Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
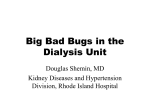
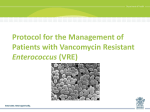
Journal of Hospital Infection 88 (2014) 170e176 Available online at www.sciencedirect.com Journal of Hospital Infection journal homepage: www.elsevierhealth.com/journals/jhin Impact of contact precautions on falls, pressure ulcers and transmission of MRSA and VRE in hospitalized patients S. Gandra a, *, C.M. Barysauskas b, D.A. Mack c, B. Barton b, R. Finberg a, R.T. Ellison III a a Division of Infectious Disease and Immunology, University of Massachusetts Medical School, Worcester, MA, USA Quantitative Health Sciences, University of Massachusetts Medical School, Worcester, MA, USA c Infection Control Department, UMass Memorial Medical Center, Worcester, MA, USA b A R T I C L E I N F O Article history: Received 27 February 2014 Accepted 10 September 2014 Available online 28 September 2014 Keywords: Contact precautions MRSA VRE Falls Pressure ulcers Transmission S U M M A R Y Background: Hospitals use contact precautions to prevent the spread of meticillinresistant Staphylococcus aureus (MRSA) and vancomycin-resistant enterococci (VRE). There is concern that contact precautions may have adverse effects on the safety of isolated patients. In November 2010, the infection control policy at an academic medical centre was modified, and contact precautions were discontinued for patients colonized or infected with MRSA or VRE (MRSA/VRE patients). Aim: To assess the rates of falls and pressure ulcers among MRSA/VRE patients and other adult medical-surgical patients, as well as changes in MRSA and VRE transmission before and after the policy change. Methods: A single-centre retrospective hospital-wide cohort study was performed from 1st November 2009 to 31st October 2011. Findings: Rates of falls and pressure ulcers were significantly higher among MRSA/VRE patients compared with other adult medical-surgical patients before the policy change (falls: 4.57 vs 2.04 per 1000 patient-days, P < 0.0001; pressure ulcers: 4.87 vs 1.22 per 1000 patient-days, P < 0.0001) and after the policy change (falls: 4.82 vs 2.10 per 1000 patient-days, P < 0.0001; pressure ulcers: 4.17 vs 1.19 per 1000 patient-days, P < 0.0001). No significant differences in the rates of falls and pressure ulcers among MRSA/VRE patients were found after the policy change compared with before the policy change. There was no overall change in MRSA or VRE hospital-acquired transmission. Conclusion: MRSA/VRE patients had higher rates of falls and pressure ulcers compared with other adult medical-surgical patients. Rates were not affected by removal of contact precautions, suggesting that other factors contribute to these complications. Further research is required among this population to prevent complications. ª 2014 The Healthcare Infection Society. Published by Elsevier Ltd. All rights reserved. * Corresponding author. Address: Center for Disease Dynamics, Economics and Policy, 1616 P Street NW, Suite 430, Washington, DC 20036, USA. Tel.: þ91 9810912566; fax: þ1 202 939 3460. E-mail address: [email protected] (S. Gandra). http://dx.doi.org/10.1016/j.jhin.2014.09.003 0195-6701/ª 2014 The Healthcare Infection Society. Published by Elsevier Ltd. All rights reserved. S. Gandra et al. / Journal of Hospital Infection 88 (2014) 170e176 Introduction 171 All adult patients were reviewed retrospectively one year before and one year after the policy change at the University of Massachusetts Memorial Medical Center (Memorial and University campuses). The hospital-wide cohort study was approved by the University of Massachusetts Medical School Institutional Review Board. The Centers for Disease Control and Prevention (CDC) recommend the use of transmission-based contact precautions for patients with documented or suspected infection or colonization with epidemiologically important pathogens.1 Based on these recommendations, many acute care facilities use infection control contact precautions to prevent the spread of multi-drug-resistant organisms, such as meticillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant enterococci (VRE). Patients placed under contact precautions are housed in private hospital rooms, and all healthcare workers involved in patient care are required to wear a gown and gloves while in the patient’s room. However, while contact precautions are in common use, their efficacy in controlling the transmission of