Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
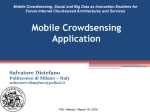
Cardiovascular Perspective Challenge of Informing Patient Decision Making What Can We Tell Patients Considering Long-Term Mechanical Circulatory Support About Outcomes, Daily Life, and End-of-Life Issues? Lucy J. Boothroyd, PhD; Laurie J. Lambert, PhD; Anique Ducharme, MD, MSc; Jason R. Guertin, MSc; Georgeta Sas, MD, MSc; Éric Charbonneau, MD; Michel Carrier, MD; Renzo Cecere, MD; Jean E. Morin, MD; Peter Bogaty, MD Background Downloaded from http://circoutcomes.ahajournals.org/ by guest on June 16, 2017 to transplantation, we do not consider in this perspective the other clinical recourses to MCS (rescue therapy and bridge to decision) where circumstances may make the informed decision-making process particularly problematic. Our work is aimed at not only specialists in the field but also the general cardiology audience that may not be familiar with this specialized literature. Our methods included a search of the peer-reviewed scientific literature published in English or French from January 2000 to the end of December 2012, using the PubMed bibliographic database and key words and reference lists of retrieved documents. We consulted primary research articles and consensus scientific statements, expert opinion editorials, and review articles. The most recent clinical practice guidelines concerning MCS by the International Society for Heart and Lung Transplantation and the most recent annual report of the Interagency Registry for Mechanically Assisted Circulatory Support, at the time of our review, were also consulted. We extracted data on outcomes from all empirical studies of DT patients who received HeartMate II (the implantable device currently most often used for DT) and that were published since 2008 (the year in which the device was approved for DT in the United States). We also extracted data from all empirical studies that involved ≥1 DT patients (or informal caregiver of a DT patient) on living with MCS, providing care to a recipient, or terminating MCS. For studies with mixed patient populations, information specific to DT patients was extracted whenever possible. An independent committee of clinical experts (1 cardiologist [A.D.] and 3 cardiac surgeons [É.C., M.C., R.C.]), active in the MCS domain, assisted with the interpretation of results. In the management of advanced heart failure, the option of long-term mechanical circulatory support (MCS) as destination therapy (DT), rather than as a temporary bridge to cardiac transplantation, is increasingly being offered to highly selected patients. Recent technological advancements in implantable devices, such as continuous flow systems and smaller pump sizes, have increased the possibility of survival with fewer complications. Informed consent before MCS is essential1–6 and is a fundamental aspect of patient-centered care. As a part of a quality decision-making process, the patient considering MCS and his/her informal caregiver(s) need to be aware of the current state of the scientific evidence, including what is known and unknown about outcomes and living with MCS and must navigate a series of interactions with clinicians before deciding on the treatment course. Editorial see p 13 The Institut National d’Excellence en Santé et en Services Sociaux is a health technology assessment and clinical guideline development organization in the province of Quebec (Canada) that provides multiple stakeholders (ie, government officials, hospital administrators, physicians, and patient organizations) with evidence-based information. In 2011, the Quebec Ministry of Health requested that the Institut National d’Excellence en Santé et en Services Sociaux provide recommendations on the use of implantable left ventricular assist devices in end-stage chronic heart failure. The current article extends the work submitted to the Ministry1 and focuses on MCS use in DT, within the framework of informed decision making. In this perspective piece, we report on our review of the scientific literature concerning clinical outcomes in DT and on perspectives of DT patients and their caregivers, to provide a summary of currently available information and identify gaps in knowledge. Besides the use of MCS as a bridge Framework: Informed Decision Making Informed decision making is an ethical norm and legal mandate, which refers to the voluntary choosing of an intervention (or of no intervention) by a patient, or by his/her decision-making proxy, in light of ongoing discussion with From the Institut National d’Excellence en Santé et en Services Sociaux, Montreal, Quebec, Canada (L.J.B., L.J.L., J.R.G., G.S., J.E.M., P.B.); Institut de Cardiologie de Montréal, Montreal, Quebec, Canada (A.D., M.C.); Centre de Recherche du Centre Hospitalier de l’Université de Montréal, Montreal, Quebec, Canada (J.R.G.); Institut Universitaire de Cardiologie et Pneumologie de Québec, Quebec, Canada (É.C., P.B.); and McGill University Health Centre, Montreal, Quebec, Canada (R.C., J.E.M.). The Data Supplement is available at http://circoutcomes.ahajournals.org/lookup/suppl/doi:10.1161/CIRCOUTCOMES.113.000243/-/DC1. Correspondence to Lucy J. Boothroyd, PhD, INESSS, 2021 Union Ave, Suite 10.083, Montreal, Quebec H3A 2S9, Canada. E-mail lucy.boothroyd@ inesss.qc.ca (Circ Cardiovasc Qual Outcomes. 2014;7:179-187.) © 2014 American Heart Association, Inc. Circ Cardiovasc Qual Outcomes is available at http://circoutcomes.ahajournals.org 179 DOI: 10.1161/CIRCOUTCOMES.113.000243 180 Circ Cardiovasc Qual Outcomes January 2014 Downloaded from http://circoutcomes.ahajournals.org/ by guest on June 16, 2017 the physician about treatment options and their respective benefits and risks.4,5,7 It is viewed as “an exchange of ideas that buttresses the physician–patient relationship.”7 The Figure summarizes the central elements of an informed decisionmaking process concerning MCS, grouped by topic. The process should ideally be (1) patient-centered, (2) timely, (3) comprehensive, (4) bidirectional (patient↔care providers), (5) multidisciplinary, (6) ongoing, and (7) responsive to changes in situation and preferences. In addition to receiving information about the reported clinical outcomes of long-term MCS,2–6,8 specific to the device being offered, we think that to be fully informed, the patient should also be made aware of the limitations of current scientific evidence2 and be given some sense of how similar patients in the literature are to him or herself. The information should be based on the best available evidence and appropriately collected, summarized, and appraised. Importantly, this information should be made comprehensible to a lay audience. We believe 3 important considerations pertain to the framing of the patient–clinician discussion about long-term MCS: (1) in advanced heart failure, as in other areas of medicine, there is inherent uncertainty on a patient’s specific course; (2) MCS may be the only option left to the patient to extend his/her life (although in some settings the patient considering MCS as DT may be less sick); and (3) the extent to which patients and their informal caregivers will be able to absorb information and grasp details about clinical outcomes and research findings can Figure. Key elements of the informed decision making process in long-term MCS.2–6,8 DT indicates destination therapy; and MCS, mechanical circulatory support. be highly variable given the gravity of a patient’s condition, the circumstances in which the discussions take place, and differing degrees of patient and caregiver comprehension. Anticipated Benefits and Risks of MCS From a total of 831 citations identified by our literature search, we retained 7 articles that addressed this theme, representing an evidence base of a maximum of ≈2000 DT patients. Five articles concerned clinical research studies: a multi-center randomized controlled trial,9 a multi-center continued protocol access case series following the trial,10 an analysis of data from these first 2 studies,11 a case series from a single center that participated in the first 2 studies,12 and a multicenter investigation of neurocognitive function on a subset of the trial patients.13 Two articles presented data from the Interagency Registry for Mechanically Assisted Circulatory Support in the