Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Coronary artery disease wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
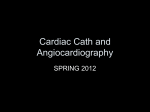
European Heart Journal (1997) 18, 1110-1114 PTCA registry of German community hospitals A. Vogt, T. Bonzel, D. Harmjanz, E.-R. v. Leitner, C. Pfafferott, H.-J. Engel, W. Niederer, P.-R. Schuster, H. G. Glunz and K.- L. Neuhaus for the Arbeitsgemeinschaft Leitender Kardiologischer Krankenhausarzte (ALKK) study group Medizinische Klinik II, Stadtische Kliniken Kassel gGmbH, Kassel, Germany Background Percutaneous transluminal coronary angioplasty (PTCA) is widely used, but no quality control has been systematically performed as yet. Methods A registry of all PTCA procedures has been established since October 1992 for the majority of the German community hospitals performing PTCA, representing about one third of all PTCA activity in Germany. Baseline demographic data, indication for PTCA, primary success and in-hospital clinical events were recorded. Each centre was visited at regular intervals to assure completeness and reliability of the data. Results Of 52 453 procedures performed from October 1992 to December 1994 the catheter laboratory and discharge forms were 997% and 98-1% complete, respectively. In 85-9% a single lesion was dilated per procedure, but 48-7% of the patients had multivessel disease. The success rate was 66-5% in complete occlusions (residual stenosis <70%) and 91-2% in non-occluded vessels (residual stenosis <50%). Abrupt vessel closure occurred in 3-4%, of which 77-5% could be recanalized by repeat intervention. In procedures not done for acute myocardial infarction, the in-hospital mortality was 0-52%, the procedure-related mortality 037%. In 302% of all patients a severe complication occurred (procedure-related death, myocardial infarction or emergency bypass surgery). Conclusion Complete recording of all PTCA procedures is feasible even on a nationwide basis. This is a pre-requisite for continuous quality control. The reporting of the procedures by itself very probably, has an impact on the quality which is, however, not measurable quantitatively. (Eur Heart J 1997; 18: 1110-1114) Key Words: Percutaneous transluminal coronary angioplasty, quality control, success, complications. Introduction and seven centres are based in community hospitals (non-university hospitals involved in the general medical To gain knowledge about the present status of percu- care of the population), of which 62 have formed a taneous transluminal coronary angioplasty (PTCA), and working group called 'Arbeitsgemeinschaft leitender to control the quality of its routine application, a kardiologischer Krankenhausarzte (ALKK)'. All but registry of all PTCA procedures from 43 centres in two of these centres participated in the registry, which Germany was started in 1992. It now includes 68 centres, thus represents approximately 35% of all PTCA proceand the data gathered from October 1992 to December dures carried out in Germany. The number of participating centres was 43 in 1992, 59 in 1993, and 65 in 1994. 1994 are reported here. Sixteen of the participating centres had an on-site cardiac surgery department. The caseload was <300 procedures/year in 27, 300-600 procedures/year in 27 and >600 procedures/year in 11 centres (median value Organization of the registry overall 352). The average number of operators per In 1994, more than 88 000 PTCA procedures were centre was 2-5. Each PTCA procedure was included on performed in 190 centres in Germany1'1. One hundred an intention-to-treat basis. A single-page form, which listed baseline demographic and angiographic data, indication for PTCA, angiographic success, and complicaRevision submitted 20 September 1996, and accepted 25 September tions in the catheterization laboratory was transmitted 1996. immediately after the procedure to the data centre in Correspondence: Prof. Dr med. Albrecht Vogt, Medizinische Klinik Kassel. A second single-page form, reporting possible II, Stadtische Kliniken Kassel gGmbH, MonchebergstraBe 41-43, complications after the patient left the catheterization D-34125 Kassel, Germany. 