Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
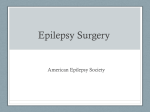
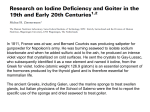
Endocrinology Phase 2a Revision Session Rhys Watkins and David Rutherford 27/3/17 The Peer Teaching Society is not liable for false or misleading information… Glucose Range: 3.5-8 mmol/L under all conditions Liver - Stores Glycogen - Glycogenolysis - Gluconeogenesis from fat, protein, glycogen Taken into cells by GLUT receptors (comes in different varieties based on location) Insulin: GlucoseGlycogen, Glucose into cells, supppresses glycogenolysis and gluconeogenesis The Peer Teaching Society is not liable for false or misleading information… Diabetes Mellitus (Type I) • B-cell destruction in Islet of Langerhans • Aetiology: Autoimmune Acute presentation: Polyuria Polydipsia Weight loss Subacute presentation: Fatigue Polyuria/dipsia Balanitis/candida The Peer Teaching Society is not liable for false or misleading information… DKA Visual change Type II – the metabolic syndrome Central obesity Elevated cholesterol/triglycerides The Peer Teaching Society is not liable for false or misleading information… Raised BP Type II Risk: Obese, advancing age, FH, certain ethnic groups Major Immediate Complication: HHS (Previously HONK) Major Long-term Complications: Kidney, Eye, Foot, Neuropathy Everything The Peer Teaching Society is not liable for false or misleading information… Diagnosis HbA1C >48 (6.5%) -- Consider ‘pre-diabetes’ if 42-47 (6.1-6.4%) Fasting glucose >7 (>6.5 = impaired GT) Oral GTT @2hrs >7.8 (>6.1 = Impaired) The Peer Teaching Society is not liable for false or misleading information… Management Stepwise SULFONYLUREA (caution glibenclamide/cholropropramide in eldery/renal impairment) METFORMIN DPP-4 INHIBITOR PIOGLITAZONE (avoid with biggest CVD risk) Triple Therapy Insulin The Peer Teaching Society is not liable for false or misleading information… Stop this from happening, please The Peer Teaching Society is not liable for false or misleading information… DKA Features: Lethargy, polyuria, dehydration, confusion, coma, abdo pain, Kussmaul breathing Diagnose: Ketone ++, Glucose >11, venous pH <7.3, bicarb <16 First priority: Fluid balance and dehydration. 0.9% saline 500ml bolus then replacement regime, typically 100ml/kg (1L over 1hr, 2hr, 4hr, 6hr) Second: Actrapid 0,1u/kg/hr IV. Avoid SC The Peer Teaching Society is not liable for false or misleading information… Resolution: pH >7.3 Bicarb >18 Ketones <0.3 Ketones poorly discriminative The Peer Teaching Society is not liable for false or misleading information… THYROID DISEASE THYROID ANATOMY Thyroid cartilage Isthmus 4th tracheal ring The Peer Teaching Society is not liable for false or misleading information… THYROID ANATOMY The Peer Teaching Society is not liable for false or misleading information… THYROID HISTOLOGY Colloid (thyroglobulin) Cuboidal epithelial cells Follicle Basement membrane The Peer Teaching Society is not liable for false or misleading information… THYROID PHYSIOLOGY The Peer Teaching Society is not liable for false or misleading information… HYPOTHYROIDISM: CAUSES PRIMARY HYPOTHYROIDISM (↓T4) - Primary atrophic hypothyroidism Hashimoto’s thyroiditis (anti-TSHR, anti-Tg, anti-TPO) Iodine deficiency Post-thyroidectomy / radioiodine / antithyroid drugs Lithium / amiodarone SECONDARY HYPOTHYROIDISM (↓TSH) - Hypopituitarism HYPOTHYROIDISM SYMPTOMS CVS: RS: Hoarse voice GI: Constipation Int: Cold intolerance Endo: Weight gain UG: Menorrhagia MSK: Myalgia, weakness Neuro / Psych: Tired, low mood, dementia SIGNS Bradycardic Reflexes relax slowly Ataxia (cerebellar) Dry, thin hair / skin Yawning / drowsy / coma Cold hands +/- ↓T°C Ascites Round puffy face Defeated demeanour Immobile +/- Ileus CCF HYPOTHYROIDISM ↓T3, ↓T4 = ↑TSH INVESTIGATIONS: (a) TFT (b) Lipids/cholesterol (c) FBC (macrocytosis) HYPOTHYROIDISM: ASSOCIATIONS