Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
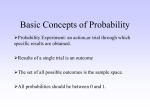
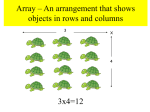
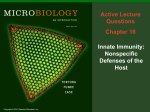
2812 Basic Science Reports Soluble Complement Receptor Type 1 Inhibits the Complement Pathway and Prevents Contractile Failure in the Postischemic Heart Evidence That Complement Activation Is Required for Neutrophil-Mediated Reperfusion Injury Suresh M.L. Shandelya, MD; Periannan Kuppusamy, PhD; Ahvie Herskowitz, MD; Myron L. Weisfeldt, MD; Jay L. Zweier, MD Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Background. Complement-mediated neutrophil activation has been hypothesized to be an important mechanism of reperfusion injury. It has been proposed that soluble complement receptor 1 (sCR1), a potent inhibitor of both classical and alternative complement pathways, may prevent the complementdependent activation of polymorphonuclear leukocytes (PMNs) that occurs within postischemic myocardium and thereby inhibit PMN-derived free radical generation and prevent postischemic contractile failure. Therefore, we performed studies to determine the effects of sCRi on contractile function, PMN adhesion, complement deposition, and PMN-derived free radical generation in the postischemic heart. Methods and Results. Studies were performed in an isolated rat heart model in which the isolated effects of given cellular or humoral factors could be determined. Plasma and PMNs were present to study the effects of sCRi on contractile function, coronary flow, leukocyte adhesion, complement deposition, and PMN-derived free radical generation. Isolated rat hearts were perfused by the method of Langendorff (n=10 in each group) and subjected to 20 minutes of global ischemia and reperfusion with PMNs and plasma in the presence or absence of sCR1. Left ventricular developed pressure (LVDP), coronary flow (CF), left ventricular end-diastolic pressure (LVEDP), and rate-pressure product (RPP) were measured during the preischemic period, during 1-minute control infusion of PMNs and plasma, and on reflow following 20 minutes of global ischemia. During the preischemic control infusion, no significant alterations in the physiologic parameters were observed, and there was no measurable free radical generation. Reperfusion with sCRI markedly improved the recovery of postischemic contractile function. LVDP after 45 minutes of reperfusion was 76+9.8% compared with 32±6.2% (P<.001). In addition, significant improvements in LVEDP, RPP, and CF were observed in hearts treated with sCRi. Additional experiments were also performed to determine the effect of sCRI on complement-mediated PMN activation. Measurements of PMN-derived free radical generation were performed in both isolated PMNs and the coronary effluent of hearts using electron paramagnetic resonance spectroscopy (EPR) with the spin trap 5,5-dimethyl-1-pyrroline-N-oxide (DMPO). EPR measurements in both isolated PMNs and coronary effluent demonstrated that sCRl blocked complement-mediated free radical generation from the PMNs. Increased accumulation of PMNs was observed both in hearts treated with sCRl and in those not treated with sCRl. Immunohistochemical staining of the postischemic myocardial tissue demonstrated marked complement deposition on the endothelial surface of small arterioles and capillaries, which was prevented by sCRI treatment. Thus, sCRI did not prevent PMN adhesion but did prevent complement deposition with activation of the PMN oxidative burst. Conclusions. The potent complement inhibitor sCRl was found to be effective at preventing postischemic myocardial contractile dysfunction and enhancing the recovery of coronary flow. This study demonstrated that complement activation occurs in postischemic myocardium and is necessary for activation of the neutrophil oxidative burst with the generation of reactive oxygen free radicals. The process of neutrophil adhesion, however, was not affected by sCRl and was independent of complement factors. These findings demonstrate the sCRi is a highly potent agent at preventing complement-mediated PMN activation and secondary free radical generation in the postischemic heart. This genetically engineered protein appears to be a promising therapeutic agent in the prevention of myocardial reperfusion injury. (Circulation. 1993;88:2812-2826.) KEY WORDS * free radicals * reperfusion * myocardium * ischemia * complement Shandelya et al Complement Receptor 1 Prevents Postischemic Injury Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 It has been suggested that the activation of the complement pathway within ischemic myocardium can promote the increased recruitment of intracardiac inflammatory cells, which then results in further myocardial injury.1-3 There has been increasing evidence from both animal and clinical studies that complement split products are formed in ischemic myocardium. With the activation of the complement cascade, the split products C3a and C5a are generated, resulting in increased activation of polymorphonuclear leukocytes (PMNs), which then adhere to the vascular endothelium and further occlude the coronary microcirculation, potentially resulting in a no-reflow phenomenon.4-6 Further experiments have demonstrated that the anaphylatoxins C3a and C5a constrict vascular smooth muscle and thereby cause a significant decrease in coronary flow by increasing the arterial vascular resistance.7,8 Longhurst et a19 have shown that intracoronary administration of purified porcine C5a in swine produces reductions in both coronary blood flow and left ventricular function. In addition, several studies have shown that the complement system is an important mediator in acute myocardial ischemia. However, it is not clear whether the complement activation that occurs causes myocardial injury with impaired cardiac contractile function.10-13 Therefore, it has been suggested that activation of the complement system of proteins may be an important mechanism in the pathogenesis of postischemic injury, but questions remain regarding the significance of this complement activation. The activation of the complement system in response to ischemia could result in either direct complementmediated injury or injury secondary to complementmediated neutrophil infiltration and activation with the generation of toxic oxygen free radicals.14-17 We developed an isolated rat heart model in which the effects of isolated cellular or humoral factors on contractile function, coronary flow, cellular adhesion, and free radical generation can be readily studied. In this isolated rat heart model, we performed studies using a recombinant form of complement receptor 1, sCR1, which was genetically engineered to lack both the transmembrane as well as the cytoplasmic domains, resulting in a soluble molecule. This sCR1 has been previously shown to be highly effective at suppressing both the classical and the alternative complement pathways.18 In the present study, we performed the first experiments to determine the efficacy of sCR1 in preventing postischemic contractile dysfunction. Further experiments were performed to determine the effect of sCR1 on PMN adhesion, complement deposition, and free radical generation. These experiments demonstrate that complement activation is required for PMN-mediated reperfusion injury and that sCR1 is highly effective at preventing this injury. It was observed that the process of PMN adhesion was independent of complement, whereas complement was required for activation of the PMN mediated oxidative burst. sCR1 was shown to Received April 16, 1993; revision accepted July 7, 1993. From the Department of Medicine, Division of Cardiology, Electron Paramagnetic Resonance Laboratories, The Johns Hopkins Medical Institutions, Francis Scott Key Medical Center, Baltimore, Md. Correspondence to Dr Jay L. Zweier, Division of Cardiology, Asthma and Allergy Center, 5501 Hopkins Bayview Circle, Johns Hopkins Medical Institutions, Baltimore, Md 21224. 