Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
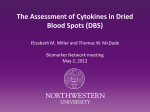
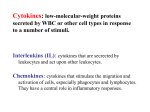
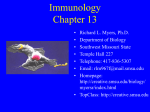
ICANCER RESEARCH 58. 3132-3141. July 15. 1998] Variable Expression of Cytokines in Human Head and Neck Squamous Cell Carcinoma Cell Lines and Consistent Expression in Surgical Specimens1 Rendra V. Woods, Adel El-Naggar, Gary L. dayman, and Elizabeth A. Grimm2 Departments of Tumor Biology IK. V. W., E. A. G.j, Head and Neck Surgery ¡K.V. W., G. L. C.], Pathology [A. E-N.I, and General Surgery [E. A. Gì,University of Texas M. D. Anderson Cancer Center. Houston. Texas 77030 ABSTRACT Head and neck squamous cell carcinomas (HNSCCs) are associated with abnormal cell-mediated immunity at the primary tumor site. We investigated tumor-derived cytokines as factors underlying such abnor malities. Cytokine mRNA and protein of eight HNSCC-derived cell lines were tested,- reverse transcription-PCR results indicated the presence of mRNAs for interleukin la (IL-la) and transforming growth factor a (8 of 8); transforming growth factor ßand IL-lß(7 of 8); and 11-4 and IL-6 (4 of 8). IL-2, IFN-y, and tumor necrosis factor a mRNA were not detected. Supernatants from six of these cell lines were analyzed by ELISA; IL-la, IL-Iß,and IL-6 were found to be markedly increased compared to human papillomavirus-16-immortalized human oral keratinocytes. To determine whether the cell line findings are applicable to primary tumors, we performed immunohistochemical analysis on tumor specimens from 12 patients with invasive HNSCC. Universal intracellular production of IL-la, IL-l/i, and IL-6 protein was detected. We conclude that the aberrant elaboration of biologically active IL-1 and IL-6 may contribute lines from primary and metastatic sites; and (b) to establish whether the IL-1 and IL-6 found in HNSCC cell lines were also present in primary tumors. MATERIALS AND METHODS Cell Lines and Culture Conditions All cell lines used in this study are shown in Table 1. Squamous carcinoma cell lines were grown in 1:1 DMEM-F12 culture medium containing 10% PCS and penicillin/streptomycin. Normal oral keratinocytes obtained by surgical resection and HOK 16B cells were cultured in keratinocyte growth medium (containing 0.15 mM calcium; Clonetics, San Diego, CA). Cells were incubated in 5% CO, in air at 37°C.Stock cultures were grown to 85% confluency and were subcultured with disruption of adherence by a 0.05% trypsin, 0.5% EDTA solution. MDA Tu 686, MDA 686LN, MDA Tu 1186, MDA Tu 1483, and MDA Tu 1586 (16) were kindly provided by Dr. Peter Sacks (Memorial Sloan-Kettering Hospital, New York, NY); MDA Tu-138 and MDA Tu 177 to altered immune status in HNSCC patients. INTRODUCTION HNSCC3 will afflict approximately microenviroment of primary invasive HNSCC. The specific aims were 2-fold: (a) to determine whether IL-la, IL-Iß,IL-2, IL-4, IL-6, IFN-y, TGF-a, TGF-ß,and/or TNF-a were expressed by HNSCC cell 67,000 people in the United States this year (1). Despite advances in diagnosis and management, survival rates for patients with head and neck cancer have remained relatively unchanged for the past 30 years (2). Patients with HNSCC manifest significant immunosuppression that is often more profound than that in patients with other malignancies (3). Immunosuppression in HNSCC has been postulated to occur in a hierarchical manner, where the primary tumor region is the most affected site, followed by draining lymph nodes (4). The level of immunosuppression in patients who have HNSCC varies widely. Known etiological risk factors that may contribute to this phenomenon include tobacco, alcohol (reviewed in Ref. 5), and HPV infection (6). Cytokines are soluble, low molecular weight, multifunctional polypeptides that mediate cellular communication and influence many aspects of cellular growth, differentiation, and function (7). These fundamental biological responses are dysregulated in cancer, as immunoreactive cytokine expression has been reported in a variety of solid tumor systems, including melanoma, ovarian carcinoma, inva sive breast cancer, colorectal cancer, soft-tissue sarcomas, and SCC (8-15). The purpose of this investigation was to assess the cytokines in the (17) cells, as well as cultured normal oral keratinocytes, were provided by Dr. Gary dayman (University of Texas M. D. Anderson Cancer Center, Houston. TX); UMSCC-1 (18) cells were provided by Dr. Thomas Carey (University of Michigan, Ann Arbor, MI); and HOK 16B. a human oral keratinocyte cell line (19), was provided by by Dr. N-H. Park (University of California at Los Angeles, Los Angeles, CA). Human Subjects Twelve patients with untreated invasive HNSCC of the oral cavity and oropharynx who presented to the Department of Head and Neck Surgery at the University of Texas M. D. Anderson Cancer Center between 1982 and 1985 were included in this study. Patient samples were provided for research after Institutional Review Board approval for use of incidental samples. Archival tissue specimens were acquired from the Department of Pathology. Medical records of each patient were reviewed for demographic and clinicopathological information (Table 2). One patient was a former smoker, and 11 were current smokers: 1 had no history of alcohol consumption, 2 were self-defined social drinkers, and 8 were self-defined heavy drinkers (no data were provided regarding alcohol consumption for one patient). Extraction of RNA Tissue-cultured cells were trypsinized and washed once in PBS, and then 3-6 X IO6 cells were pelleted by centrifugation at 7000 rpm in a microcen trifuge. The pellets were frozen at —¿ 70°Cfor no longer than 72 h until RNA Received 6/24/97; accepted 5/18/98. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 This study was supported by National Cancer Institute. NIH Grants ROI CA45225 could be extracted. TRIREAGENT (Molecular Research Center, Inc., Cincin nati. OH), a commercially available reagent, was used to extract total RNA from the cell pellets according to the manufacturer's instructions. Briefly, and ROÕ CA64906 (to E. A. G.) and CA16672 (to the University of Texas M. D. Anderson Cancer Center) and through the generosity of a fellowship from Drs. G. L. dayman and Helmuth Goepfert in the Department of Head and Neck Surgery at the University of Texas M. D. Anderson Cancer Center (to K. V. W.). 