United States from June 23, 2006, to June 30, 2012 (114 centers),14 and to December 31, 2011 (specific to DT).15 The registry did not include the patients enrolled in the trial or the continued access series. Overall, the average age of DT patients in the literature was ≈63 years, and the majority (80%) of patients in the research studies were men. Before MCS in the research studies, most patients (66%) were in New York Heart Association class IV (heart failure symptoms were experienced even at rest), 64% were not ambulatory, and 75% were receiving intravenous inotropic therapy. Before MCS, ≈75% of registry DT patients were in 1 of the 3 most severe Interagency Registry for Mechanically Assisted Circulatory Support profile levels, indicating their hemodynamic status: 11% critical cardiogenic shock (level 1), 38% progressive decline (level 2), and 30% stable but inotrope-dependent (level 3). The research studies specify that the median duration of MCS was 1.7 to 2.1 years (minimum <1 month, maximum 6 years). Table 1 summarizes the results with respect to clinical outcomes documented in the literature (What We Know column). We also summarize limitations and missing elements (What We Do Not Know column). In Table I in the Data Supplement, the number of persons with data is specified for each outcome, and details about study patients are provided. Table 1 shows that survival, functional capacity, end-organ function, and quality-of-life results are favorable in the published literature. Based on the most recent available data, DT patients have shown a 75% chance of surviving for 1 year and a 66% chance of surviving for 2 years.10,15 The patient considering DT needs to understand that there is a certain level of uncertainty surrounding study-based estimates. For individualized assessment of expected survival whether the patient accepts or declines MCS, the clinician considers patient risk factors such as age, clinical status (including Interagency Registry for Mechanically Assisted Circulatory Support profile level, renal dysfunction, and right ventricular function), the patient’s unique psychosocial profile, medical history, medication intolerance, and the complexity of the surgical procedure(s) being considered.2,14,19,20 Risk models are used to help assess likelihood of survival,19 as well as the likelihood of complications during MCS for an individual patient,21,22 but are likewise associated with uncertainity2 (a review of these is beyond the scope of this perspective). Moreover, the value Boothroyd et al Informing Patients About Cardiac Assist Devices 181 Table 1. Clinical Outcomes for DT Patients What We Know What We Do Not Know Survival* No published information beyond 2 y After 1 y, about three fourths of recipients were alive on support (most recent data).10,14 After 2 y, about two thirds of recipients were alive10,14 Limited numbers of patients with 2-y data: 100–150 persons for NYHA class, 6-minute walk distance, activity level, time spent readmitted, adverse events; <50 patients for end-organ function NYHA class No published information on other important end-organ function (hepatic, renal) Before implantation, 0% of patients in class I/II; at 6 mo, this figure was 80%9,10 (a change of 1 class is considered important).16 Same result after 2 y9,10 For functional, end-organ, and quality-of-life tests, results (and patients’ features) not known for those who could not be evaluated 6-minute walk distance Before implantation, ambulatory patients could walk an average of ≈200 m.9,10 At 6 mo, this figure was >340 m9,10 (>100 m farther; 25 m farther is considered important).16 Same result at 2 y9,10 We do not know whether research study participants do better, or worse, than other DT patients Activity level† Downloaded from http://circoutcomes.ahajournals.org/ by guest on June 16, 2017 Before implantation, 4% of patients could perform moderate to very high activity. At 6 mo, this figure was 62%11 (a change of 1 activity level is considered important).16 Same result at 2 y11 End-organ function Compared with before implantation, recipients had stable or improved neurocognition‡ at 6 mo using standardized tests.13 Same result at 2 y13 Quality of life§ Based on standardized tests and compared with scores before implantation, recipients showed improvements in overall quality of life scores at 6 mo that are considered important in real life.9,10,14 Same results at 19,10,14 and 2 y9,10 Initial hospitalization After the implantation procedure, 50% of patients spent ≥23 days in hospital.10 A total of 87% of patients were discharged9,10 No information about either the range in length of the initial hospitalization or the features of those who were not discharged Hospital readmissions during support No information on how many patients have ≥1 readmission A total of 81% were readmitted at least once for an average of 8 days/patient per year12 No information about the outcomes for those who had repeated readmissions Per patient there were 0.4–2.3 readmissions/y12 No information about the range (in days) in length of support time in hospital Primary causes: bleeding (30% of readmissions); cardiac-related (24%); infection (14%); thrombosis (7%); major neurological event (6%); liver-related (4%); pump alarm or abnormal readout (3%)12 Recipients spent 12% of support time in hospital9 Adverse events during support Categories are nonexclusive Percentage of recipients affected (most recent data10): Bleeding, transfusion║,¶ 74 Renal failure║ 11 Cardiac arrhythmias# 50 Pump replacement 8 Local infection 45 Ischemic stroke 8 Sepsis 28 Pump pocket infection 7 Respiratory failure║ 38 RVAD required║ 6 Device-related infection 30 Pump thrombosis 6 Driveline infection 27 Hemorrhagic stroke 5 Bleeding requiring surgery║ 20 Hemolysis 5 Right heart failure║ 21 Hepatic dysfunction 29 Other neurological** 17 9 No information about either the length of hospital stay (if any) related to complications or impact on patient quality of life We do not know whether research study participants do better or worse than other DT patients in terms of adverse events (Continued ) 182 Circ Cardiovasc Qual Outcomes January 2014 Table 1. Continued What We Know What We Do Not Know Percentage of recipients readmitted to hospital for event12: Cardiac problem‡‡ 38 Major neurological event## Bleeding§§ 36 Alarm/readout 14 7 Infection║║ 23 Biliary problem 6 Thrombosis¶¶ 14 Downloaded from http://circoutcomes.ahajournals.org/ by guest on June 16, 2017 DT indicates destination therapy; NYHA, New York Heart Association; and RVAD, right ventricular assist device. *Kaplan–Meier estimates with censoring at any left ventricular assist device explantation. †Patient-reported exercise ability. Highest level of activity varied from very low (eg, bedridden; unable to care for self; no physical activity) to moderate (eg, casual walking speed; gardening; vacuuming; golfing; wall painting) to very high (eg, dancing; climbing stairs; rapid stationary cycling; heavy shoveling). ‡Stable results if normal at baseline; improved function if abnormal. Tests included visual/spatial perception, memory, executive functions, language, and processing speed. §Tests specific to heart failure: Kansas City Cardiomyopathy Questionnaire, Minnesota Living With Heart Failure Questionnaire; scores improved by ≥30 points (≥5 is considered important).16 General tests: EQ-5D questionnaire, EQ-5D visual analogue scale. ║Occurs more often in first 30 days of support, according to temporal data from patients on bridge to transplantation.17,18 ¶Requiring packed blood cells. #Requiring cardioversion or defibrillation. **Including transient ischemic attack, seizures, and confusion. ‡‡Arrhythmia, heart failure, or chest pain. §§Any bleeding, anemia. ║║Device-related or unrelated. ¶¶Thromboembolism, suspected device thrombosis. ##Cerebrovascular accident or intracranial bleed. given to survival estimates on MCS will vary as a function of the importance each patient assigns to the possibility of living longer, and better (see below), and the price the patient is willing to pay in terms of constraints and potential complications. Current data estimate that 80% of tested left ventricular assist device recipients had no or only slight activity limitations at 2 years after implantation (ie, New York Heart Association class I or II symptoms).9,10 