Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
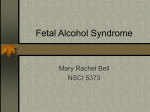
Vol. 5, 3529 –3533, November 1999 Clinical Cancer Research 3529 Circulating Soluble Fas Concentration in Breast Cancer Patients Takayuki Ueno, Masakazu Toi,1 and Takeshi Tominaga Department of Surgery, Tokyo Metropolitan Komagome Hospital, Tokyo 113-0021, Japan ABSTRACT Fas/Fas ligand (FasL) system, a major regulator of apoptosis, is involved in cancer cell death induced by the immune system and anticancer drugs. Fas is a cell-surface receptor that exists in two forms, transmembrane and soluble. The former induces apoptosis by ligation of FasL or agonistic anti-Fas antibody, whereas the latter inhibits Fasmediated apoptosis by neutralizing its ligand. In this study, we examined circulating soluble Fas (sFas) concentration in 118 healthy people, 162 primary and 71 recurrent breast cancer patients by ELISA. In the healthy group, men showed higher sFas concentrations than women (P < 0.001). In both sexes, sFas levels increased with age, and the agematched cutoff value was determined. The median sFas concentration in primary and recurrent cancer patients was 0.815 and 1.510 ng/ml, both of which were higher than in normal female controls (0.580 ng/ml; P 5 0.024 and P < 0.001, respectively). Among primary cancer patients, although no significant correlation was found between sFas concentration and clinical parameters other than menopausal status, high-sFas patients had a worse prognosis than low-sFas patients for both overall and disease-free survival (P 5 0.013 and P 5 0.032, respectively). The multivariate analysis confirmed that circulating sFas concentration was an independent prognostic indicator (P 5 0.020 for overall survival, P 5 0.025 for disease-free survival). We looked at the recurrent cancer patients, and sFas levels were higher in patients with liver metastasis compared with those with other recurrent sites (P 5 0.010), and high-sFas patients showed a worse prognosis than low-sFas patients (P 5 0.037). Our data demonstrate that, compared with healthy female controls, breast cancer patients, especially those with liver metastases, have higher circulating sFas levels. sFas may be useful once these results are confirmed by larger studies. Received 1/11/99; revised 8/5/99; accepted 8/9/99. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 To whom requests for reprints should be addressed, at Department of Surgery, Tokyo Metropolitan Komagome Hospital, 3-18-22 Honkomagome, Bunkyo-ku, Tokyo 113-0021, Japan. Phone: 81-3-3823-2101; Fax: 81-3-3824-1552. INTRODUCTION Fas (Apo-1, CD95) is a cell-surface receptor that is a member of the tumor necrosis factor/nerve growth factor receptor superfamily (1). By ligation of FasL2 (Ref. 2; CD95 ligand) or agonistic anti-Fas antibody, Fas induces apoptosis in various types of cells, including hepatocytes, T and B cells, and mammary epithelial cells (2). Fas-mediated apoptosis is deeply involved in cancer cell death brought about by the immune system or anticancer drugs. After activation through T-cell receptor, CTLs express FasL, which binds to Fas on the target cells, including cancer cells, to induce apoptosis (3). It has been reported that the loss of Fas function led to lymphoma in T cell-deficient mice and in Em L-myc transgenic mice (4, 5), suggesting that the Fas/FasL system plays an important role in the regulation of tumor development. In addition, several studies have suggested that the Fas/FasL system is involved in druginduced apoptosis in cancer cells (6, 7). Fas is found in two forms, transmembrane and soluble. The soluble form of Fas (sFas), which has five variants produced via alternative mRNA splicing, inhibits Fas-mediated apoptosis by neutralizing FasL or anti-Fas antibody (8 –10). Increased concentration of serum sFas has been reported in various diseases, including not only autoimmune diseases but also neoplastic diseases such as leukemia, lymphoma, and