Clot Numbness/Tingling/Weakness Pregnancy Diabetes Gastrointestinal/Bowel Issues Drug Abuse/Addiction Smoking/Tobacco Use Alcoholism Allergies Depression Fractures Chronic Cough Dermatitis/Rash/Eczema HIV/AIDS Anemia Thyroid Problems Asthma Anorexia Loss of Appetite Abnormal Weight Gain/Loss Metal/Surgical Implants Please Mark area(s) of injury or discomfort using (A) Letters to describe your pain (B) Numbers for the degree of pain using a scale from 1 (discomfort) to 10 (extreme pain) N = Numbing P = Pins and Needles B = Burning A = Aching S = Stabbing Is there anything else you feel is pertinent to today’s visit?__________________________________ ___________________________________________________________________________________ Patient Signature:_______________________________________________________________ Evolve Wellness, LLC, Kelly Barrett, DC 3125 E. Burnside St. Portland, OR 97214 (503)758-9760