The patients who were tested before implantation were in New York Heart Association class III (30% of patients) or class IV (70%).9,10 Patients who were ambulatory before receiving MCS became able to walk an average of >340 m in 6 minutes (ie, the length of 3 football fields) 2 years later.9,10 Sixty percent of recipients could perform at least moderate if not more strenuous activities at 2 years (eg, walking at a casual speed, light gardening, or housekeeping); only 4% reported such activity levels before implantation.11 Tested patients reported significantly improved quality of life at 2 years compared with before MCS.9,10 Impact on quality of life, rather than only survival, is central to the decision-making process for a patient considering DT.4,9,23,24 However, it is at present difficult to predict whether functional and quality-of-life benefits are likely to be experienced by the individual patient,21 and the postoperative course (including the possible development of complications) is uncertain. Table 1 shows that adverse events during left ventricular assist device support are common, and many are life-ending or life-altering (eg, stroke). Based on the most recent article that provides data in terms of the number of patients affected,10 74% of DT patients had bleeding that required a transfusion (≥2 U of red blood cells within 24 hours), 50% had an arrhythmia requiring cardioversion or defibrillation, and at least 27% developed a device-related or blood-borne infection requiring antimicrobial therapy. Although bleeding requiring surgery or transfusion was much more frequent in the first 30 days after implantation, arrhythmias and infections could occur throughout MCS (based on temporal data from bridge to transplantation MCS patients). The most frequent infections related to a device component were those involving the driveline exiting the body; most infections of this type occur after the first 30 days of support. Ischemic stroke affected 8%, hemorrhagic stroke affected 5%, and 8% had their pump replaced. In the first 6 months after implantation, readmissions for complications were most often the result of bleeding and cardiac problems (arrhythmia, heart failure, or chest pain).12 Besides the complexity of individualized risk assessment, the main limitations of the findings on clinical outcomes include the paucity of data >2 years of support. Even during the first 2 years, relatively small numbers of patients provide data for some outcomes (eg, neurocognition). These are critical points because DT is by definition intended as long-term support. The possibility that the results are biased toward patients doing better should also be considered because not everyone could be tested at all time points for all outcomes. Expectations for Daily Life Patients using MCS must maintain regular contact with the MCS team, travel to medical appointments, undergo frequent clinical tests, manage equipment (eg, tend to dressings, respond to alarms, change batteries, perform system tests, and protect parts from moisture), and continue to adhere to a strict medication regimen.25,26 Adaptation of lifestyle is required,3,25,27 and availability of social support is essential.3,5,26 As another part of the informed decision-making process, therefore, the patient considering DT requires information on what to expect in daily life on MCS.4 Meeting and being able to exchange with a patient already on MCS can be most helpful. From a total of 108 citations identified by our literature search, we retained 7 articles that examined this theme.28–34 Boothroyd et al Informing Patients About Cardiac Assist Devices 183 Although multiple domains of life were addressed, this literature was limited: studies had small sample sizes (5–15 persons), all took place at single sites, and 5 studies were from the same institution in the United States. Information specific to DT patients or their informal caregivers were almost always lacking because 6 study samples also included patients who received MCS for other indications (notably MCS as a bridge to cardiac transplantation). For most of the results presented below (unless otherwise indicated), ≈20% of study participants received DT. Patients varied in age from 31 to 76 years, and caregivers were 39 to 71 years of age. Eight-five percent of patients were men; all caregivers were women. Results and their limitations are summarized in Table 2, whereas details on the evidence base for each outcome are provided in Table II in the Data Supplement. The studies show that life on MCS required major adjustment for both patients and their caregivers, and that the early experience could be frightening and overwhelming.28–30 Despite a new lease on life offered by the treatment, MCS affected multiple aspects of life, including hygiene, sleep, the environment, daily routines, and personal and intimate relationships.28,31 An initial adjustment period of ≈3 months was difficult for both MCS recipients and informal caregivers.28,30 Informal caregivers, who described caregiving as a 24/7 responsibility, settled into their role and new lifestyle with time.28,30 Most MCS recipients reported being satisfied with intimate relations after implantation, after various adaptations and self-care behaviors Table 2. Patient/Caregiver Perspectives on Daily Life With MCS Downloaded from http://circoutcomes.ahajournals.org/ by guest on June 16, 2017 What We Know What We Do Not Know Lifestyle adaptation 28,29 Adjustment took time Poor quality of life and major limitations before MCS Positive feelings on MCS as well as awe, dismay, feeling overwhelmed about care Early adjustment involved changes in hygiene, sleep, home environment, clothing, routines, personal relationships, socialization, and employment Early fear, anxiety, and low self-confidence Adjustment process difficult for many recipients Late adjustment (after 3 mo) involved accepting a new way of living; DT patients reported positively embracing MCS Except for the study on psychological disorders, we do not have much information specific to DT patients (or their caregivers) unless indicated because the investigations include patients bridged to transplant We do not know whether the results for recipients in these research studies are applicable to most DT patients. For example, study participants may do better or worse than other patients We do not know whether the caregiving results are applicable to most caregivers of DT patients or to male caregivers We do not know how reproducible the results on caregiving,30 sex/intimacy,31 and psychological disorders34 are because they come from single studies Feelings reported by recipients: facing the unknown, feeling confined (in hospital; because of dependence on others), shame when out with the device, overwhelming fear, and hope for the future Despite difficulties, would accept MCS again Adjustment to caregiving30 Caregiving a 24/7 responsibility Feelings reported by caregivers: hyper-vigilance, less time for personal activities, settling into role with time, adjusting was overwhelming in first 3 mo Caregiving extended beyond technical tasks to a supportive role, requiring a new lifestyle and coping strategies; satisfaction with caregiving developed with time Sex and intimacy31 Improved sexual functioning after MCS Most recipients satisfied with their sexual relations and intimacy Adaptations and self-care behaviors used to maintain normal intimate relations Most recipients reported partners being fearful of sex; some partners wanted to abstain Sleep32,33 Significant sleep disturbances before MCS and at 6 mo of support Short sleep duration and quality before MCS and at 6 mo of support Average total sleep time: 4.2 h before MCS and 4.6 h at 6 mo At 6 mo, significant improvement in overall quality of life, modest improvement in sleep quality, and daytime alertness Psychological disorders34 Diagnoses among DT patients seen by a psychologist in the postoperative period: adjustment disorder (47%), acute stress reaction (20%), depressive episode (20%), panic disorder (7%), and 13% had no disorder DT indicates destination therapy; and MCS, mechanical circulatory support. We do not know whether patients on MCS seen by a psychologist differ from those not seen 184 Circ Cardiovasc Qual Outcomes January 2014 were undertaken although some of their partners