Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
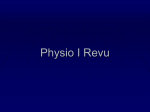
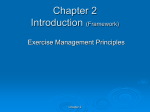
Variations in Maximal Oxygen Intake with Physical Activity in Middle-Aged Men By JoHN R. MCDONOUGH, M.D., FuSAKo KusuMI, B.S., AND ROBERT A. BRUCE, M.D. SUMMARY Data on maximal exercise performance are presented for normal middle-aged men Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 free of cardiovascular disease. Maximal oxygen intake, oxygen pulse, heart rate, and lactate levels all decrease with increasing age. Physical activity defined by habitual running of any amount had a highly significant effect on maximal oxygen consumption. The enhanced effect of physical activity was found equivalent to nearly 10 years of age effect on maximal aerobic capacity. Multivariate analysis revealed significant association between maximal oxygen intake and several coronary risk factors; specifically, physical activity, vital capacity, cigarette smoking, and body weight. Notably lacking in significance were other known risk factors, serum cholesterol, and blood pressure. Data for maximal oxygen intake on healthy men aged 40 to 70 years are presented by age group and physical activity class; and regression equations are provided for estimation of maximal oxygen intake from age, physical activity status, and duration of the multistage treadmill test. These data should prove useful as normal standards for assessment of aerobic capacity in middle-aged men until such time as larger numbers of data on maximal exercise testing become available. Additional Indexing Words: Blood pressure Age Exercise Coronary risk factors Cholesterol Vital capacity uninterrupted submaximal and maximal exercise is utilized.13 The linear relationship between duration of effort and oxygen intake, under these testing conditions, varies in healthy middle-aged men with age and physical status. Accordingly, when these items are known, maximal oxygen intake may be estimated from observed duration of exertion. Methods Oxygen intake (Vo2) was measured during the FUNCTIONAL aerobic capacity (power) which is best defined by measurement of maximal oxygen intake1 varies with body weight, especially lean body mass," 2 physical activity status, and aging.3-'2 Usually measurement of maximal oxygen intake requires two or more tests of maximal exercise to demonstrate an asymptotic relationship between intake and work load.' It is of interest, therefore, to report that maximal oxygen intake can be measured in a single testing procedure, when a multistage treadmill test of last 2 to 4 minutes of treadmill exercise on 86 healthy middle-aged men (84 Caucasians, one Oriental, and one Negro) in the YMCA cohort. Expired air samples were collected at 1-min intervals in evacuated neoprene bags; volumes were measured in a calibrated gasometer and corrected to standard temperature and barometric pressure. Oxygen and carbon dioxide concentrations in aliquots from each bag were measured using micro-Scholander technic. The final minute of gas collection during which maximal exercise tolerance and highest oxygen intake were reached From the Department of Medicine (Cardiology), University of Washington, Seattle, Washington. This study has been supported by Grants-In-Aid HE-09773 from the National Heart and Lung Institute and HS-00092 from the National Center for Health Services. Received November 19, 1969; revision accepted for publication December 29, 1969. Csrculation, Volume XLI, May 1970 Cigarette smoking Weight 743 McDONOUGH ET AL. 744 was used for maximal oxygen consumption (Vo2 max), whereas one to three samples immediately Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 preceding at submaximal work loads defined the approach to the maximal level. Fingertip blood samples, under standardized conditions, were obtained after exercise for measurement of lactate concentration by the method of Strom.'4 Of 225 Seattle YMCA men who were recruited as part of a cohort studied annually since 1962,15-18 150 were retested during 1968. Seven were found with cardiovascular disease, and the remaining 143 were clinically healthy. The 75 men in the cohort not tested during 1968 included 28 who had moved from the area, six who died, 32 who refused the test, and nine for whom testing was contraindicated. Follow-up