nonhematopoietic malignancy (8, 11–14). In bladder cancer patients, the association between increase in serum sFas and poor prognosis was indicated (15). These findings suggest that cancer cells upregulate or stimulate sFas production to protect themselves from Fas-mediated apoptosis (16, 17). In this study, to clarify the clinical significance of sFas, we examined serum sFas concentration in primary and recurrent breast cancer patients and revealed the relationship between sFas concentration and clinical features including prognosis. MATERIALS AND METHODS Patients. One hundred and eighteen healthy people, 59 men and 59 women, and 233 breast cancer patients, including 162 primary and 71 recurrent cancers, treated at Tokyo Metropolitan Komagome Hospital from 1990 to 1997 were enrolled in this study. All cancer patients were female. Primary cancer patients had no distant metastases. Patients with liver dysfunction (aspartate aminotransferase .35 IU/l or alanine aminotransferase .35 IU/l) were excluded from the study because it was reported that hepatitis patients had increased levels of sFas (18). The average age of the cancer patients was 55.1 years (range, 30 – 88). Informed consent was obtained from all. Clinical stages were determined according to the criteria of the Japanese Breast Cancer Society, which is based on the Union International Contre Cancer criteria. All primary patients had 2 The abbreviations used are: FasL, Fas ligand; sFas, soluble Fas; ER, estrogen receptor; PgR, progesterone receptor. Downloaded from clincancerres.aacrjournals.org on June 16, 2017. © 1999 American Association for Cancer Research. 3530 Soluble Fas in Breast Cancer Patients Table 1 Circulating sFas concentration in normal control Female Age group No. 30s 40s .50 Total 20 20 19 59 a Male sFas (ng/ml) No. sFasa (ng/ml) 0.200 (0.150–0.760) 0.695 (0.150–1.455) 1.240 (0.150–1.782) 0.580 (0.150–1.380)b 19 20 20 59 1.050 (0.233–2.042) 1.570 (0.150–2.415) 2.235 (1.160–2.725) 1.760 (0.705–2.440)b a Median (25th to 75th percentile). Male controls showed higher concentration of sFas than female controls (P , 0.001 by Mann-Whitney U test). b Fig. 1 Circulating sFas concentration. Circulating sFas levels in primary and recurrent breast cancer patients were significantly higher than in normal controls (P 5 0.024 and P , 0.001, respectively). The recurrent cancer patients with liver metastases showed higher sFas levels than those with the other sites of recurrence (P 5 0.010). The central box covers the middle 50% of the data values between the upper and lower quartiles. The central line is at the median. The bars below and above the box represent 10th and 90th percentile, respectively. Circles demonstrate the distribution of more extreme values. undergone either mastectomy or partial mastectomy with axillary lymph node dissection. Adjuvant treatments were applied according to the following criteria, which did not take into account circulating sFas concentration. Polychemotherapy, containing doxorubicin, 5-fluorouracil, and cyclophosphamide, was given for 6 months to patients ,55 years with metastasized lymph nodes, and hormonal therapy (tamoxifen) was given to ER-positive patients for .2 years. One hundred and thirty-one patients received adjuvant therapy, including 26 chemotherapy, 35 hormonal therapy, and 70 chemo-endocrine therapy. For all patients, including patients with no adjuvant treatments, postoperative physical examinations were performed at least every 3 months. The median follow-up period of surviving patients was 46 months (range, 23– 87). Liver, lung, brain, and distant lymph node metastases were diagnosed using computed tomographic scan, and bone metastasis was diagnosed using X-ray and bone scintigraphy. Among 71 recurrent cancer patients, 30 had single recurrent sites, and 41 had multiple recurrent sites. Major recurrent sites were liver (n 5 16), lung (n 5 22), brain (n 5 6), bone (n 5 39), and soft