were fearful of sexual activity.31 Sleep disturbances were common: in a study of 12 patients (25% DT), all displayed both short sleep duration (average 4.5 hours) and poor sleep quality at 6 months after implantation despite significant improvement in overall quality of life.32,33 In a study of recipients of DT who consulted an in-hospital psychology service in the postoperative period, adjustment disorders affected nearly half of patients; both an acute stress reaction and a depressive episode affected 20% of recipients.34 These studies provide useful real-world information for DT candidates, although they may be more reflective of recipients who are willing to participate in research studies, of particular centers, or of recipients who receive MCS as a temporary measure (because most study participants were actually awaiting transplantation). Finally, these studies may represent success stories rather than mirroring all experiences. Downloaded from http://circoutcomes.ahajournals.org/ by guest on June 16, 2017 Device Deactivation and Other End-of-Life Issues Documented end-of-life care planning, in general, and explicit discussions about device deactivation, in particular, are recommended before MCS.2–4,6,8,20 There is a consensus in American and European position statements that patients (or their surrogate decision makers) have the right to request active discontinuation of MCS.2,35 This differs from assisted suicide and euthanasia because the intent is ending a treatment that is preventing natural progression of a pre-existing disease.4,36,37 Recent position statements highlight the importance of involving a collaborative, multidisciplinary team in end-of-life care planning and the central role of palliative care professionals in these discussions.2,3,19,35 From a total of 108 citations identified by our literature search, we retained 5 articles pertaining to end-of-life issues.35,38–41 This literature was very limited: studies were small (14–68 persons), and 4 were from single sites (3 from the same hospital). Two studies involved exclusively DT patients. Patients varied in age from 19 to 83 years; 86% were men. Results and their limitations are summarized in Table 3, whereas details on the evidence base for each outcome are provided in Table III in the Data Supplement. Table 3 lists some examples of issues that were not addressed by the available literature that include optimal timing of discussions and psychological effects. The studies show that DT patients were more likely to have documented care directives in their medical charts if they were formally involved in advance care preparedness planning,38 and that palliative care consultations for patients using MCS (≈60% DT) were both appreciated and associated with increased clarity about treatment plans.38,39 A 2003 to 2009 study (≈50% DT) found that none of the care directives of MCS patients in medical charts specifically mentioned the circumstances in which MCS might be deactivated.40 However, requests to terminate MCS were not uncommon: at the same center from 2003 to 2009, such requests were made for 21% of recipients (50% of these DT), usually by surrogate decision makers (85% of the time), because the patients no longer had decision-making capacity.35 Two studies we reviewed, one exclusive to DT, reported that decision making about terminating MCS was facilitated by open discussions with a multidisciplinary care team and by care providers giving detailed information about the deactivation process and palliative treatments.35,41 Most DT patients who actively participated in deactivation decisions had experienced a decline in quality of life because of clinical or functional deterioration.41 Discussion This perspective focuses on information transfer as an integral part of the decision-making process for patients considering long-term MCS and for whom subsequent heart transplantation is unlikely. Like the informed consent process itself, the exchange of information between care providers and patients should be bidirectional, timely, comprehensive, and responsive to changes in patient preferences and clinical course. We have summarized the current status of the scientific evidence in DT on 3 overarching topics. Information on clinical outcomes for DT patients is relatively plentiful. However, there is much less scientific literature about the impact of MCS on daily life for recipients and their informal caregivers/family. Nonetheless, this limited literature provides valuable information on the lived experience, including the ending of treatment. For all 3 topics, current data apply mostly to men.20 Sex-specific analyses among transplantation-eligible patients indicate similar clinical benefits in women and men, but differences in risks of adverse events.42 The unknowns that we have identified included gaps in knowledge, where information is lacking, and the applicability of findings from groups of research or registry participants to the individual patient considering MCS. For a DT candidate with advanced heart failure, his/her own clinical course, with or without MCS, is somewhat uncertain.2 Perhaps the most critical gap in knowledge for DT relates to the difficulty in precisely predicting who will achieve clinical and quality-of-life benefits afforded by long-term MCS and who will experience life-altering complications. There is a pressing need for predictive models that go beyond survival to guide patient decision making.2,24,26 Our results capture the state of the science as of early 2013. We searched peer-reviewed scientific publications and did not explore information available from other sources. Nevertheless, we have combined results from multiple themes and sources (eg, research studies, registries, and qualitative investigations). We have focused on patients considering MCS as DT rather than other indications such as bridge-to-transplantation. We appreciate that these categories are neither strictly distinct nor always easily discernible in clinical practice. Information transfer to patients is only 1 component of the decision-making process.7 Other aspects are careful, individualized assessment of the patient’s clinical, social, and psychological state; the use of risk models to assist with prognosis; and broader discussion about the goals of care.2 A scientific statement from the American Heart Association on decision making in advanced heart failure provides advice and tools addressing communication and the doctor–patient relationship.2 The complexity and time-consuming nature of treatment discussions in MCS and particularly DT is recognized, and decision aids are suggested to assist with the presentation of numeric data (such aids are conceived as more than simple information pamphlets; http://decisionaid.ohri.ca). Training for physicians in communication methods and a supportive environment for multidisciplinary, patient-centered care are Boothroyd et al Informing Patients About Cardiac Assist Devices 185 Table 3. Patient/Family Perspectives on Terminating MCS and Advance Care Planning What We Know What We Do Not Know PC consultation and AD 38–40 PC consultation received by 68% of 19 DT patients who were offered this service. The consultations occurred 5 days before to 16 days after implantation For 2 of the studies,39,40 no information specific to the DT patients A total of 85% of patients with consultation had documented ADs in chart vs 50% without consultation We do not know whether these results are applicable to most DT patients or those offered a different type of PC consultation Not all patients/families understood what PC consultation was We do not know whether patients on MCS who receive PC consultation differ from those who do not receive it Caregivers did not interpret candid discussion of issues negatively Patients seriously ill when DT was discussed; thus, there was variable engagement with PC team After implantation, some patients only vaguely recalled advance planning A total of 47% of MCS recipients had ADs in chart (39% for DT patients) Most (78%) of ADs completed before implantation Downloaded from http://circoutcomes.ahajournals.org/ by guest on June 16, 2017 No ADs specifically mentioned MCS deactivation; general statements about life-sustaining treatments in 63% of ADs We did not find information about the following: Level of satisfaction