Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
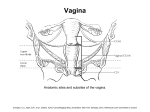
TNM Staging: Colon and Rectum TONYA BRANDENBURG, MHA, CTR KENTUCKY CANCER REGISTRY Overview Colorectal Anatomy Common Terms Rules for Colorectal Cancer Changes in T,N,M Staging from AJCC 6th edition to 7th edition Elements of Staging: TX-T4, NX-N2b, and M0-M1b Stage Groups and Prognostic Factors Helpful Hints Colon/Rectal Examples C18.4 C18.3 C18.5 C18.2 C18.6 C18.0 C18.0 C18.1 C18.7 C18.1 C21.--- C20.9 Not Shown: Rectosigmoid C19.9 Anatomy of the Colon and Rectum RIGHT COLON Appendix (C18.1) Cecum (C18.0): 150 cm from anal verge Ascending Colon (C18.2): 132-150 cm from verge Hepatic Flexure (C18.3) Transverse Colon (C18.4): 82-132 cm from verge LEFT COLON Splenic Flexure (C18.5) Descending Colon (C18.6): 57-82 cm from anal verge Sigmoid Colon (C18.7):17-57 cm from verge Rectosigmoid (C19.9): 1517 cm from verge Rectum (C20.9): 4-16 cm from verge Colon and Rectum Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer Anatomic subsites of the rectum Common Terms . Circumferential margin – Any aspect of the colorectum that is not covered by a serosal layer and must be dissected from the retroperitoneum or subperitoneum to remove the viscus. Familial polyposis, familial adenomatous polyposis (FAP) a condition characterized by the development of many adenomatous polyps, often seen in several members of the same family Polyp, adenoma – These mean the same thing! Adenoma - A benign lesion composed of tubular or villous structures showing intraepithelial neoplasia Non-Peritonealized Surface or Serosalized Area Some colon surfaces have no serosa at the exterior surface (around the hollow organ) The serosa acts as barrier for tumors that begin on inside surface of the colon and invade down into the mucosa and through the wall of the colon (the serosa) When there is no serosa – you lose a natural barrier that helps contain the colon cancer Non-Peritonealized Surfaces in Colon-Rectum: Rectum – no serosa in rectum below peritoneal reflection Descending Colon – no serosa covering posterior surfaces Ascending Colon – no serosa covering posterior surfaces Non-Peritonealized Surface or Serosalized Area No Serosa Here Source: Clinical Anatomy for Medical Students, 5th Edition, Richard S. Snell. Little, Brown and Company, 1995. Rules for Colon/Rectal Cancer Every individual site is a separate primary Use C18.8 for one lesion that overlaps two segments of colon where tumor point of origin cannot be determined Code C18.9 for multiple malignant adenomatous polyps or malignant adenomatous polyposis coli in various segments. Tumor size must be 998; histology = 8220/3 or 8221/3 Code C19.9 if one lesion overlaps the colon and rectum and point of origin cannot be determined If malignant polyp & frank malignancy in same segment of colon, code the frank malignancy Changes in T,N,M Staging for Colon/Rectum from 6th edition to 7th edition Expansion of Stages II and III based on survival and relapse data that was not available for the 6th edition. Subdivision of T4, N1, and N2 M1 Also subdivided: M1a for a single metastatic site, M1b if multiple metastatic sites TNM scheme for carcinoma only; GIST and Neuroendocrine tumors now have their own chapters Elements of Staging: TX, T0, and Tis TX: Tumor not seen on films T0: No evidence of primary tumor (use when you have metastasis that is consistent with colon/rectum primary, but no evidence of a primary tumor can be found) Tis: Tis is confined to glandular basement membrane or lamina propria with NO extent through muscularis mucosa Tumor in stalk of polyp is Tis if limited to lamina propria, but T1, T2, etc. if further invasion is noted Elements of Staging: T1, T2, and T3 T1: Tumor invades the submucosa T2: Tumor invades the muscularis propria T3: Invasion into subserosa, or through subserosa into pericolorectal tissues Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer T1 tumor invades submucosal. Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer T2 tumor invades muscularis propria. Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer T3 tumor invades through the muscularis propria into pericolorectal tissues. Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer Circumferential resection margin. T4a (left side) has perforated the visceral peritoneum. In contrast, T3; R2 (right side) shows macroscopic involvement of the circumferential resection margin of a nonperitonealized surface of the colorectum by tumor with gross disease remaining after surgical excision. Elements of Staging: T4 (T4a and T4b) T4: Tumor directly invades other organs or structures, and/or perforates visceral peritoneum: T4a: tumor penetrates to the surface of the visceral peritoneum T4b: tumor directly invades or is adherent to other organs or structures Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer T4a tumor penetrates to the surface of the visceral peritoneum. The tumor perforates (penetrates) visceral peritoneum, as illustrated here. Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer T4a tumor perforates visceral peritoneum (shown with gross bowel perforation through the tumor). Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer T4b tumor directly invades or is adherent to other organs or structures, as illustrated here with extension into an adjacent loop of small bowel. Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer T4b tumor directly invades or is adherent to other organs or structures (such as the sacrum shown here). Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer The regional lymph nodes of the colon and rectum are colored by anatomic location, e.g., dark brown – right colon and cecum; blue – hepatic flexure to mid transverse colon; red – splenic flexure, left colon and sigmoid colon. Lymphatic Drainage Each subsite of the colon has its own drainage system For all colon subsites, these include: Colic, NOS; Paracolic/ Pericolic. Right Colon Cecum and appendix: Right colic, middle colic Transverse: Middle colic Splenic flexure: Ileocolic, right colic, middle colic Hepatic Flexure: Cecal, anterior & posterior; ileocolic, right colic Ascending: Left Colon Descending colon: Middle colic & left colic; inferior mesenteric Left colic, sigmoid, inferior mesenteric Sigmoid: Sigmoidal, superior hemorrhoidal, superior rectal, inferior mesenteric Satellite Nodules Satellite peritumoral nodule in the pericolorectal tissue of a primary carcinoma without histologic evidence of residual lymph node in the nodule may represent discontinuous spread, venous invasion with extravascular spread, or a totally replaced lymph node Replaced nodes should be counted separately as positive nodes in the N category Elements of Staging: NX, N0, N1a, and N1b NX: Regional lymph nodes can’t be assessed N0: No regional lymph node metastasis N1: Metastasis in 1-3 regional lymph nodes N1a: Metastasis in 1 regional lymph node N1b: Metastasis in 2-3 regional lymph nodes Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer N1a is defined as metastasis in one regional lymph node. Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer N1b is defined as metastasis in 2 to 3 regional lymph nodes. Elements of Staging: N1c N1c: Tumor deposits in the subserosa, mesentery, or non peritonealized pericolic or perirectal tissues WITHOUT regional nodal metastasis Foci of tumor found in the pericolic or perirectal fat or in adjacent mesentery (mesocolic fat) away from the leading edge of the tumor and showing no evidence of residual lymph node tissue are classified as N1c If tumor nodules are seen in lesions that would otherwise be classified as T1 or T2, then the primary tumor classification is not changed, but the nodule is recorded as an N1c positive node. Elements of Staging: N2a and N2b N2: Metastasis in four or more regional lymph nodes N2a: Metastasis in 4-6 regional lymph nodes N2b: Metastasis is 7 or more regional lymph nodes Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer N2a is defined as metastasis in 4 to 6 regional lymph nodes. Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer N2b is defined as metastasis in seven or more regional lymph nodes. Compton, C.C., Byrd, D.R., et al., Editors. AJCC CancerStaging Atlas, 2nd Edition. New York: Springer, 2012. ©American Joint Committee on Cancer N2b showing nodal masses in more than 7 regional lymph nodes. Elements of Staging: MX, M0, and M1 MX: No longer exists in TNM Staging M0: No distant metastasis (Remember: not possible for pathologic staging) M1: Distant Metastasis M1a: Metastasis confined to one organ or site M1b: Metastasis in more than one organ/site or the peritoneum Common metastatic sites include liver*, lungs, seeding of other segments of the colon, small intestine, or peritoneum *Involvement of the liver is not considered distant metastasis if tumor has directly extended into the liver from the hepatic flexure or the right side of the transverse colon Stage Groups Prognostic Factors for Colon and Rectum Preoperative or pretreatment carcinoembryonic antigen (CEA) Tumor deposits Circumferential resection margin (CRM) Perineural invasion Microsatellite instability Tumor regression grade (with neoadjuvant therapy) KRAS gene analysis Note: None of these are required for staging. They are however, clinically significant Hints for Colorectal Cancer Involvement of serosal surface is T4a Direct extension to certain organs (such as liver) from certain areas of colon (transverse, flexures, ascending, cecum) is T4b If T4 due to direct extent to abdominal organ & there is discontinuous metastasis there as well, M1a or M1b also applies Tumor that is adherent to other organs or structures grossly is classified T4b. If no tumor is present microscopically in the adhesion, then it is pT1-4a, depending upon depth of wall invasion. Colon Case 1 Answers Topography: C18.5 Histology: 8263/3 This case is one primary per rule M2 Clinical Staging Pathological Staging cT pTis pT 2 cN 0 pN 0 cM 0 pM cM0 Clinical Stage Group 0 Pathologic Stage 1 Group SEER Summary Stage: 1 - Localized Colon Case 2 Answers Topography: C18.4 Histology: 8140/3 This case is one primary per rule M2 Clinical Staging Pathological Staging cT X pT 3 cN X pN 2a cM pM1a pM 1b Clinical Stage Group IVA Pathologic Stage IVB Group SEER Summary Stage: 7 - Distant