multi-drug-resistant organisms is unclear, compliance is poor, and contact precautions may result in unintended harmful consequences.2e7 Specifically, reported consequences of contact precautions include: reduced patient contact with healthcare workers;2,8e12 increased numbers of preventable adverse events;13e15 decreased psychological well-being;7 decreased patient satisfaction;13 delays in access to radiological examinations;16 and decreased quality of hospital care.17 Stelfox et al. reported that patients placed under contact precautions were eight times more likely to experience supportive care failures (e.g. falls, pressure ulcers, and fluid or electrolyte disturbances) than patients who were not placed under contact precautions.13 Unfortunately, the prevalence of MRSA and VRE infection has increased in acute care, chronic care and community settings, thus increasing the number of patients at risk of potential complications from contact precautions. On 1st November 2010, the infection control policy of the University of Massachusetts Memorial Medical Center, Worcester, MA, USA was changed to discontinue the use of contact precautions among patients colonized or infected with MRSA or VRE (MRSA/VRE patients). Noting the work of Stelfox et al.,13 the impact of the policy change on rates of falls and new-onset pressure ulcers among MRSA/VRE patients compared with the general patient population was studied. It was hypothesized that the rates of complications would decrease among MRSA/VRE patients, and the rate of hospital-acquired MRSA or VRE transmission would remain constant. All patients admitted to the University of Massachusetts Memorial Medical Center adult medical-surgical inpatient units from 1st November 2009 to 31st October 2011 were included in this study. Paediatric, maternity and psychiatric inpatient wards were excluded. Patients who fell or developed a newonset Stage 2 (or greater) pressure ulcer during hospitalization were identified through mandatory reports entered into the web-based incident reporting system (STARZ, Chicago, USA). Only one fall and one pressure ulcer per admission were included amongst patients with multiple events. All MRSA/VRE patients admitted during the study period were identified using an infection control data management system (Theradoc, Salt Lake City, USA). All colonized or infected inpatient falls and pressure ulcers were identified at least two days after MRSA or VRE identification. As the study objective was to assess the impact of contact precautions, MRSA/VRE patients who were placed under contact precautions for other reasons after the policy change were excluded from the analysis. The total number of MRSA and VRE patient-days was calculated from Theradoc, and the total number of adult medical-surgical patient-days was calculated from hospital census data. Hospital MRSA and VRE acquisition rates were calculated using the standard CDC national healthcare safety network definition for all actively and passively obtained cultures.18 Active surveillance was performed on admission and weekly for both MRSA and VRE in the institution’s seven adult intensive care units, and for VRE alone in the bone marrow transplant unit. Passive surveillance for MRSA and VRE was performed throughout the study period in all other inpatient units. Patient characteristics including age, gender, date and unit of occurrence, length of hospital stay and Braden scale score19 (risk for pressure ulcer development) were obtained from STARZ, and the Charlson comorbidity index was calculated through medical record review. Methods Outcome measures Design and setting First, the rates of falls and pressure ulcers among adult MRSA/VRE patients were compared before and after the policy change. In addition, the rates of falls and pressure ulcers among adult MRSA/VRE patients were compared with the rates among other adult medical-surgical patients before and after the policy change. Further, due to the association between disease severity and the occurrence of falls20 and pressure ulcers,21 the degree of comorbidity in MRSA/VRE patients was compared with the degree of comorbidity in other medical-surgical patients using the Charlson comorbidity index.22 Finally, the impact of the policy change on hospital-associated MRSA and VRE transmission was assessed. On 1st November 2010, the University of Massachusetts Memorial Medical Center discontinued the use of contact precautions for MRSA/VRE patients. Patients colonized