2813 effectively block complement-mediated PMN free radical generation. Methods Isolated Heart Perfusion Female Sprague-Dawley rats (weight, 250 to 400 g) were heparinized and anesthetized with intraperitoneal pentobarbital. The hearts were excised, the ascending aorta was cannulated, and retrograde perfusion was initiated. The hearts were then perfused with Krebs bicarbonate perfusate (17 mmol/L glucose, 120 mmol/L sodium chloride, 25 mmol/L sodium bicarbonate, 2.5 mmol/L calcium chloride, 0.5 mmol/L EDTA, 5.9 mmol/L potassium chloride, and 1.2 mmol/L magnesium chloride) at 37°C with a constant pressure of 80 mm Hg. The perfusate was bubbled with 2 /min of 95% 02-5% CO2 gas. A sidearm in the perfusion line allowed infusion of leukocytes and plasma directly into the heart (Fig 1, top). To measure contractile function, a latex balloon was inserted through an opening in the left atrium across the mitral valve into the left ventricular cavity and connected to a pressure transducer as described previously.14 The balloon was initially inflated with a volume of distilled water sufficient to produce an end-diastolic pressure in the range of 8 to 14 mm Hg. Subsequent measurements of developed pressures were calculated as the difference between the peak systolic and end-diastolic pressure. Left ventricular pressure was recorded with a Gould RS3400 fourchannel recorder. Coronary flow and heart rates were measured periodically every 5 minutes before ischemia and after 20 minutes of global ischemia for 45 minutes of reperfusion. Leukocyte (PMN) Preparation Human neutrophils were prepared by the method of Kensler and Trush,19 which yields PMNs with a purity of >95%. Freshly sampled blood (50 mL) was drawn from volunteer donors in heparinized 10-mL vacutainers and centrifuged at 500g in a Beckman TJ-6 for 10 minutes. The plasma and buffy coat were aspirated, leaving the red cell layer. The cells were then mixed with an equal volume of 6% dextran (1 g 500 K, 5 g 80 K, and 100 mL 0.9% normal saline), with the tubes rinsed thoroughly to secure all the cells. The mixture was then transferred to 30-mL plastic syringes that were inverted and incubated at 37°C for 1 hour until a clear separation was obtained. Next, the upper layer was ejected through a 16-gauge needle with a 90' bend into 50-mL plastic centrifuge tubes and spun for 10 minutes at 500g. The supernatant was discarded, and the pellet was resuspended in ice-cold ACK lysing buffer (0.155 mol/L NH4Cl, 0.01 mol/L KHCO3, and 0.1 mmol/L EDTA at pH 7.4) and respun for 10 minutes at 500g. Finally, the pellet was washed, resuspended in Dulbecco's phosphate-buffered saline plus 1% glucose, and spun for 5 minutes at 340g. A small volume of the cells resuspended in Dulbecco's phosphate-buffered saline was counted using a hemocytometer. Rat Plasma Rat blood was obtained by performing a closed-chest intracardiac puncture with a 10-mL heparinized syringe and immediately centrifuging it at 500g for 15 minutes; Circulation Vol 88, No 6 December 1993 2814 _ 95 % 02 5% CO, 1 INFUSION: PMNa +Ra (Rat A Hmw PMNa +Pm (Rat & Hur) +sgm Gould RS3400 Chart Recorder 80 mm Hg Constant Pressure F ___1 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 FIG 1. Top, Diagram of the isolated heart preparation used. Bottom, Diagram of the experimental protocol. EXPERIMENTAL PROTOCOL WSEONPERIOD PREMTIhC PrOD T 10.15 N srUBILIZAMON , 1 MSN PREWosQ r 10.1SMEN r 30SEC IRON* POST NHONA 1NMMON r 20MIN SCUENA BERE ISHMA *INFLSIONW7TH& W7TTHOVfSCR) RA SMIN 4oMIN REOW EINFSION U1M TPL4SMA ORI MMUMJASORBEDHUMANPL4SMA & PMMN the plasma was aspirated into and kept on ice. a 50-mL centrifuge tube Preparation of Human Plasma Human plasma was obtained from healthy donors after whole blood was centrifuged for the isolation of neutrophils. The human plasma was treated with homogenized rat heart tissue to absorb any cross-reactive antibodies to rat heart antigens. The rat heart tissue was homogenized in a tissue grinder (Omni 5000) in the presence of 25 mL Dulbecco's phosphate-buffered saline. Subsequently, this tissue was centrifuged in a high-speed centrifuge at 5000g for 30 minutes at 40C. This step was repeated three times until the supernatant was clear. The pellet was then incubated in the presence of 10 mL of human plasma at 40C for 20 minutes. After this incubation, the immunoabsorbed plasma was separated from the heart tissue by centrifugation at 40C. The plasma was then aspirated into a 50-mL centrifuge tube and stored on ice for use, and the homogenized rat heart tissue pellet was discarded. Electron Paramagnetic Resonance Measurements Hearts were isolated and perfused as described above except that no EDTA was included in the perfusate in each of the groups. The experimental protocol remained the same except that the spin trap 5,5 -dimethyl1-pyroline-N-oxide (DMPO) was infused through a second sidearm located at the level of the heart with a final concentration of 40 mmol/L, as described previously.'4 Periodic collections of the effluent were made in 20second aliquots during the control period and also for the first 2, 5, 7.5, and 10 minutes during reperfusion. In addition, experiments were performed to detect the generation of oxygen free radicals from PMNs plus plasma in the presence or absence of zymosan, an activator of the complement cascade.20 Care was taken to keep the DMPO-containing solutions covered to prevent any light-induced degradation. The DMPO purchased from Aldrich was further purified by double distillation. Electron paramagnetic resonance (EPR) spectra were recorded in flat cells at room temperature with a Bruker-IBM ER 300 spectrometer operating at X-band with a TM 110 cavity using a modulation Shandelya et al Complement Receptor 1 Prevents Postischemic Injury frequency of 100 kHz, modulation amplitude of 0.5 G, microwave power of 20 mW, microwave frequency of 9.77 GHz, and acquisitions of 10 1-minute scans. The digitized Bruker spectral data files were transferred to an AST 386 personal computer for analysis. Software capable of isotropic spectral simulation, developed in this laboratory, was used for component analysis of experimental spectra as described previously.21 Spectral simulations consisting of linear combinations of the component signals were performed to match the observed spectra. From the weighted intensities of each component in these simulations, the relative amount of each component signal was determined. The total radical concentration was then determined from the ratio of the double integral of the observed spectra to the known concentration of 2,2,6,6-tetramethylpiperidinoxy (TEMPO) free radical in aqueous solution. Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Immunohistochemistry Immunocytochemical staining was performed on hearts removed from female Sprague-Dawley rats weighing 250 to 400 g that had been perfused in the presence or absence of sCR1. Hearts were quickly removed from the cannula and embedded in OCT compound (Miles Scientific, Naperville), immediately quick-frozen in liquid nitrogen, and stored at -700C until ready for staining. Cryostat sections (6 gm) were placed onto pretreated slides (Histostik, Accurate Chemical, Westbury, NY) and dried in a desiccator at 40C overnight. The tissue sections were warmed to room temperature, fixed at room temperature (alum filtered) for 10 minutes, and then washed twice in Tris-buffered saline, pH 7.6, for 5 minutes. To eliminate endogenous peroxidase activity, the sections were incubated for 30 minutes in a TBS-milk solution (TBS with 0.55 Carnation nonfat dry milk containing 0.5% hydrogen peroxide and 1% normal goat serum). This and all subsequent incubations were performed at room temperature in a humidified chamber. The sections were washed with the TBS-milk solution for 5 minutes and then incubated for 1 hour with CSb-9 antibody (1:200). The sections were washed in TBS and then in TBS-milk solution for 5 minutes each and then incubated for 1 hour with biotinylated goat anti-mouse IgG (Sigma Chemical Co, St Louis, Mo) diluted in TBS-milk solution with 1% normal goat serum. After washing, the sections were incubated for 5 minutes with avidin-peroxidase-diluted TBS-milk solution, washed in TBS-milk solution for 5 minutes followed by TBS for 5 minutes, and then incubated with filtered DAB substrate solution (0.05 mol/L Tris buffer [pH 7.6] containing 0.06% 3,3'diamino-benzidine tetrahydrochloride and 0.003% hydrogen peroxide) for 8 minutes. The sections were rinsed in TBS and then in running tap water followed by a 2-minute immersion in a copper sulfate solution (0.5% copper sulfate in 0.15 NaCI) and again in running tap water for 2 minutes, and counter stained in Mayersmodified hematoxylin (Poly-Scientific, Bay Shore, NY). Following immersion in running tap water for 5 minutes, the sections were dehydrated in a graded ethanol series, cleared in toluene, and mounted using Diatex (American Scientific Products; McGaw Park, Ill).22 2815 Histology After completion of