2 To whom requests for reprints should be addressed, at the Department of Tumor lowed by precipitation of RNA with isopropanol. The RNA was then washed with 75% ethanol and subsequently solubilized in diethyl pyrocarbonatetreated water. The RNA was finally resuspended in 24 ^1 of diethyl pyrocarbonate-treated water and frozen at —¿ 70°C. Biology, Box 79. University of Texas M. D. Anderson Cancer Center. 1515 Holcombe Boulevard, Houston, Texas 77030. ' The abbreviations used are: HNSCC. head and neck squamous cell carcinoma; SCC. PCR Primers squamous cell carcinoma; HPV. human papillomavirus; IL, interleukin; TGF. transform ing growth factor; TNF. tumor necrosis factor; DMEM-F12. DMEM-Ham's F-12; G3PDH. glyceraldehyde-3-phosphate dehydrogenase; RT-PCR. reverse transcriptionPCR; NF. nuclear factor. Oligonucleotide primers for amplification of the cytokines were purchased from Clontech Laboratories (Palo Alto, CA). Each of these Oligonucleotide primer pairs was constructed to span an intron to distinguish cDNA transcribed homogenization of the cells occurred by phenol-chloroform extraction, 3132 Downloaded from cancerres.aacrjournals.org on June 16, 2017. © 1998 American Association for Cancer Research. fol VARIABLE CYTOKINE EXPRESSION IN HUMAN HNSCC RT-PCR Table l HNSCC cell lines After mRNA was extracted from the cell lines, the protocol for gene amplification was accomplished in four steps: (a) reverse transcription of mRNA; (b) establishment of proper experimental controls (optimizing the amplification cycling to simultaneously detect each of the nine cytokines involved varying the concentration of Mg2+, reaction buffer, and oligonucleo nudemiceYesYes"Not originFloor of lineUMSCC-1MDATu Cell mouthLower of welldifferentiatedWell 138MDATu 177M 686MDA DA Tu 686LNMDATu lipLarynxBase differentiatedModerately testedYesYesYesYesYesin differentiatedPoorly tongueMetastasis of differentiatedPoorly baseof from differentiatedModerately tongueSupraglottic larynxRetromolar differentiatedWell 1186MDA differentiatedWell 1483MDATu Tu trigoneLarynxGradeModerately differentiatedTumorigenicin 1586a TumorigenicSite severe combined immunodeficient mice. Table 2 Characteristics Age Sex (male:female) Race (African American:Caucasian) Anatomical site of primary tumor Oral tongue Base of tongue Floor of mouth Palate Histológica! grade of primary tumor Moderately differentiated Well differentiated Metastatic to neck at diagnosis (yes:no) TNM stage T2N2bM0 tide primers); (c) amplification of the template with a portion of the G3PDH gene to verify mRNA integrity; and (d) amplification of cell line cDNA for cytokine expression. A reaction without any cDNA template and one in which mRNA without reverse transcriptase were included as a negative controls. Positive-control cDNAs corresponding to each cytokine (Clontech, Palo Alto, CA) were amplified to confirm primer specificity. Amplification of mRNA with primers to G3PDH and pAW109 (IL-la) RNA (supplied in the RNA PCR kit by Perkin-Elmer Corp., Foster City, CA) also served as positive controls for each experiment. RT-PCR was used according to a published protocol by Brenner et al. (20). Briefly, total RNA was subjected to RT-PCR using a Perkin-Elmer RT-PCR RNA Amplification kit. Six of p.1 total cellular RNA were added to 34 /¿Ireverse transcription buffer containing 2.5 /mini of random hexamers, 1 mmol/liter dNTPs (dATP, dCTP, dGTP, and dTTP), 2.5 units of MuLV reverse transcriptase (Perkin-Elmer), and 40 units of RNase inhibitor. After initial incubation at 22°Cfor 10 min, followed by 45 min at 42°Cand 9 min at 98°Cin a Perkin-Elmer 9600 thermocycler, a 4.6-^.1 sample of study population 40-74 yr (median. 58.4 yr) 7:5 2:10 3 5 3 1 was suspended in 24.4 jil of PCR buffer containing l /J.Meach primer, 10 HIM Tris-HCl (pH 8.3), 50 mM KC1, 1.5 ITIMMgCU, dNTPs at a final concentration of 200 ßM each, and Taq polymerase at 0.8 units//xl. After an initial denaluration at 94°Cfor 5 min, 35 cycles of amplification (denaturation at 94°Cfor 15 s, annealing at 60°Cfor 12 s, and extension at 72°Cfor 90 s) were followed by a terminal extension at 72°Cfor 7 min. Amplification was performed in the 9 3 6:6 1 4 Perkin-Elmer 9600 thermocycler. The high sensitivity of PCR requires rigorous adherence to anticontamination precautions in the preparation of reagents and reactions. Positive displace ment pipettes (Rainin. Wobum. MA) were used for all pipetting procedures. Prior to the addition of template DNA, the PCR mixture was placed on a transilluminator and irradiated with UV light for 10 min to denature any contaminating double-stranded DNA. Reaction preparation and amplification T4N,M0 from mRNA and DNA templates. Although these primers bind to both DNA and RNA sites, the sizes of the bands differ. Our bands correspond to the expected sizes of products amplified from transcribed mRNA not the larger DNA (see Table 3). All oligonucleotide primers were tested, aliquoted. and stored frozen at —¿20°C according to the manufacturer's instructions. The were performed in separate rooms. All experiments were performed in dupli cate using both positive and negative controls as detailed above. Manipulation, analysis, and storage of amplified products was isolated in a separate labora tory using different equipment than that used in reagent preparation and amplification. primers are shown in Table 3. Amplification primers used as internal controls to ensure the presence of intact human cellular RNA were designed to amplify an approximately 213-bp fragment of the G3PDH gene, a gene that is present Analysis of Amplified DNA in every human nucleated cell. through 4% agarose gels (3% NuSieve agarose; 1% SeaKem agarose; FMC Fifteen ^.1 of each PCR-amplified product was separated by electrophoresis Table 3 PCR primers G3PDH gene primers Positive-strand primer sense, 5'-ACGGATTTGGTCGTATTGGG-3' Negative-strand primer antisense 5'-TGATTTTGGAGGGATCTCGC-3' Predicted size of G3PDH PCR products, 213 bp Cytokine primers Positive-strand primer IL-la, 5'-ATGGCCAAAGTTCCAGACATGTTTG-3' IL-10, 5'-ATGGCAGAAGTACCTAAGCTCGC-3' IL-2. 