or infected with selected multi-drug-resistant organisms (e.g. extendedspectrum beta-lactamase-positive or carbapenemase-positive Gram-negative organisms, other highly multi-drug-resistant Gram-negative bacteria or vancomycin-resistant S. aureus), as well as those soiling the environment with secretions due to active draining wounds, diarrhoeal disease or uncontrolled respiratory secretions, continued to be placed under contact precautions. Study participants and data collection 172 S. Gandra et al. / Journal of Hospital Infection 88 (2014) 170e176 Statistical methods Demographic and clinical characteristics of MRSA and VRE patient groups were compared using Chi-squared statistic for categorical data and Student’s t-test for continuous data. Rates of falls and pressure ulcers for each group were reported as per 1000 patient-days. A Z-test was used to compare the rates between the groups. A sensitivity analysis was performed to assess the difference in the rates of falls and pressure ulcers between MRSA/VRE patients and other adult medical-surgical patients if there was misassignment of 2500 patient-days between the groups. Fifty MRSA/VRE patients with falls and pressure ulcers were matched at random [1:1 on hospital unit and admission date ( 30 days)] with 50 MRSA/VRE patients without falls and pressure ulcers, 50 other adult medical-surgical patients with falls and pressure ulcers, and 50 other adult medical-surgical patients without falls and pressure ulcers. Student’s t-test was used to compare the Charlson comorbidity indexes between groups. An interrupted time-series analysis was performed to estimate monthly changes in MRSA and VRE acquisition rates before and after the policy change for the study period. P 0.05 was considered to indicate significance. All statistical analyses were performed using SAS Version 9.3 (SAS Institute, Inc., Cary, NC, USA). Results compared with before the policy change (Table I). No significant difference in the Braden score for MRSA/VRE patients who developed pressure ulcers was found after the policy change compared with before the policy change. Number of falls and pressure ulcers during study period In total, 741 falls and 491 new-onset Stage 2 (or greater) pressure ulcers occurred during the two-year study period. Among MRSA/VRE patients, there were 77 falls and 82 pressure ulcers during the year before the policy change, and 82 falls and 71 pressure ulcers during the year after the policy change. Corresponding figures for other adult medical-surgical patients were 288 falls and 172 pressure ulcers, and 294 falls and 166 pressure ulcers. Total number of patient-days For MRSA/VRE patients, there were 16,822 patient-days during the year before the policy change and 17,012 patientdays during the year after the policy change. Corresponding figures for other adult medical-surgical patients were 140,690 and 139,466 patient-days. Rates of falls and pressure ulcers before and after the policy change Patient characteristics No significant differences were observed between demographic and clinical covariates for MRSA/VRE patients who had a fall or developed a pressure ulcer after the policy change No significant differences in the rates of falls among MRSA/VRE patients and among other adult medical-surgical patients were found after the policy change compared with before the policy change (Table II). The rate of pressure ulcers Table I Demographic and clinical characteristics of patients colonized or infected with meticillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci (VRE) who sustained a fall or developed a pressure ulcer Falls before policy Falls after policy P-value Pressure ulcers before Pressure ulcers after P-value change (N ¼ 77) change (N ¼ 82)a policy change (N ¼ 82) policy change (N ¼ 71)b Patient characteristics Age, mean (SD) Male (%) LOS, mean days (SD) MRSA (%) VRE (%) MRSA and VRE (%) Colonized (%) Infected (%) CCI, mean (SD) Braden score, mean (SD) Unit characteristics Medicine (%) Surgery (%) Critical care (%) 66.1 47 15.4 25 38 14 69 8 3 (14.3) (61%) (14.7) (32.5%) (49.4%) (18.2%) (89.6%) (10.4%) (2.1) NA 59 (76.6%) 9 (11.7%) 9 (11.7%) 63.7 51 18.2 37 29 16 69 13 3.4 (15.8) (62%) (17.6) (45.1%) (35.4%) (19.5%) (84.2%) (15.8%) (2.7) NA 0.32 0.88 0.27 0.10 0.07 0.83 0.31 0.31 0.33 e 64 (78.1%) 11 (13.4%) 7 (8.5%) 0.83 0.74 0.51 64.5 52 30.1 27 34 21 57 25 3.9 9.5 (15.5) (63%) (24.7) (39.2%) (41.5%) (25.6%) (69.5%) (30.5%) (2.6) (7.4) 31 (37.8%) 8 (9.8%) 43 (52.4%) 