Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
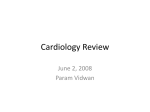
Journal of Cardiovascular Diseases & Diagnosis Barman et al., J Cardiovasc Dis Diagn 2014, 2:3 http://dx.doi.org/10.4172/2329-9517.1000152 Research Case Report Article Open OpenAccess Access Acute Aortic Dissection in a Young Healthy Athlete with Androgenic Anabolic Steroid Use: A Case Report from Qatar Manish Barman*, Bendaas Djamel and Joji Mathews Department of Cardiology, Al Ahli Hospital, Doha, Qatar Abstract Acute aortic dissection can occur at the time of intense physical exertion in strength-trained athletes like weightlifters, bodybuilders, throwers, and wrestlers. Rapid rise in blood pressure and history of hypertension are the most common causes of aortic dissection in athletes. It is a very tragic event because of its high mortality rate of about 32% in young patients. We report a case of aortic dissection in a young weightlifter with history of anabolic steroid usage with an extensive intimal tear of the aorta at Sino tubular junction and arch. Keywords: Acute aortic dissection; Anabolic steroids Family history Introduction No family history of sudden cardiac death, premature ischemic heart disease or structural heart disease. Acute aortic dissection results from a tear in the intima and media of the aortic wall, with the subsequent creation of a false lumen in the outer half of the media and elongation of this channel by pulsatile blood flow. Dissection of the aorta is associated with a high degree of morbidity and mortality despite continuing improvements in diagnostic and surgical techniques and hypertension is present as the most common cause in 70-90% of patients with aortic dissection [1,2]. A number of normal daily and athletic activities require isometric or static exercise. Sports such as weightlifting and other high-resistance activities are used by power athletes to gain strength and skeletal muscle bulk. These exercises significantly increase blood pressure, heart rate, myocardial contractility, and cardiac output. Hypertension has long been recognized as an important risk factor for the development of aortic aneurysms and dissections [1,3]. Also, it has been speculated that the very high blood pressure generated during the lifting of weights, particularly with staining accompanied by a Valsalva maneuver, may be the cause of an aortic intimal tear [3]. Pre-participation cardiovascular evaluation of young competitive athletes is warranted on the basis of the available evidence [4]. Patients with pre-disposing conditions to aortic dissection, including hypertension, should be sturdily encouraged to refrain from weightlifting. We present a case of aortic dissection in a young athlete with no history of hypertension. Risk profile No hypertension, diabetes, dyslipidemia or cardiovascular disease. Anabolic steroids for body building. Non-smoker and no alcohol consumption. Physical examination BP: 120/65 mmHg [R], 114/65 mmHg [L], PR: 95/min regular, Peripheral pulses palpable normal bilaterally symmetrical. No radiofemoral delay. No edema. CVS- mid-late relatively loud diastolic murmur. Chest- bilateral scattered R>L coarse crepitation with wheeze and tubular breath sounds at Right infra scapular region. Investigations ECG: NSR 95/minute. No acute ST-T changes (Figure 1). Labs: Complete blood count WBC13.63 X 10^3 /ul, Neutrophils 10.72 [78.6%] Lymphocytes 11%, Monocytes 8.5% Case Presentation Hb 15.7 gm/dl A 34 Year old male athlete, an active runner and weightlifter was seen by cardiologist on referral request from Internal Medicine for evaluation of cardiac murmur in emergency. D-dimer 1.76 mg/l [n<0.5], Relevant history BNP 7853 The patient visited ER with complaints of cough with expectoration [blood tinged], low grade fever with gradual onset shortness of breath and orthopnea since 2 days. Generalized fatigue and body aches. Right upper abdominal pain, No chest pain. No syncope/No palpitations. He gave history of daily exercises in Gym, body building, takes protein supplements and anabolic steroids (winstrol 25 mg/day since more than a year). Past history None significant except recently seen two days ago In ER with pain abdomen which wasdiagnosed as renal colic. J Cardiovasc Dis Diagn ISSN: 2329-9517 JCDD, an open access journal CRP 85 *Corresponding author: Manish Barman, Department of Cardiology, Al Ahli Hospital, PO Box 6401, Doha, Qatar, Tel: 974-66936385; E-mail: [email protected] Received February 26, 2014; Accepted April 07, 2014; Published April 14, 2014 