0195-668X/97/071110 + 05 S18.00/0 ^, 1997 The European Society of Cardiology PTCA registry of German community hospitals Months since start of registry Figure 1 Procedures in the registry since its initiation in October 1992. laboratory, was completed and transmitted immediately after hospital discharge. Each centre was visited twice per year and the local records were compared with the procedures entered into the registry to ensure completeness. This audit revealed that 11% of PTCA procedures performed were not reported to the data centre. Incomplete data forms were immediately completed by telephone query from the data centre if possible, or otherwise returned for completion to the participating centres. Complications were classified centrally, with respect to their relation to the procedure, by looking up the individual case reports. Myocardial infarction after the procedure was diagnosed when typical clinical symptoms were accompanied by creatine kinase levels more than twice the upper limit of normal and/or ECG changes diagnostic of myocardial infarction. The database was installed on a personal computer using dBase IV software (Ashton-Tate). Statistical calculations were performed with the Statsoft CSS software package. Completeness of the data From 1 October 1992 to 31 December 1994, 53 834 PTCA procedures were entered into the registry (Fig. 1). Of these, 1381 were not performed for various reasons (withdrawal of consent, intermittent other disease, change in therapeutic strategy), leaving 52 453 procedures actually performed. The procedure-reporting forms of the latter are 99-7% complete, and the discharge forms are 981% complete at the time of writing. In 72-8%, details of the procedures were given to the data centre in advance by fax or telephone. In this report the procedures incompletely reported are excluded. LAD RCA 1111 Cx Figure 2 Anatomical location of lesions dilated. LAD = left anterior descending coronary artery, RCA=right coronary artery, Cx=circumflex coronary artery. • = lesions in the proximal part; 0=distally located lesions of the respective coronary artery except for bypass grafts, where no such differentiation was made. 4 7 10 13 16 19 22 Months of registry (1 = Oct. 1992) Figure 3 Proportion of immediate interventions during the primary diagnostic procedure. There is a significant increase in the proportion of immediate PTCA from October 1992 to December 1994. dilated lesions. One-, two- and three-vessel coronary disease was present in 51-3, 33-4, and 15-3% of the procedures, respectively. Left-ventricular function was visually classified by the operator as normal in 600%, depressed in 35-7%, and severely depressed in 4-4% of those who underwent ventriculography. PTCA was performed without a left ventricular angiogram in 12-7% (6665 procedures); in 6-6% after prior coronary bypass surgery; in 20-2% after one or more prior PTCA procedures; in 16-6% one or more recurrent stenoses were dilated; in 299%, the procedure was performed immediately after diagnostic catheterization in the same session (Fig. 3); in 14-1% >2 lesions were dilated in a single session; in only 114 procedures were >3 lesions treated. The lesion characteristics and immediate angiographic results are specified in Table 1. Baseline data PTCA was performed in 43 947 patients; the mean age was 60-7 ± 9-7 years, and 22-3% were women. Figure 2 shows the distribution of the anatomical locations of the Indications for PTCA The majority of the procedures was performed in symptomatic patients with stable (59-9%) or unstable angina Eur Heart J, Vol. 18, July 1997 1112 A. Vogt et al. Table 1 Lesion characteristics and angiographic success n Type of lesion (%) A Bl B2 Cl C2 Balloon size (mm) Complete occlusion (%) Successful recanalization (%) Non-occluded vessels % stenosis before PTCA % stenosis after PTCA % angiographic success Table 2 Lesion 1 Lesion 2 Lesion 3 52 273 7379 935 15-8 32-6 35-9 9-6 61 2-90 ± 0-44 16-9 67-3 20-4 37-2 29-9 7-8 4-8 2-71 ±0-43 6-7 54-2 21-7 37-3 30-2 6-4 4-4 2-62 ± 0 43 5-3 500 88-2 ±8-7 27-1 ±17-8 91 -5 83-3 ± 10 7 28-3 ±18-4 89-4 82-7 ± 10-9 28-5 ± 19-4 89-2 Complications by indication for PTCA Stable AP n Abrupt closure (%) PTCA-related MI (%) Emergency CABG (%) PTCA-related death (%) In-hospital mortality (%) PTCA-related death, MI or emergency CABG (%) 31 300 830 (2-65) 587 (1-88) 192 (0-61) 78 (0-25) 86 (0-27) 111 (2-48) Unstable AP 13 362 643 (4-81) 420 (3-14) 171 (1-28) 95 (0-71) 155 (1-16) 606 (4-54) AMI Prognostic 2879 169 (5-87) 0 4737 120 (2-53) 71 (1-50) 20 (0-42) 12 (0-5) 15 (0-32) 99 (209) 44 (1 52) 25 (0-87) 267 (9-27) 112 (3-89) AMI = acute myocardial infarction; CABG = coronary artery bypass grafting. pectoris (21-8%). In 5-5%, PTCA was performed in acute myocardial infarction, and in 3-8% in severe acute myocardial ischaemia with ECG-changes not diagnostic for acute infarction. In 495/2879 procedures the acute myocardial infarction and in 442/1965 the acute ischaemia leading to PTCA resulted from abrupt vessel closure after a preceding intervention. The same is true for 1905/11 397 procedures performed for