5'-ATGTACAGGATGCAACTCCTGTCTT-3' IL-4, 5'-ATGGGTCTCACCTCCCAACTGCT-3' IL-6. 5'-ATGAACTCCTTCTCCACAAGCGC-3' IFN--V,5'-ATGAAATATACAAGTTATATCTTGGCTTT-3' TGF-a. 5'-ATGGTCCCCTCGGCTGGACAG-3' TGF-ß,5'-GCCCTGGACACCAACTATTGCT- 3' TNF-a, 5'-ATGAGCACTGAAAGCATGATCCGG- 3' Negative-strand primer 5'-GTTTTCCAGTATCTGAAAGTCAGT-3 ' S'-ACACAAATTGCATGGTGAAGTCAGTT- 3' 5'-GTCAGTGTTGAGATGATGCTTTGAC-3 ' 5'-CGAACACTTTGAATATTTCTCTCTCAT-3' 5'-GAAGAGCCCTCAGGCTGGACTG-3' 5'-GATGCTCTTCGACCTCGAAACAGCAT- 3' 5'-GGCCTGCTTCTTCTGGCTGGCA- 3' 5'-AGGCTCCAAATGTAGGGGCAGG-3 ' 5'-GCAATGATCCCAAAGTAGACCTGCCC-3 ' Predicted size of cytokine PCR products (bp) IL-la, 808 IL-Iß,802 IL-2, 458 IL-4, 456 IL-6, 628 IFN-y. 494 TGF-a, 297 TGF-ß,161 TNF-a, 695 3133 Downloaded from cancerres.aacrjournals.org on June 16, 2017. © 1998 American Association for Cancer Research. VARIABLE CYTOKINE EXPRESSION IN HUMAN HNSCC cell number. The supernatants were aliquoted and frozen at —¿ 70°C.On the day 2 "o è "2 "e CO. Q of the assay, the frozen supernatants were allowed to thaw at room tempera ture, subjected to a pulse spin in a microcentrifuge, and then immediately assayed in triplicate for IL-la, IL-Iß.and IL-6 according to the manufactur er's instructions. Briefly, the supernatants were incubated in the cytokine- O lìs2èIÃŒ333ÃŒg|ÉÌ specific antibody-coated well of the supplied microtiter plate. A second distinct anticytokine antibody conjugated to alkaline phosphatase was added to each well. This was followed by the addition of the chromogenic substance paranitrophenyl phosphate. After 30 min, a reversible inhibitor of acetylcholines- 603 terase activity was added as a stop solution, and the absorbance at 450 nm (reference filter 570 nm) was immediately determined by spectrophotometry (ELISA reader, Dynatech, Chantilly, VA). The concentration of the cytokine was determined from a standard curve. The sensitivity of the specific ELISAs was as follows: IL-la, <2 pg/ml; IL-1/3. <1 pg/ml; and IL-6. <4 pg/ml. Immunohistochemistry Fig. 1. Establishment ot' optimal conditions for cytokine mRNA amplification by RT-PCR. Simultaneous PCR amplification of control cDNAs corresponding to each cylokine was performed. Fifteen fil of PCR product were loaded onto a 4% agarose gel and resolved by electrophoresis. The DNA was visualized by staining with ethidium bromide. Controls: second lane. Perkin-Elmer DNA kit positive control (A template) amplified with kit primers: lliirtl lane, water instead of nucleic acid template amplified with G3PDH primers: fourth lane. Perkin-Elmer RNA PCR kit control amplified with kit primers (DM 151 and DM 152) after reverse transcription; fifth Itine. Perkin-Elmer RNA PCR kit control without reverse Iranscriptase amplified with kit primers (DM 151 and DM 152). X O 2 e cc Antibodies. The following manufacturer-supplied monoclonal mouse antihuman antibodies were used in dilutions for all studies: anti-IL-la (IgGl K; Oncogene Science, Uniondale. NY). anti-IL-lß (IgGl; Genzyme, Cambridge, 603 ee 603 bp~ Fig. 2. Analysis of cytokine mRNA detection in cultured normal oral keratinocytes for constitutive cytokine expression. Cells were incubated in serum-free medium for 16 h prior to RNA extraction. Reverse transcription was followed by simultaneous amplifica tion of cytokine cDNA. Fifteen /il of PCR product were loaded onto a 4% agarose gel and resolved by electrophoresis. The DNA was visualized by staining with ethidium bromide. —¿ Control, cultured normal oral keratinocyte mRNA amplified with G3PDH without reverse transcriptase. Fig. 3. Analysis of cytokine mRNA detection in MDA Tu 177 by RT-PCR for constitutive cylokine expression. Cell lines were incubated in serum-free medium tor 16 h prior to RNA extraction. Reverse transcription was followed by simultaneous amplifica tion of cytokine cDNA. Fifteen fil of PCR product were loaded onto a 4% agarose gel and resolved by electrophoresis. The DNA was visualized by staining with ethidium bromide. + Control, Perkin-Elmer RNA kit positive control RNA amplified with kit primers (DM 151 and DM 152) after reverse transcription; - Control, autoclaved water in place of nucleic acid template amplified with G3PDH primers. 500 400 Corp., Rockland, ME). The PCR products were made visible by staining with ethidium bromide and exposure to UV light (254 nm) on a transilluminator. The molecular weights of the amplification products were determined by comparison with either Hindi or //udii restriction fragments derived from bacteriophage <f>x174 DNA (United States Biochemical Corp, Cleveland, OH). Measurement - 300 ~5t 5 200 of Secreted Cytokines (ELISAs) 100 Secreted cytokine (IL-la, IL-Iß,and IL-6) concentration was determined by ELISA (AMAC Inc., Westbrook. ME) using the manufacturer's protocol. Cell lines were counted and plated at equal concentrations into culture flasks in DMEM-F12 medium with the addition of 10% PCS and penicillin/strepto HOK16B mycin. Cells were cultured to approximately 75% confluency and then washed three times with HBSS. Serum-free DMEM/F12 or serum-free DMEM/F12 plus a specified concentration of recombinant cytokine (IL-la, IL-Iß,or IL-6) was added as indicated in figure legends, and the cells were further incubated for 72 h. Supernatants were collected, cells were trypsinized and counted, and the total number per flask was recorded to standardize cytokine production for i UMSCC-1 TU 138 6861,N 1186 USI 1586 Fig. 4. Maximum cytokine secretion by HNSCC cell lines. Supernatants were collected following a 72-h incubation in serum-free medium alone. The maximum production of II-la, IL-1 j3, and IL-6 is shown for each of the HNSCC cell lines compared to HOK 16B. All samples were analyzed in triplicate by ELISA, and SDs are shown. •¿. mean was statistically significantly different from the control value (HOK I6B) by Tukey's honestly significant multiple comparison test (P < 0.05) after first determining that differences existed among means by a one-way ANOVA (P < 0.05). 