Citation: Barman M, Djamel B, Mathews J (2014) Acute Aortic Dissection in a Young Healthy Athlete with Androgenic Anabolic Steroid Use: A Case Report from Qatar. J Cardiovasc Dis Diagn 2: 152. doi:10.4172/2329-9517.1000152 Copyright: © 2014 Barman M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Volume 2 • Issue 3 • 1000152 Citation: Barman M, Djamel B, Mathews J (2014) Acute Aortic Dissection in a Young Healthy Athlete with Androgenic Anabolic Steroid Use: A Case Report from Qatar. J Cardiovasc Dis Diagn 2: 152. doi:10.4172/2329-9517.1000152 Page 2 of 4 • High blood pressure • Fluid retention • Liver disorders • Risk of contracting blood borne diseases like HIV from sharing infected needles • Sexual and reproductive disorders Figure 1: ECG. Renal Function Tests deranged, BUN 60, Creatinine 2.2 Liver function tests- Normal CX-ray: R>L lower lobe consolidation. Heart, Mediastinum normal, No pneumothorax or pleural effusion. No hilar or Mediastinal lymphadenopathy. CT ratio<0.5 ECHO: Normal LV dimensions and systolic function. Dilated Aortic root with visible intimal flap in Aorta. Mod-severe aortic insufficiency (Figures 2a-c). Course: Mr A was diagnosed with acute aortic dissection with modsevere AR and acute heart failure in context with Lower respiratory tract infection. He was immediately referred to cardiothoracic surgeon and was operated the same day. Operative findings revealed ascending aortic aneurysm 8 cms. Dissection within the aneurysm and tears at Sino tubular junction and arch. Severe aortic incompetence due to dilated root and normal leaflets. Surgery included tube graft replacement of root, ascending and arch with preservation and reimplantation of valve leaflets within the tube graft [David’s Procedure]. Post-operative period was complicated with bleeding renal impairment requiring temporary dialysis and hepatic impairment. He was subsequently discharged with normal renal and hepatic function. Figure 2a: Echocardiogram showing intimal tear/flap. Discussion What are anabolic steroids? Anabolic-androgenic steroids (AAS) are synthetically produced variants of the naturally occurring male sex hormone testosterone. “Anabolic” refers to muscle-building, and “androgenic” refers to increased male sexual characteristics. Figure 2b: Echocardiogram (short axis) showing intimal flap in aorta. Why are steroids abused? Fueled by money and desire to excel, steroids dominated the world of sports. Abuse began shortly after creation of and the discovery of performance enhancement effects. What are the physical and psychological dangers? There are many short term and long term effects of steroid abuse. Short term effects are fairly well known and most are reversible with discontinuation of use. Long term effects are more prevalent in women. Possible side effects include • High blood cholesterol levels • Severe acne • Thinning of hair or baldness J Cardiovasc Dis Diagn ISSN: 2329-9517 JCDD, an open access journal Figure 2c: Enlarged parasternal view showing mobile intimal flaps in the aorta. Volume 2 • Issue 3 • 1000152 Citation: Barman M, Djamel B, Mathews J (2014) Acute Aortic Dissection in a Young Healthy Athlete with Androgenic Anabolic Steroid Use: A Case Report from Qatar. J Cardiovasc Dis Diagn 2: 152. doi:10.4172/2329-9517.1000152 Page 3 of 4 Male side effects Congestive heart failure without pain • Decrease in sperm production Cerebrovascular accident without pain • Breast and prostate enlargement Abnormal chest roentgenogram without pain • Sterility Pulse loss without pain • Loss of sexual drive • Wasting away of tissue of the testicles Aortic dissection- differential diagnosis Acute coronary syndrome with and without ST-elevation Female side effects Aortic regurgitation without dissection • Menstrual irregularity Aortic aneurysms without dissection • Infertility Musculoskeletal pain • Permanent effects such as facial hair, a deepened voice, enlarged Pericarditis clitoris and decrease in breast size Mediastinal tumors Short term psychological effects include Pleuritis • Depression • Nervousness • Irritability • Mood swings • Hostility and aggression, commonly known as “roid rage” • Impaired judgment Pulmonary embolism Cholecystitis Atherosclerotic or cholesterol embolism (Table 1) Hypertension is a main risk factor of aortic sclerosis and subsequent aortic aneurysm formation and aortic dissection. Smoking and hypercholesterolemia are additional risk factors. 