Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
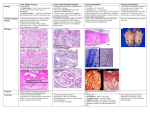
Renal Pathophysiology: Tubulointerstitial Diseases (Zeng) ACUTE RENAL FAILURE: Definition of Acute Renal Failure: Acute and rapid decline in renal function characterized by: o Azotemia o Oliguria (<400ml urine/day; often earliest sign of impaired renal function) o Increased ECF volume o Hyperkalemia o Metabolic acidosis May be due to processes affecting ANY compartment of the kidney Development of Acute Renal Failure: Outside the Hospital: minority of cases* o Evaluation of the following immediately: Hyperkalemia Metabolic acidosis Pulmonary edema Edema/ascites o Usually a SINGLE cause o Good prognosis Inside the Hospital: most cases* o Common causes: Hypovolemia Effects of anesthesia or surgery Diuretics Nephrotoxic drugs Contrast media o Multiple renal insults, often leading to SEVERE failure o Prognosis not as good Principal Causes of Acute Renal Failure: Pre-Renal Causes: due to HYPOPERFUSION of the kidney o Absolute decrease in effective blood volume: Hemorrhage (trauma, surgery) GI fluid loss (diarrhea, vomiting, NG suction) Renal losses (diuretics, glycosuria) o Relative decrease in peripheral vascular resistance: Sepsis Anaphylaxis Shock o Reduced cardiac output MI Pulmonary embolism CHF o Local renal vasoconstriction Post-Renal Causes: due to OBSTRUCTION of urine flow (obstructive uropathy) o Upper Urinary Tract Obstruction: ureteral obstruction of one or both kidneys Tumor Fibrosis o Lower Urinary Tract Obstruction: bladder outlet obstruction (more common) Prostatic hypertrophy Renal (Intrinsic) Causes: processes affecting any of the renal compartments o Glomerular causes: Crescentic Glomerulonephritis o Vasculature causes o Interstitial/Tubular Causes: Acute Tubulo-Interstitial Nephritis (related to drugs, infections, or cancer) Acute Tubular Necrosis (due to ischemia or toxicities) ACUTE TUBULAR NECROSIS: Basics: results from the injury and/or destruction of the RENAL TUBULAR EPITHELIUM May be responsible for ¾ of cases of acute renal failure Causes (2 Categories): Ischemic Injury: due to inadequate blood flow to the kidneys (usually secondary to a pre-renal cause) o Shock/hypotension from sepsis o Massive burns o Major surgery or hemorrhage Tubulo-Toxic Injury: introduction of a substance that is toxic to tubular cells o Nephrotoxic drugs (ie. aminoglycoside Abx such as gentamycin) o Solvents o Heavy metals (ie. mercury) o Pigments (ie. diagnostic radiocontrast dyes) Result- Injury to Tubular Epithelial Cells: Features: o Impaired synthetic functions (cells cannot make ATP or proteins) o Decreased high energy phosphate stores (not making ATP) o Activation of destructive lysosomal processes Important Point: although the name suggests death of the tubular cells, this is RARELY the case* o Cells may become injured and lose most functions without actually becoming necrotic o However, actual necrosis MAY occur if insult is severe Regeneration of necrotic cells is possible if basement membrane is intact Insult must be removed and patient must be supported for regeneration to occur Pathology of Acute Tubular Necrosis: Basics: pathological changes vary based on severity of insult and when biopsy is done Mild Cases: o Loss of tubule cell brush border (cell injury) o Vacuolization of cytoplasm o Swelling of cells Severe Cases: o Necrosis of cells slough off into tubular lumen o Bare basement membranes Changes of Recovery: seen when biopsy is done after patient recovery has begun* o Flattened epithelial cells (as they attempt to re-cover basement membranes) o Mitotic figures o Reactive nuclei with large nucleoli Reduction in GFR: Mechanisms for GFR Reduction in ATN: o Vasoconstriction: ischemic injury/nephrotoxin may also lead to vasoconstriction (in addition to direct tubular damage) o Obstruction of Tubules by Necrotic Cells (Casts): causes increased tubular pressure and decreased filtration o Backleak of Filtered Urine: leaks through damaged tubules back into kidney vasculature and interstitium ACUTE TUBULO-INTERSTITIAL NEPHRITIS: Basics: inflammation of the interstitium of the kidney, which also affects the tubules Immunologic Phenomenon: Patients have a history or evidence of hypersensitivity Immune complexes may be present in tubular basement membranes Anti-tubular basement membrane Abs may be found in some patients T cell mediated damage (type IV hypersensitivity) has been shown to occur* o Likely the explanation in MOST cases Causes: Drug Reaction: most common cause* o Mechanism: drug acts as a hapten to elicit the immune response o Common Drugs: Beta-lactam antibiotics (ie. penicillin, methicillin, ampicillin) Sulfonamides (ie. Bactrim) NSAIDs (ie. Motrin) Diuretics (only some) Systemic Infections: o Mechanism: antigens are deposited in the tubulo-interstitium, eliciting