3134 Downloaded from cancerres.aacrjournals.org on June 16, 2017. © 1998 American Association for Cancer Research. VARIABLE CYTOKINF EXPRESSION Table 4 Cytokine gene expression in HNSCC cell lines" Cell line IL- la IL-lß 1L-4 IL-6 TGF-a IN HUMAN HNSCC min, rinsed once in distilled water, placed in PBS for 5 min. and then stained immediately. Staining Procedure. To quench endogenous peroxidases, the slides were immersed in a 3% H2O2 solution in methanol for 15 min at 4°Cand air dried TGF-0 UMSCC-1 MDA Tu 138 MDA Tu 177 MDA Tu 686 MDA 686LN MDA 1186 MDA 1483 MDA 1586 " IL-2, INF-y. and TNF-a mRNAs were not detected in these cell lines. for 4-5 min. The ingredients in an avidin-biotin-peroxidase complex kit (Vectastain. Vector Laboratories. Burlingame, CA) were used to complete the staining procedure previously reported by us (9, 21). (The slides were evalu ated independently by two of the authors (A. E-N. and K. V. W.) for confir mation of positivity.) Statistical Analysis. All data are presented as means ±SD. An ANOVA was performed with Dunnett's ; test whenever two samples were compared. An MA), and anti-IL-6 (IgGl; Genzyme. Cambridge, MA). A mouse monoclonal antibody to cytokeratin (AE1/AE3. Boehringer Mannheim. Indianapolis, IN) was used as a positive control for squamous epithelium. MOPC-21, a purified mouse IgGl K immunoglobulin. and UPC-10, a clarified mouse IgG2 K immunoglobulin (Sigma Chemical Co., St. Louis, MO), were used as nonspe cific IgG-negative controls. Purified Protein. Purified recombinant human IL-la. IL-Iß,and IL-6. generously provided by Immunex Research and Development Corp. (Seattle, WA), were used in antibody preadsorption studies for analysis of nonspecific staining. A 10:1 molar excess of purified recombinant cytokine was incubated with each specific monoclonal antibody for 2 h at 37°C.The antigen/antibody ANOVA appropriate to multisample hypothesis testing was performed with the multiple comparison ANOVA. Statistical significance was defined as P < 0.05. When statistical significance was determined for a multiple com parison, Tukey's honestly significant difference test was performed to ascer tain which samples were different. Statistical analysis was performed using SPSS Statistical Package Version 6.0 for Windows on an IBM personal computer. RESULTS mixtures were centrifuged in a microcentrifuge for 3 min at 10,000 X g and then used in immunohistochemical staining. Tissue Preparation. All immunohistochemistry was performed on formalinfixed, paraffin-embedded specimens. The cell lines were also formalin-fixed and paraffin-embedded as pellets prior to immunohistochemical staining, as reported by Tyler et al. (21 ). Antigen Retrieval. To enhance the immunohistochemical staining, the slides were subjected to antigen retrieval using a dilute lead thiocyanate solution (BioGenex Laboratories. San Ramon. CA) according to the manufac turer's specifications. Following antigen retrieval, the slides were cooled for 15 Establishment of Optimal Conditions for Cytokine mRNA Amplification. Fig. 1 shows the result of optimizing the PCR proto col to coamplify of all nine cytokines in a single PCR experiment. The presence of a sharp single band, at the expected molecular weight for each of the cytokines, supports optimal amplification while maintain ing appropriate controls. Optimization experiments were performed using cDNA-positive controls. Rigorous controls, including two dif ferent sets of positive (amplification of Perkin-Elmer kit control pAW109 and G3PDH) and negative controls (double-autoclaved wa ter substituted for nucleic acid template and mRNA not subjected to UMSCC-1 * 1 A ANTI IL-1a T,*?* **2 : ANTI IL-1a + IL-1a ANTI IL-1a + IL-1B Fig. 5. Immunohistochemical staining of paraffin-cm bedded, formalin-fixed pellet of UMSCC-l with anti-IL-la following preadsorption with purified rIL-la or rIL-lß.A, staining of the positive cytokeratin; B. staining with the negati ve-control mouse myeloma protein UPC-IO; C. staining of tumor cells with anti-IL-la; D, at a molar ratio of 10:1 of antigen (rIL-la) to antibody (anti-IL-la). all of the antibody had been complexed to antigen and was therefore unable to stain the cells; E, specificity of the antibody because anti-IL-la staining is not abrogated by preadsorption with rIL-1/3. 3135 Downloaded from cancerres.aacrjournals.org on June 16, 2017. © 1998 American Association for Cancer Research. VARIABLE CYTOKINE EXPRESSION IN HUMAN HNSCC Fig. 6. Immunohistochemical staining of Tu 138 showing constitutive intracellular production of IL-lor, IL-10. and IL-6. A. anlicytokcralin (positive control); B. UPC-10 (negative control); C, anti-IL-la; D, anti-IL-lß;£,anti-IL-6. reverse transcription) were run simultaneously with each of the nine cytokines (as seen in the control lanes of Fig. 1). Summary of Cytokine mRNA in Cultured Normal Oral Keratinocytes. Fig. 2 shows the amplification of mRNA from cultured normal oral keratinocytes. TGF-a is the only cytokine of the nine expressed from these cells (positive and negative controls are shown in the second and third lanes, respectively). Summary of Cytokine mRNA in HNSCC Cell Lines. Fig. 3 shows the amplification of MDA Tu 177 as a SCC example. This cell line expressed mRNA for IL-la, IL-Iß,TGF-a, and TGF-ß.Positive and negative controls are shown in the second and third lanes, respec tively. The cDNA from each cell line was amplified at least three different times. A summary of all cytokine expression as detected by RT-PCR is compiled in Table 4 from each HNSCC cell line tested. All cell lines expressed IL-la and TGF-a; seven cell lines expressed IL-Ißand TGF-ß;four expressed IL-4 and IL-6. IL-2, IFN--y, and TNF-a mRNA were not detected by any cell line tested. IL-la, IL-Iß, and IL-6 Protein Secretion. ELISAs were per formed to determine the relative levels of secreted IL-la, IL-Iß,and IL-6 present in the supernatants obtained from six HNSCC cell lines during 72 h of incubation in