unstable angina pectoris. In 9 1 % , PTCA was performed for prognostic reasons in asymptomatic patients with or without positive exercise tests. Procedural success In all the lesions in which an attempt to dilate was made, 15-5% were complete occlusions. Of those, 66-5% were successfully recanalized, with a residual stenosis <70%. If acute occlusions in the setting of myocardial infarction are excluded, the primary success rate of recanalizations was 61-8%. In non-occluded vessels, the overall success rate was 91-2%, with a residual stenosis <50%. Coronary stents were implanted in 2-8%. The success Eur Heart J. Vol. 18. July 1997 rate was clearly dependent on stenosis morphology. In type A or Bl stenosis was classified according to the AHA/ACC criteria121, the per lesion success was 92-4% (residual stenosis <50%), whereas in type B2 or C stenosis it was only 810% (/><00001). In elective interventions for stable angina or in asymptomatic patients the success rate was 86-6% per lesion, in unstable angina 88-1% and in acute myocardial infarction 78-4% (/><00001). Gender had no influence on the success rates, but in patients <65 years the success rates were significantly higher (68-2% in occluded, 92-3% in non- occluded vessels) than in patients >65 years (65-2% and 90-1% in occluded and nonoccluded vessels, / > <0001). Complications Overall, 1578 procedures (302%) caused severe complications leading to myocardial infarction, emergency bypass surgery, or death. Of the patients with emergency bypass surgery 8-4% eventually died. A complete listing of complications broken down by indication for PTCA PTCA registry of German community hospitals 1/93 111/93 1/94 Quarters of registry 111/94 Figure 4 Techniques applied in repeat interventions for abrupt vessel closure. From October 1992 to December 1994 the proportion of standard balloon PTCA procedures ( • ) remained essentially unchanged. The use of perfusion balloons ( • ) decreased slightly in favour of the implantation of coronary stents (D). is given in Table 2. The majority of PTCA-related clinical events was associated with abrupt vessel closure documented after a total of 1762 procedures (3-4%). Abrupt vessel closure was treated with repeat PTCA with standard balloons in 782, with perfusion balloons in 217, and with coronary stents in 291 cases (Fig. 4). In 87 cases other interventions (e.g. atherectomy, laser, intracoronary thrombolysis) were performed, and in 222 cases no repeat intervention was undertaken. Of the repeat interventions 77-5% were successful angiographically with a residual stenosis <70%. Despite this, 407 patients were referred to emergency coronary bypass and a further 17 patients to elective coronary surgery. Of the patients with abrupt vessel closure, 569 had a procedure-related myocardial infarction (maximum serum creatine kinase 603 ± 542 U/l), and 112 patients eventually died. Procedure-related death, myocardial infarction or emergency bypass surgery occurred in 756/1762 cases after abrupt vessel closure, i.e. 42-9%. If the procedures done for acute myocardial infarction are excluded, the total in-hospital mortality is 0-52% (256 patients), and the procedure-related mortality 037% (185 patients). Overall, 1482 patients (30%) of those with elective PTCA had at least one severe complication (procedure-related death, emergency bypass surgery, or procedure-related myocardial infarction). Discussion The PTCA registry of the German community hospitals was established to monitor quality control of this widely used intervention. It was possible to record >98% complete and reliable data on all procedures in the participating centres with respect to the immediate results in 1113 the catheterization laboratory and clinical events until discharge. The regular on-site monitoring revealed that less than 1% procedures had not been reported to the data centre. Despite complete data on the whole spectrum of PTCA procedures, the rating of appropriateness of indication, performance and results is an unresolved issue. In our project, an expert rating of a random subset of 2% (stratified by centres, at least five cases per centre) was performed. These results will be reported elsewhere. As in the RAND study'31, roughly 5% of the procedures were deemed inappropriate. The rate of major PTCA complications has decreased as compared to earlier reports'451, even though elective as well as emergency procedures are included. The case volume of the centres had no significant impact on the complication rate or on the immediate angiographic success rate; no significant differences were seen when centres with <300, 300-600 and >600 procedures