tissue (n 5 43). All recurrent patients were provided with treatments: 29 with systemic chemotherapy, 12 with hormonal therapy, 20 with chemo-endocrine therapy, 9 with surgical resection, and 1 with radiation therapy. Samples and Assay. Venous blood samples were drawn into sterile vacuum tubes at detection of primary breast cancer or recurrent cancer, prior to treatments being administered. They were centrifuged at 3000 rpm for 10 min and stored at 220°C until use. The level of sFas in the sera was determined by ELISA method using an sFas ELISA kit (Mitsubishi Bio-clinical Laboratories, Inc., Tokyo, Japan). This ELISA system adopted a specific sandwich method using peroxidase-labeled monoclonal antibody to the extracellular domain of Fas (amino acids 110 – 120) and polyclonal antibody to the intracellular domain (amino acids 305–319). This system detects the transmembrane-deficient type of sFas, which is the predominant form in humans. Five-fold diluted serum was used for determination, and the standard curve was drawn at concentrations from 0.015 to 2.0 ng/ml. Hormone Receptor Assay. ER and PgR were measured by the dextran-coated charcoal method using [3H]17b-estradiol or by the EIA method. The cutoff values were determined as 5 fmol/mg protein for both hormone receptors. Statistical Analysis. The distribution of sFas was drawn by box plots (Fig. 1). Unpaired groups were compared by the Mann-Whitney U tests or the Kruskal-Wallis rank tests. The x2 test was carried out for qualitative analysis. The survival curves were drawn by the Kaplan-Meier method, and the difference in prognosis between two groups was analyzed by the log-rank test. The multivariate analyses were performed using the Cox proportional hazards model. P , 0.05 was considered to indicate statistical significance. RESULTS In healthy controls, the median concentration of circulating sFas was 1.135 ng/ml (25th to 75th percentile, 0.150 to 2.000; mean 6 SD, 1.238 6 1.035). Men had significantly higher sFas levels than women (P , 0.001; Table 1). The sFas level showed a gradual increase with age in both sexes, and sFas was higher in men than in women in all age groups (Table 1). Among the 162 primary breast cancer patients, the median sFas level was 0.815 ng/ml (25th to 75th percentile, 0.590 to 1.200), which was significantly higher than in the normal female controls (median, 0.580 ng/ml; 25th to 75th percentile, 0.150 to 1.380; P 5 0.024; Fig. 1). Table 2 shows sFas concentrations by clinical stage, menopausal status, ER/PgR status, nodal involvement, and adjuvant therapy administered. sFas concentrations differed significantly by menopausal status (P , 0.001) but was not significantly associated with any of the other clinical parameters. The median sFas level in 71 recurrent breast cancer patients was 1.510 ng/ml (25th to 75th percentile, 1.140 to 2.263), which was significantly higher than in both normal female controls and primary cancer patients (P , 0.001, both; Fig. 1). Downloaded from clincancerres.aacrjournals.org on June 16, 2017. © 1999 American Association for Cancer Research. Clinical Cancer Research 3531 Table 2 sFas concentration according to clinical parameters in primary breast cancer patients Clinical parameters Clinical stage I II IIIa IIIb Menopausal status PrePost ER 2 1 Unknown PgR 2 1 Unknown Nodal metastasis (n) 2 1 Adjuvant therapies Chemotherapy Hormonal therapy Chemo-endocrine therapy None a Median sFas No. of level (ng/ml) patients (25th to 75th percentile) 35 103 13 11 0.730 (0.518 to 1.078) 0.810 (0.590 to 1.188) 0.880 (0.710 to 1.215) 1.030 (0.600 to 1.350) P NSa 0.643 85 77 0.680 (0.520 to 0.890) ,0.001 0.980 (0.730 to 1.350) 65 74 23 0.750 (0.545 to 1.177) 0.870 (0.650 to 1.280) 0.630 (0.282 to 1.077) NS 0.070 81 57 24 0.870 (0.640 to 1.210) 0.750 (0.545 to 1.263) 0.660 (0.355 to 1.135) NS 0.267 74 88 0.850 (0.595 to 1.270) 0.810 (0.610 to 1.190) NS 0.959 26 35 70 31 0.935 (0.690 to 1.270) 0.860 (0.540 to 