serum-free medium as compared to a Table 5 Summary of cytokine elaboration IL-1/3P" I+ E I P E I+ UMSCC-1MDA ++ + + + ± ++ ++ + + + + ++ 138MDA Tu ++ + + + + ++ 686LNMDA + NT + ± NTIL-6P Tu 1483IL-la ' P. PCR; E. ELISA; 1, ¡mmunohistochemistry;NT. not tested. E + + + + NT HPV-16-immortalized oral keratinocyte cell line. The results of these ELISAs are shown in Fig. 4; MDA Tu 138 is the highest secretor of each cytokine (440.8 pg/ml of IL-la, 384.5 pg/ml of IL-6, and 27.1 pg/ml of IL-Iß).IL-1 o was secreted in the greatest quantity in all cell lines, followed by IL-6, then followed by IL-1 ß.The concentration of cytokines secreted and measured by ELISA were all within the range of the cytokine standards provided in the commercial kits; therefore, no serial dilution of supernatants was necessary. Intracellular IL-la, II,-Iß,and IL-6. The number of cell lines tested for intracellular cytokines was limited to the three that were derived from tumors within the oral cavity, UMSCC-1, MDA TU 138, and MDA 686LN, because their common location might suggest a more homogeneous natural history and because we had available control tissue that did not express these cytokines. Immunohistochem ical staining was chosen to develop a cell-line model that would allow us to test specifically whether the tumor cells themselves, rather than tumor-infiltrating lymphocytes, were the source of the cytokines in vivo. To control for potential nonspecific binding, antigen-adsorption experiments were performed on all antibodies to establish the speci ficity of each antibody. Purified recombinant antigen was incubated in molar excess with each antibody prior to staining paraffin-embedded formalin-fixed cell pellets of the cell lines. Purified recombinant IL-la abolished the staining of tumor cells when preadsorbed to anti-IL-la as demonstrated in Fig. 5 for UMSCC-1 as a representative HNSCC cell line. Antigen preadsorption experiments were also per formed and demonstrate the specificity of monoclonal antibodies anti-IL-lß and anti-IL-6 (data not shown). The paraffin-embedded tissue sections of all three paraffin-embedded cell line sections, UMSCC-1, MDA Tu-138, and MDA 686LN, each stained positively for IL-1 a, IL-1 ß,and IL-6, in contrast to the negative control TBS or 3136 Downloaded from cancerres.aacrjournals.org on June 16, 2017. © 1998 American Association for Cancer Research. VARIABLE CYTOKINE EXPRESSION IN HUMAN HNSCC Fig. 7. Immunohislochemical staining of a primary oral tongue tumor from a patient with negative-control MOPC-21 protein. , UPC-10. The data for MDA Tu 138 as a representative cell line are shown in Fig. 6. Summary of Cytokine Detection in Cell Lines. The combined results of mRNA, intracellular protein, and secreted protein strongly suggest that each HNSCC cell line tested produced IL-1 a, IL-1 ß,and IL-6 (Table 5). Unfortunately, the cell line MDA Tu 1483 lost viability and was no longer available for testing by immunohistochemistry. These experiments demonstrate that cytokines are pro duced by HNSCC cell lines, and not only is cytokine mRNA ex pressed, but also intracellular and secreted protein. IL-la and TGF-a mRNA were expressed in 8 of 8 cell lines, IL-Ißand TGF-ßin 7 of 8, and IL-4 and IL-6 mRNA in 4 of 8. IL-la, IL-Iß,and IL-6 proteins were secreted by 6 of 6 cell lines as detected by ELISA, and IL-1 and IL-6 intracellular proteins were confirmed in 3 of 3 of these cell lines by immunohistochemistry. Intracellular Cytokine Detection in HNSCC Paraffin-embedded Tumor Specimens. One of the concerns of working with cultured HNSCC is the possibility that cytokine expression is an artifact of tissue culture conditions. It was therefore imperative to demonstrate the presence of the cytokines in resected HNSCC. We hypothesized that the same set of cytokines as that found in the cell lines would be detected in human tumor specimens; this hypothesis was tested by immunostaining of paraffin-embedded tissue sections to determine whether intracellular cytokine protein was produced by tumor cells rather than tumor-infiltrating lymphocytes or macrophages. Primary tumor specimens from 12 patients were analyzed for the intracellular production of IL-la, IL-Iß,and IL-6. Fig. 7 shows the immunohistochemical staining of a primary tumor from one repre sentative patient with the negative control MOPC-21. Figs. 8-10 show the results of immunohistochemical analysis of three represent ative patients' primary tumors from the oral tongue, base of tongue, and floor of mouth, respectively, with antibodies to cytokeratin, IL-la, IL-Iß,and IL-6. The results are summarized in Table 6. Our results show universal expression of IL-1 and IL-6 in invasive . compared to the mRNA of normal oral keratinocytes. Only TGF-a was expressed in cultured normal oral keratinocytes. Whereas IL-la and TGF-a mRNAs were expressed in every SCC cell line, and IL-1 ß and TGF-ßmRNAs were expressed by all but one, IL-4 and IL-6 mRNA expression varied among the cell lines (Table 4). Even our control reactions using IL-2 cDNA produced bands that were very faint (Fig. 1). Thus, our inability to detect IL-2 with certainty in these tumors may be due to suboptimal amplification conditions. Therefore, we cannot conclude anything about IL-2 expression from these ex periments. These cell lines were derived from all grades of SCC and divergent anatomical sites of the head and neck region. Despite the fact that malignancies of different sites within the HNSCC may reflect varying carcinogenic insults and may represent unique biological entities, the cytokine profiles among the various cell lines differed only slightly. Our subsequent studies focused on IL-1 and IL-6 for the following reasons. These cytokines are immunopotentiating; they have both been reported to synergize with IL-2. which has shown some thera peutic efficacy in the treatment of HNSCC (22, 23). Additionally, IL-1 and IL-6 protein and mRNA have recently been detected in the mRNA of melanoma cells in our laboratory (9). IL-1 and IL-6 are, therefore, candidate cytokines for investigating this phenomenon in HNSCC. They