per year were compared. This is in contrast to reports from the United States, where the complication rate increased in centres with lower case loads, especially in those with less than 200 cases per year'6"81. One reason for this may be that in Germany the work load per operator is usually higher than in the U.S.; in the smaller centres usually only one to three operators perform PTCA. While the rate of myocardial infarction after PTCA has remained relatively constant, the rate of emergency bypass surgery decreased from around 6%'5' to one tenth of that in this registry. This is mainly due to improved techniques and operator experience allowing for successful repeat intervention in the majority of cases even after abrupt vessel closure, whereas the incidence of abrupt closure itself did not decrease significantly. As in the United States'71, the majority of interventions are still single-lesion PTCA despite the many optimistic reports on the high success rates at acceptably low risk of multivessel interventions'9""1. Since nearly one half of the patients in this registry had multivessel disease it becomes clear that in a significant proportion only partial revascularization was achieved. The rate of immediate PTCA during a primarily diagnostic procedure increased during the time reported here from 23 to 40%. This is not due to an increase in emergency interventions; the proportion of PTCA in acute myocardial infarction remained relatively constant at around 5% during the time reported here. There are, however, extreme differences between centres, with proportions of immediate PTCA varying between 3 to 74%. This demonstrates that the decision for immediate intervention in elective cases is driven by logistic rather than medical reasons. We conclude that complete recording of all PTCA procedures is feasible, even on a nationwide basis. The model project reported here covers about one third of all procedures performed in Germany. The data demonstrate that the risk from PTCA in the 1990s has decreased, as compared to earlier registries, which in turn may lead to a widening of the indications. The Eur Heart J, Vol. 18, July 1997 1114 A. Vogt et al. rating of appropriateness remains a largely unresolved issue, despite complete and reliable data, since no generally accepted standards exist. Very probably the reporting of the procedures by itself has some impact on the quality which is, however, not measurable quantitatively. References [1] Gleichmann U, Mannebach H, Lichtlen P. 11. Bericht iiber Struktur and Leistungszahlen der Herzkatheterlabors in der Bundesrepublik Deutschland. Z Kardiol 1995; 84: 953-62 [2] Myler RK, Shaw RE, Stertzer SH et al. Lesion morphology and coronary angioplasty: Current experience and analysis. J Am Coll Cardiol 1992; 7: 1641-52. [3] Hilborne LH, Leape LL, Bernstein SJ et al. The appropriateness of use of percutaneous transluminal coronary angioplasty in New York State. JAMA 1993; 6: 761-5. [4] Dorros G, Cowley MJ, Janke L, Kelsey SF, Mullin SM, van Raden M. In-hospital mortality rate in the national heart, lung, and blood institute percutaneous transluminal coronary angioplasty registry. Am J Cardiol 1984; 53: 17C-21C. [5] Holmes DR, Holubkov R, Vlietstra RE et al. Comparison of complications during percutaneous transluminal coronary Eur Heart J, Vol. 18, July 1997 angioplasty from 1977 to 1981 and from 1985 to 1986: The National Heart, Lung, and Blood Institute percutaneous transluminal coronary angioplasty registry. J Am Coll Cardiol 1988; 5: 1149-55. [6] Jollis JG, Peterson ED, DeLong ER et al. The relation between the volume of coronary angioplasty procedures at hospitals treating medicare beneficiaries and short-term mortality. N Engl J Med 1994; 331: 1625-9. [7] Ritchie JL, Phillips KA, Luft HS. Coronary angioplasty. Statewide experience in California. Circulation 1993; 88: 2735-43. [8] Kimmel SE, Berlin JA, Laskey WK. The relationship between coronary angioplasty procedure volume and major complications. JAMA 1995; 274: 1137-42. [9] Hollman J, Simpfendorfer C, Franco I, Whitlow P, Goormastic M. Multivessel and single-vessel coronary angioplasty: A comparative study. Am Heart J 1992; 124: 9-12. [10] Bredlau CE, Roubin GS, Leimgruber PP, Douglas JS, King SB III, Gruentzig A. In-hospital morbidity and mortality in patients undergoing elective coronary angioplasty. Circulation 1985; 5: 1044-52. [11] Sim I, Gupta M, McDonald K, Bourassa MG, Hlatky MA. A meta-analysis of randomized trials comparing coronary artery bypass grafting with percutaneous transluminal coronary angioplasty in multivessel coronary artery disease. Am J Cardiol 1995; 76: 1025-9.