1.268) 0.770 (0.590 to 1.060) 0.895 (0.630 to 1.700) NS 0.581 NS, not significant. In addition, the patients with liver metastasis (median, 2.710 ng/ml; 25th to 75th percentile, 1.340 to 3.440) showed significantly higher concentrations than those with other sites of recurrence (median, 1.430 ng/ml; 25th to 75th percentile, 1.140 to 2.040; P 5 0.010; Fig. 1). There was no significant difference in sFas concentration between patients with multiple sites of recurrence (median, 1.730 ng/ml; 25th to 75th percentile, 1.140 to 2.615) and those with single sites of recurrence (median, 1.435 ng/ml; 25th to 75th percentile, 1.130 to 2.060; P 5 0.409). We evaluated the prognostic value of sFas with cutoff values set at a median, a 75th percentile, and a 90th percentile of female controls by age decades, and the cutoff value at the 75th percentile provided the most significant difference in prognosis (log-rank test). Thus, we determined the agematched cutoff value as a 75th percentile of female controls in each age group (shown in Table 1). Between primary cancer patients with high sFas levels (above the cutoff value; n 5 18) and those with low levels (below the cutoff value; n 5 144), there was no significant difference in age, type of adjuvant treatment, or clinical parameters including tumor size, lymph node metastases, hormone receptor status, and clinical stage. All primary cancer patients had no metastases. Survival analysis demonstrated that patients with high sFas concentrations had a worse prognosis than those with low concentrations in both overall survival and disease-free survival (P 5 0.013 and P 5 0.032, respectively, log-rank test; Fig. 2, A and B). Furthermore, multivariable analysis confirmed that the circulating sFas concentration was an independent prognostic indicator in overall and disease-free survival (P 5 0.020 and P 5 0.025, Cox proportional hazards Fig. 2 A, overall survival curves in primary breast cancer patients. B, disease-free survival curves in primary breast cancer patients. C, overall survival curves in recurrent breast cancer patients. All survival curves were drawn by the Kaplan-Meier method. Bold lines, circulating sFas more than the age-matched cutoff value (n 5 18 in primary cancer patients and n 5 32 in recurrent cancer patients); thin lines, circulating sFas less than or equal to the cutoff value (n 5 144 in primary cancer patients and n 5 39 in recurrent cancer patients). In primary breast cancer, patients with high sFas concentrations had a worse prognosis than those with low sFas concentrations in overall survival (P 5 0.013, log-rank test; A) and in disease-free survival (P 5 0.032; B). The significant difference in overall survival was also seen in recurrent cancer patients (P 5 0.037; C). model; Table 3). For recurrent cancer patients, high-sFas patients (n 5 32) had a worse prognosis than low-sFas patients (n 5 39) in overall survival after detection of recurrence (P 5 0.037, log-rank test; Fig. 2C), but sFas concentration was not an independent prognostic indicator by multivariable analysis, which showed that liver metastasis was an independent predictor (data not shown). Downloaded from clincancerres.aacrjournals.org on June 16, 2017. © 1999 American Association for Cancer Research. 3532 Soluble Fas in Breast Cancer Patients Table 3 Multivariable analysis in primary breast cancer patients (Cox proportional hazards model) A. Overall survival Circulating sFas: high vs. lowb Lymph node metastasis: 1 vs. 2 ER: 2 vs. 1 Tumor size: .2.0 cm vs. ,2.0 cm Adjuvant therapies Chemotherapy Hormonal therapy Chemo-endocrine therapy B. Disease-free survival Circulating sFas: high vs. low Lymph node metastasis: 1 vs. 2 ER: 2 vs. 1 Tumor size: .2.0 cm vs. ,2.0 cm Adjuvant therapies Chemotherapy Hormonal therapy Chemo-endocrine therapy a b Hazard ratio 95% CIa P 4.178 7.475 1.564 1.358 1.250–13.961 1.361–41.065 0.563–4.340 0.136–13.537 0.020 0.021 0.391 0.794 3.164 0.644 2.958 