AUTOIMMUNE Type 1 Diabetes Mellitus Addison’s disease Pernicious anaemia Primary biliary cirrhosis INHERITED Turner’s syndrome Down’s syndrome Cystic fibrosis HYPOTHYROIDISM: TREATMENT • Levothyroxine (T4) – review at 12 weeks, adjust 6 weekly • NB: give smaller doses if elderly as risk of angina or MI The Peer Teaching Society is not liable for false or misleading information… The Peer Teaching Society is not liable for false or misleading information… HYPERTHYROIDISM: CAUSES 1. GRAVES’ DISEASE: - IgG autoantibodies bind to and stimulate TSH receptors (triggers = infection, stress, childbirth) - Eye disease, pretibial myxoedema, thyroid acropachy - Autoimmune (vitiligo, type 1 DM, Addison’s) 2. TOXIC MULTINODULAR GOITRE 3. TOXIC ADENOMA 4. ECTOPIC THYROID TISSUE (mets / struma ovarii) 5. EXOGENOUS (Iodine / T4 excess) 6. DE QUERVAIN’S THYROIDITIS (post-viral) Pretibial Myxoedema Thyroid Acropachy HYPERTHYROIDISM SYMPTOMS CVS: Palpitations RS: GI: Diarrhoea Int: Heat intolerance Endo: ↓Weight, ↑appetite UG: Oligomenorrhoea +/infertility MSK: Neuro / Psych: Tremor, irritability, labile emotions SIGNS HANDS: - Palmar erythema; warm, moist skin; fine tremor PULSE: - Tachycardia; SVT; AF FACE: Thin hair; lid lag / retraction NECK: Goitre; nodules; bruit HYPERTHYROIDISM ↑T3, ↑T4 = ↓TSH INVESTIGATIONS: (a) TFT (b) FBC (normocytic anaemia) (c) ESR (↑) (d) Calcium (↑) (e) LFT (↑) (f) Thyroid autoantibodies (g) Visual fields, acuity, eye movements HYPERTHYROIDISM: TREATMENT (i) β-blockers: - Propanolol (rapid control of symptoms) (ii) Antithyroid medication: - Titration (carbimazole: SE = AGRANULOCYTOSIS) - Block and replace (carbimazole + thyroxine) (iii) Radioiodine (131I) (iv) Thyroidectomy THYROID EYE DISEASE • 25-50% have Graves’ disease • Main risk factor = smoking • Eye and thyroid disease may not correlate SYMPTOMS: Eye discomfort, grittiness, diplopia SIGNS: Exophthalmos, proptosis, ophthalmoplegia TESTS: Clinical diagnosis +/- CT/MRI orbits MANAGEMENT: Conservative measures (stop smoking, sunglasses, Fresnel prism); IV methylprednisolone; Surgical decompression; Eyelid surgery CAUSE OF GOITRE DIFFUSE - Physiological - Graves’ disease - Hashimoto’s thyroiditis - De Quervain’s NODULAR - Multinodular - Adenoma / cyst - Carcinoma THYROID CANCERS 1. Papillary (60%) 2. Follicular (≤25%) 3. Medullary (5%) 4. Lymphoma (5%) 5. Anaplastic EMERGENCIES 1. Myxoedema coma (↓T4) 2. Thyrotoxic storm (↑T4) ADRENAL DISORDERS ADRENAL GLANDS ADRENALS HISTOLOGY CUSHING’S SYNDROME • CHRONIC glucocorticoid excess • LOSS of normal feedback mechanisms • LOSS of circadian rhythm. • Most common cause = IATROGENIC • If due to pituitary adenoma = Cushing’s DISEASE • “Lemon on sticks” appearance The Peer Teaching Society is not liable for false or misleading information… CUSHING’S SYNDROME: CAUSES ACTH DEPENDENENT (↑ACTH) CUSHING’S DISEASE Bilateral adrenal hyperplasia from ACTH-secreting pituitary adenoma ECTOPIC ACTH PRODUCTION Small cell lung Ca and carcinoid tumours ACTH INDEPENDENT (↓ACTH DUE TO NEGATIVE FEEDBACK) ADRENAL ADENOMA / CARCINOMA Abdo pain +/- virilisation in females ADRENAL NODULAR HYPERPLASIA ECTOPIC CRH PRODUCTION IATROGENIC Thyroid medullary and prostate cancers Steroids (common) CUSHING’S SYNDROME SYMPTOMS Int: Acne Endo: ↑ Weight UG: Gonadal dysfunction MSK: Proximal weakness Psych: Mood change SIGNS FAT DISTRIBUTION: - Central obesity - Moon face - Buffalo neck hump - Supraclavicular fat distribution SKIN CHANGES: - Skin and muscle atrophy - Bruises - Purple abdominal striae OTHER: - Osteoporosis - Hypertension, hyperglycaemia - Infection-prone / poor healing BASIC RULES OF ENDOCRINOLOGY: 1. EXCESS hormone – INHIBIT the gland 2. LOW hormone – STIMULATE the gland The Peer Teaching Society is not liable for false or misleading information… The Peer Teaching Society is not liable for false or misleading information… CUSHING’S SYNDROME: INVESTIGATIONS 1. Bloods (↑plasma cortisol) 2. Overnight dexamethasone suppression test - Dexamethasone 1mg PO at 00:00 - Measure serum cortisol at 08:00 - Normal <50nmol/L (no suppression in Cushing’s) 3. 