with end-of-life care Effects of advance care planning and end-of-life care on other aspects such as psychological well-being, decisional burden, quality of life, grief, and bereavement of loved ones Optimal timing for discussion(s) and best practices for end-of-life decision making Psychological effects of MCS deactivation on loved ones DT patients not more or less likely than transplantation-eligible patients to have ADs in chart PC consulted for: symptom management (mostly pain, insomnia), clarifying goals of therapy, advance care planning, hospice referral, and end-of-life care After consultation: decreased opioid use, improved management of pain and other symptoms, and increased clarity about treatment plans/goals PC consultation well received by patients/families A total of 30% of patients completed ADs after consultation Termination of MCS35,41 Two patients and 12 surrogates requested deactivation: ie, 21% of 68 patients receiving MCS in 2003–2009 Most had multi-organ failure, and on some other kind of support (eg, ventilation) A total of 50% had ADs in chart; none mentioned MCS For ≈80%, multidisciplinary conference held before deactivation to facilitate decision making A total of 85% of DT patients participating in end-of-life decisions chose to actively turn off device (vs waiting until unconscious) We do not know whether more patients would opt for device deactivation if discussions were carried out while the patient was still capable of decision making For one of these studies,35 information specific to the DT patients was not provided We do not know whether these results are applicable to most DT patients We do not know whether patients/surrogates who request termination of MCS differ from those who do not request it Situations motivating deactivation: infection/sepsis, renal failure, cancer, stroke /neurological decline, impending pump failure, illegibility for pump replacement Time from decision to deactivation: <1–14 days for active deactivation; 2–5 mo for those who waited to be unconscious Death ≤20 min after deactivation; 55% of patients died at home Discussions initiated by both patient/family and care providers after quality-of-life decline Open discussion with MCS team and supportive care at death appreciated by family AD indicates advance directives; DT, destination therapy; MCS, mechanical circulatory support; and PC, palliative care. recommended.2 And perhaps one of the most important elements in clinical encounters is helping the patient recognize that uncertainty persists in modern medicine.2 Indeed, these considerations highlight the inherent relativity of the fully informed concept, given the imponderables and the uniqueness of each patient with advanced heart failure. In this perspective, we have presented what we believe is the most comprehensive examination of the outcomes and experiences of DT patients in the scientific literature to date. The summaries of the themes herein presented may serve as the basis for an information tool for care providers to use with patients considering long-term MCS and with their informal caregivers. Such work will likely become increasingly relevant as waiting times for heart transplantation lengthen, availability of donor organs diminishes, and more and more patients are offered MCS as ultimate treatment for severe heart failure. Acknowledgments We are grateful to Dr Lynne Stevenson for her encouragement of our research and for her helpful comments on our article. 186 Circ Cardiovasc Qual Outcomes January 2014 Sources of Funding This work was supported by public funds. Disclosures None. References Downloaded from http://circoutcomes.ahajournals.org/ by guest on June 16, 2017 1. Institut National d’Excellence en Santé et en Services Sociaux. Évaluation des données probantes sur les dispositifs d’assistance ventriculaire gauche HeartMate II® et HeartWare® pour le traitement de l’insuffisance cardiaque chronique terminale. Montreal, Canada: INESSS; 2012. www. inesss.qc.ca/fileadmin/doc/INESSS/Rapports/Cardio/ETMIS2012_Vol8_ No15.pdf. Accessed December 18, 2013. 2.Allen LA, Stevenson LW, Grady KL, Goldstein NE, Matlock DD, Arnold RM, Cook NR, Felker GM, Francis GS, Hauptman PJ, Havranek EP, Krumholz HM, Mancini D, Riegel B, Spertus JA; American Heart Association; Council on Quality of Care and Outcomes Research; Council on Cardiovascular Nursing; Council on Clinical Cardiology; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Surgery and Anesthesia. Decision making in advanced heart failure: a scientific statement from the American Heart Association. Circulation. 2012;125:1928–1952. 3. Feldman D, Pamboukian SV, Teuteberg JJ, Birks E, Lietz K, Moore SA, Morgan JA, Arabia F, Bauman ME, Buchholz HW, Deng M, Dickstein ML, El-Banayosy A, Elliot T, Goldstein DJ, Grady KL, Jones K, Hryniewicz K, John R, Kaan A, Kusne S, Loebe M, Massicotte MP, Moazami N, Mohacsi P, Mooney M, Nelson T, Pagani F, Perry W, Potapov EV, Eduardo Rame J, Russell SD, Sorensen EN, Sun B, Strueber M, Mangi AA, Petty MG, Rogers J; International Society for Heart and Lung Transplantation. The 2013 International Society for Heart and Lung Transplantation Guidelines for mechanical circulatory support: executive summary. J Heart Lung Transplant. 2013;32:157–187. 4. Dudzinski DM. Ethics guidelines for destination therapy. Ann Thorac Surg. 2006;81:1185–1188. 5. Rizzieri AG, Verheijde JL, Rady MY, McGregor JL. Ethical challenges with the left ventricular assist device as a destination therapy. Philos Ethics Humanit Med. 2008;3:20. 6. Petrucci RJ, Benish LA, Carrow BL, Prato L, Hankins SR, Eisen HJ, Entwistle JW. Ethical considerations for ventricular assist device support: a 10-point model. ASAIO J. 2011;57:268–273. 7. Paterick TJ, Carson GV, Allen MC, Paterick TE. Medical informed consent: general considerations for physicians. Mayo Clin Proc. 2008;83:313–319. 8.Kirkpatrick JN, Fedson SE, Verdino R. Ethical dilemmas in device treatment for advanced heart failure. Curr Opin Support Palliat Care. 2007;1:267–273. 9. Slaughter MS, Rogers JG, Milano CA, Russell SD, Conte JV, Feldman D, Sun B, Tatooles AJ, Delgado RM III, Long JW, Wozniak TC, Ghumman W, Farrar DJ, Frazier OH; HeartMate II Investigators. Advanced heart failure treated with continuous-flow left ventricular assist device. N Engl J Med. 2009;361:2241–2251. 10. Park SJ, Milano CA, Tatooles AJ, Rogers JG, Adamson RM, Steidley DE, Ewald GA, Sundareswaran KS, Farrar DJ, Slaughter MS; HeartMate II Clinical Investigators. Outcomes in advanced heart failure patients with left ventricular assist devices for destination therapy. Circ Heart Fail. 2012;5:241–248. 11. Rogers JG, Aaronson KD, Boyle AJ, Russell SD, Milano CA, Pagani FD, Edwards BS, Park S, John R, Conte JV, Farrar DJ, Slaughter MS; HeartMate II Investigators. Continuous flow left ventricular assist device improves functional capacity and quality of life of advanced heart failure patients. J Am Coll Cardiol. 2010;55:1826–1834. 12. Hasin T, Marmor Y, Kremers W, Topilsky Y, Severson CJ, Schirger JA, Boilson BA, Clavell AL, Rodeheffer RJ, Frantz RP, Edwards BS, Pereira NL, Stulak JM, Joyce L, Daly R, Park SJ, Kushwaha SS. Readmissions after implantation of axial flow left ventricular assist device. J Am Coll Cardiol. 2013;61:153–163. 13. Petrucci RJ, Rogers JG, Blue L, Gallagher C, Russell SD, Dordunoo D, Jaski BE, Chillcott S, Sun B, Yanssens TL, Tatooles A, Koundakjian L, Farrar DJ, Slaughter MS. Neurocognitive function in destination therapy patients receiving continuous-flow vs pulsatile-flow left ventricular assist device support. J Heart Lung Transplant. 2012;31:27–36. 14. Kirklin JK, Naftel DC, Kormos RL, Stevenson LW, Pagani FD, Miller MA, Timothy Baldwin J, Young JB. Fifth INTERMACS annual report: risk factor analysis from more than 6,000 mechanical circulatory support patients. J Heart Lung Transplant. 2013;32:141–156. 15. Kirklin JK, Naftel DC, Pagani FD, Kormos RL, Stevenson L, Miller M, Young JB. Long-term mechanical circulatory support (destination therapy): on track to compete with heart transplantation? J Thorac Cardiovasc Surg. 2012;144:584–603; discussion 597. 16. Hrobowski T, Lanfear DE. Ventricular assist devices: is destination therapy a viable alternative in the non-transplant candidate? Curr Heart Fail Rep. 2013;10:101–107. 