0.254–39.394 0.371 0.037–11.085 0.762 0.380–23.057 0.301 4.022 7.610 1.029 0.371 1.190–13.596 1.950–29.705 0.407–2.603 0.112–1.230 2.239 0.710 2.086 0.335–14.976 0.406 0.099–5.113 0.734 0.423–10.282 0.366 0.025 0.004 0.951 0.105 CI, confidence interval. High, above the cut-off value; low, below the cut-off value. DISCUSSION In this study, we demonstrated that circulating sFas concentration was increased in breast cancer patients, particularly recurrent cancer patients, and that sFas concentration was an independent prognostic indicator for both overall and diseasefree survival. The sFas function has not yet been fully elucidated, but there are several investigations suggesting the role of sFas in cancer progression. sFas has been reported to play an important role in the regulation of apoptosis as an inhibitor of Fas-mediated apoptosis (8 –10). Recent studies have revealed that the Fas/FasL system is an important mechanism for tumor escape from the immune system: expression of FasL on tumor cell surfaces and emission of soluble form of FasL (19 –24). sFas is thought to be another mechanism for tumor immune evasion (16, 17), and it was documented that there was an inverse correlation between serum sFas levels and anti-autologous tumor cytotoxicity in bladder cancer patients, suggesting that sFas is related with tumor immune evasion in cancer patients (15). In addition, because the Fas-mediated apoptosis has been demonstrated to be involved in anticancer drug-induced apoptosis (6, 7), it is conceivable that sFas causes resistance to treatments by inhibiting Fas-mediated apoptosis in cancer cells. Although the precise functions of sFas remain to be clarified, these functions related to the immune evasion or drug resistance may contribute to the poor prognosis for both overall and disease-free survival in high-sFas patients. Because the number of patients with high sFas concentration was small in this study, further clinical studies will be needed to confirm our results. We determined the age-matched cutoff value in this study. Seishima et al. (25) first reported that sFas concentration in healthy people increased with age and differed in sex. Therefore, it is important to take account of age and sex in evaluation of serum sFas concentration, and we showed the prognostic value of sFas using the age-matched cutoff value of women. This age-matched cutoff value will be useful to further assess the circulating sFas concentration in various diseases. The sFas values in healthy controls were different among studies (12–15, 18, 25). Although the exact reason for the difference is unclear, several factors seem to be involved, including differences in control groups, in sensitivity of the antibodies, and in characters of the standards. Recurrent cancer patients with liver metastasis showed a remarkable increase in sFas level in this study. As is well known, the appearance of liver metastasis is a predictor of poor prognosis for a variety of solid tumors, including breast cancer. However, little is known about the reason. It may be possible that this notable elevation in sFas contributes to rapid progression of metastatic liver tumors. In colon cancer, no difference in sFas levels was reported between primary patients and patients with liver metastasis (12). Thus, the mechanism of sFas induction might differ depending on tumor type. The expression mechanism and cellular origins of sFas are still unclear. In gastric cancer, sFas-mRNA expression was demonstrated in cancer cells and lymphocytes of metastasized lymph nodes by in situ reverse transcription-PCR (26). It was further reported that all of the following express sFas mRNA: activated peripheral blood mononuclear cells of healthy donors, hepatocytes, and several tumor cell lines, including leukemia, osteosarcoma, and glioma (9, 10, 16, 27, 28). Interestingly, it was reported that an Adriamycin-resistant breast cancer cell line (MCF7Adr) produced sFas, although