65.7 40 23.8 21 33 17 48 23 3.5 8.3 (15) (57%) (18.6) (29.6%) (46.5%) (23.9%) (67.6%) (32.4%) (1.8) (8.2) 0.63 0.47 0.08 0.66 0.53 0.81 0.80 0.80 0.34 0.34 28 (39.4%) 9 (12.7%) 34 (49.9%) 0.84 0.57 0.57 CCI, Charlson comorbidity index; LOS, length of stay in hospital; NA, not applicable; SD, standard deviation. a Eight patients colonized or infected with MRSA or VRE were excluded as they were placed under contact precautions (Clostridium difficile, N ¼ 2; multi-drug-resistant organisms, N ¼ 3; extended-spectrum beta-lactamase-positive organisms, N ¼ 3). b Seventeen patients colonized or infected with MRSA or VRE were excluded as they were placed under contact precautions (extendedspectrum beta-lactamase-positive organisms, N ¼ 8; Clostridium difficile, N ¼ 7; multi-drug-resistant organisms, N ¼ 2). S. Gandra et al. / Journal of Hospital Infection 88 (2014) 170e176 Table II Rates of falls and pressure ulcers in patients colonized or infected with meticillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci (VRE) and other adult medicalsurgical patients before and after the policy change MRSA/VRE patients (rate per 1000 patient-days) Before policy change Falls 4.57 Pressure 4.87 ulcers After policy change Falls 4.82 Pressure 4.17 ulcers P-value Falls 0.74a Pressure 0.33c ulcers Other adult medical-surgical patients (rate per 1000 patient-days) P-value 2.04 1.22 <0.0001 <0.0001 2.10 1.19 <0.0001 <0.0001 0.72b 0.80d a Comparing rate of falls among MRSA/VRE patients. Comparing rate of falls among other adult medical-surgical patients. c Comparing rate of pressure ulcers among MRSA/VRE patients. d Comparing rate of pressure ulcers among other adult medicalsurgical patients. b among MRSA/VRE patients decreased after the policy change; however, this was not statistically significant. Rates of falls and pressure ulcers in MRSA/VRE patients compared with other adult medical-surgical patients A significant difference was found between the rate of falls among MRSA/VRE patients compared with other adult medicalsurgical patients before the policy change (4.57 vs 2.04 per 1000 patient-days; P < 0.0001) and after the policy change (4.82 vs 2.10 per 1000 patient-days; P < 0.0001) (Table I). Similarly, there was a significant difference in the rate of pressure ulcers among MRSA/VRE patients compared with other adult medical-surgical patients before the policy change (4.87 vs 1.22 per 1000 patient-days; P < 0.0001) and after the policy change (4.17 vs 1.19 per 1000 patient-days; P < 0.0001) (Table II). 173 Table III Comparison of mean Charlson comorbidity index among various groups of patients colonized or infected with meticillin-resistant Staphylococcus aureus (MRSA) or vancomycin-resistant enterococci (VRE) and other adult medical-surgical patients Groups compared 1. All MRSA/VRE patients vs other adult medical-surgical patients 2. All patients before vs after policy change 3. MRSA/VRE patients with fall vs no fall before policy change 4. MRSA/VRE patients with fall vs no fall after policy change 5. Other adult medical-surgical patients with fall vs no fall before policy change 6. Other adult medical-surgical patients with fall vs no fall after policy change 7. MRSA/VRE patients with fall before vs after policy change 8. Other adult medical-surgical patients with fall before vs after policy change 9. MRSA/VRE patients with PU vs no PU before policy change 10. MRSA/VRE patients with PU vs no PU after policy change 11. Other adult medical-surgical patients with PU vs no PU before policy change 12. Other adult medical-surgical patients with PU vs no PU after policy change 13. MRSA/VRE patients with PU before vs after policy change 14. Other adult medical-surgical patients with PU before vs after policy change Mean Charlson P-value comorbidity index 3.32 vs 2.75 0.002 3.08 vs 3.12 0.81 3.04 vs 2.97 0.86 3.43 vs 2.93 0.23 2.48 vs 2.30 0.68 2.70 vs 2.88 0.73 3.04 vs 3.44 0.33 2.48 vs 2.70 0.64 3.75 vs 2.90 0.03 3.42 vs 3.52 0.81 3.46 vs 2.48 0.04 3.46 vs 2.22 0.006 3.75 vs 3.43 0.38 3.46 vs 3.46 1.00 PU, pressure ulcer. The mean Charlson comorbidity index was also significantly higher for individuals who developed a pressure ulcer, but not for those who sustained falls (Table III). Sensitivity analysis The sensitivity analysis revealed that the rates of falls and pressure ulcers among MRSA/VRE patients and other adult medical-surgical patients remained unaffected by the policy change. Charlson comorbidity index score in MRSA/VRE patients