48h dexamethasone suppression test - Dexamethasone given qds for 2 days - Measure cortisol at 0h and 48h - No suppression in Cushing’s LOCALISING THE LESION • If above tests +ve → PLASMA ACTH • ACTH undetectable → ADRENAL TUMOUR → CT ADRENAL GLANDS • ACTH detectable → PITUITARY vs ECTOPIC: - 48h HIGH-DOSE dexamethasone suppression test - CRH TEST (measure cortisol at 120 mins) The Peer Teaching Society is not liable for false or misleading information… CUSHING’S SYNDROME: TREATMENT • Iatrogenic – stop steroids • Cushing’s disease – trans-sphenoidal surgery or bilateral adrenalectomy (caution Nelson’s syndrome) • Adrenal adenoma – adrenalectomy • Adrenal carcinoma – adrenalectomy, RT and adrenolytics (mitotane) • Ectopic ACTH – surgery (if localised) YOU HAVE NO ADRENAL GLANDS ADDISON’S DISEASE The Peer Teaching Society is not liable for false or misleading information… ADDISON’S DISEASE • Primary adrenocortical insufficiency • Destruction of adrenal cortex • ↓Glucocorticoids and ↓Mineralocorticoids The Peer Teaching Society is not liable for false or misleading information… ADDISON’S DISEASE: CAUSES • Autoimmune (80%) – commonest in UK • TB – commonest worldwide • • • • • Adrenal metastases (lung, breast, kidney) Lymphoma Opportunistic infections in HIV (e.g. CMV) Adrenal haemorrhage (e.g. SLE, APS) Congenital adrenal hyperplasia (late-onset) The Peer Teaching Society is not liable for false or misleading information… ADDISON’S DISEASE SYMPTOMS GI: N/V, abdo pain, constipation / diarrhoea Int: Tanned skin Endo: Lean build MSK: Weakness, flu-like arthralgias, myalgias Neuro: Dizzy, faints Psych: Tired, tearful, anorexia, depression, psychosis SIGNS SKIN: - Pigmented palmar creases and buccal mucosa - Vitiligo CVS: - Postural hypotension - Shock (↑BP, ↓HR, coma) BASIC RULES OF ENDOCRINOLOGY: 1. EXCESS hormone – INHIBIT the gland 2. LOW hormone – STIMULATE the gland The Peer Teaching Society is not liable for false or misleading information… The Peer Teaching Society is not liable for false or misleading information… ADDISON’S DISEASE: INVESTIGATIONS 1. Bloods: - FBC (anaemia, eosinophilia) - U&E (↓Na+, ↑K+, ↑Ca2+, ↑Urea) - BM (↓) 2. Short ACTH Stimulation Test: - Measure plasma cortisol before and 30mins after IM Tetracosactide (SynACTHen) - Addison’s excluded if 30min cortisol >550nmol/L 3. 9AM ACTH levels: inappropriately high in Addison’s 4. 21-hydroxylase adrenal autoantibodies ADDISON’S DISEASE: TREATMENT • Replace steroids with 15-25mg Hydrocortisone daily • Replace mineralocorticoids with Fludrocortisone • Drug card and bracelet • DOUBLE dose if febrile illness, injury or stress • IV fluids if dehydrated The Peer Teaching Society is not liable for false or misleading information… SECONDARY ADRENAL INSUFFICIENCY: • Lack of ACTH (and therefore cortisol) • Commonest cause = IATROGENIC • Long-term steroid therapy suppresses HPA axis • Other rare causes include hypothalamo-pituitary disease (no hyperpigmenation as ↓ACTH and mineralocorticoid levels normal) The Peer Teaching Society is not liable for false or misleading information… CONN’S SYNDROME • • • • Excess aldosterone independent of RAAS Solitary aldosterone-producing adenoma ↑ retention of Na+ and water Often asymptomatic. May have signs of ↓K+ • Ix: U&E, renin, aldosterone • Tx: Laparoscopic adrenalectomy. Spironolactone for 4 weeks pre-op to control BP and K+ ACROMEGALY • Excess GH from pituitary tumour (99%) or hyperplasia (e.g. ectopic GHRH carcinoid tumour) • Male : Female = 1:1 • 5% associated with MEN-1 • If before epiphyses fuse – GIGANTISM The Peer Teaching Society is not liable for false or misleading information… ACROMEGALY SYMPTOMS CVS: RS: Snoring GI: “Wonky bite” (malocclusion) Int: ↑Sweating Endo: ↑Weight UG: ↓libido; amenorrhoea MSK: Arthralgia; backache Neuro: Acroparaesthesia; headache SIGNS Skin darkening Acanthosis nigricans Big supraorbital ridge Interdental separation Macroglossia Prognathism Laryngeal dyspnoea OSA Spade-like hands and feet Tight rings Carpal tunnel syndrome ACROMEGALY: COMPLICATIONS • Impaired glucose tolerance (40%) and Diabetes Mellitus (15%) • Vascular: HTN; LVH; cardiomyopathy; arrhythmias; IHD; stroke • Colon cancer The Peer Teaching Society is not liable for false or misleading information… ACROMEGALY: INVESTIGATIONS • GOLD STANDARD = IGF-1 and OGTT • Don’t rely on random GH: pulsatile secretion • ↑Glucose, ↑Ca2+, ↑PO43• MRI pituitary fossa, visual field and acuity • Old photos ACROMEGALY: TREATMENT • Trans-sphenoidal surgery to remove tumour • Somatostatin analogue (SSA) – e.g. IM octreotide or lanreotide (NB GI side effects) • Radiotherapy • Pegvisomant (recombinant GH analogue) The Peer Teaching Society is not liable for false or misleading information… ADH (AVP) Action of ADH Collecting duct 300 This is the collecting duct in water-rich conditions H20 1200 ADH (2) Action of ADH Collecting duct 300 ADH increases expression of Aquaporins in collecting duct and therefore the retention of water H20 1200 Diabetes Insipidus Lack of ADH Diabetes Insipidus Lack of ADH Collecting duct 300 Water not sufficiently reabsorbed from collecting duct H20 Large amounts of undilute urine 1200 Diabetes Insipidus Lack of ADH = Polydipsia = Polyuria • Glucose metabolism preserved • Dehydration • Hypernatremia Fluid restriction has minimal effect on urination Diabetes Insipidus Urine output falls, osmolarity increases Desmopressin stimulation Central = lack of ADH No change Rare causes (dipsogenic, gestational) Nephrogenic DI Diabetes Insipidus Treat with Desmopressin if neurogenic (central) Thiazide diuretics (hydrocholorothiazide) and amiloride are useful if nephrogenic And of course, if there’s a detectable underlying cause, you should treat that too The Peer Teaching Society is not liable for false or misleading information… SIADH It’s exactly the opposite of DI excessive ADH production The Peer Teaching Society is not liable for false or misleading information… SIADH Excess ADH production Collecting duct 300 Very small volumes of concentrated urine H20 1200 SIADH - symptoms Varied and generic Anorexia/nausea Aches and weakness Neuromuscular (myoclonus, reflex changes, tremor, ataxia…) Respiratory (cheyne-Stokes respiration, apparently) Neurological The Peer Teaching Society is not liable for false or misleading information… SIADH - Causes Natural causes fall into three main camps Central Nervous System Pulmonary Paraneoplastic Infection Infection Mass/bleed GBS/MS Really rare stuff First described in small cell lung cancer Other types too e.g. Ewing Sarcoma, GI and GU Abcess Asthma CF DRUG SIDE EFFECTS The Peer Teaching Society is not liable for false or misleading information… Diagnosis & Treatment Euvolaemic with Hyponatraemia Urine osmolarity > 100mOsm/kg Urine Sodium >40mEq/L Fluid restriction – increases Na concentration Tolvaptan – V2 vasopressin blocker The Peer Teaching Society is not liable for false or misleading information… I hope you all like arrows (I’m very sorry) Calcium Homeostasis Bone deposition Thyroid releases Calcitonin Ca absorption decreased Calcium falls Calcium rises Serum Calcium Approx 9-10mg/dL Calcium falls Calcium rises Bone resorption Increased GI uptake Ca absorption up Vit D production up The Peer Teaching Society is not liable for false or misleading information… PTH level rises Calcium Homeostasis Serum Calcium Approx 9-10mg/dL Calcium falls Calcium rises PTH level rises Bone resorption Increased GI uptake Ca absorption up Vit D production up The Peer Teaching Society is not liable for false or misleading information… Calcium Homeostasis (PTH only) Serum Calcium