of health status was successful for all 225 men, and details appear elsewhere.'9 Oxygen intake measurements were obtained on 86 of the 143 healthy men. In the remaining 57, it was not feasible because of technical and scheduling problems. Physical activity levels for this group were assessed by questionnaire which included recreational, occupational, and exercise participation at the YMCA and were defined as follows: (1) sedentary-no evidence of significant exercise from occupational or recreational sources, and nonparticipation in YMCA exercise, (2) lightparticipation in exercise activities such as weightlifting or calisthenics, but no regular running exercises, (3) moderate-habitual runrning exercises (jogging, running, handball, squash, etc.) equivalent to less than 3 miles/week, (4) heavy-habitual running exercises in excess of 3 miles/week. Since all the men included in this study were volunteers, the data obtained will not necessarily be identical to data obtained in a probability sample from the population at large. Only eight of 86 men smoked cigarettes. Results Relationship of Oxygen Intake to Duration of Multistage Exercise The 225 measurements of Vo2 for the 86 healthy men have been plotted for the last 2 to 4 consecutive min of treadmill exercise to define the relationships of oxygen intake to duration of this particular multistage test. Several aspects of the relationship are of interest. First, despite stepwise increases in the work load every 3 min the cardiovascular oxygen transport response is virtually linear during the 6 to 12-min range over which Vo2 was measured (table 1; fig. 1). Second, the relationship is highly precise as seen by the close proximity of the mean values to the regression line, and by the narrow range of Aerobic cost multistage treadmill test healthy men aged 40-69 (mean± 1 s. e.) 50 C Table 1 Relationships of Oxygen Intake to Duration of Multistage Treadmill Test* 40 ^ x 30 - 20 - cm Multistage test, stage (speed, grade) II (2.5 mph, 12%) III (3.4 mph, 14%) IV (4.2 mph, 10%) V t02 Min N 6 7 8 9 10 11 12 13 (mI/kg X min) Mean* SE 6 24.5 0.50 15 43 58 59 33 9 1 27.7 31.5 33.7 37.2 42.2 44.2 47.2 0.45 0.31 0.36 0.46 0.52 0.93 E 00,,z 0 (5.0 mph, 18 %) * Of values observed, rather than from regression equation. 10I °lleV 2 = 4.5+(min x 3.3) 1 2 3 4 5 6 7 8 9 10 11 12 treadmill exercise (min) Figure 1 Aerobic cost of multiple treadmil test of healthy men, aged 40 to 69 years (mean SE). Regression equation to estimate Vo2 from duration of maximally tolerated exertion with this multistage test is: Estimated Vo2max (mi/kg X min) = 3.26 (min) + 6.14. Coefficient of correlation, a, equals +0.85; P < 0.001. Circulation, Volume XLU, May 1970 745 MAXIMAL 02 INTAKE WITH AGE AND ACTIVITY Table 2 Maximal Aerobic Capacity for Normal Middle-Aged Men by Age Group Duration of exercise V02 max (mI/kg X min) Age group (yr) N Mean SD 40-44 45-49 50-54 55-59 60-64 65-69 10 24 20 19 9 3 40.5 38.4 37.5 4.7 5.3 5.3 36.2 32.6 27.7 2 SD SD 31-50 28-49 27-48 10.3 10.2 9.8 1.1 1.1 1.3 8-12 8-12 7-12 5.7 25-48 9.3 1.6 6-12 4.7 4.2 23-42 8.7 7.5 1.6 3.0 5-12 2-10 x 2 SD 19-36 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 coefficient of age and Vo2 max was r = 0.43, and the regression equation for predicting V02 max from age for healthy males is Vo2 max (ml/kg x min) = 55.8-0.41 (years of age) for sedentary men. The corresponding regression equation for physically active men is predicted: Vo2 max = 58.5-0.39 (years of age). From measured maximal heart rate (HR max) and Vo2 max, maximal oxygen pulse (02 pulse max) can be derived from the Fick equation*; this represents the product of maximal stroke volume and peripheral oxygen *Vo = HR x SV x AVo2. VO2maxof healthy men by age group (mean ± 1 s. d.) VO2 MaX The healthy subjects studied spanned an age of 40 to 69 years. Data were sufficient to examine the effect of age on Vo2 max in 5-year age groups from 40-44 through 65-69 years (table 2; fig. 2). Mean Vo2 max decreased linearly from 40.5 ml/kg x min for age group 40-44 years to 36.2 ml/kg x min for age group 55-59 years. This represents a loss of V02 max of approximately 0.3 ml/kg x min for each year of age during the 15 years spanned by the min-intervals of these age groups. Beyond age 60, the decline in V02 max appears to be further accelerated