the experiments, hearts were quickly removed from the cannula, and the ventricles were sliced into sections 3 to 5 mm thick. The hearts were immediately immersed and stored in 10% Formalin at 40C. Histologic processing was done by conventional methods. Sections were stained with hematoxylin and eosin. The histologic sections were examined for the extent of polymorphonuclear binding to the vascular endothelium as well as for infiltration into myocardial interstitium. Measurement of Complement Activation Measurement of complement activation by red cell lysis assay was performed to determine if the mixture of human PMNs and rat plasma caused any nonspecific activation of complement. In these assays, 0.4 mL of the PMN-containing buffer and 0.1 mL plasma were added to 0.5 mL packed human blood cells and incubated at 37°C for 30 minutes. The red blood cells were then pelleted by centrifugation at 50g for 5 minutes. Spectrophotometric measurements of hemoglobin in the supernatant solution were then performed. No hemolysis was observed on mixing the PMNs and plasma, which demonstrated that there was no nonspecific complement activation. On addition of the complement activator zymosan (1 mg/mL), however, marked hemolysis was observed. Chemicals Zymosan and other chemicals used were purchased from Sigma Chemical Co. Double-distilled deionized water was used to prepare the perfusate and other solutions. DMPO, 97% pure, was purchased from Aldrich Chemical Co and further purified by double distillation. Recombinant sCR1 was provided by T Cell Sciences, Boston, Mass. Experimental Protocol After a 10- to 15-minute equilibration period, baseline left ventricular developed pressure, left ventricular end-diastolic pressure, and coronary flow were measured (Fig 1, bottom). The hearts were subjected to a 1-minute preischemic control infusion with PMNs and plasma and then were allowed to equilibrate again with Krebs bicarbonate buffer for a period of 10 minutes, during which measurements of coronary flow and developed pressure were noted. Hearts subsequently received a 30-second infusion of PMNs and plasma with or without sCR1 before the onset of the 20-minute period of 37°C global ischemia. At the onset of ischemia, the balloon was deflated. The intraventricular balloon volume was then reinflated with the same volume as previously used to set the baseline end-diastolic pressure immediately after the onset of reflow. At the onset of reperfusion, the hearts were reperfused for the first 5 minutes with PMNs and plasma in the presence or absence of sCR1, after which perfusion was continued with Krebs buffer alone for a total of 45 minutes of reflow, during which time serial measurements of coronary flow and developed pressure were performed every 5 minutes. One or more sidearm ports were placed just above the aortic cannula, allowing administration of cells, plasma, or both (Fig 1, top). To 2816 Circulation Vol 88, No 6 December 1993 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 determine free radical generation, hearts were similarly perfused in each of the groups in the presence of 40 mmol/L DMPO, as described above. Two sets of experiments were performed-one in which rat plasma was used and the other in which immunoabsorbed human plasma was used-to access the efficacy of sCR1 at inhibiting both human complement and rat complement. Therefore, there were four experimental groups, with 10 hearts in each group. Group 1. Hearts were subjected to ischemia and reperfusion in the presence of PMNs and rat plasma, without sCR1. The PMNs were suspended in 5 mL of Dulbecco's phosphate-buffered saline with 0.1% glucose and then infused during a 1-minute preischemic control infusion, a 30-second period prior to ischemia, and then again during the first 5 minutes of reperfusion. The cells and plasma were infused through a sidearm at 1:20 dilution to achieve a final concentration of 300 000 PMNs/mL. Group 2. Hearts were subjected to ischemia and reperfusion in the presence of PMNs and rat plasma, in the presence of sCR1 suspended in plasma. The PMNs and plasma were infused as described for group 1. The final concentration of sCR1 administered to hearts was 10 pug/mL. Group 3. Hearts were subjected to ischemia and reperfusion in the presence of PMNs and immunoabsorbed human plasma, in the absence of sCR1. The PMNs and plasma were infused as described in group 1. Group 4. Hearts were subjected to ischemia and reperfusion in the presence of PMNs and immunoabsorbed human plasma, in the presence of sCR1. PMNs and plasma were infused as described for group 1. The final concentration of sCR1 administered to hearts was 10 gg/mL. Validation of the Model The present model was developed to enable the study of the effect of isolated cellular and humoral factors on myocardial contractile function and cellular injury in the postischemic heart, as described previously.14 In the present study, we sought to determine the efficacy of sCR1 at inhibiting either rat or human complement thereby preventing neutrophil-mediated myocardial reperfusion injury. Human PMNs can be isolated in large numbers, 30 to 60 million, and can be readily purified from other blood elements by procedures that do not result in activation of the cells. In practice, 50 mL blood is required to isolate sufficient cells for one or two experiments. Therefore, human PMNs are used in this model. To similarly isolate this number of PMNs from the rat, complete phlebotomy of 10 animals would be required, and it is difficult to purify the cells to >70% purity. On infusion of rat plasma in rat hearts, no toxicity was seen and no alterations in left ventricular developed pressure occurred. To verify that the human PMNs did not activate rat complement or cause other adverse reactions, all hearts studied were first subjected to control preischemic infusion of both the PMNs and plasma, and it was observed in all hearts studied that after infusion the left ventricular developed pressure and coronary flow were not significantly altered. In contrast, if complement was activated with 1 mg/mL zymosan or PMNs activated with 200 ng/mL TPA, phorbol 12-myristate 13-acetate, marked sustained injury was observed with a >60% decrease in contractile function. To further validate the observations that mixture of the human PMNs and rat plasma did not cause PMN activation, EPR measurements were performed on solutions of PMNs and plasma. When 300000 PMNs/mL were mixed with 5% plasma in phosphate-buffered saline in the presence of 50 mmol/L DMPO, no signal was observed. Repeated measurements with up to 1 million PMNs/mL and up to 50% plasma also showed no significant signal, confirming that the rat plasma did not cause activation of an oxidative burst from the human PMNs. To further confirm that the PMNs did not induce any activation of complement, red cell lysis assays were performed as described above. These assays demonstrated that mixture of human PMNs and rat plasma did not result in any measurable complement activation. If complement was intentionally activated with 1 mg/mL zymosan, however, marked red cell lysis and marked free radical generation were observed. Thus, these validation experiments demonstrated that there was no baseline complement activation, neutrophil activation, or alterations in preischemic function in this rat heart model perfused with human PMNs and rat plasma. To determine if there were any adverse effects of human plasma on rat hearts, pilot studies were performed infusing human plasma into control rat hearts. Even at a 1:20 dilution, human plasma resulted in irreversible asystole. This appeared to be due to crossreactive human antibodies reacting with the rat antigens. We observed that this toxicity could be prevented by immunoabsorption of the human plasma with rat heart homogenate using the procedure described above. To verify that immunoabsorption of human plasma did not deplete the complement proteins, we performed experiments to determine if these complement proteins remained. EPR experiments were conducted with PMNs and immunoabsorbed plasma with 1 mg/mL zymosan added to activate the complement system of proteins. In the presence of zymosan, free radical generation was observed identical to that of native human plasma. In the presence of sCR1 (10 ,ug/mL), suppression of the complement pathway was observed, and free radical generation was abolished. These experiments demonstrated that the process of immunoabsorption of human plasma with rat heart