interact through NF-IL-6 and NF-«B(24, 25). When supernatants from six of our cell lines were analyzed by ELISA, a marked increase in concentration of secreted IL-la and IL-6 was found in comparison to HPV 16-immortalized oral keratinocytes (Fig. 4). HOK 16B cells are not normal but are included in this study because they may provide a snapshot of cells early in the multistep transformation process. Secreted cytokine products are available to interact with cellular receptors; thus, they are able to exert paracrine or autocrine effects. Both IL-la and IL-Ißwere produced and se creted by each cell line and they both bind to the same receptors and exert the same biological effects (reviewed in Ref. 26). Moreover, the presence of secreted protein means that the mRNA transcripts have HNSCC tumors, regardless of the histológica! grades. been translated and processed for secretion. These proteins may be biologically active only if they are secreted in a mature form (26). The DISCUSSION concentrations of cytokines secreted in this study are clearly within a We investigated the elaboration of IL-la, IL-Iß,IL-2, IL-4, IL-6, range expected to have biological activity; these cytokines have been IFN-y, TGF-a, TGF-ß,and TNF-a mRNA in eight cell lines derived shown to exert their effects in the femtomolar range (26). The presence of IL-la, IL-Iß,and IL-6 and their localization to the from invasive head and neck primary tumors or their métastases, 3137 Downloaded from cancerres.aacrjournals.org on June 16, 2017. © 1998 American Association for Cancer Research. VARIABLE CYTOKINE EXPRESSION IN Hl MAN HNSCV Fig. 8. Immunohistochemica! staining of a primary oral tongue tumor from a patient. A. anticytokeratin (positive control): B. anti-IL-la; C, anti-IL-l/3; D. ami-IL-6. ^¿j& . «CT>...* intracellular compartment was confirmed by immunohistochemistry. The finding that IL-1 and IL-6 are present intracellularly in HNSCC tumors does not necessitate their secretion, specify their biological form, or delineate their specific action. The observation of IL-IßmRNA and intracellular IL-Ißwithout significant levels of IL-Ißsecretion is not surprising because cleavage of the intracellular product by IL-Ißcon verting enzyme is necessary for secretion. Whether intracellular cytokines possess autocrine activity is not known. The molecular weight that the active forms have, as well as any potential intracellular regulatory influences these cytokines exert, is also not known. To determine whether our cell line findings were reflective of in vivo tumor expression, immunohistochemistry was performed on bi opsy material. Intracellular production of IL-la, IL-Iß, and IL-6 protein was detected in all patients' SCCs. Previous investigators had noted that IL-1 secretion in tumors correlated with local inflammation and the synthesis of prostaglandins, suggesting that the cytokines were not produced by the tumor itself, but rather by infiltrating lympho cytes or macrophages in in lung adenocarcinomas and gliomas (27, 28). In contrast, our results support tumor cell production of cyto kines. We have found similar production of IL-1 and IL-6 in mela noma (9, 21). It is possible, however, that the staining reflects ILs that have been sequestered rather than elaborated by tumor cells. How ever, the intensity and pattern of intracellular staining support our hypothesis that the tumor cells are more likely to be the actual producers. The phenotypic immunohistochemical features suggest that (in addition to tumor infiltrating lymphocytes or tumor infiltrating macrophages) the tumor cells are, in certain cases, producing these cytokines. Additionally, our study of primary HNSCC tumors reveals two patterns of cytokine staining. One is a distinct staining pattern associated with more well-differentiated squamous cells within the 3138 Downloaded from cancerres.aacrjournals.org on June 16, 2017. © 1998 American Association for Cancer Research. VARIABLE. CYTOKINK F.XPRKSION IN Hl'MAN HNSCC B Fig. 9. Immunohistochcmical staining of a primary base of tongue tumor from a patient. A. anticytokeratin (positive control): if. anti-IL-la; C. anti-IL-lj3: O. anti-IL-6. m fis play a role in invasive bone destruction associated with HNSCC tumors (33). To support this. Ahn et al. (14) identified IL-1 in HNSCC primary tumors in the vicinity of osteoclasts involved in destroying osseous structures adjacent to tumors. The presence of IL-6 mRNA is surprising, because it usually reflects inflammatory stimulation, which would tend to inhibit tumor formation. IL-6 is detected in the skin and peripheral blood mononuclear cells of patients with psoriasis (34). The detection of IL-6 mRNA in HNSCC cell lines may explain the finding by Gallo et al. (35) of high levels of IL-6 in the sera of HNSCC patients and of elevated circulating acute-phase proteins in the serum of patients with HNSCC and (36). IL-6 is known to stimulate acute-phase proteins. Additionally, elevated serum levels of IL-1 and/or IL-6 have been transcriptional level (reviewed in Ref. 32) and may provide the advantage the tumor needs to invade the basement membrane. IL-1 is also respon implicated in the development of cancer cachexia in animal models sible for the prostaglandin-independent bone resorbing activity and may (37, 38) and in human renal cell carcinoma (39), as well as HNSCC. 