17. Pagani FD, Miller LW, Russell SD, Aaronson KD, John R, Boyle AJ, Conte JV, Bogaev RC, MacGillivray TE, Naka Y, Mancini D, Massey HT, Chen L, Klodell CT, Aranda JM, Moazami N, Ewald GA, Farrar DJ, Frazier OH; HeartMate II Investigators. Extended mechanical circulatory support with a continuous-flow rotary left ventricular assist device. J Am Coll Cardiol. 2009;54:312–321. 18. Starling RC, Naka Y, Boyle AJ, Gonzalez-Stawinski G, John R, Jorde U, Russell SD, Conte JV, Aaronson KD, McGee EC Jr, Cotts WG, DeNofrio D, Pham DT, Farrar DJ, Pagani FD. Results of the post-U.S. Food and Drug Administration-approval study with a continuous flow left ventricular assist device as a bridge to heart transplantation: a prospective study using the INTERMACS (Interagency Registry for Mechanically Assisted Circulatory Support). J Am Coll Cardiol. 2011;57:1890–1898. 19.McKelvie RS, Moe GW, Cheung A, Costigan J, Ducharme A, Estrella-Holder E, Ezekowitz JA, Floras J, Giannetti N, Grzeslo A, Harkness K, Heckman GA, Howlett JG, Kouz S, Leblanc K, Mann E, O’Meara E, Rajda M, Rao V, Simon J, Swiggum E, Zieroth S, Arnold JM, Ashton T, D’Astous M, Dorian P, Haddad H, Isaac DL, Leblanc MH, Liu P, Sussex B, Ross HJ. The 2011 Canadian Cardiovascular Society heart failure management guidelines update: focus on sleep apnea, renal dysfunction, mechanical circulatory support, and palliative care. Can J Cardiol. 2011;27:319–338. 20. Goodlin SJ, Hauptman PJ, Arnold R, Grady K, Hershberger RE, Kutner J, Masoudi F, Spertus J, Dracup K, Cleary JF, Medak R, Crispell K, Piña I, Stuart B, Whitney C, Rector T, Teno J, Renlund DG. Consensus statement: palliative and supportive care in advanced heart failure. J Card Fail. 2004;10:200–209. 21. Alba AC, Rao V, Ivanov J, Ross HJ, Delgado DH. Usefulness of the INTERMACS scale to predict outcomes after mechanical assist device implantation. J Heart Lung Transplant. 2009;28:827–833. 22. Bonde P, Ku NC, Genovese EA, Bermudez CA, Bhama JK, Ciarleglio MM, Cong X, Teuteberg JJ, Kormos RL. Model for end-stage liver disease score predicts adverse events related to ventricular assist device therapy. Ann Thorac Surg. 2012;93:1541–1547; discussion 1547. 23. Grady KL, Warner Stevenson L, Pagani FD, Teuteberg J, Pamboukian SV, Birks E, Moore S, Kirklin JK. Beyond survival: recommendations from INTERMACS for assessing function and quality of life with mechanical circulatory support. J Heart Lung Transplant. 2012;31:1158–1164. 24. Allen LA, Gheorghiade M, Reid KJ, Dunlay SM, Chan PS, Hauptman PJ, Zannad F, Konstam MA, Spertus JA. Identifying patients hospitalized with heart failure at risk for unfavorable future quality of life. Circ Cardiovasc Qual Outcomes. 2011;4:389–398. 25. Eshelman AK, Mason S, Nemeh H, Williams C. LVAD destination therapy: applying what we know about psychiatric evaluation and management from cardiac failure and transplant. Heart Fail Rev. 2009;14:21–28. 26.Peura JL, Colvin-Adams M, Francis GS, Grady KL, Hoffman TM, Jessup M, John R, Kiernan MS, Mitchell JE, O’Connell JB, Pagani FD, Petty M, Ravichandran P, Rogers JG, Semigran MJ, Toole JM; American Heart Association Heart Failure and Transplantation Committee of the Council on Clinical Cardiology; Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; Council on Cardiovascular Disease in the Young; Council on Cardiovascular Nursing; Council on Cardiovascular Radiology and Intervention, and Council on Cardiovascular Surgery and Anesthesia. Recommendations for the use of mechanical circulatory support: device strategies and patient selection: a scientific statement from the American Heart Association. Circulation. 2012;126:2648–2667. 27. Goldstein NE, May CW, Meier DE. Comprehensive care for mechanical circulatory support: a new frontier for synergy with palliative care. Circ Heart Fail. 2011;4:519–527. 28. Casida JM, Marcuccilli L, Peters RM, Wright S. Lifestyle adjustments of adults with long-term implantable left ventricular assist devices: a phenomenologic inquiry. Heart Lung. 2011;40:511–520. 29. Zambroski CH, Combs P, Cronin SN, Pfeffer C. Edgar Allan Poe, “The pit and the pendulum,” and ventricular assist devices. Crit Care Nurse. 2009;29:29–39. Boothroyd et al Informing Patients About Cardiac Assist Devices 187 Downloaded from http://circoutcomes.ahajournals.org/ by guest on June 16, 2017 30. Marcuccilli L, Casida JM. From insiders’ perspectives: adjusting to caregiving for patients with left ventricular assist devices. Prog Transplant. 2011;21:137–143. 31. Marcuccilli L, Casida JJ, Peters RM, Wright S. Sex and intimacy among patients with implantable left-ventricular assist devices. J Cardiovasc Nurs. 2011;26:504–511. 32. Casida JM, Davis JE, Brewer RJ, Smith C, Yarandi H. Sleep and daytime sleepiness of patients with left ventricular assist devices: a longitudinal pilot study. Prog Transplant. 2011;21:131–136. 33. Casida JM, Brewer RJ, Smith C, Davis JE. An exploratory study of sleep quality, daytime function, and quality of life in patients with mechanical circulatory support. Int J Artif Organs. 2012;35:531–537. 34. Heilmann C, Kuijpers N, Beyersdorf F, Berchtold-Herz M, Trummer G, Stroh AL, Schlensak C, Fritzsche K. Supportive psychotherapy for patients with heart transplantation or ventricular assist devices. Eur J Cardiothorac Surg. 2011;39:e44–e50. 35.Mueller PS, Swetz KM, Freeman MR, Carter KA, Crowley ME, Severson CJ, Park SJ, Sulmasy DP. Ethical analysis of withdrawing ventricular assist device support. Mayo Clin Proc. 2010;85:791–797. 36. Bramstedt KA, Wenger NS. When withdrawal of life-sustaining care does more than allow death to take its course: the dilemma of left ventricular assist devices. J Heart Lung Transplant. 2001;20:544–548. 37. Jaarsma T, Beattie JM, Ryder M, Rutten FH, McDonagh T, Mohacsi P, Murray SA, Grodzicki T, Bergh I, Metra M, Ekman I, Angermann C, Leventhal M, Pitsis A, Anker SD, Gavazzi A, Ponikowski P, Dickstein K, Delacretaz E, Blue L, Strasser F, McMurray J; Advanced Heart Failure Study Group of the HFA of the ESC. Palliative care in heart failure: a position statement from the palliative care workshop of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2009;11:433–443. 38. Swetz KM, Freeman MR, AbouEzzeddine OF, Carter KA, Boilson BA, Ottenberg AL, Park SJ, Mueller PS. Palliative medicine consultation for preparedness planning in patients receiving left ventricular assist devices as destination therapy. Mayo Clin Proc. 2011;86:493–500. 39. Schwarz ER, Baraghoush A, Morrissey RP, Shah AB, Shinde AM, Phan A, Bharadwaj P. Pilot study of palliative care consultation in patients with advanced heart failure referred for cardiac transplantation. J Palliat Med. 2012;15:12–15. 40. Swetz KM, Mueller PS, Ottenberg AL, Dib C, Freeman MR, Sulmasy DP. The use of advance directives among patients with left ventricular assist devices. Hosp Pract (1995). 2011;39:78–84. 41. Brush S, Budge D, Alharethi R, McCormick AJ, MacPherson JE, Reid BB, Ledford ID, Smith HK, Stoker S, Clayson SE, Doty JR, Caine WT, Drakos S, Kfoury AG. End-of-life decision making and implementation in recipients of a destination left ventricular assist device. J Heart Lung Transplant. 2010;29:1337–1341. 42. Hsich EM, Naftel DC, Myers SL, Gorodeski EZ, Grady KL, Schmuhl D, Ulisney KL, Young JB. Should women receive left ventricular assist device support?: findings from INTERMACS. Circ Heart Fail. 2012;5:234–240. Key Words: decision support techniques ◼ heart failure ◼ heart-assist devices Downloaded from http://circoutcomes.ahajournals.org/ by guest on June 16, 2017 Challenge of Informing Patient Decision Making: What Can We Tell Patients Considering Long-Term Mechanical Circulatory Support About Outcomes, Daily Life, and End-of-Life Issues? Lucy J. Boothroyd, Laurie J. Lambert, Anique Ducharme, Jason R. Guertin, Georgeta Sas, Éric Charbonneau, Michel Carrier, Renzo Cecere, Jean E. Morin and Peter Bogaty Circ Cardiovasc Qual Outcomes. 