homogenate at 4°C did not inactivate the complement system of proteins. Further validation of this was done with the measurement of complement activation by red cell lysis in the presence of PMNs and plasma. In the presence of zymosan (1 mg/mL), marked hemolysis was observed. To verify that remixing of human PMNs and human plasma did not activate complement or cause other adverse reactions, all hearts studied were first subjected to control preischemic infusion of both the PMNs and human plasma, and it was observed in all hearts studied that after infusion left ventricular developed pressure and coronary flow were not significantly altered. In contrast, if complement was activated with 1 mg/mL of zymosan or PMNs activated with 200 ng/mL TPA, phorbol 12-myristate 13-acetate, marked sustained injury was again observed contractile function. with a >60% decrease in Shandelya et al Complement Receptor 1 Prevents Postischemic Injury 2817 I 0 20 5 10 FIG 2. Plots demonstrating the recovery of left ventricular developed pressure (LVDP). Top, Data obtained using the model with rat plasma. Closed circles, Hearts without soluble complement receptor 1 (sCR1) treatment; open circles, hearts that were treated with sCR1 (10 jig/mL). Bottom, Data obtained using the model with immunoabsorbed human plasma. Closed squares, Hearts infused in the absence of sCR1; open squares, hearts infused with sCR1 (10 ,gg/mL). 15 Time Course ofReperfusion ml I4 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 5 10 15 0 5 20 10 15 Time Course ofReperfusion 20 25 Thus, these validation experiments demonstrated that there was no baseline complement activation, neutrophil activation, or alteration in preischemic function with the use of either rat plasma or immunoabsorbed human plasma in this model. Statistical Analysis Data are presented as the mean±1 SEM. Comparisons between the groups during preischemic control infusion as well as postischemic groups were made by a one-way ANOVA designed for repeated measures. Since multiple comparisons were made, a conventional value of P<.05 was accepted as statistically significant. Results Data Physiologic Experiments were conducted to evaluate the efficacy of sCR1 at preventing the alterations in hemodynamic parameters that occur secondary to complement-mediated neutrophil activation. Two sets of experiments were performed - one in which rat plasma was used and the other in which immunoabsorbed human plasma was used -to assess the efficacy of sCR1 at inhibiting both human complement and rat complement. Left ventricular developed pressure. GROUPS 1 AND 2 (RAT PLAsMA). Preischemic baseline pressures for hearts in the absence or presence of sCR1 were 135±7.2 and 132±8.5 mm Hg, respectively. On reperfusion following 20 minutes of ischemia, the sCR1-treated hearts exhib- 30 45 ited higher recovery of left ventricular developed pressure. By 45 minutes of reflow marked differences were seen with developed pressures of only 43.3 ±9.5 mm Hg for hearts not treated with sCR1 and 97.2±11.9 mm Hg for those hearts treated with sCR1 (Fig 2, top). This corresponds to a final recovery of developed pressure of 31.9±6.2% for hearts not treated with sCR1 and 76±9.8% for sCR1-treated hearts. With the administration of sCR1, a more than twofold increase in left ventricular developed pressure was observed that was highly significantly different with P<.0001. GROUPS 3 AND 4 (HUMAN PLASMA). Preischemic baseline pressures were 118±3.0 mm Hg for the untreated hearts and 123±4.7 mm Hg for the sCR1-treated group. Immediately following reperfusion, the sCR1-treated hearts exhibited higher recovery of left ventricular developed pressure, and by 45 minutes of reflow marked differences were seen with developed pressures of only 53±2 mm Hg for hearts not treated with sCR1 and 121.8±4.8 mm Hg for those hearts treated with sCR1 (Fig 2, bottom). This corresponds to a final recovery of 87.1±15.2% for hearts treated with sCR1 and 36.2±1.4% for untreated hearts. Both groups were significantly different with P<.0001. Thus, in these experiments with either rat plasma or human plasma, similar marked decreases in developed pressures were observed after 45 minutes of reflow. Reperfusion in the presence of sCR1 improved the recovery of left ventric- 2818 Circulation Vol 88, No 6 December 1993 Time Course ofReperfsion Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 FIG 3. Plots showing the recovery of ratepressure product (RPP). Top, Data obtained using the model with rat plasma. Closed circles, Hearts infused in the absence of soluble complement receptor 1 (sCR1); open circles, hearts that were treated with sCR1 (10 jig/mL). Bottom, Data obtained using the model with immunoabsorbed human plasma. Closed squares, Hearts infused in the absence of sCR1; open squares, hearts that were treated with sCR1 (10 jig/mL). I 5 10 15 20 Time Course of Reperfusion ular contractile function with a more than twofold increase in developed pressure. Rate-pressure product. The product of heart rate and left ventricular developed pressure, the rate-pressure product was determined as a measure of cardiac contractile work. GROUPS 1 AND 2 (RAT PLASMA). Preischemic baseline rate-pressure product was 39.4±2.3 min' mm Hg for hearts not treated with sCR1 and 34.0±2.3 min' mm Hg for those hearts treated with sCR1. On reflow following 20 minutes of global ischemia, the hearts treated with sCR1 were observed to have a much higher recovery of rate-pressure product. After 45 minutes of reperfusion, the rate-pressure product for hearts treated with sCR1 was 24.7±3.3 min' mm Hg but only 12.1±3.1 min' mm Hg for those hearts not treated with sCR1 (Fig 3, top). Thus, hearts treated with sCR1 exhibited a 2.5-fold increase in the recovery of ratepressure-product hearts with sCR1 treatment, with recovery of 76±10.3% of basal function while only 30±7.0% recovery was observed in untreated hearts. The two groups were significantly different with a P<.001. GROUPS 3 AND 4 (HUMAN PLAsMA). Experiments were also conducted with immunoabsorbed human plasma in the presence and absence of sCR1. Preischemic baseline rate-pressure product in the absence of sCR1 was 38.0+2.8 min' mm Hg and 32.1+1.9 min' mm Hg in the presence of sCR1. Again, on reflow following 20 minutes of global ischemia, the hearts treated with sCR1 were observed to have a much higher recovery of rate-pressure product. After 45 minutes of reperfusion, the rate-pressure product for hearts treated with sCR1 was 27.2±2.1 min' mm Hg compared with a 14.3±1.4 min' mm Hg in untreated hearts (Fig 3, bottom). The hearts treated with sCR1 demonstrated a more than twofold greater final recovery of rate-pressure product compared with untreated hearts with an 83.8±6.4% recovery versus a 25.0±5.3% recovery in the absence of sCR1. The two groups were significantly different at P<.001. These data demonstrate that sCR1 treatment resulted in much higher recovery of cardiac contractile work in hearts subjected to ischemia and reflow in the presence of PMNs and either rat or human plasma. This confirms that sCR1 has efficacy in blocking both human and rat complement pathways. End-diastolic pressure. GROUPS 1 AND 2 (RAT PLASMA). Preischemic baseline end-diastolic pressure was measured for hearts in the presence and absence of sCR1 Shandelya et al Complement Receptor 1 Prevents Postischemic Injury 00 Time Course ofReperfusion 2819 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 FIG 4. Plots showing the recovery of left ventricular end-diastolic pressure (LVEDP). Top, Data obtained using the model with rat plasma. Closed circles, Hearts infused in the absence of soluble complement receptor 1 (sCR1); open circles, hearts that were treated with sCR1 (10 gg/mL). Bottom, Data obtained using the model with immunoabsorbed human plasma. Closed squares, Hearts infused in the absence of sCR1; open squares, hearts that were treated with sCR1 (10 gg/mL). to Time Course of Reperfusion and was not significantly different with values of 11±1 and 10±1 mm Hg, respectively. After reperfusion, much higher values of left ventricular developed pressure were observed in the untreated hearts. Marked differences were observed as early as the first 5 minutes of reflow and persisted out to 45 minutes of reflow with a final recovery of end-diastolic pressure in hearts treated with sCR1 of 37.2± 9.5 mm Hg compared with a value of 75.8±7.2 mm Hg in untreated hearts (Fig 4, top). These groups were significantly different at P<.001. GROUPS 