the response Note: condition is NOT due to the direct infectious nature of the organisms themselves* o Common Infectious Agents: Group A strep Diphtheria Toxoplasmosis Legionnaire’s disease (Legionella) Systemic Illnesses: SLE Pathology: Tubules separated by pronounced edema Inflammatory infiltrate (lymphocytes, monocytes, eosinophils, neutrophils) o Lymphocytes may be noted “percolating” through the tubular epithelium Clinical Features: features of HYPERSENSITIVITY* Fever Hematuria Eosinophilia Pyuria Skin rash Mild proteinuria Eosinophiluria INFECTION OF THE KIDNEY- ACUTE PYELONEPHRITIS: Basic Definitions: Urinary Tract Infection: general term that implies a patient has a bacterial/viral/fungal infection at any point in the urinary tract (from urethra to kidney) o Generally used to describe LOWER UTIs o Most common cause of acute pyelonephritis Acute Pyelonephritis: actual infection of the renal parenchyma o Usually associate with a UTI Causative Organisms: the organisms that cause UTI/AP are the same as the one’s found in the patient’s own gut o E.coli o Klebsiella o Proteus o Enterococcus o Enterobacter o Other infections in special scenarios: Candida albicans (immunosuppressed patients and diabetics) CMV (transplant and other immunosuppressed patients) Route of Infections in Acute Pyelonephritis: Hematogenous Infection (5%): o Bacteremia in septic patients o Infected emboli (endocarditis) Ascending Infection (95%): o Pre-existing UTI that ascends (urethra bladder ureter renal pelvis kidney) Risk Factors for Ascending Infections: Obstruction of urine flow: may occur at ANY level o Urethral/ureteral stricture o Functional bladder obstruction with incomplete emptying (neurogenic bladder of DM) o Prostatic hypertrophy (urethral obstruction) Vesicoureteral reflex: covered later Instrumentation of the GU tract: catheters, diagnostic procedures Pregnancy: uterus obstructs one or both ureters Age and sex: covered later Immune dysfunction: AIDS, diabetes, steroids Risk Factors for UTIs (May Lead to Acute Pyelonephritis): Age and Sex VERY IMPORTANT: o <1 year old: male infants more likely (congenital anomalies more common- urethral/ureteral valves) o 1-50 years old: females much more likely (8:1) Shorter urethra (less distance for migration) Lack of antibacterial prostatic secretions (men) Hormonal influences Trauma during sexual intercourse (“honeymoon cystitis”) o >50 years old: men more likely Secondary to prostatic hypertrophy Vesico-Ureteral Reflux: o Process: reflux of urine from the bladder to the ureters If urine infected, the infected column of urine makes its way to the renal pelvis and parenchyma o Cause: interference with the functional sphincter that normally closes off the ureters with contraction of the bladder (ureters normally enters the wall at an angle) Absence of the intravesicular ureter (ureter enters perpendicular to the bladder wall) Congenital para-ureteral diverticulum (interferes with normal function) Inflammation of bladder wall Pathology of Acute Pyelonephritis: Gross: o Outer kidney has pinpoint pustules that may become confluent in severe cases o Inner kidney shows streaks of yellow pus extending from renal pyramids into the cortex (streaks of infected tubules) Microscopic: o Intense neutrophilic interstitial AND tubular infiltrate o Marked tubular destruction o Glomeruli relatively unaffected (early in disease) Complications of Acute Pyelonephritis: Pyonephrosis: infection so severe that the kidney is transformed into a “bag of pus” Perinephric Abscess: infection breaks through the renal capsule and infection spreads to perinephric soft tissue Necrotizing Papillitis (Papillary Necrosis): necrosis of the renal papillae; slough off into the renal pelvis and cause further destruction o Requirements: papillary necrosis requires 3 elements to be present in order to occur* Acute pyelonephritis (infection) Obstruction to urinary flow Compromised blood flow Severe arteriolosclerosis (ie. diabetics) Clogging of vasa recta (ie. sickle cell anemia) o Gross Appearance: coagulation necrosis with sharply demarcated edges undergoing inflammation INFECTION OF THE KIDNEY- CHRONIC PYELONEPHRITIS: Basics: represents recurrent, repeated bouts on acute pyelonephritis Causes SEVERE SCARRING of the renal parenchyma, calyces and pelvis Common Associations: Patients with chronic urine reflux and numerous episodes of UTIs (most common)* Patients with vesico-ureteral reflex Patients with intrarenal reflux Patients with acute pyelonephritis Pathology: Gross: o Scarred and asymmetric kidneys o Pelvis and calyces are markedly thickened and scarred o Cortex thinned by numerous broad cortical scars Microscopic: NON-SPECIFIC (requires GROSS diagnosis); all components of the kidney are affected o Glomerulosclerosis o Interstitial fibrosis o Tubular atrophy