with a mean of 27.7 ml/kg x min seen for the 65-69 year age group, a mean annual decrease from 60 to 69 years of 0.8 ml/kg x min. The correlation Circulation, Volume XLI, May 1970 X Mean the standard errors which were 0.3 to 0.5 ml/ kg x min for most means. Third, when the regression line is extrapolated to zero time, the Vo2 approximates 6 ml/kg x min which is similar to the metabolic rate of men at standing rest. Because energy costs of this test are well defined, Vo2 max can be roughly estimated with reasonable precision if duration of the test is known. The linear response of Vo2 (to the nonlinear stepwise progression of work loads every 3 min used in multistage testing) allows the use of test duration as an estimator of Vo2 max. For healthy men the regression equation was found to be: Vo2 max (ml/kg x min) = 3.26 (min) + 6.14 This equation is not preferred for the estimation of oxygen intake at submaximal work loads. Effect of Age on (min) r W X 40- . '\ 30 CN 20 0 10. -A. 40 a 45 I I 50 55 60 I 65 70 Age (years) Figure 2 Vo2max of healthy men by age group (mean + 1 SD). 746 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 extraction (maximal arteriovenous oxygen difference). From table 3 it can be seen that both HR max and 02 pulse max parallel Vo2 max in showing a downward trend with advancing age. Whether the decrease of 02 pulse max with age represents diminished stroke volume, oxygen extraction, or both, cannot be determined from these data. Others have shown slightly lower stroke volumes and slightly higher arteriovenous oxygen differences in older compared to younger men at equivalent levels of submaximal exercise.20 Physical Activity and Vo, max The groups of sedentary, light, moderate, and heavy physical exercise individuals previously described were analyzed for a series of variables including age, body size, pulmonary function, blood chemistry, and response to exercise; and the data appear in table 4. The only variables showing significant associations were: age, with moderate and heavy groups being somewhat older; resting heart rate, with moderate and heavy groups averaging 8 to 9 beats/min slower; and test duration, Vo2 max and 02 pulse max all showing higher values in moderate and heavy as contrasted with sedentary and light physical activity groups. To assess the joint effect of age and physical activity on these variables, 5-year ages were combined to form three 10-year groups, and sedentary was combined with light, while moderate and heavy physical activity groups were combined. Since this division into two activity classes separates the runners from the nonrunners, this appears to be a reasonable cut-point for a 3 by 2 table analysis. Data on various parameters of oxygen transport appear in tables 5 and 6. Large and highly significant differences in Vo2 max and 02 pulse max are seen at every age when contrasting sedentary with physically active groups. HR max was significantly lower (P < 0.001.) for active men aged 40 to 49, but differences were not significant between sedentary and active men at the older ages. Lactate levels immediately following exercise did not differ significantly between groups, except for the anticipated fall in both active and sedentary men with advancing age. The McDONOUGH ET AL. magnitude of the differences in Vo2 max and 02 pulse max can be seen from the age trends. Although age trends are parallel, the heavy activity group consisting of runners has approximately a 10-year advantage in Vo2 and a 20-year advantage in 02 pulse max over the light activity group composed of nonrunners of similar ages. Multivariate Analysis Stepwise multiple regression analysis was done using Vo2 max as a dependent variable and the factors listed in table 4 as independent variables. Test duration was found to have the highest individual correlation with V02 max (r =0.85), while inclusion of the other variables raised the multiple regression coefficient to r = 0.88. Because of its overwhelming influence on the other variables, test duration was removed and the analysis repeated. The multiple r was 0.80 for 18 variables, of which the first six provided a multiple r of 0.73. In decreasing order of their influence on Vo2 max these variables were lactate level, physical activity, age, vital capacity, cigarette smoking, and body weight (table 7).. It should be noted that both age and smoking were inversely related, with negative rather than positive coefficients. Thus younger nonsmokers had higher V02 max values than older smokers. Discussion Maximal oxygen intake has recently been proposed as a standard for cardiovascular fitness.21 Its importance is based on the fact that it defines in otherwise healthy and motivated subjects maximal performance for cardiovascular transport capacity in terms of the maximal cardiac output and maximal whole body arteriovenous oxygen difference (which encompasses maximal distribution of blood flow to working muscle and maximal oxygen extraction).22 Since approximately 85% of arterial oxygen content is extracted during maximal exercise, and since oxygen extraction is nearly complete in blood delivered to strenuously exercising muscle, the rate limiting factor in Vo2 max is the cardiac output.23 Aging diminishes Vo2 max by decreasing Circulation, Volume XLI, May 1970 MAXIMAL 02 INTAKE WITH AGE AND ACTIVITY 7477 Table 3 Maximal Heart Rate and Oxygen Pulse for Normal Middle-Aged Men by Age Group HR max (beat/min) Age group (yr) N Mean SD 40-44 45-49 50-54 55-59 60-64 65-69 10 24 20 19 9 3 184 178 171 175 165 150 9.6 12.2 9.3 12.6 14.9 6.8 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 maximal cardiac output, and this effect seems to be partly due to a decreased maximal heart rate.24' 25 Measurement of '02 max has been shown to be a precise, reliable, and useful method for assessing impairment in functional capacity or reserve resulting from cardiac disease.1' 13 Irrespective of the lesion (outflow obstruction, regurgitant flow, impaired myocardial contractility, decreased ventricular distensibility, etc.), the common denominator for all lesions producing cardiac impairment is reduced maximal forward cardiac output.26' 27 In the absence of changes in maximal A-Vo2 difference, this impairment is readily quantified by measurement of Vo2 max during the multistage maximal treadmill test.2"2 To assess cardiovascular performance in terms of fitness or its complement, impair- Xi4 2 SD 165-203 154-202 152-190 150-200 135-195 136-164 02 pulse max (ml 02/kg X min X beat) Mean SD 2 SD 0.22 0.22 0.21 0.20 0.20 0.18 0.02 0.03 0.04 0.03 0.02 0.02 0.18-0.26 0.16-0.28 0.13-0.29 0.14-0.26 0.16-0.24 0.14-0.22 groups exceeded their sedentary comparison groups of similar age. Thus, if one knows the age and whether a subject habitually engages in running exercises, and if the subjects are then tested to maximal using duration of the multistage treadmill test or by measuring V02 on any test of maximal capacity, individual performance can be compared to normal men of the same age and activity status by referring to the data in tables 2 and 5. By using the data or the regression equation which appears at the bottom of these tables a predicted Vo2 max can be determined for a given subject. Using this value as a denominator, and the measured (or estimated from test duration) Vo2 max as a numerator, individual performance can be derived as a percentage of average normal capacity, as follows: - Observed Vo2 max x 100. % Average normal V02 max - Pred ed Vo2 maxf Predicted V02 max for age ment, two major influences on Vo2 max, namely, age and habitual physical activity level, should be considered. In the present study a simple classification was found to discriminate adequately. This was whether the individual engaged routinely in running, either as jogging, or in sports activity such as tennis, handball, squash, etc. The fact that the individual engaged in running appeared more important as a discriminator than the amount of running. This is shown in the analysis of Vo2 max levels comparing men who ran less than 3 miles/week with those who ran more than that amount. Both groups were found to have similar levels of Vo2 max, and both Csrculation, Volume XLI, May 1970 This expression relates individual performance to a normative standard for the appropriate peer group. When oxygen intake is not measured, a reasonable estimate may be derived from the duration of maximal exercise with this multistage exercise test. Examples of this derivation are shown in table 8. The results of the multivariate analysis were of interest in identifying the noncardiovascular variables which bear a relationship to (o2 max in order of importance and after removing the correlation between independent variables by covariance analysis. The important variables aside from serum lactate, which is known to reflect the intensity of exercise, are McDONOUGH ET AL. 748 cq ad 01 tt>z . v v 18Nst I 0 . Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Go . . b t~~~~~~~~~~0 w It 0 - 2 X0. O 0 to -. ee . 't* m b1 M . Dio ; r s< X: D S 00 00 00 t-1 Caoo _0 CZ 't mC t- t O .SO <N -. r-. sa' zt N ; r4 r4 '4 '4 ci C ttbs X C sC CQ£iC r- b sce q N O O £1O °D~~~~~~~~~~t st O O O~~~r-. _ O O O _ _ st +' . . . ,,1° ° ~~~~~~~~O -) ; to .0 r-- .0o-- M . Xt V V V N t ss m m I' co* O. t-Cs0 00 X -4 °O c OCes) r-- LO 6 -:o U~~~~~~~~~~~ flc 44,:S wo Ei 4 , ¢~~~~~~~~~t R - > 00 pRi p E *; E X N 0 OC) 00 t- t- g _, X e X= > E 10 | m,y E W X Cicsato?s fm L,My17 MAXIMAL 02 INTAKE WITH AGE AND ACTIVITY 749 Table 5 Maximal Aerobic Capacity for Normal Middle-Aged Men by Age and Physical Activity* V02 max (ml/kg X min)t Active Sedentary Age group (yr) N Mean SD N Mean SD Mean differencet 40-49 50-59 60-69 15 7 5 36.8 33.1 29.4 5.4 5.8 5.0 19 32 7 40.9 37.6 32.9 4.3 5.1 4.0 4.1 4.5 3.5 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 * Sedentary-nonrunners; active runners (jogging, tennis, handball, basketball, squash, etc. regardless of amount). tRegression equations to estimate Vo2 max from age: V02 max (ml/kg X min) according to physical activity status 58.3-0.39 (age in yr) Active = Sedentary = 55.8-0.41 (age in yr) (active vs. sedentary: P < 0.001). t Significance of the difference between active and sedentary for the entire group is P < 0.001. Table 6 Maximal Heart Rate, Oxygen Pulse, and Lactate for Normal Middle-Aged Men by Age and Physical Activities * 02 pulse max (ml O2'/kg X. min X beat) SD Mean (yr) N HR max (beats/min) SD Mean Sedentary 40-49 50-59 60-69 Active 15 7 5 185 9.3 180 14.3 174 0.20 0.18 0.18 40-49 50-59 60-69 19 32 7 176 11.6 171 7.1 164 11.0 0.23 0.21 0.20 Age group Mean SD 0.03 0.03 0.02 105 100 56 33 58 20 0.02 0.04 0.02 94 91 67 21 20 33 * Contrasts between sedentary and active men for: HR max P < 0.001 for ages for ages 50-54 and 60-69; 02 pulse max P < 0.001; lactate, P NS physical activity, age, vital capacity, cigarette smoking, and body weight. All of these variables (except lactate which has not been studied) have been shown to have a significant association with coronary heart disease incidence in prospective studies.33 Whether Vo2 max is a predictor of coronary disease risk is an intriguing question and remains unanswered, principally because data have not been collected on a large enough population followed for an adequate number of years. Acknowledgment The authors wish to acknowledge with gratitude the assistance of the following persons: Mrs. Gladys Pettet, Research ECG Technician, and Mrs. Myrella Circulation, Volume XLI, May 1970 Lactate (mg/100 ml) 40-49, NS Beyer, Data Processing Technician, Division of Cardiology, University of Washington School of Medicine; Mr. Belvin Doane and Mr. Gaylon Kipp, Staff members, Seattle YMCA; physicians previously connected with the follow-up evaluation of this cohort: Drs. Allen Doan, Albert Most, John Mazzarella, and Tom Homsten; and especially the subjects themselves who so willingly gave of their time and of themselves. References 1. TAYLOR HL, BusiRK E, HENSCHEL A: Maximal oxygen intake as an objective measure of cardio-respiratory performance. J Appl Physiol 8: 73, 1955 2. BusxnIR E, TAYLOR HL: Maximal oxygen intake and its relation to body composition, with McDONOUGH ET AL. 750 Table 7 Maximal Oxygen Intake Stepwise Multiple Regression Analysis* Independent variable Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 r F Coefficient Lactate (mg/lOO ml) Physical activity (sed., It., mod., heavy) Age (yr) Vital capacity (L) Cig. smoking (never, quit, current sm) 0.541 0.605 0.655 0.688 0.715 23.4 6.7 6.3 5.9 3.9 0.56 2.18 -0.12 3.86 -0.94 Body weight (kg) HR max (B/min) Diastolic BP max (mm Hg) Height (cm) Systolic BP max (mm Hg) Serum K (mEq/L) HR rest (B/min) Systolic BP rest (mm Hg) Hct (vol %) Diastolic BP rest (mm Hg) Heart vol (cc) Serum cholesterol (mg/100 ml) FEV1 (L) 0.734 0.747 0.759 0.770 0.778 0.785 0.790 0.794 0.795 0.795 0.796 0.796 0.797 2.6 2.4 2.1 2.1 1.4 1.4 1.0 0.7 0.1 0.1 0.1 0.1 0.1 -0.14 0.06 0.09 -0.25 0.06 -1.66 0.07 -0.04 -0.10 * 3. 