the wild-type (MCF7) did not (29), indicating that cancer cells may change the expression level of sFas, depending on their phenotypes. These findings suggest that circulating sFas derives from various origins, including cancer cells, stromal cells, and other visceral cells. In conclusion, this study demonstrates that circulating sFas concentration is increased in breast cancer patients, especially those with liver metastases. The patient number is small in this study. Larger clinical studies are important to establish the clinical significance of sFas. The determination of sFas may be useful once additional studies confirm the results of the present study. ACKNOWLEDGMENTS We thank Mariko Muta, Eiko Isobe, and Masahiro Fuwa for technical and statistical assistance. REFERENCES 1. Itoh, N., Yonehara, S., Ishii, A., Yonehara, M., Mizushima, S., Sameshima, M., Hase, A., Seto, Y., and Nagata, S. The polypeptide encoded by the cDNA for human cell surface antigen Fas can mediate apoptosis. Cell, 66: 233–243, 1991. 2. Leithauser, F., Dhein, J., Mechtersheimer, G., Koretz, K., Bruderlein, S., Henne, C., Schmidt, A., Debatin, K. M., Krammer, P. H., and Moller, P. Constitutive and induced expression of apo-1, a new member of the nerve growth factor/tumor necrosis factor receptor superfamily, in normal and malignant cells. Lab. Investig., 69: 415– 429, 1993. 3. Nagata, S., and Golstein, P. The Fas death factor. Science (Washington DC), 267: 1449 –1456, 1995. 4. Peng, S. L., Robert, M. E., Hayday, A. C., and Craft, J. A tumorsuppressor function for Fas (CD95) revealed in T cell-deficient mice. J. Exp. Med., 184: 1149 –1154, 1996. 5. Zörnig, M., Grzeschiczek, A., Kowalski, M-B., Hartmann, K-U., and Möröy, T. Loss of Fas/Apo-1 receptor accelerates lymphomagenesis in Em L-MYC transgenic mice but not in animals infected with MoMuLV. Oncogene, 10: 2397–2401, 1995. Downloaded from clincancerres.aacrjournals.org on June 16, 2017. © 1999 American Association for Cancer Research. Clinical Cancer Research 3533 6. Friesen, C., Herr, I., Krammer, P. H., and Debatin, K-M. Involvement of CD95 (APO-1/Fas) receptor/ligand system in drug-induced apoptosis in leukemia cells. Nat. Med., 2: 574 –577, 1996. 7. Micheau, O., Solary, E., Hammann, A., Martin, F., and DimancheBoitrel, M-T. Sensitization of cancer cells treated with cytotoxic drugs to Fas-mediated cytotoxicity. J. Natl. Cancer Inst., 89: 783–789, 1997. 8. Cheng, J., Zhou, T., Liu, C., Shapiro, J. P., Brauer, M. J., Kiefer, M. C., Barr, P. J., and Mountz, J. D. Protection from Fas-mediated apoptosis by a soluble form of the Fas molecule. Science (Washington DC), 263: 1759 –1762, 1994. 9. Cascino, I., Fiucci, G., Papoff, G., and Ruberti, G. Three functional soluble forms of the human apoptosis-inducing Fas molecule are produced by alternative splicing. J. Immunol., 154: 2706 –2713, 1995. 10. Papoff, G., Cascino, I., Eramo, A., Starace, G., Lynch, D. H., and Ruberti, G. An N-terminal domain shared by Fas/Apo-1 (CD95) soluble variants prevents cell death in vitro. J. Immunol., 156: 4622– 4630, 1996. 11. Knipping, E., Debatin, K-M., Stricker, K., Heilig, B., Eder, A., and Krammer, P. H. Identification of soluble APO-1 in supernatants of human B- and T-cell lines and increased serum levels in B- and T-cell leukemias. Blood, 85: 1562–1569, 1995. 12. Midis, G. P., Shen, Y., and Owen-Schaub, L. B. Elevated soluble Fas (sFas) levels in nonhematopoietic human malignancy. Cancer Res., 56: 3870 –3874, 1996. 13. Yufu, Y., Choi, I., Hirase, N., Tokoro, A., Noguchi, Y., Goto, T., Uike, N., and Kozuru, M. Soluble Fas in the serum of patients with non-Hodgkin’s lymphoma: higher concentration in angioimmunoblastic T-cell lymphoma. Am. J. Hematol., 58: 334 –336, 1998. 14. Jodo, S., Kobayashi, S., Nakajima, Y., Matsunaga, T., Nakayama, N., Ogura, N., Kayagaki, N., Okumura, K., and Koike, T. Elevated serum levels of soluble Fas/APO-1 (CD95) in patients with hepatocellular carcinoma. Clin. Exp. Immunol., 112: 166 –171, 1998. 