Approx 9-10mg/dL Calcium falls Calcium rises PTH level rises Bone resorption Increased GI uptake Ca absorption up Vit D production up The Peer Teaching Society is not liable for false or misleading information… Hyperparathyroidism Primary 80% due to adenoma Serum calcium RAISED – STONES BONES MOANS GROANS, as well as weakness and fatigue, muscle symptoms polyuria, polydipsia Asymptomatic actually most common Lab results PTH High Calcium High Phosphate (usually) low Phosphatase (usually) High Treat underlying cause (usually surgical) if symptomatic or asymptomatic with grossly abnormal test results (urine calcium or bone weakess) The Peer Teaching Society is not liable for false or misleading information… Hyperparathyroidism Secondary PTH is high to attempt to correct persistently low calcium levels CKD and vit D deficiency most common – GI disease such as bypass and Crohn’s are also possible PTH High Calcium Low Phosphate High Phosphatase High Usually asymptomatic in early stages ymptoms are predominantly bony – osteomalacia, joint pain The Peer Teaching Society is not liable for false or misleading information… Hyperparathyroidism Tertiary After many years of uncorrected secondary hyperparathyroidism The Peer Teaching Society is not liable for false or misleading information… Hyperparathyroidism Differentiating blood results PTH Calcium Phosphate Alk Phos Primary Secondary Tertiary The Peer Teaching Society is not liable for false or misleading information… Hypoparathyroidism LOW CALCIUM --- Parasthaesia (especially around mouth and lips) --- Tetany (Chvostek’s sign & Trousseau’s sign) --- Increased reflexes --- QT elongation as well as reduced rate and contractility Convulsions Arrhythmia Tetany Go numb The Peer Teaching Society is not liable for false or misleading information… Yes, this was available with a simple Google search Hypoparathyroidism Surgical the big one Autoimmune DiGeorge (and other, rarer causes of Parathyroid absence) Haemochromatosis Familial forms Pseudohypoparathyroidism – PTH levels OK, peripheral resistance Pseudopseudo (RARE) – skeletal defects, inherited via father, biochemically normal The Peer Teaching Society is not liable for false or misleading information… Thanks, Wiki The Peer Teaching Society is not liable for false or misleading information… Oh, whilst we’re here The Peer Teaching Society is not liable for false or misleading information… Hypocalcaemia The Peer Teaching Society is not liable for false or misleading information… Hypocalcaemia There are an unbelievable number of possible causes Drug therapy – bisphosphonates calcitonin included, as well as other weird stuff REDUCED INTAKE Dietary insufficiency Malabsorption Alkalosis Because the albumin dissociates from hydrogen and picks up calcium Reduced Vit D Lack of sunlight Vit-D dependent rickets Anticonvulsant therapy Kidney failure Rhadomyolysis The Peer Teaching Society is not liable for false or misleading information… Hypocalcaemia I wrote all that then found that Derbyshire NHS trust has conveniently already done this… The Peer Teaching Society is not liable for false or misleading information… Hypocalcaemia Admit if severe - <1.8mmol or <2.0mmol/L with symptoms Calcium replacement with calcium glucoronate – IV for severe Out in general practice everyone* takes Adcal (Calcium + Vit D3) *I’m exaggerating, obviously** **Although not much The Peer Teaching Society is not liable for false or misleading information… HYPOKALAEMIA • K+ < 3.5mmol/L (severe <2.5mmol/L) • Muscle weakness, cramps, ↓tone, ↓reflexes, palpitations, arrhythmias, constipation • ECG: In ↓K+, U have no Pot and no Tea but a long PR and a long QT • Causes = Diuretics; V/D; Cushing’s; Conn’s; Pyloric stenosis; Alkalosis HYPERKALAEMIA • K+ > 5.5mmol/L (severe >6.5mmol/L) • Myocardial excitability → VF and cardiac arrest • ECG: Tall tented T waves, small P waves, wide QRS (eventually