vs other adult medical-surgical patients The mean Charlson comorbidity index was significantly higher among MRSA/VRE patients compared with other adult medical-surgical patients (3.32 vs 2.75; P ¼ 0.0002) (Table III). Hospital-associated MRSA and VRE transmission using interrupted time-series analysis The MRSA acquisition rate prior to the policy change was 0.77 cases per 1000 patients. After the policy change, acquisition increased immediately by 0.12 cases per 1000 patients (P ¼ 0.510), and then decreased by 0.017 cases per 1000 per month for the remainder of the study period (Figure 1). Overall, there was no change in MRSA acquisition during the study period (P ¼ 0.695). The VRE acquisition rate was 1.39 cases per 1000 patients. After the policy change, acquisition increased immediately by S. Gandra et al. / Journal of Hospital Infection 88 (2014) 170e176 a b 0.4 MRSA acquisition rate (per 1000) 0.6 0.8 1 1.2 174 0 5 10 15 Study month 20 25 Figure 1. Hospital-associated acquisition rates for meticillin-resistant Staphylococcus aureus (MRSA) from November 2009 to October 2011. (a) Before implementation of policy change, (b) after implementation of policy change. 0.80 cases per 1000 patients (P ¼ 0.004), and then decreased by 0.016 cases per 1000 per month for the remainder of the study period (Figure 2). There was no overall change in VRE acquisition during the study period (P ¼ 0.438). Discussion a b 0.5 VRE acquisition rate (per 1000) 1.0 1.5 2 Several studies have assessed the harmful effects of contact precautions.2,8e12,15e17 However, only two studies have reported on falls and pressure ulcers.13,14 Stelfox et al. performed a matched cohort study between 1999 and 2002 at two academic medical centres in North America.13 Among patients colonized or infected with MRSA, they found that patients placed under contact precautions were eight times more likely to experience supportive care failures including falls and pressure ulcers compared with patients who were not placed under contact precautions.13 Karki et al. compared the rates of adverse events among Australian patients colonized or infected with VRE prior to and subsequent to initiation of contact precautions, and demonstrated an increased risk among patients with pressure ulcers after initiation of contact precautions.14 Both studies hypothesized that the use of contact precautions contributed to adverse events. The present study demonstrated among an inpatient population that MRSA/VRE patients were at a greater risk of falls or pressure ulcers compared with other medical-surgical patients, regardless of the use of contact precautions. To the authors’ knowledge, this is the first study to assess the impact of discontinuation of contact precautions on the rates of falls and pressure ulcers among MRSA/VRE patients, and hospital transmission of MRSA and VRE. This study included all adult hospitalized patients admitted to the regular acute 0 5 10 15 Study month 20 25 Figure 2. Hospital-associated acquisition rates for vancomycin-resistant enterococci (VRE) from November 2009 to October 2011. (a) Before implementation of policy change, (b) after implementation of policy change. S. Gandra et al. / Journal of Hospital Infection 88 (2014) 170e176 care medical and surgical floors of a two-campus academic medical centre over the two-year study period. The study population consisted of 6400 MRSA/VRE patients and 65,000 general medical-surgical patients. The rates of falls and pressure ulcers were significantly higher among MRSA/VRE patients compared with other adult medical-surgical patients before and after the policy change. The rate of falls was two times higher in MRSA/VRE patients compared with other adult medical-surgical patients before and after the policy change. Similarly, the rate of pressure ulcers was at least three times higher in MRSA/VRE patients compared with other adult medical-surgical patients before and after the policy change. These results are consistent with the findings of Stelfox et al. that patients who are colonized or infected with MRSA and placed under contact precautions are at significantly higher risk of falls and pressure ulcers.13 It was hypothesized that the removal of contact precautions would decrease the rates of falls and pressure ulcers among MRSA/VRE patients to rates similar to the general adult patient population. However, after the policy change, the overall increased risk of these adverse events persisted among MRSA/VRE