15. Mizutani, Y., Yoshida, O., and Bonavida, B. Prognostic significance of soluble Fas in the serum of patients with bladder cancer. J. Urol., 160: 571–576, 1998. 16. Owen-Schaub, L. B., Angelo, L. S., Radinsky, R., Ware, C. F., Gesner, T. G., and Bartos, D. P. Soluble Fas/APO-1 in tumor cells: a potential regulator of apoptosis? Cancer Lett., 94: 1– 8, 1995. 17. Natoli, G., Ianni, A., Costanzo, A., Petrillo, G. D., Ilari, I., Chirillo, P., Balsano, C., and Levrero, M. Resistance to Fas-mediated apoptosis in human hepatoma cells. Oncogene, 11: 1157–1164, 1995. 18. Iio, S., Hayashi, N., Mita, E., Ueda, K., Mochizuki, K., Hiramatsu, N., Kanto, T., Sasaki, Y., Kasahara, A., and Hori, M. Serum levels of soluble Fas antigen in chronic hepatitis C patients. J. Hepatol., 29: 517–523, 1998. 19. Walker, P. R., Saas, P., and Dietrich, P-Y. Role of Fas ligand (CD95L) in immune escape. The tumor cell strikes back. J. Immunol., 158: 4521– 4524, 1997. 20. Nagata, S. Apoptosis by death factor. Cell, 88: 355–365, 1997. 21. Hahne, M., Rimoldi, D., Schroter, M., Romero, P., Schreier, M., French, L. E., Schneider, P., Bornand, T., Fontana, A., Lienard, D., Cerottini, J-C., and Tschopp, J. Melanoma cell expression of Fas (Apo1/CD95) ligand: implications for tumor immune escape. Science (Washington DC), 274: 1363–1366, 1996. 22. Strand, S., Hofmann, W. J., Hug, H., Muller, M., Otto, G., Strand, D., Mariani, S. M., Stremmel, W., Krammer, P. H., and Galle, P. R. Lymphocyte apoptosis induced by CD95 (APO-1/Fas) ligand expressing tumor cells: a mechanism of immune evasion. Nat. Med., 2: 1361–1366, 1996. 23. O’Connell, J., O’Sullivan, G. C., Collins, J. K., and Shanahan, F. The Fas counterattack: Fas-mediated T cell killing by colon cancer cells expressing Fas ligand. J. Exp. Med., 184: 1075–1082, 1996. 24. Tanaka, M., Suda, T., Haze, K., Nakamura, N., Sato, K., Kimura, F., Motoyoshi, K., Mizuki, M., Tagawa, S., Ohga, S., Hatake, K., Drummond, A. H., and Nagata, S. Fas ligand in human serum. Nat. Med., 2: 317–322, 1996. 25. Seishima, M., Takemura, M., Saito, K., Sano, H., Minatoguchi, S., Fujiwara, H., Hachiya, T., and Noma, A. Highly sensitive ELISA for soluble Fas in serum: increased soluble Fas in the elderly. Clin. Chem., 42: 1911–1914, 1996. 26. Lee, S. H, Kim, S. Y., Lee, J. Y., Shin, M. S., Dong, S. M., Na, E. Y., Park, W. S., Kim, K. M., Kim, C. S., Kim, S. H., and Yoo, N. J. Detection of soluble Fas mRNA using in situ reverse transcriptionpolymerase chain reaction. Lab. Investig., 78: 453– 459, 1998. 27. Krams, S. M., Fox, C. K., Beatty, P. R., Cao, S., Villanueva, J. C., Esquivel, C. O., and Martinez, O. M. Human hepatocytes produce an isoform of Fas that inhibits apoptosis. Transplantation, 65: 713–721, 1998. 28. Weller, M., Malipielo, U., Rensing-Ehl, A., Barr, P. J., and Fontana, A. Fas/APO-1 gene transfer for human malignant glioma. Cancer Res., 55: 2936 –2944, 1995. 29. Cai, Z., Stancou, R., Körner, M., and Chouaib, S. Impairment of Fas-antigen expression in Adriamycin-resistant but not TNF-resistant MCF7 tumor cells. Int. J. Cancer, 68: 535–546, 1996. Downloaded from clincancerres.aacrjournals.org on June 16, 2017. © 1999 American Association for Cancer Research. Circulating Soluble Fas Concentration in Breast Cancer Patients Takayuki Ueno, Masakazu Toi and Takeshi Tominaga Clin Cancer Res 1999;5:3529-3533. Updated version Cited articles Citing articles E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://clincancerres.aacrjournals.org/content/5/11/3529 This article cites 29 articles, 13 of which you can access for free at: http://clincancerres.aacrjournals.org/content/5/11/3529.full.html#ref-list-1 This article has been cited by 7 HighWire-hosted articles. Access the articles at: /content/5/11/3529.full.html#related-urls Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from clincancerres.aacrjournals.org on June 16, 2017. © 1999 American Association for Cancer Research.