3139 tumor, and the other is a more diffuse staining pattern that seems to be consistent throughout various differentiation stages within a tumor. The physiological role of IL-1 and IL-6 in mucosa is not well estab lished. IL-1 production by keratinocytes and interdigitating reticulum cells of the skin has been reported (13, 29-31). IL-1 inhibitors are secreted by keratinocytes of the gingiva and from epithelial cells of the submandibular gland (32). IL-1 regulates some of the key enzymes of the extracellular matrix and takes pan in the removal of tissue damaged from infection or trauma. IL-1 also increases the proliferation of fibroblasts that express high-affinity IL-1 receptors with the resultant secretion of neutral proteases, such as collagenase, elastase, stromolysin, and plasminogen activator (32). Up-regulation of these proteases by IL-1 occurs at the Downloaded from cancerres.aacrjournals.org on June 16, 2017. © 1998 American Association for Cancer Research. VARIABLE CYTOKINE EXPRESSION IN HUMAN HNSCC Fig. 10. Immunohistochemical staining of a pri mary floor of mouth tumor from a patient. A, anticytokeratin (positive eontrol); H. anti-IL-la; C, anti-IL-1/3; £>. anti-IL-6. Although we have not tested whether the intracellular IL-6 detected in primary tumors is actually secreted, such release into the serum and subsequent regulation of liver function could explain the presence of the circulating acute-phase proteins. This investigation reports the finding of universal intracellular expres sion of IL-la, IL-Iß,and IL-6 in invasive SCC of the oral cavity. Although the demonstration of intracellular IL-1 and IL-6 protein in Table 6 Cvtokine expression in invasive HNSCC lutmtrs sile°Oral Anatomical la8/81/12/21/1IL- 108/81/12/21/1IL-68/81/12/21/1 tongueBase tongueFloor of mouthPalateILof " Anatomical site delineations in this tahle refer to the actual site of the tissue stained rather than the established site of the primary tumor. invasive HNSCC tumors is a novel finding, the authors duly recognize that the sample size is small. The interaction of one cytokine with another and the regulation of one by another are not assured merely by the presence of two distinct cytokines. Further investigations are necessary to establish the relationship between IL-1 and IL-6 in HNSCC to determine the putative roles these cytokines have in regulating the tumor microenvironment. Whether IL-6 in HNSCC tumors has developed resistance to regulation by other immune mediators, including cytokines, and hence fosters immunosuppression at that site needs to be investigated. In conclusion, our findings support the hypothesis that the aberrant elaboration of biologically active IL-1 and IL-6 may contribute to altered immune status in HNSCC patients. The ectopie production of these cytokines by tumor cells may influence the hierarchical immu nosuppression, seen most profoundly in HNSCC patients at the level block of the primary tumor and decreasing with distance from the primary 3140 Downloaded from cancerres.aacrjournals.org on June 16, 2017. © 1998 American Association for Cancer Research. VARIABLE CYTOKINE EXPRESSION tumor site. However, it is important to qualify our findings because our studies were performed on tumors and cell lines derived from invasive oral SCCs. Future studies should address the functional relationship between these cytokines and the differences in the ex pression and regulation of ILs in advanced carcinomas versus premalignant and in situ carcinomas, to both elucidate the role that cytokines play in tumor invasion and progression and to establish whether an acquisition of altered cytokine regulation occurs. ACKNOWLEDGMENTS We thank Dr. Mitchell Frederick for normal oral keratinocyte mRNA. Dr. Douglas Boyd for advice with the preadsorption assays as well as access to his ELISA reader, Velma Harris for expert assistance with the histology speci mens, and Pat Wolf for statistical analysis. We are grateful to Dr. Demetrios Petropoulos for useful discussions and careful review of the manuscript. REFERENCES 1. Parker, S. L.. Tong. T.. Bolden. S., and Wingo. P. Cancer statistics. CA Cancer J. Clin., 47: 5-27, 1997. 2. Pavelic. Z. P.. Lasmar. M.. Pavelic. L.. Sorensen. C., Slambrook. P. J., Zimmermann. N.. and Gluckman. J. L. Absence of retinoblastoma gene product in human primary oral cavity carcinomas. Eur. J. Cancer B Oral Oncol.. 32B: 347-351, 1996. 3. Schantz. S. P.. and Guillamondegui, O. M. Developing perspective in head and neck tumor immunology. Prob. Gen. Surg.. 5: 99-1II. 1988. 4. Wang. M. B., Lichtenstein, A., and Mickel, R. A. Hierarchical immunosuppression of regional lymph nodes in patients with head and neck squamous cell carcinoma. Otolaryngol. Head Neck Surg.. 705: 517-527, 1991. 5. Schlepper. J. R. Prevention, detection and diagnosis of head and neck cancer. Semin. Oncol. Nursing. 5: 139-149, 1989. 6. Woods, K. V., Shillitoe. E. J.. Spitz, M. R., Schantz. S. P.. and Adler-Storthz. K. Analysis of human papillomavirus DNA in oral squamous cell carcinomas. J. Oral Pathol. Med.. 22: 101-108, 1993. 7. Vilcek, J., and Le. J. Immunology of cytokines: an introduction. In: Angus Thompson (ed.) The Cytokine Handbook, pp. 1-17. London: Academic Press. 1991. 8. Kerbel. R. S. Expression of multi-cytokinc resistance and multi-growth factor inde pendence in advanced stage metastatic cancer: malignant melanoma as a paradigm. Am. J. Pathol., 141: 519-524, 1992. 9. Francis. G. M.. Krohn. E. G.. Woods. K. V.. Buzaid, A. C., and Grimm, E. A. Interleukin-6 production and secretion in human melanoma cell lines: regulation by interleukin-l. Melanoma Res.. 6. 1-11. 1996. 10. Vitólo, D.. Zebe, T., Kanbour. A.. Dahl. C.. Herberman. R. B.. and Whiteside. T. L. Expression of mRNA for cytokines in tumour-infiltrating mononuclear cells in ovarian adenocarcinonma and invasive breast cancer. Int. J. Cancer, 51: 573-580. 1992. 11. Ito, R.. Kitadai. Y.. Kyo. E.. Yokozaki. H.. Yasui. W., Yamashita, U., Nikai. H., and Tahara. E. Interleukin-l o acts as an autocrine growth stimulator for human gastric carcinoma cells. Cancer Res., 53: 4102-4106, 1993. 12. Spellman. J. E.. Gollnick. S. O.. Zhang, P. J.. and Tornasi, T. B. Cytokine production by human soft tissue sarcomas: implications for immunosuppression within the tumour bed. Surg. Oncol.. 5: 237-244, 1996. 13. Partridge, M.. Chantry, D., Turner. M.. and Feldman, M. Production of interleukin-l and interleukin-6 by human keratinocytes and squamous cell carcinoma cell lines. J. Invest. Dermatol.. 96: 771-776. 1991. 14. Ahn. J. M.. Huang. C. C.. and Cho. H. T. Localization of interleukin-l in human squamous carcinomas of the head and neck. Laryngoscope. 103: 529-532. 1993. 15. Letessier. E. M., Sacchi, M.. Johnson, J. T.. Herberman. R. B., and Whiteside. T. L. The absence of lymphoid suppressor cells in tumor-involved lymph nodes of patients with head and neck cancer. Cell Immunol.. 