patients. Previous studies have shown an association between higher Charlson comorbidity indexes and the occurrence of falls20 and pressure ulcers,21 and further analysis demonstrated that MRSA/VRE patients had higher Charlson comorbidity indexes compared with other adult medicalsurgical patients. No overall change in MRSA and VRE transmission was identified during the two-year study period. However, an initial spike in VRE acquisition after the policy change was noted in the analysis. This increased incidence correlated with a cluster of patients with VRE in one intensive care unit. The increased rate of VRE acquisition decreased steadily after the policy change, with rates returning to just below the level at the beginning of the study. There was no significant increase in VRE acquisition at the end of the study compared with the beginning of the study. It is unclear whether this initial increase was due to factors related to the policy change, or due to normal cyclical trends seen with VRE acquisition at the study institution. This study has several limitations. First, it was a retrospective study; therefore, causality cannot be inferred. It has been assumed that all institution-based infection control practices were followed throughout the study period. Second, it was hypothesized that removing contact precautions would increase the access of healthcare workers to patients; however, this was not addressed in the study. Third, previous reviews identified several risk factors for falls23 and pressure ulcers;24 however, it was not possible to investigate these risk factors further in this study. Fourth, this study was limited as it was an unadjusted analysis given the large population size. Fifth, the surveillance database used in patient identification of MRSA or VRE was not confirmed. Therefore, the number of newly infected or colonized patients in the study population may have been overestimated if the patients in the study period had been colonized or infected with MRSA or VRE previously but this was not active at the time of acute hospitalization. In addition, patients were identified as being infected with MRSA or VRE based on microbiology results; however, the presence of organisms in culture may not verify true infection in some cases. Sixth, the accuracy of the falls and pressure ulcer data obtained from the risk management database was 175 not verified; however, this information must be publicly reported to the Centers of Medicare and Medicaid Services by acute care hospitals as hospital-acquired condition measures. Seventh, MRSA and VRE surveillance in the study hospital only involves active screening in the intensive care units. This technique is accepted by infectious disease societies as a sufficient method to determine hospital-wide MRSA/VRE disease incidence and prevalence adequately and accurately;25 however, it could theoretically lead to under-recognition of MRSA/ VRE cases and acquisition. The surveillance standard and the potential for underestimation remained constant throughout the study period; therefore, it is not believed to have had a significant impact on the observed results. Lastly, the study findings are limited by the short two-year study period. During this period, only a small number of falls and pressure ulcers occurred in the MRSA/VRE patients, and the time period may have been too short to allow accurate assessment of longitudinal changes in the rates of MRSA or VRE transmission. Given these limitations, there is a need for a more rigorous multicentre prospective study with adequate follow-up time to confirm the findings of this study. In summary, this study found that patients colonized or infected with MRSA or VRE were at significantly higher risk of falls and pressure ulcers than the general adult medical- surgical patient population. Simply removing the routine use of contact precautions for this patient population did not affect the increased incidence of falls, although it was associated with a decreasing trend in the incidence of pressure ulcers. This study demonstrated that MRSA/VRE patients are significantly more ill than other medical-surgical patients; this is a major concern given that the previous literature suggests that patients placed under contact precautions receive less interaction with healthcare workers. These findings should be considered when planning the treatment of infected or colonized patients, and the modification of infection control isolation polices. Acknowledgements Preliminary data were published in abstract form and presented at the Annual Meeting of the Infectious Disease Society of America on 19th October 2012. Conflict of interest statement None declared. Funding source None. References 1. Siegel JD, Rhinehart E, Jackson M, Chiarello L. 2007 Guideline for isolation precautions: preventing transmission of infectious agents in health care settings. Am J Infect Control 2007;35:S65eS164. 