2014;7:179-187; originally published online January 14, 2014; doi: 10.1161/CIRCOUTCOMES.113.000243 Circulation: Cardiovascular Quality and Outcomes is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2014 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-7705. Online ISSN: 1941-7713 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circoutcomes.ahajournals.org/content/7/1/179 Data Supplement (unedited) at: http://circoutcomes.ahajournals.org/content/suppl/2014/02/12/CIRCOUTCOMES.113.000243.DC1 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Cardiovascular Quality and Outcomes can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Cardiovascular Quality and Outcomes is online at: http://circoutcomes.ahajournals.org//subscriptions/ CIRCCQO/2013/000243R2 SUPPLEMENTAL MATERIAL 1 Supplemental Table S1. Benefits and risks: evidence base Outcome SURVIVAL at 1 year at 2 years Who this is based on Registry: 2006-2012, 114 US centers; almost Registry of 1694 recipients of a CF device* as DT and 1 DT research study2 of 281 HM II recipients. all HM II; data for 1160 DT patients implanted in 2006-2011 in 104 US centers3: average patient age 63.6; average BSA 2.04 m2; 11% cardiogenic shock Same sources as above Research patients: 2007-2009, 38 US centers; average age 63.3; 79% male; average BSA 1.96 m2; 78% on inotropes 1 At baseline, average patient age ≈63; 79% male (data for all 414 patients who received a HM II in 2005-2009 in 38 US centers) at 2 years 2 DT research studies2, 4 of 393 HM II recipients evaluated at baseline (before implantation) and 276 evaluated at 6 months Same sources; 153 patients evaluated at 2 years 6-MINUTE WALK DISTANCE at 6 months 2 DT research studies2, 4 of 150 HM II recipients evaluated at baseline and 221 evaluated at 6 months At baseline, average patient age ≈63; 79% male (data for all 414 patients who received a HM II in 2005-2009 in 38 US centers) at 2 years Same sources; 134 patients evaluated at 2 years ACTIVITY LEVEL at 6 months 2 DT research studies2, 4 of 365 HM II recipients evaluated at baseline and 254 evaluated at 6 months. (reported by Rogers et al.5) at 2 years Same sources; 101 patients evaluated at 2 years END-ORGAN FUNCTION at 6 months 1 DT research study6 of 72 patients† evaluated both at baseline and at 6 months. at 2 years Same source; 33 patients† evaluated both at baseline and at 2 years NYHA CLASS at 1 year At baseline, average patient age ≈63; 79% male (data for all 414 patients who received a HM II in 2005-2009 in 38 US centers) Implantations in 2005-2007; 12 US centers At baseline, average patient age 61; 73% male; average BSA 2.0 m2; 76% on inotropes; 20% prior stroke (data for 96 HM II patients tested at baseline) 2 QUALITY OF LIFE at 6 months Registry1 of CF DT recipients: 852 persons evaluated at baseline and 466 evaluated at 6 months (general quality of life test) 2 DT research studies2, 4 of 360 HM II recipients evaluated at baseline and 270 evaluated at 6 months (tests specific to heart failure) at 1 year Same sources; 230 research study patients and 281 registry recipients evaluated at 1 year at 2 years Same research studies; 161 research study patients evaluated at 2 years INITIAL HOSPITALIZATION 1 DT research study2 of 281 HM II recipients; 1 earlier DT research study4, 134 patients randomly assigned to receive HM II. At baseline, average patient age ≈63; 79% male (data for all 414 patients who received a HM II in 2005-2009 in 38 US centers) HOSPITAL READMISSIONS: time spent in hospital 1 DT research study4 of 134 patients randomly assigned to HM II. At baseline, average patient age 62 (min: 26; max: 79); 81% male; 38 US centers 7 Rate and causes of readmissions 1 research study of 73 DT HM II patients (this sample likely overlaps somewhat with an earlier study of 281 HM II recipients2) ADVERSE EVENTS: % of recipients affected 2 DT research studies2, 4 of 414 HM II recipients who were observed for an average support duration of 20.5 months per person. Data on respiratory failure and hepatic dysfunction are available from one of these studies4 (133 patients observed for an average support duration of 19 months per person). Registry: At baseline, average patient age ≈64 (data for all 1160 DT patients implanted in 2006-2011 in 104 US centers3) Research patients: At baseline, average age ≈63; 79% male (data for all 414 patients who received a HM II in 2005-2009 in 38 US centers) At baseline, average age ≈62; 83% male; average initial hospital stay 16 days; 65% on inotropes; 1 US center (data for all 115 patients discharged who received a HM II in January 2008-June 2011; 42 of these patients were transplant-eligible) At baseline, average patient age ≈63; 79% male (data for all 414 patients who received a HM II in 2005-2009 in 38 US centers) 3 Data on timing of events from 1 research study8 of 281 HM II bridge-to-transplant recipients observed for an average support duration of 7.8 months, and from 169 registry patients9 who received HM II as bridge to transplant and were observed for an average support duration of 10.1 months % of recipients readmitted 1 research study7 of 73 DT HM II patients who were to hospital for each type of observed for an average support duration of 18 months per person (this sample likely overlaps event somewhat with an earlier study of 281 HM II recipients2) At baseline, average patient age 50; 76% male; received HM II in 2005-2008 in 33 US centers At baseline, patients aged 40-59 years; 78% male; received HM II in 2008 in 77 US centers At baseline, average age ≈62; 83% male; average initial hospital stay 16 days; 65% on inotropes; 1 US center (data for all 115 patients discharged who received a HM II in 2008-2011; 42 patients were transplanteligible) CF: continuous flow; DT: destination therapy; HM II: HeartMate II®; MCS: mechanical circulatory support; US: United States of America; BSA: body surface area; NYHA: New York Heart Association; min: minimum; max: maximum *We assume the continuous-flow devices in INTERMACS are almost exclusively HeartMate II®. †Sample size is the smallest number of patients tested for the various domains. 4 Supplemental Table S2. Expectations for daily life: evidence base Outcome LIFESTYLE ADAPTATION Who this is based on Research study , 1 US hospital; recruitment in 2009-2010 7 men, 2 women; aged 31-70 years (average 56); 0.54 years of support with HM II; most Caucasian, high Patients selected if on support for ≥ 3 months, out of hospital; interviewed in person for 15-102 minutes in school graduates, married, had a family caregiver outpatient clinic; asked about experience of living with 7 were transplant-eligible; 2 men were DT patients, MCS, lifestyle adjustments and adjustment strategies supported for 1 and 3.5 years, aged 56 and 66 10 Research study11, 1 US hospital Patients selected if were implanted in previous year Patients interviewed in person for 45-90 minutes in their homes; asked about living with MCS, how daily life had changed and other issues considered important to them 2 men, 4 women; aged 42-76 years (average 59); 113.5 months of support (likely HM II); most were Caucasian, married; 5 had received a heart transplant by time of interview; 1 had chosen DT All lived within a 3-hour drive of hospital ADJUSTMENT TO CAREGIVING Research study12, 1 US hospital Caregivers selected if had cared for a MCS recipient at home for ≥3 months; interviewed in person for 24-62 minutes in out-patient clinic; asked about their lifestyle adaptations and the meaning of MCS caregiving 5 women; aged 39-71 years Most were Caucasian, college educated, married, give care 24 hours/day 1 caregiver of a DT patient 4 caregivers of transplant-eligible patients SLEEP Research study13, 1 US hospital; recruitment in 2008-2009 Patients selected if MCS candidates; no sleep disorders Patients completed diaries/questionnaires and wore a wrist device to measure sleep for 3 days (at home), before MCS and up to 6 months after) 9 men, 4 women; average age 55 years Most were Caucasian, college educated, married 3 DT patients; 8 transplant-eligible (1 received a heart after 5 months); 2 bridge-to-decision (BTD) All had stage D heart failure Research study14, 1 US hospital; recruitment in 2008-2010 Patients completed standardized questionnaires before MCS and after 6 months, at the hospital 8 men, 4 women; average age 54 years; all HM II Almost all the same patients as above (but no heart recipient nor BTD); most patients NYHA class IV 5 SEX AND INTIMACY Research study15, 1 US hospital Patients selected if on support for ≥3 months, out of hospital; interviewed in person for 15-102 minutes in outpatient clinic; asked about experience of living with MCS, and their personal, social and intimate experiences 7 men, 2 women; aged 31-70 years (average 59); 0.54 years of support with HM II; most Caucasian, high school graduates, married, had