130: 446-458. 1990. 16. Sacks, P. G., Hong. W. K., and Hittelman, W. N. in vitro studies of the premalignant process: initial culture of oral premalignant lesions. Cancer Bull.. 43: 485-489, 1991. 17. Liu. T. J.. Zhang. W-W.. Taylor. D. L., Roth. J. A.. Goepfert, H.. and dayman, G. L. Growth suppression of human head and neck cancer cells by introduction of a wild-type p53 gene via recombinant adenovirus. Cancer Res., 54: 3662-3667. 1994. IN HUMAN HNSCC 18. Krause, C. J.. Carey, T. E., Ott, R. W.. Hurbis. C.. McClatchey. K. D., and Regezi. J. L. Human squamous cell carcinoma: establishment and characterization of new permanent cell lines. Arch. Otolaryngol., 107: 703-710, 1981. 19. Park, N-H., Min. B-M., Li. S-l.. Huang. M. Z., Cherick. H. M.. and Doniger. J. Immortalization of normal human oral keratinocytes with type 16 human papillo mavirus. Carcinogenesis (Lond.l, 12: 1627-1631. 1991. 20. Brenner, C. A.. Tarn. A. W.. Nelson. P. A., Engleman. E. G., Suzuk, i N.. Fry, K. E., and Larrick. J. W. Message amplification phenotyping (MAPPing): a technique to simultaneously measure multiple mRNAs from small numbers of cells. BioTechniques. 7: 1096-1103. 1989. 21. Tyler. D. S.. Francis, G. M., Frederick. M.. Tran, A. H.. Ordonez, N. G.. Smith. J. L., Eton. O.. Ross. M.. and Grimm. E. A. Interleukin-l production in tumor cells of human melanoma surgical specimens. J. Interferon Cytokine Res.. 15: 331-340. 1995. 22. Forni, G.. Cavallo. G. P., Giovarelli, M.. Benetton. G.. Jemma. C.. Barioglio, M. G., de Stefani. A.. Forni. M.. Santoni. A.. Modesti. A.. Cavallo. G.. Menzio, P., and Cortesina. G. Tumor immunotherapy by local injection of intcrleukin 2 and nonréactivelymphocytes. Prog. Exp. Tumor Res.. 32: 187-221. 1988. 23. Mattijssen. V., de Mulder, P. H.. Schomagel, J. H., Verweij. J.. Van den Broek. P.. Galazka, A., Foy, S., and Ruiter. D. J. Clinical and immunopathologica! results of a phase II study of perilymphatically injected recombinant interleukin-2 in locally far advanced, nonpretreated head and neck squamous cell carcinoma. J. Immunother.. 10: 63-68, 1991. 24. Hirano. T. Interleukin-6. In: A. Thompson (ed.) Cytokine Handbook., pp. 169-190. London: Academic Press. 1991. 25. Leung. K.. Betts. J. C., Xu. L.. and Nalse, G. J. The cytoplasmic domain of the interleukin-l receptor is required for nuclear factor-xB signal transduction. J. Biol. Chem.. 269: 1579-1582, 1994. 26. Dinerello. C.A.TheIL-1 family: 10 years of discovery. FASEB J., 8: 131-132, 1994. 27. Roussel. E.. Gingras. M. C.. Grimm. E. A., and Rom. J. A. High expression of adhesion molecules/activation markers with liltle interleukin-2, intcrferon y, and tumor necrosis factor ßgene activation in fresh tumor-infiltrating lymphocytes from lung adenocarcinoma. Cancer Immunol. Immunother.. 41: 1-9. 1995. 28. Roussel. E.. Gingras, M. C.. Grimm. E. A.. Bruner. J. M., and Moser. J. P. Predom inance of type 2 intratumoral response in fresh tumor-infiltrating lymphocytes from human gliomas. Clin. Exp. Immunol.. 105: 344-352. 1996. 29. Hsu. S-M.. and Zhao, X. Localization of interleukin-1 in normal or reactive lymphoid tissues and skin: abundance of IL-1 in inlerdigitating reticulum cells. Lymphokine Res.. 6: 13-18. 1987. 30. Arsenault. T. V.. Sauder. D. N.. Harley, C. B.. and McKenzie. R. C. Identification and characterization of a partial cDNA expressing interleukin-l like activity in keratino cytes. Mol. Immunol.. 29: 431-438. 1992. 31. Schoel. D. C., Johannessen. A. C.. Kristoffersen, T.. and Nilsen. R. Expression of HLA-DR and ICAM-1 on cultured human keratinocytes and their influences on the alloimmune response. J. Dermatol., 22.- 839-844, 1995. 32. Wustrow. T. P. U., and Ising. W. J. Immunological determinants as predictors for prognosis in patients with head and neck cancer. In: J. T. Johnson and M. S. Didolkar (eds.) Head and Neck Cancer. Vol. Ill, pp. 409-430. Amsterdam: Excerpta Medica. 1993. 33. Meghji. S.. Sandy, J. R.. Scutt. A. M.. Harvey, W.. Carter, R. L.. and Harris, M. Macromolecular osteolytic factor synthesized by squamous carcinoma cell lines from the head and neck in vitro is interleukin 1. Br. J. Cancer, 58: 17-21, 1989. 34. Neuner. P., Urbanski, A.. Trautinger. F.. Moller. A.. Kirnbauer. R.. Kapp. A.. Schöpf, E.. Schwarz, T., and Luger, T. Increased IL-6 production in monocytes and kerati nocytes in patients with psoriasis. J. Invest. Dermatol., 97: 27-33, 1991. 35. Gallo, O., Cori, A. M., Attanasio, M., Martini. F., Paola, G.. Storchi. O. F., and Abbate. F. Acute-phase proteins and interleukin-6 serum level in head and neck cancer. Arch. Otolaryngol. Head Neck Surg.. 118: 1366-1367, 1992. 36. dayman. G. L.. Liu, F. J., Savage, H. E., Taylor, D. L., Lavedan. P.. Buschsbaum, R. M., Pellegrino, C., Trujillo. J. M.. Young. G.. and Schantz, S. P. Acute-phase proteins in patients with head and neck cancer treated with interleukin 2/interferon a. Arch. Otolaryngol. Head Neck Surg., 118: 41-48, 1992. 37. Strassman, G., Fong. M., Kenney, J. S., and Jacob. C. O. Evidence for the involvement of interleukin-6 in experimental cancer cachexia. J. Clin. Invest., 89: 1681-1684. 1992. 38. Keller, U. Pathophysiology of cancer cachexia. Support. Care Cancer, /: 290-294, 1993. 39. Dosquet. C., Schaetz, A., Faucher, C., Lepage, E., Wautier. J-L., Richard. F.. and Cabane, J. Tumor necrosis factor-a. interleukin-Iß and interleukin-6 in patients with renal cell carcinoma. Eur. J. Cancer. 30A: 162-167, 1994. 3141 Downloaded from cancerres.aacrjournals.org on June 16, 2017. © 1998 American Association for Cancer Research. Variable Expression of Cytokines in Human Head and Neck Squamous Cell Carcinoma Cell Lines and Consistent Expression in Surgical Specimens Kendra V. Woods, Adel El-Naggar, Gary L. Clayman, et al. Cancer Res 1998;58:3132-3141. Updated version E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cancerres.aacrjournals.org/content/58/14/3132 Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cancerres.aacrjournals.org on June 16, 2017. © 1998 American Association for Cancer Research.