2. Morgan DJ, Pineles L, Shardell M, et al. The effect of contact precautions on healthcare worker activity in acute care hospitals. Infect Control Hosp Epidemiol 2013;34:69e73. 3. Manian FA, Ponzillo JJ. Compliance with routine use of gowns by healthcare workers (HCWs) and non-HCW visitors on entry into the rooms of patients under contact precautions. Infect Control Hospital Epidemiol 2007;28:337e340. 176 S. Gandra et al. / Journal of Hospital Infection 88 (2014) 170e176 4. Huskins WC, Huckabee CM, O’Grady NP, et al. Intervention to reduce transmission of resistant bacteria in intensive care. N Engl J Med 2011;364:1407e1418. 5. Kirkland KB. Improving healthcare worker hand hygiene: show me more! Qual Saf Health Care 2009;18:419. 6. Morgan DJ, Diekema DJ, Sepkowitz K, Perencevich EN. Adverse outcomes associated with contact precautions: a review of the literature. Am J Infect Control 2009;37:85e93. 7. Abad C, Fearday A, Safdar N. Adverse effects of isolation in hospitalised patients: a systematic review. J Hosp Infect 2010;76:97e102. 8. Kirkland KB, Weinstein JM. Adverse effects of contact isolation. Lancet 1999;354:1177e1178. 9. Saint S, Higgins LA, Nallamothu BK, Chenoweth C. Do physicians examine patients in contact isolation less frequently? A brief report. Am J Infect Control 2003;31:354e356. 10. Evans HL, Shaffer MM, Hughes MG, et al. Contact isolation in surgical patients: a barrier to care? Surgery 2003;134:180e188. 11. Masse V, Valiquette L, Boukhoudmi S, et al. Impact of methicillin resistant Staphylococcus aureus contact isolation units on medical care. PloS One 2013;8:e57057. 12. Harris AD, Pineles L, Belton B, et al. Universal glove and gown use and acquisition of antibiotic-resistant bacteria in the ICU: a randomized trial. JAMA 2013;310:1571e1580. 13. Stelfox HT, Bates DW, Redelmeier DA. Safety of patients isolated for infection control. JAMA 2003;290:1899e1905. 14. Karki S, Leder K, Cheng AC. Patients under contact precautions have an increased risk of injuries and medication errors: a retrospective cohort study. Infect Control Hosp Epidemiol 2013;34:1118e1120. 15. Zahar JR, Garrouste-Orgeas M, Vesin A, et al. Impact of contact isolation for multidrug-resistant organisms on the occurrence of medical errors and adverse events. Intens Care Med 2013;39:2153e2160. 16. Karki S, Leder K, Cheng AC. Delays in accessing radiology in patients under contact precautions because of colonization with 17. 18. 19. 20. 21. 22. 23. 24. 25. vancomycin-resistant enterococci. Am J Infect Control 2013;41:1141e1142. Morgan DJ, Day HR, Harris AD, Furuno JP, Perencevich EN. The impact of contact isolation on the quality of inpatient hospital care. PloS One 2011;6:e22190. Centers for Disease Control and Prevention. The National Healthcare Safety Network (NHSN) manual. Patient safety component protocol. Atlanta, GA: Division of Healthcare Quality Promotion, CDC. Available at: http://www.cdc.gov/ncidod/ dhqp/pdf/nhsn/NHSN_Manual_PatientSafetyProtocol_CURRENT. pdf (last accessed 07.08.14). Bergstrom N, Braden BJ, Laguzza A, Holman V. The Braden scale for predicting pressure sore risk. Nurs Res 1987;36:205e210. Bates DW, Pruess K, Souney P, Platt R. Serious falls in hospitalized patients: correlates and resource utilization. Am J Med 1995;99:137e143. Kalava UR, Cha SS, Takahashi PY. Association between vitamin D and pressure ulcers in older ambulatory adults: results of a matched caseecontrol study. Clin Intervent Aging 2011;6:213e219. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373e383. Evans D, Hodgkinson B, Lambert L, Wood J. Falls risk factors in the hospital setting: a systematic review. Int J Nurs Pract 2001;7:38e45. Coleman S, Gorecki C, Nelson EA, et al. Patient risk factors for pressure ulcer development: systematic review. Int J Nurs Stud 2013;50:974e1003. Muto CA, Jernigan JA, Ostrowsky BE, et al. SHEA guideline for preventing nosocomial transmission of multidrug-resistant strains of Staphylococcus aureus and enterococcus. Infect Control Hosp Epidemiol 2003;24:362e386.