4. 5. 6. 7. 8. 0.02 -0.001 0.004 -0.31 When test duration is not included as a variable special reference to chronic physical activity and obesity. J Appl Physiol 11: 72, 1957 RORINSON S: Experimental studies of physical fitness in relation to age. Arbeitsphysiologie 10: 251, 1938 DILL DB, CONSOLAZIO CF: Responses to exercise as related to age and environmental temperature. J Appl Physiol 17: 645, 1962 ANDERSON KL, HERMANSEN L: Aerobic work capacity in middle-aged Norwegian men. J Appl Physiol 20: 432, 1964 AsTRAND I: Aerobic work capacity in men and women with special reference to age. Acta Physiol Scand 49 (suppl. 169): 14, 1960 SALTIN B, AsTRAND PO: Maximal oxygen uptake in athletes. J Appl Physiol 23: 353, 1967 RoBINsON S, HARMON PM: Effects of training and of gelatin upon certain factors which limit muscular work. Amer J Physiol 133: 161, 1941 9. KHEHi CA, DmIL DB, NEUFELD W: Training and its effects on man at rest and at work. Amer J Physiol 136: 148,,1942 10. ROWELL LB: Factors affecting the prediction of the maximal oxygen intake from measurements made during submaximal work. Ph.D. Thesis, University of Minnesota, 1962 11. NAUGHrON V, NAGLE F: Peak oxygen intake during physical fitness program for middleaged men. JAMA 191: 103, 1965 12. SALITIN B, BLOMQvISr G, MITCHELL JH, ET AL: Responses to exercise after bed rest and after 13. 14. 15. 16. 17. training. Circulation 37 (suppl VII): VII-1, 1968 BRUCE RA, KusuMI F: Aerobic costs of multistage treadmill test. Unpublished observations, 1970 STR6M G: The influence of anoxia on lactic and utilization in man after prolonged muscular work. Acta Physiol Scand 17: 440, 1949 DoAN AE, PETERSON DR, BLACKMON JR, ET AL: Myocardial ischemia after maximal exercise in healthy men. Amer Heart J 69: 11, 1965 DOAN AE, PETERSON DR, BLACKMON JR, ET AL: Myocardial ischemia after maximal exercise in healthy men. Amer J Cardiol 17: 9, 1966 BRUCE RA: Comparative prevalence of segmental ST depression after maximal exercise in healthy men in Seattle and Taipei: Physical Activity and the Heart. In Proceedings of a Symposium, Table 8 Example of Clinical Appraisal by Estimated TVO2 Max for a 50-year-old male, weighing 80 kg, when predicted 1702 max = 38 ml/kg X min or 3.04 L/min Observed duration (min) 8.5 10.0 11.5 Estimated Vo2 max ml/kg X min L/min 33.9 38.7 43.6 2.71 3.10 3.79 Estimated Predicted (%) 89 102 124 Circulatioe, Volume XLI, May 1970 MAXIMAL 02 INTAKE WITH AGE AND ACTIVITY Helsinki, Finland, edited by MJ Karvonen, AJ Barry. Springfield, Illinois, Charles C Thomas, Publisher, 1967, p 326 18. MOST MD, HORNSTEN TR, HOFER V, ET AL: Exercise ST changes in healthy men. Arch Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Intern Med (Chicago) 121: 225, 1968 19. MCDONOUGH JR, BRUCE RA: Earlier detection of coronary heart disease: Appraisal of 1125 man years of ECG observation by periodic maximal exercise testing of healthy middle-aged men. Unpublished data 20. BEVEGARD BS, SHEPHERD JT: Regulation of the circulation during exercise in man. Physiol Rev 47: 178, 1967 21. SHFEPHARD RJ, ALLEN C, BENADE AJS, ET AL: The maximum oxygen intake: An international standard of cardiorespiratory fitness. Bull WHO 38: 757, 1968 22. MITCHELL JH, SPROULE BJ, CHAPMAN CB: The physiological meaning of the maximal oxygen intake test. J Clin Invest 37: 538, 1958 23. ASTRAND PO, CUDDY TE, SALTIN B, ET AL: Cardiac output during submaximal work. J Appl Physiol 19: 268, 1964 24. AsTRAND I, ASTRAND PO, RODAHL K: Maximal heart rate during work in older men. J Appl Physiol 14: 562, 1959 Circulation, Volume XLI, May 1970 751 25. HANSEN JS, TABAKIN BS, LEvY AM: Comparative exercise-cardiorespiratory performance of normal men in the third, fourth, and fifth decades of life. Circulation 37: 345, 1968 26. BLACKMON JR, ROWELL LB, KENNEDY JW, ET AL: Physiological significance of maximal oxygen intake in "pure" mitral stenosis. Circulation 36: 497, 1967 27. BRUCE RA: The role of exercise in cardiovascular diagnosis. Extract from Symposia of the International Congress of Cardiology, 1966, pp 448-459 28. BRUCE RA: Evaluation of functional capacity in patients with cardiovascular disease. Geriatrics 12: 317, 1957 29. BRUCE RA, JOHNSON W: Exercise tolerance in pregnant cardiac patients. Clin Obstet Gynec 4: 665, 1961 30. BRUCE