3 AND 4 (HUMAN PLASMA). Preischemic baseline end-diastolic pressure was again fixed at similar values of approximately 10 mm Hg in both groups. After reperfusion, much higher values of end-diastolic pressure were again observed in hearts not treated with sCR1. Following 20 minutes of global ischemia and 45 minutes of reperfusion, the left ventricular end-diastolic pressure of hearts treated with sCR1 was 21.7±2.3 and 56±2.3 mm Hg for hearts that did not receive sCR1 (Fig 4, bottom). Both groups were significantly different at P<.001. Thus, in hearts subjected to ischemia and reflow in the presence of either rat or human plasma, sCR1 resulted in markedly lowered values of left ventricular end-diastolic pressure after reperfusion. Coronary flow. GROUPS 1 AND 2 (RAT PLASMA). Coronary flow was measured before the onset of global ischemia and was identical in both groups with values of 16+1 mL/min for those hearts that did not receive sCR1 and 17±1 mL/min for the hearts treated with sCR1. Throughout the entire 45 minutes of reperfusion, however, marked differences were seen with higher recovery in the sCR1-treated hearts (Fig 8). The final recovery of coronary flow was 12.8±1.6 mL/min in hearts treated with sCR1 versus 7.5±2.2 mL/min in untreated hearts (Fig 5, top), which corresponds to 73.7±8.6% and 43.7±9.9% recoveries, respectively. The two groups were significantly different at P<.001. GROUPS 3 AND 4 (HUMAN PLASMA). Experiments conducted in the presence of human plasma demonstrated similar cardioprotective effects with baseline coronary flows of 15.3±1.3 mL/min in the absence of sCR1 and 15.5±1 mL/min in the presence of sCR1. Following 45 minutes of reflow, hearts treated with sCR1 had much higher coronary flow, with a recovery of 14.25±1.3 mL/min, a 91.8±4.2% recovery compared with hearts not receiving sCR1, which recovered to 5.13±1.3 mL/ minm a 33.3+7.8% recovery (Fig 5, bottom). Both groups were significantly different at P<.0001. Therefore, it was observed that sCR1 treatment significantly increased the recovery of coronary flow in either model. Polymorphonuclear Leukocyte Adherence Leukocyte adherence was measured by performing a differential count on the perfusate solution entering the 2820 Circulation Vol 88, No 6 December 1993 .t 3 FIG 5. Plots showing the recovery of coronary flow (CF). Top, Data obtained using the model with rat plasma. Closed circles, Hearts infused in the absence of soluble complement receptor 1 (sCR1); open circles, hearts that were treated with sCR1 (10 jig/mL). Bottom, Data obtained using the model with immunoabsorbed human plasma. Closed squares, Hearts infused in the absence of sCR1; open squares, hearts that were treated with sCR1 (10 ug/mL). 0 Time Course ofReperfusion Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 10U .1 5 10 15 0 20 5 10 is 20 25 30 45 Time Course ofReperfision heart cannula and the coronary effluent collected during control infusion prior to ischemia and the first 5 minutes of reflow. Prior to ischemia during control infusion, only approximately 25% to 30% of the PMNs remained adherent with more than 70% of the infused PMNs appearing in the effluent. After ischemia, as reported previously, there was a marked increase in PMN adherence within the heart. Adherence of PMNs were quite similar in all four groups studied, suggesting that the mechanism of neutrophil adherence is largely independent of the complement system of proteins (Table 2). In the model with rat plasma in the absence of sCR1 treatment, 90% of the PMNs remained within the heart, while with sCR1 treatment, 70% of the PMNs remained. In the model with human plasma, in either the presence or absence of sCR1, approximately 70% of the PMNs remained in the heart. Thus, in postischemic hearts treated with sCR1 approximately 70% to 90% of the PMNs infused remain within the heart. These data suggested that the process of PMN adherence was largely independent of complement. Histology Histologic sections were examined from hearts that were treated with and without sCR1. In hearts that received sCR1, the myofibrillar structure of the myocytes as well as the interstitial spaces appeared normal, whereas in hearts that were not treated with sCR1, areas of myocyte necrosis were seen as reported previously in this model.14 In both sCR1-treated and untreated hearts, PMNs were seen adherent to the endothelial surfaces of arterioles and capillaries; however, only in untreated hearts were PMNs noted to have migrated across the endothelium. As noted previously, in the absence of treatment, degranulating PMNs were observed adjacent to cardiac myocytes. Therefore, sections from sCR1treated hearts appeared different from those of untreated hearts with PMNs only observed adherent to the endothelium without endothelial transmigration and myocardial structure appeared normal (Fig 6). Immunohistochemistry Hearts were subjected to the protocol described above in the presence or absence of sCR1. These hearts were stained with monoclonal antibody to the C5b-9 attack complex using a standard immunoperoxidase method. Normal rat heart tissue failed to reveal any staining. Control, nonischemic rat hearts subjected to perfusion with neutrophils and plasma failed to demonstrate any staining. Standard controls using either no primary or no Shandelya et al Complement Receptor 1 Prevents Postischemic Injury 2821 TABLE 1. Final Recovery Physiologic Parameters RPP LVDP Groups: n=10 In each group CF LVEDP, mm Hg 75.8±7.2 37±9.5 56±2.3 % Rec. % Rec. % Rec. min-1 mm Hg mL/min 7.5+2.2 43.7+9.9 30+7.0 12.1+3.1 32±6.2 76+9.8 24.7±3.3 76±10.0 12.8±1.6 73.7+8.6 36.2±1.4 53±2.0 14.3+1.4 25.0+5.3 5.13+1.3 33.3±7.8 121.8±4.8 87.1±15.2 27.2+2.1 83.8±6.4 21.7+2.3 14.3+1.3 91.8+4.2 74.6±11.9X 64.5+8.8 XX 22.7±3.0 66.9±7.0 45.7±5.7 10.8±1.7 71.2±8.8 85.4+10.5 60.6±9.9 22.4±3.2 59.8±9.8 42.7+7.4 12.0±1.7 68.3+8.7 75.8+7.0 63.6±7.2 20.0±1.8 62.8±5.5 46.0±5.9 10.1±0.9 68.0±5.5 LVDP indicates left ventricular developed pressure; RPP, rate-pressure product; LVEDP, left ventricular end-diastolic pressure; and CF, coronary flow. *Experiments conducted with rat plasma. tExperiments conducted with immunoabsorbed human plasma. *Control data with neutrophils only, plasma, or perfusate alone, shown for comparison as previously described.14 No sCR1 (r)* sCR1 (r)* No sCR1 (h)t sCR1 (h)t PMNs onlyt Plasma onlyt Perfusate alone mm Hg 43.3+9.5 97.2+12.0 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 primary and secondary antibodies failed to show any staining. In rat hearts subjected to ischemia and reperfusion, marked positive staining with anti C5b-9 was observed, while no staining with a control isotype-matched irrelevant antibody was observed. The distribution of positive staining was seen throughout both ventricles but did not appear random; rather, discrete patches staining arterioles and microcirculatory capillaries were present. Even within these stained patches, not all capillaries appeared positive. No interstitial or myocyte sarcolemmal staining was present. sCR1-treated rat hearts subjected to ischemia and reperfusion revealed only very faint staining within rare patches of microcirculatory capillaries. No dense staining of capillaries or staining of arterioles, interstitial spaces, or myocyte surfaces was seen (Fig 7). Therefore, in sCR1-treated hearts, there was marked diminution in complement deposition compared with untreated hearts. Measurement of Free Radical Generation It has been suggested that oxygen free radicals are important mediators of the myocardial injury that occurs on postischemic reperfusion23-25 and that PMNs are important sources of this radical generation. To assess if the complement blocker sCR1 could prevent this neutrophil-mediated free radical generation, experiments were performed to determine if sCR1 could prevent complement-mediated activation of the neutrophil oxiTABLE 2. Polymorphonuclear Leukocyte Adherence Postischemic Infusion Groups No sCR1 (r)* sCR1(r)* No sCR1 (h)t sCR1 (h)t PMNs In PMNs PMNs Infused, nxl16 Effluent, nxlO65 Adherent, nxlO6l 26.4+3.5 30.1±2.0 27.3±3.1 28.2±2.8 2.7±0.92 9.1±2.30 23.7±3.4 21.0±3.5 18.9±2.6 19.9±1.8 8.4±-f..41.3 8.3±0.9 PMN indicates polymorphonuclear leukocyte. *Experiments conducted with rat plasma. tExperiments conducted with immunoabsorbed human plasma. dative burst and prevent the generation of reactive oxygen free radicals in vitro. Complement was activated with 1 mg/mL zymosan, a potent activator of the complement pathway, and