becoming sinusoidal), VF • CAUSES: Oliguric renal failure; K-sparing diuretics; Rhabdomyolysis; Addison’s; Burns; Metabolic acidosis (DM); ACEi HYPERKALAEMIA: TREATMENT NON-URGENT: - Treat underlying cause, review meds, polystyrene sulfonate resin (binds K+ in gut) EMERGENCY: - Stabilize cardiac membrane: 10ml 10% Calcium Gluconate - Drive K+ into cells: 10U Actrapid (insulin) in 50ml 20% glucose (salbutamol nebs, NaHCO3-) The Peer Teaching Society is not liable for false or misleading information… CARCINOID TUMOURS • Diverse group of tumours of enterochromaffin cell (neural crest) origin • Produce 5HT (serotonin) • May also secrete bradykinin, tachykinin, substance P, VIP, insulin, etc • Appendix (45%), ileum (30%), rectum (20%) • Consider all as malignant QUESTION 1 A 46-year-old woman is referred to endocrine with a tender neck swelling. Blood results are as follows: TSH <0.1 mU/l T4 188 nmol/l Hb 14.2 g/dl Plt 377 * 109/l WBC 6.4 * 109/l ESR 65 mm/hr Technetium thyroid scan shows decreased uptake globally The Peer Teaching Society is not liable for false or misleading information… QUESTION 1 What is the most likely diagnosis? (a) Sick thyroid syndrome (b) Acute bacterial thyroiditis (c) Hashimoto’s thyroiditis (d) Subacute thyroiditis (e) Toxic multinodular goitre The Peer Teaching Society is not liable for false or misleading information… QUESTION 1 What is the most likely diagnosis? (a) Sick thyroid syndrome (b) Acute bacterial thyroiditis (c) Hashimoto’s thyroiditis (d) Subacute thyroiditis (e) Toxic multinodular goitre The Peer Teaching Society is not liable for false or misleading information… QUESTION 1: RATIONALE • Subacute thyroiditis (also known as De Quervain’s thyroiditis) is suggested by the tender goitre, hyperthyroidism and raised ESR. • The globally reduced uptake on technetium thyroid scan is also typical The Peer Teaching Society is not liable for false or misleading information… QUESTION 2 QUESTION 2 What does the ECG show? (a) (b) (c) (d) (e) Hypokalaemia Hyperkalaemia Hypercalcaemia Hyponatraemia WPW syndrome The Peer Teaching Society is not liable for false or misleading information… QUESTION 2 What does the ECG show? (a) (b) (c) (d) (e) Hypokalaemia Hyperkalaemia Hypercalcaemia Hyponatraemia WPW syndrome The Peer Teaching Society is not liable for false or misleading information… RATIONALE FOR QUESTION 2 This ECG displays many of the features of hyperkalaemia: • Prolonged PR interval. • Broad, bizarre QRS complexes — these merge with both the preceding P wave and subsequent T wave. • Peaked T waves. The Peer Teaching Society is not liable for false or misleading information… QUESTION 2 QUESTION 3 QUESTION 3 What does the ECG show? (a) (b) (c) (d) (e) Hypokalaemia Hyperkalaemia Hypercalcaemia Hyponatraemia WPW syndrome The Peer Teaching Society is not liable for false or misleading information… QUESTION 3 What does the ECG show? (a) (b) (c) (d) (e) Hypokalaemia Hyperkalaemia Hypercalcaemia Hyponatraemia WPW syndrome The Peer Teaching Society is not liable for false or misleading information… RATIONALE FOR QUESTION 3 Hypokalaemia: • • • • ST depression. T wave inversion. Prominent U waves. Long QU interval. The Peer Teaching Society is not liable for false or misleading information… QUESTION 3 QUESTION 4 Patient comes in with: - Low sodium Raised potassium Raised calcium Eosinophilia What is the diagnosis? QUESTION 4 Addison’s disease RATIONALE: Destruction of the adrenal cortex leads to loss of mineralocorticoid and corticosteroid production. Sodium is therefore not retained as normal and potassium not expelled. QUESTION 5 What is the treatment for HYPERthyroidism? HYPERTHYROIDISM: TREATMENT (i) β-blockers: - Propanolol (rapid control of symptoms) (ii) Antithyroid medication: - Titration (carbimazole: SE = AGRANULOCYTOSIS) - Block and replace (carbimazole + thyroxine) (iii) Radioiodine (131I) (iv) Thyroidectomy