15%–20% of death secondary to high speed accidents are related to aortic trauma frequently associated with myocardial contusion. Iatrogenic aortic dissection is often related to cardiac catheterization, angioplasty, or surgery. Inflammatory diseases can affect the aorta as in Takayasu arteritis and syphilis as well as in Behcet’s or Ormond’s disease. Cocaine and amphetamine associated with aortic aneurysm formation and dissection are newly detected etiologies Aortic dissection - common presenting symptoms Pain -Pain alone -Pain with syncope -Pain with signs of congestive heart failure -Pain with cerebrovascular accident (stroke) Disease/Condition The cardiovascular system adapts to exercise. Top-level training is often associated with morphological changes in the heart including increases in the left ventricular chamber size, wall thickness, and mass. The increase in the left ventricular mass as a result of training is called” athletes’ heart” [5]. Morgan Roth et al. [6] distinguished two different morphological forms of athletes’ heart: a strength-trained heart and an endurance-trained heart. According to their theory, athletes involved in endurance training, sports with a high dynamic component like running, are presumed to demonstrate eccentric left ventricular hypertrophy, characterized an unchanged relationship between left ventricular wall thickness and left ventricular radius (i.e. ratio of wall thickness to radius), which means an increased left ventricular chamber size with a proportional increase in wall thickness. On the other hand, strength-trained athletes involved in mainly static or isometric exercise like weightlifting, bodybuilding, and wrestling, are presumed to demonstrate concentric left ventricular hypertrophy, which is characterized by an increased ratio of wall thickness to radius, which means an increased left ventricular wall thickness with an unchanged left ventricular chamber size. In addition to the aforementioned changes, in weightlifters as strength-trained athletes, cardiac output, heart rate, and blood pressure tend to increase. A rapid increase in the systemic arterial blood without a decrease in the peripheral vascular resistance, in combination with aortic medial degeneration, may contribute to Differentiating Signs/Symptoms Differentiating Tests Chest pain is typically pressing. There may be a history of prior exertional chest pain. ECG and troponin T may indicate myocardial infarction or ischemia. ST segment depression may occur in acute dissection, but ST elevation rare. Pericarditis Chest pain typically pleuritic. ECG typically shows diffuse ST elevation. Aortic aneurysm Stable (nondissecting and nonleaking) aneurysms are asymptomatic. Diagnosis is usually incidental to workup for another entity. CT scan of the chest does not show dissection. Musculoskeletal pain Pain may be reproducible on palpation of the affected area. CT scan of the chest does not show dissection. Pulmonary embolus Dyspnea, hypoxia, and pleuritic chest pain. There may be evidence of deep vein thrombosis: for example, calf swelling or tenderness. CT scan of the chest shows pulmonary embolus. Mediastinal tumor Possible cough or hemoptysis. CT scan of the chest shows evidence of tumor. Acute coronary syndrome Table 1: Differential Diagnosis. J Cardiovasc Dis Diagn ISSN: 2329-9517 JCDD, an open access journal Volume 2 • Issue 3 • 1000152 Citation: Barman M, Djamel B, Mathews J (2014) Acute Aortic Dissection in a Young Healthy Athlete with Androgenic Anabolic Steroid Use: A Case Report from Qatar. J Cardiovasc Dis Diagn 2: 152. doi:10.4172/2329-9517.1000152 Page 4 of 4 the development of the aortic dissection [7]. This is an event that may occur in non-trained weightlifters or those with predisposing factors for aortic dissection, like hypertension, congenital cardiovascular disease (e.g. coarctation of aorta, congenital stenotic aortic valve, and unicuspid and bicuspid aortic valve), supravalvular aortic stenosis, connective tissue disorders (e.g. the Marfan syndrome and familial cystic medial degeneration syndromes), and fibro muscular dysplasia. Also in athletes who have mild-to-moderate aortic enlargement, an increased blood pressure due to heavy weightlifting, raises aortic wall stress to a level that begets aortic dissection [8]. Aortic dissection is a very tragic event because of its high mortality rate of about 32%, and the most common causes of death after aortic dissection involving the ascending aorta include the rupture into the pericardial cavity with resultant tamponade, occlusion of the coronary arteries, and free rupture into the chest or abdomen (Figure 3) [2]. The majority of reports