added to PMNs in the presence or absence of sCR1. The overall kinetics of free radical generation was measured for a 35-minute period by EPR spectroscopy in the presence of the spin-trap DMPO, at a 50 mmol/L concentration. In the presence of zymosan, marked free radical generation was observed with prominent DMPO-OOH and DMPO-OH adducts signals. These signals were totally quenched in the presence of 200 U/mL SOD, demonstrating that the observed signals were derived from superoxide. The intensity of these radical signals peaked after 20 minutes. In the presence of sCR1, however, complete inhibition of free radical generation was observed (Fig 8). Further experiments were performed in the isolated rat heart model to determine if sCR1 also prevented the generation of PMN-derived free radicals in the heart. Hearts were subjected to 20 minutes of global ischemia and reperfused with the presence or absence of sCR1. These hearts were also perfused with 40 mmol/L concentration of the spin-trap DMPO, and the coronary effluent was sampled every 20 seconds for the first 2, 5, 7.5, and, finally, 10 minutes of reflow. We have previously demonstrated in the presence of both PMNs and plasma that the total magnitude of free radical generation is increased with a prolongation in the duration of free radical generation. In isolated hearts treated with sCR1, the magnitude and duration of radical generation were observed to be less than that of hearts reperfused with PMNs and plasma in the absence of the drug. Radical generation in sCR1-treated hearts was similar to that observed in the absence of PMNs and plasma, consisting of a short burst peaking at 30 seconds of reflow with no radical generation observable after 2 minutes of reflow. In the absence of sCR1 treatment, radical generation was prolonged and persisted for more than 10 minutes as reported previously.14 Thus, reperfusion with sCR1 prevented the increased magnitude and duration of free radical generation that occurs in hearts secondary to PMN-mediated free radical generation. This suggests that complement is required for PMN-mediated free radical generation in the postischemic heart (Fig 8). Wid:gf4X,0$-2'&;?KA.tvS<iEQs_jV?:'7d,g-4. Circulation Vol 88, No 6 December 1993 2822 -X, r-: ~>}t4 *,~ i:.7 2: .: .? 1K'?B-.S. ->) jA .e: X- Q y:gf ,fg,:fiR .... s*590 -9 4:' ~ _' , -40. ,&N b ,1 .-,l; sE. St o- - _ rl POW->,j: Psf f?- i V Sb %'0 A i: ;.tSB#-;S .ffd i; AIM10pX _ 1-1 A` .. ::dome Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Discussion There is considerable evidence that myocardial ischemia is associated with the activation of the complement system and that this process promotes further cardiac injury with the enhancement of a series of inflammatory events, including neutrophil chemotaxis and activation.26,27 This cellular inflammatory response with PMN activation has been hypothesized to result in the increased generation of reactive oxygen free radicals28'29 and coronary endothelial dysfunction,30'31 which in turn Shandelya et al Complement Receptor 1 Prevents Postischemic Injury FIG 6. Facing page. A, Photomicrograph showing the histology of postischemic rat myocardium that was subjected to ischemia and reperfusion in the presence of soluble complement receptor 1 (sCR1), 10 gg/mL. Original magnification x100. Note the normal myocardial structure of the myocytes, sinusoids, and the small arterioles. This is in contrast to hearts not treated with sCR1 as shown previously.14 B, Photomicrograph of an intramural artery demonstrating the numerous neutrophils adherent to the endothelium, with no infiltration of neutrophils beyond the endothelial lining of the vessel. 2823 cause further myocardial injury.32-34 In the presence of the nonspecific complement inhibitor cobra venom factor, it has been demonstrated that myocardial injury can be significantly reduced. With the administration of cobra venom factor in primates before ligation of the coronary artery, a reduction in infarct size was observed 24 hours later.3 Therefore, it has been hypothesized that new therapeutic agents with the ability to inhibit and block the complement cascade could be effective in preventing the myocardial damage that occurs after ischemia. One such novel and highly potent inhibitor is a genetically Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 FIG 7. A, 4mmunoperoxidase staining with a monoclonal antibody to C5b-9 of a frozen section of left ventricular myocardium from a soluble complement receptor 1 (sCR1i)treated rat subjected to 20 minutes of ischemia followed by 45 minutes of reperfusion with neutrophils and rat plasma. Only very faint staining of rare capillaries (large arrowhead) can barely be apprecated and most capilares are devoid of any staining (small arrowheads). No staining is seen within a small arteriole as well (arrow). (x 40O.) B, Immunoperoxidase staining with a monoclonal anti- body to C5b-9 of a frozen section of left ventricular myocardium from a rat subjected to 20 minutes ischemia followed by 45 minutes of reperfusion with neutrophl and rat plasma. A representative patch of myocardium with POsitive staining is shown. Note the dense staining within the lumen of a small, branchand arteriole (arrows) ingollwdby4 intso ~5 ~ j$>v; 25t~~( *2s60~ ~ within a microcirculatory capN ~~~~illary (arrowhead). Other * neighboring capillaries appear devoid of staining. No appreciable staining is noted within the myocardial interstitium or on myocyte surfaces. 2824 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 3440 Circulation Vol 88, No 6 December 1993 3465 3490 3515 Magnetic Field (Gauss) FIG 8. Electron paramagnetic resonance spectra of free radical generation by isolated neutrophils in the presence of activated complement. Spin-trapping experiments were performed on 1 0 neutrophils/mL in the presence of 50 mmol/L DMPO. A, Neutrophils+ rat plasma activated in the presence of zymosan 200 ,g/mL. B, PMNs+rat plasma activated in the presence of zymosan (200 Lg/ mL) +soluble complement receptor 1 (sCR1) (10 ,g/mL). C, Neutrophils+ human plasma activated in the presence of zymosan (200 ,ug/mL). D, PMNs+human immunoabsorbed plasma activated in the presence of zymosan (200,g/mL)+sCR1 (10 ,ug/mL). engineered soluble form of complement receptor 1, sCR1. It has been hypothesized that a more specific and potent complement inhibitor such as sCR1 might be an effective therapeutic agent at preventing reperfusion injury in the clinical setting of acute myocardial infarction. We have previously shown that sCR1 inhibits both the classical and the alternative complement pathways and have demonstrated that sCR1 can decrease infarct size in rats.18 It was not known, however, whether a specific complement inhibitor such as sCR1 could enhance the recovery of cardiac contractile function and coronary flow in postischemic myocardium. There are also a number of important unanswered mechanistic questions regarding the effect of complement inhibition on neutrophil adhesion, chemotaxis, and activation as well as the generation of highly reactive oxygen free radicals. An understanding of the effect of complement inhibition with respect to these mechanisms of injury is essential to enable a rational comparison of the potential efficacy of this approach in preventing reperfusion injury compared with that of other new agents such as those directed at scavenging free radicals or preventing neutrophil adhesion. Therefore, we performed the present study in an isolated heart model where these mechanistic and functional questions could be readily addressed. We designed this study to evaluate the specific role of complement activation on neutrophil-mediated contractile dysfunction, neutrophil adhesion and activation, and oxygen free radical generation. The efficacy of sCR1 at preventing contractile dysfunction, alterations in coronary flow, complement deposition, as well as neutrophil adhesion, chemotaxis, and activation with the generation of reactive free radicals was determined. The complement system of proteins includes five regulatory proteins that inhibit the proteolytic enzymes that activate C3 and C5, namely, the C3 and C5 convertases of the alternative and classical pathways. These regulatory components consist of two plasma proteins, factor H35,36 and C4-binding protein (C4bp),37,38 and three membrane proteins complement receptor 1,39-41 decay accelerating factor,42 and membrane cofactor protein.43 This set of proteins have commonly referred to as the