RA, BLACKMON JR, JONES JW, ET AL: Exercise testing in adult normal subjects and cardiac patients. Pediatrics 32: 742, 1963 31. BRUCE RA, HORNSTEN TR: Exercise stress testing in evaluation of patients with ischemic heart disease. Progr Cardiovasc Dis 11: 371, 1969 32. BRUCE RA, McDONOUGH JR: Coronary disease and exercise. Texas Med 65: 73, 1969 33. STAMLER J: Lectures on Preventive Cardiology. New York, Grune & Stratton, Inc., 1967 752 AMERICAN HEART ASSOCIATION Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Minuscule Review Symposium on Physiological and Clinical Aspects of Cardiac Rehabilitation. Cagliari, Sardinia, June 1968. Mallatie Cardiovascolari 10: nos. 1 and 2, 1969. A 1968 symposium, sponsored by the Council for Rehabilitation of the International Society of Cardiology and Cagliari University in Sardinia, attempted to review the physiologic, clinical, psychologic, and social aspects of rehabilitation in cardiovascular diseases. This initiative, by distinguished practicing cardiologists and researchers, points up the important integration under way between the discipline of traditional diagnostic and therapeutic medicine, and those of preventive, rehabilitative, and social medicine. The volume contains much information of interest to the physician in practice in readable, short presentations. As in the case of most symposia, their quality is not uniform. Considerable attention is given to stress testing including concepts and information about the freedom from rigid testing constraints now possible by the use of more "equivalent" physiologic stresses relating to maximal work capacity or to target heart rates, the relatively good repeatability of progressive stress tests, a large experience of maximal tests in post-infarction patients, and the advantages of beat-tobeat cardiac monitoring during stress tests. Method and procedure are discussed including telemetry and extended monitoring of heart rate and blood pressure during stress tests and during daily activities. A phenomenon that most have observed, the delayed ischemic response occurring during recovery, is explored and partly explained by findings on indirect estimations of cardiac work during recovery. Evidence is presented that the exercise ECG response in post-infarction patients is predictive of subsequent risk of reinfarction. The characteristics, advantages, and disadvantages of different types and modes of exercise testing are well reviewed. Among the problems discussed are those relating brachial artery pressure measured during work to a tension-time index (cardiac work and myocardial oxygen consumption). Evidence is presented that peripheral blood pressure measurement overestimates the work load of the ventricles during exercise. Exercise studies in hypertensive subjects revealed higher work blood pressures and vascular resistance with normal cardiac output. Exercise studies in coronary patients revealed normal hemodynamic responses when they remained "within the limits of their work capacity." Inappropriate hemodynamic responses to work are described in some cardiac patients. Heart volume during work and its changes as a result of conditioning are discussed, as well as variations of total hemoglobin which are found to relate to age, to physical restriction, and to hypoxia, but not otherwise to the type or severity of chronic cardiopulmonary diseases. Evidence is given of the remarkable pressure load imposed on the heart by static work and its potential danger to the cardiac patient. The response to physical conditioning is found to depend on the initial level of fitness in relation to one's potential, expressed as the expected "normal level" for age. Potential for conditioning is very low at advanced ages. Some of the experience is recounted of formal, ongoing conditioning programs among cardiac patients, in the U. S. and in Europe. HENRY BLACKBURN Circulation, Volume XLI, May 1970 Variations in Maximal Oxygen Intake with Physical Activity in Middle-Aged Men JOHN R. MCDONOUGH, FUSAKO KUSUMI and ROBERT A. BRUCE Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Circulation. 1970;41:743-752 doi: 10.1161/01.CIR.41.5.743 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1970 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/41/5/743 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/