a family caregiver 2 men were DT patients, supported for 1 and 3.5 years, aged 56 and 66 years PSYCHOLOGICAL DISORDERS Research study16, 1 hospital in Germany; all MCS patients offered psychological services DT patients recruited in 2008-2010; all seen by a psychologist and ICD-10 diagnoses assessed 13 men, 2 women; average age 62 years; 9-153 days of support (average 56) with HM II for 12 patients (3 had other devices) All DT patients HM II: HeartMate II®; MCS: mechanical circulatory support; US: United States; DT: destination therapy; NYHA: New York Heart Association; ICD-10: International Classification of Diseases version 10 6 Supplemental Table S3. MCS deactivation and other end-of-life issues: evidence base Outcome PALLIATIVE CARE (PC) CONSULTATION AND ADVANCE DIRECTIVES (AD) TERMINATION OF MCS Who this is based on Research study , 1 US hospital 16 men, 3 women; aged 55-78 years (median All DT patients were offered a standardized, integrated PC 70.9); all HM II and all DT patients consultation for “advance care planning” in 2009-2010, All patients NYHA class IIIb/IV; average duration before implantation or shortly afterwards of heart failure: 5.9 years Medical charts of all DT patients were reviewed 17 Research study18, 1 US hospital Medical charts of all MCS recipients from 2003-2009 were reviewed (before start of PC consultation service) 56 men, 12 women; average age 59 years; mostly Caucasian, some college education, married 33 DT and 32 transplant-eligible patients; 3 implanted as bridge-to-recovery; 78% of devices continuous flow, otherwise pulsatile Research study19, 1 US hospital Medical charts of the first 20 patients who received a PC consultation in 2009-2010 were reviewed; patients/families asked about the impact of the PC consultation service 18 men, 2 women; aged 19-83 years (average 54) 4 DT patients Most patients required transient inotropic support Research study20, 1 US hospital Medical charts of all recipients who had MCS terminated from 2003-2009 were reviewed 13 men, 1 woman; aged 41-68 years (median 57); length of support 1 day to 2.8 years (median 64 days); 7 DT patients (all men; 48-68 years; 2 with CF device; 16 days to 2.8 years of support) Utah Artificial Heart Program registry21: all DT patients DT patients: 18 men, 2 women; aged 23-82 years (1999-2009) actively participating in end-of-life decisions (average 67); 2.5 months to 4.8 years of support Primary informal caregiver interviewed in person within 2 (pulsatile devices) weeks of patient’s death; asked what events prompted Caregivers were mostly spouses; 2 were adult decision to withdraw MCS; how end-of-life decision was children; 1 was a parent reached; if adequate assistance was provided at end of life HM II: HeartMate II®; MCS: mechanical circulatory support; US: United States; DT: destination therapy; PC: palliative care; AD: advance directives; CF: continuous flow 7 REFERENCES 1. Kirklin JK, Naftel DC, Pagani FD, Kormos RL, Stevenson L, Miller M, Young JB. Long-term mechanical circulatory support (destination therapy): on track to compete with heart transplantation? J Thorac Cardiovasc Surg 2012;144:584-603. 2. Park SJ, Milano CA, Tatooles AJ, Rogers JG, Adamson RM, Steidley DE, Ewald GA, Sundareswaran KS, Farrar DJ, Slaughter MS; HeartMate II Clinical Investigators. Outcomes in advanced heart failure patients with left ventricular assist devices for destination therapy. Circ Heart Fail 2012;5:241-8. 3. Kirklin JK, Naftel DC, Kormos RL, Stevenson LW, Pagani FD, Miller MA, Timothy Baldwin J, Young JB. Fifth INTERMACS annual report: risk factor analysis from more than 6,000 mechanical circulatory support patients. J Heart Lung Transplant 2013;32:141-56. 4. Slaughter MS, Rogers JG, Milano CA, Russell SD, Conte JV, Feldman D, Sun B, Tatooles AJ, Delgado RM 3rd, Long JW, Wozniak TC, Ghumman W, Farrar DJ, Frazier OH; HeartMate II Investigators. Advanced heart failure treated with continuous-flow left ventricular assist device. N Engl J Med 2009;361:2241-51. 5. Rogers JG, Aaronson KD, Boyle AJ, Russell SD, Milano CA, Pagani FD, Edwards BS, Park S, John R, Conte JV, Farrar DJ, Slaughter MS; HeartMate II Investigators. Continuous flow left ventricular assist device improves functional capacity and quality of life of advanced heart failure patients. J Am Coll Cardiol 2010;55:1826-34. 6. Petrucci RJ, Rogers JG, Blue L, Gallagher C, Russell SD, Dordunoo D, Jaski BE, Chillcott S, Sun B, Yanssens TL, Tatooles A, Koundakjian L, Farrar DJ, Slaughter MS. Neurocognitive function in destination therapy patients receiving continuous-flow vs pulsatile-flow left ventricular assist device support. J Heart Lung Transplant 2012;31:27-36. 7. Hasin T, Marmor Y, Kremers W, Topilsky Y, Severson CJ, Schirger JA, Boilson BA, Clavell AL, Rodeheffer RJ, Frantz RP, Edwards BS, Pereira NL, Stulak JM, Joyce L, Daly R, Park SJ, Kushwaha SS. Readmissions after implantation of axial flow left ventricular assist device. J Am Coll Cardiol 2013;61:153-63. 8. Pagani FD, Miller LW, Russell SD, Aaronson KD, John R, Boyle AJ, Conte JV, Bogaev RC, MacGillivray TE, Naka Y, Mancini D, Massey HT, Chen L, Klodell CT,Aranda JM, Moazami N, Ewald GA, Farrar DJ, Frazier OH; HeartMate II Investigators. Extended mechanical circulatory support with a continuous-flow rotary left ventricular assist device. J Am Coll Cardiol 2009;54:312-21. 8 9. Starling RC, Naka Y, Boyle AJ, Gonzalez-Stawinski G, John R, Jorde U, Russell SD, Conte JV, Aaronson KD, McGee EC Jr, Cotts WG, DeNofrio D, Pham DT, Farrar DJ, Pagani FD. Results of the post-U.S. Food and Drug Administration-approval study with a continuous flow left ventricular assist device as a bridge to heart transplantation: a prospective study using the INTERMACS (Interagency Registry for Mechanically Assisted Circulatory Support). J Am Coll Cardiol 2011;57:1890-8. 10. Casida JM, Marcuccilli L, Peters RM, Wright S. Lifestyle adjustments of adults with long-term implantable left ventricular assist devices: a phenomenologic inquiry. Heart Lung 2011;40:511-20. 11. Zambroski CH, Combs P, Cronin SN, Pfeffer C. Edgar Allan Poe, “The pit and the pendulum,” and ventricular assist devices. Crit Care Nurse 2009;29:29-39. 12. Marcuccilli L, Casida JM. From insiders’ perspectives: adjusting to caregiving for patients with left ventricular assist devices. Prog Transplant 2011;21:137-43. 13. Casida JM, Davis JE, Brewer RJ, Smith C, Yarandi H. Sleep and daytime sleepiness of patients with left ventricular assist devices: a longitudinal pilot study. Prog Transplant 2011;21:131-6. 14. Casida JM, Brewer RJ, Smith C, Davis JE. An exploratory study of sleep quality, daytime function, and quality of life in patients with mechanical circulatory support. Int J Artif Organs 2012;35:531-7. 15. Marcuccilli L, Casida JJ, Peters RM, Wright S. Sex and intimacy among patients with implantable left-ventricular assist devices. J Cardiovasc Nurs 2011;26:504-11. 16. Heilmann C, Kuijpers N, Beyersdorf F, Berchtold-Herz M, Trummer G, Stroh AL, Schlensak C, Fritzsche K. Supportive psychotherapy for patients with heart transplantation or ventricular assist devices. Eur J Cardiothorac Surg 2011;39:e44-50. 17. Swetz KM, Freeman MR, AbouEzzeddine OF, Carter KA, Boilson BA, Ottenberg AL, Park SJ, Mueller PS. Palliative medicine consultation for preparedness planning in patients receiving left ventricular assist devices as destination therapy. Mayo Clin Proc 2011;86:493-500. 18. Swetz KM, Mueller PS, Ottenberg AL, Dib C, Freeman MR, Sulmasy DP. The use of advance directives among patients with left ventricular assist devices. Hosp Pract (Minneap) 2011;39:78-84. 9 19. Schwarz ER, Baraghoush A, Morrissey RP, Shah AB, Shinde AM, Phan A, Bharadwaj P. Pilot study of palliative care consultation in patients with advanced heart failure referred for cardiac transplantation. J Palliat Med 2012;15:12-5. 20. Mueller PS, Swetz KM, Freeman MR, Carter KA, Crowley ME, Anderson Severson CJ, Park SJ, Sulmasy DP. Ethical analysis of withdrawing ventricular assist device support. Mayo Clin Proc 2010;85:791-7. 21. Brush S, Budge D, Alharethi R, McCormick AJ, MacPherson JE, Reid BB, Ledford ID, Smith HK, Stoker S, Clayson SE, Doty JR, Caine WT, Drakos S, Kfoury AG. End-of-life decision making and implementation in recipients of a destination left ventricular assist device. J Heart Lung Transplant 2010;29:1337-41. 10