regulator of complement activation (RCA) proteins because of their structural and functional similarities. Based on this molecular and functional similarity the RCA family has been regarded as a potential group of proteins that could selectively inhibit complement activation. Homeister et al44 have shown that purposeful heterologous activation of the complement system in rabbit hearts perfused with human plasma generates Bb, C3a, C5a, and C5b-9. Their observation of increased amounts of Bb indicates that the alternative pathway was activated in their rabbit heart model. It has been hypothesized that in ischemic myocardium, either the alternative or classical complement pathway could be activated. Therefore, sCR1, which uniquely blocks both pathways, may have a greater potential for benefit in the prevention of myocardial reperfusion injury than other complement-directed therapeutic agents. sCR1 has a molecular weight of 200 kd consistent with a deletion of 67 residues of the full-length receptor.35 The mechanism of sCR1 inhibition of the complement pathway has been extensively investigated. Fearon et a118 suggested that sCR1 has the greatest potential of the RCA family because it has the specificity for binding C3b and C4b, with distinct sites for both proteins, thereby possessing the capacity for displacement of the catalytic subunits from the C3 or C5 convertases of both the pathways and also activating as cofactor for the degradation of C3b and C4b by factor 1. In the present study, experiments were performed in an isolated rat heart model in the presence of either rat or human complement factors and human PMNs. sCR1 blocks formation of the membrane attack complex C5b-9 in both human plasma and rat plasma by interaction with the C3 and C5 convertase of both complement pathways.16'45 We have demonstrated that sCR1 has marked cardioprotective effects in preventing the neutrophil-mediated reperfusion injury that occurs secondary to the activation of complement. Efficacy was observed against either rat complement or human com- Shandelya et al Complement Receptor 1 Prevents Postischemic Injury Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 plement. Greater than twofold increased coronary flow was observed in the sCR1-treated hearts than in similar untreated hearts. In the hearts treated with sCR1, much lower end-diastolic pressures were observed demonstrating improved diastolic relaxation of the left ventricle, most likely secondary to decreased myocyte calcium loading. sCR1 treatment resulted in a more than twofold reduction in left ventricular end-diastolic pressure. Both postischemic recovery of left ventricular developed pressure and the rate-pressure product were markedly increased in the sCR1-treated hearts compared with untreated controls with a more than twofold increase seen. Thus, sCR1 treatment greatly improved the recovery of both contractile function and coronary flow in postischemic hearts. The recovery in left ventricular developed pressure, rate-pressure product, enddiastolic pressure, and coronary flow observed in the presence of sCR1 was identical to that of hearts subjected to ischemia in the absence of PMNs, plasma, or PMNs and plasma, demonstrating that sCR1 totally prevented complement-mediated and PMN-mediated injury (Table 1). Immunohistochemical staining of the tissue of hearts subjected to ischemia and reperfusion in the presence of PMNs and plasma demonstrated the presence of complement deposition throughout both ventricles with the C5b-9 attack complex localized primarily on the endothelium of the arterioles and capillaries. In normally perfused hearts in the presence of PMNs and plasma or in postischemic hearts in the absence of PMNs and plasma, complement deposition was not seen. In hearts subjected to ischemia and reperfusion in the presence of PMNs and plasma, sCR1 prevented this complement deposition. These studies demonstrate that complement is activated in ischemic myocardium with the deposition of the membrane attack complex on the coronary endothelium and that sCR1 effectively prevents this complement deposition. In postischemic hearts, increased PMN adhesion was noted; however, sCR1 did not prevent this increase. No significant alternations in PMN accumulation or adherence were observed in the presence or absence of sCR1 in measurements of the arterial venous gradient in PMN concentration or the histologic visualization of PMNs adherent to the vascular endothelium. This suggests in this model that PMN adhesion is not complement dependent. The process of PMN adhesion is probably primarily controlled by the expression of PMN and endothelial adhesion molecules. In postischemic myocardium upregulation of adhesion molecule surface expression has been hypothesized to occur, and this process alone may be responsible for the increased PMN adhesion that was observed in the postischemic myocardium. In both in vivo canine and feline models of myocardial ischemia and reperfusion it has been demonstrated that specific antibodies to the CD18 neutrophil adhesion molecule can prevent neutrophil accumulation and decrease infarct size.46 Electron paramagnetic resonance studies were performed that demonstrated that sCR1 could prevent the neutrophil-derived oxidative burst triggered by complement activation. sCR1 totally prevented the generation of superoxide and superoxide-derived free radicals that occurs in neutrophils incubated in the presence of activated complement. In the postischemic hearts, sCR1 2825 prevented the amplification in the magnitude and duration of free radical generation that is observed in the presence of PMNs and plasma. Thus, sCR1 did not prevent PMN adhesion within postischemic myocardium, but it did prevent the complement-dependent process of free radical generation from these adherent PMNs. These data suggest that while the process of PMN adhesion within ischemic myocardium is complement independent, complement is required for PMN activation with the generation of reactive superoxide and superoxide-derived free radicals, which in turn cause tissue injury. In summary, these studies demonstrate that complement-mediated neutrophil activation occurs in the postischemic heart. This process causes marked reperfusion injury with impaired contractile function and decreased coronary flow. Neutrophil adhesion was increased in postischemic myocardium, and this process was observed to be independent of the presence of complement proteins. Activation of the neutrophil oxidative burst, however, was observed to be complement dependent. sCR1 was observed to be a particularly potent inhibitor of this neutrophil-derived complement dependent postischemic injury. It totally prevented the neutrophil-derived alterations in contractile function and coronary flow and prevented neutrophil-derived free radical generation. Thus, sCR1 appears to be a promising therapeutic agent in the prevention of myocardial reperfusion injury. Since it is a recombinant human molecule, which is highly effective in inhibiting human complement, it should be suitable for extension to clinical use in humans. Acknowledgments Supported by National Institutes of Health grants HL17655-18 and HL-383224. J.L.Z. is also supported by an Established Investigator Award from the American Heart Association. We gratefully acknowledge the valuable advice and comments of Dr Douglas Fearon, Johns Hopkins University School of Medicine. We would like to thank Dr Robert L. Engler, University of California San Diego School of Medicine, and Dr Lewis Becker, Johns Hopkins University School of Medicine, for helpful comments and advice. References 1. Maroko PR, Carpenter CD, Chiariello M, Fishbein MC, Radvany P, Knostman JD, Hale SL. Reduction by cobra venom factor of myocardial necrosis after coronary artery occlusion. J Clin Invest. 1987;61:661-670. 2. Rossen RD, Michael LH, Kagiyama A, Savage HE, Hanson G, Reisberg MA, Moake JN, Kim SH, Self D, Weakley S, Giannine E, Entman ML. Mechanism of complement activation following coronary artery occlusion: evidence that myocardial ischemia causes release of constituents of myocardial subcellular origin which complex with human Clq in vivo. Circ Res. 1988;62:572-584. 3. Crawford MH, Grover FL, Kolb WP, McMahan CA, O'Rourke RA, McManus LM, Pinckard RN. Complement and neutrophils activation in the pathogenesis of ischemic myocardial injury. Circulation. 1988;78:1449-1458. 4. Engler RL, Dahlgren MD, Morris D, Petersen M, Schmid Schonbein GW. Role of leukocytes in response to acute myocardial ischemia and reflow in dogs. Am J Physiol. 