describe ascending Aortic dissection (the area of greatest hemodynamic stress), which is also the most common location for dissection secondary to connective tissue disorders and congenital anomalies [2]. In these cases, the medial portion of the aorta is weakened not from hypertension induced degeneration (as is the case with the older population), but instead is secondary to a congenital defect [1]. Perhaps the most well-known connective tissue disorder is Marfan’s syndrome. Recent work suggests that aortic involvement may be related to premature termination codon mutations and to other mutations in the gene for fibrillin-1 (chromosome 15q21.1) [9]. All athletes must be assessed for predisposing factors for aortic dissection, and all patients should be encouraged to undergo appropriate diagnostic studies like echocardiography and blood pressure monitoring while weightlifting to recognize possible predisposing factors for aortic dissection. Athletes who do have a problem should be encouraged to avoid or limit their exercise or activity by their cardiologist. It is vital that this disastrous event be prevented in young people. Prevention of aortic dissection in inherited diseases (Marfan’s Syndrome, Ehlers-Danlos Syndrome, Annuloaortic ectasia) [10] 1. Life-long beta-adrenergic blockade 2. Periodic routine imaging of the aorta 3. Prophylactic replacement of the aortic root before diameter exceeds 5·0 cm in patients with family history of dissection 4. Prophylactic replacement of the aortic root before diameter exceeds 5·5 cm + C 5. Moderate restriction of physical activity Conclusion In conclusion, although a rare occurrence, AD should be considered in symptomatic patients with any family history of early cardiac deaths, a history suggestive of a connective tissue disorder (that is, multiple joint surgeries) or whopractice weightlifting. The investigation and surveillance of fibrillinopathies patients is ill defined,but prompt referral and/or admission for further investigation is merited. Cessation of weight lifting or isotonic stress activities until a definitive investigation has been obtained is prudent. Data for Anabolic steroids usage and acute aortic dissection is inadequate till date but the associations have been infrequently reported, so an alert and suspicious mind in the ER should be always welcome. References 1. Biddinger A, Rocklin M, Coselli J, Milewicz DM (1997) Familial thoracic aortic dilatations and dissections: a case control study. J Vasc Surg 25: 506-511. 2. Gammie JS, Katz WE, Swanson ER, Peitzman AB (1996) Acute aortic dissection after blunt chest trauma. J Trauma 40: 126-127. 3. Fikar CR, Koch S (2000) Etiologic factors of acute aortic dissection in children and young adults. ClinPediatr (Phila) 39: 71-80. 4. Corrado D, Pelliccia A, Bjornstad HH, Vanhees L, Biffi A, et al. (2005) Cardiovascular pre-participation screening of young competitive athletes for prevention of sudden death: proposal for a common European protocol. Consensus Statement of the Study Group of Sport Cardiology of the Working Group of Cardiac Rehabilitation and Exercise Physiology and the Working Group of Myocardial and Pericardial Diseases of the European Society of Cardiology. Eur Heart J 26:516-524. 5. Pluim BM, Zwinderman AH, van der Laarse A, van der Wall EE (2000) The athlete’s heart. A meta-analysis of cardiac structure and function. Circulation 101: 336-344. 6. Morganroth J, Maron BJ, Henry WL, Epstein SE (1975) Comparative left ventricular dimensions in trained athletes. Ann Intern Med 82: 521-524. 7. de Virgilio C, Nelson RJ, Milliken J, Snyder R, Chiang F, et al. (1990) Ascending aortic dissection in weight lifters with cystic medial degeneration. Ann ThoracSurg 49: 638-642. 8. Hatzaras I, Tranquilli M, Coady M, Barrett PM, Bible J, et al. (2007) Weight lifting and aortic dissection: more evidence for a connection. Cardiology 107: 103-106. 9. Hogan CJ (2005) An aortic dissection in a young weightlifter with nonMarfanfibrillinopathy.Emerg Med J22: 304-305. 10.Erbel R, Alfonso F, Boileau C, Dirsch O, Eber B, et al. (2001) Diagnosis and management of aortic dissection. Eur Heart J 22: 1642-1681. DeBakey Stanford I II A Figure 3: Classification of Aortic dissection. J Cardiovasc Dis Diagn ISSN: 2329-9517 JCDD, an open access journal III B Citation: Barman M, Djamel B, Mathews J (2014) Acute Aortic Dissection in a Young Healthy Athlete with Androgenic Anabolic Steroid Use: A Case Report from Qatar. J Cardiovasc Dis Diagn 2: 152. doi:10.4172/2329-9517.1000152 Volume 2 • Issue 3 • 1000152