1984;251:H314-322. 5. Engler RL, Dahlgren MD, Petersen M, Dobbs A, Schmid Schonbein GW. Accumulation of polymorphonuclear leukocytes during 3-hour experimental myocardial ischemia. Am J Physiol. 1986;251:H93-H100. 6. Rossen RD, Swain JL, Michael LH, Weakley S, Giannini E, Entman ML. Selective accumulation of the first component of complement and leukocytes in ischemic canine heart muscle: a 2826 Circulation Vol 88, No 6 December 1993 possible initiator of an extra myocardial mechanism of ischemic injury. Circ Res. 1985;57:119-130. 7. Del Balzo UH, Levi R, Polley MJ. Cardiac dysfunction by purified human C3a anaphylatoxin. Proc Natl Acad Sci U S A. 1985;82: 886-890. 8. Del Balzo U, Sakuma I, Levi R. Cardiac dysfunction caused by human C5a anaphylatoxin: mediation by histamine, adenosine, and cyclooxygenase arachidonate metabolites. J Pharmacol EIxp Ther. 1990;253:171-179. 9. Martin SE, Chenoweth DE, Engler RL, Roth DM, Longhurst JC. C5a decreases regional coronary blood flow and myocardial function in pigs: implications for a granulocyte mechanism. Circ Res. 1988;63:483-491. 10. Imai T, Takase S, Arai M, Fujita T. Serial changes of complement titers in the acute phase of myocardial infarction. Jpn Circ J. 1983;47:289-293. 26. 27. 28. 29. 11. Bennett WR, Yawn DH, Migilore PJ, Young JB, Pratt CM, Raizner AE, Roberts R, Bolli R. Activation of the complement system by recombinant tissue plasminogen activation. J Am Coll 30. Cardiol. 1987;10:627-632. 12. Langlois PF, Gawryl MS. Detection of the terminal complement complex in patient plasma following acute myocardial infarction. 31. Atherosclerosis. 1988;70:95-105. Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 13. Pinckard RN, O'Rourke RA, Crawford MH, Grover FS, McManus LM, Ghidoni JJ, Storrs SB, Olson MS. Complement localization and mediation of ischemic injury in baboon myocardium. J Clin Invest. 1980;66:1050-1056. 14. Shandelya SML, Periannan K, Weisfeldt ML, Zweier JL. Evaluation of the Role of Polymorphonuclear leukocytes on contractile function in myocardial reperfusion injury: evidence for plasmamediated leukocyte activation. Circulation. 1993;87:536-546. 15. Ito BR, Roth DM, Chenweth DE, Engler RL. Mechanisms of complement 5a induced myocardial ischemia: formed blood elements are required: depressed contractile function is secondary to blood flow reduction. Circulation. 1988;78(suppl II):II-484. 16. Zweier JL, Rao SML, Weisfeldt ML. Evidence that leukocyte mediated reperfusion injury is complement dependent. Circulation. 1989;80(suppl II):II-34. 17. Shandelya S, Fearon D, Weisfeldt M, Zweier JL. Soluble complement receptor 1 administered only at the time of reperfusion prevents post-ischemic contractile failure. Circulation. 1991; 84(suppl II):II-83. 18. Weisman HF, Bartow T, Leppo MK, Marsh HC Jr, Carson GR, Concino MF, Boyle MP, Rouz KH, Weisfeldt ML, Fearon DT. Soluble human complement receptor type one: in vivo inhibitor of complement suppressing post-ischemic myocardial inflammation and necrosis. Science. 1990;249:146-151. 19. Kensler TW, Trush MA. Inhibition of phorbol ester-stimulated chemiluminescence in human polymorphonuclear leukocytes by retinoic acid and 5,6-epoxyretinoic acid. Cancer Res. 1981;41: 216-222. 20. Hugle TE, Gerard C, Kawahara M, Scheetz ME, Barton R, Koppel G, Russel S. Isolation of 3 separate anaphylatoxins from complement activated serum. Molecular Cell Biochem. 1981;41:59-66. 21. Kuppusamy P, Zweier JL. Identification and quantitation of free radicals and paramagnetic center from complex multicomponent EPR spectra. Appl Radiation Isotopes. 1993;44:367-372. 22. DeLellis RA. Diagnostic immunohistochemistry. In: DeLellis RA, ed. Basic Techniques ofImmunohistochemistry. New York: Masson; 1981. 23. Zweier JL. Measurement of superoxide-derived free radicals in the reperfused heart. J Biol Chem. 1988;263:1353-1357. 24. Kuppusamy P, Zweier JL. Characterization of free radical generation by xanthine oxidase. J Biol Chem. 1989;264:9880-9884. 25. Zweier JL, Kuppusamy P, Williams R, Rabyburn BK, Smith D, Weisfeldt ML, Flaherty JT. Measurement and characterization of 32. 33. 34. postischemic free radical generation in the isolated perfused heart. J Biol Chem. 1989;264:18890-18895. Entman ML, Michael L, Rossen RD, Dreyer WJ, Anderson DC, Smith CW. Inflammation in the course of early myocardial ischemia. FASEB J. 1991;5:2529-2537. Yasuda M, Takeuchi K, Hiruma M, Hida H, Tahara A, Itagane H, Toda I, Akioka K, Teragaki M, Oku H, Yoshiharu K, Takeda T, Kolb WP, Tamerius JD. The complement system in ischemic heart disease. Circulation. 1990;81:156-163. Zweier JL. Measurement of superoxide-derived free radicals in the reperfused heart: evidence for a free radical mechanism of reperfusion injury. J Biol Chem. 1988;263:1353-1357. Von Andrian UH, Hansell P, Chambers JD, Berger EM, Filho IT, Butcher EC, Arfors K-E. L-Selectin function is required for B2-integrin medicated neutrophils adhesion at physiologic shear rates in-vivo. Am J Physiol. 1992;263:H1-H11. Van Benthuysen KM, McMurtry, Horwitz LD. Reperfusion after acute coronary occlusion in dogs impairs endothelium dependent relaxation to acetylcholine and augments contractile reactivity in vitro. J Clin Invest. 1987;79:265-274. Tsao PS, Akoi N, Lefer DJ, Hjohnson G, Lefer AM. Time course of endothelial dysfunction and myocardial injury during myocardial ischemia and reperfusion in the cat. Circulation. 1990;82: 1402-1412. Lucchesi BR. Modulation of leukocyte-mediated myocardial reperfusion injury. Annu Rev Physiol. 1990;52:561-576. Engler R, Covell JW. Granulocytes cause reperfusion ventricular dysfunction after 15-minute ischemia in the dog. Circ Res. 1987; 61:20-28. Lucchesi BR, Werns SW, Fantone JC. The role of the neutrophil and free radicals in ischemic myocardial injury. J Mol Cell Cardiol. 1989;21:1241-1251. 35. Whaley K, Ruddy S. Modulation of the alternative complement pathways by beta 1 H globulin. J Exp Med. 1976;144:1147-1163. 36. Weiler JM, Daha MR, Austen KF, Fearon DT. Control of the amplification convertase of complement by the plasma protein beta 1H. Proc Natl Acad Sci U S A. 1976;73:3268-3272. 37. Shiraishi S, Stroud RM. Cleavage products of C4b produced by enzymes in human serum. Immunochemistry. 1975;12:935-939. 38. Gigli I, Fujita T, Nussenzweig V. Modulation of the classical pathway C3 convertase by plasma proteins C4 binding proteins and C3b inactivation. Proc Natl Acad Sci U S A. 1979;76:6596-6600. 39. Fearon DT. Regulation of the amplification C3 convertase of human complement by an inhibitory protein isolated from human erythrocyte. Proc Natl Acad Sci U S A. 1979;76:5867-5871. 40. Ross GD, Medof ME. Membrane receptors specific for bound fragments of C3. Adv Immunol. 1985;37:217-267. 41. Iida K, Nussenweig. Complement receptor is an inhibitor of the complement cascade. J Exp Med. 1981;153:1138-1150. 42. Nicholson WA, Burge J, Fearon DT, Weller PF, Austen KF. Isolation of a human erythrocyte membrane glycoprotein with decay accelerating activity for C3 convertase of the complement system. J Immunol. 1982;129:184-189. 43. Seya T, Turner J, Atkinson P. Purification and characterization of a membrane protein (gp45-70) that is a cofactor for cleavage of C3b and C4b. J Exp Med. 1986;163:1424. 44. Homeister JW, Satoh P, Lucchesi BR. Effects of complement activation in the isolated heart: role of the terminal complement components. Circ Res. 1992;71:303-319. 45. Weisman HF, Zweier JL, Leppo MK, Fearon DT, Ip SH, Weisfeldt ML. Reduction of infarct size by human soluble recombinant complement receptor type I (rCR1) in a rat reperfusioninfarct model: evidence for complement mediated injury. Circulation. 1989;80(suppl II):II-401. 46. Ma X-I, Tsao PS, Lefer AM. Antibody to CD-18 exerts endothelial and cardioprotective effects in myocardial ischemia and reperfusion. J Clin Invest. 1991;88:1237-1243. Soluble complement receptor type 1 inhibits the complement pathway and prevents contractile failure in the postischemic heart. Evidence that complement activation is required for neutrophil-mediated reperfusion injury. S M Shandelya, P Kuppusamy, A Herskowitz, M L Weisfeldt and J L Zweier Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Circulation. 1993;88:2812-2826 doi: 10.1161/01.CIR.88.6.2812 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1993 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/88/6/2812 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/