Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
HCM (Evaluation)
PREVALENCE
1.
The prevalence of HCM in general population, as determined from echocardiographic studies
in the United States, Japan, and China, is approximately 1 out of every 500 adults (0.2%).
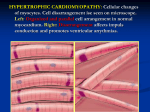
HISTOLOGIC FINDING
1. Histopathology in patients with HCM reveals hypertrophied myocytes arranged in chaotic and
disorganized fashion with varying amount of interstitial fibrosis intertwined among myocyte.
In addition, intramural coronary arterioles are structurally abnormal with decreased luminal
cross-sectional area and impaired vasodilatory capacity resulting in blunted myocardial blood
flow during stress ("small vessel ischemia"). Over time, repetitive bouts of small vessel
ischemia lead to myocyte cell death and ultimately repair in form of replacement fibrosis.
CLINICAL MANIFESTATION
1. Many patients with HCM have no or only minor symptoms; thus, affected individuals are
often diagnosed as result of family screening, detection of murmur during routine
examination, or identification of abnormal ECG. However, among those who come to clinical
attention at referral centers, LVOT gradients and symptoms of dyspnea, fatigue, chest pain,
and syncope are the most common clinical manifestations. Patients with mild to moderate
limitation usually experience slow progression of symptoms with advancing age in association
with modest deterioration in left ventricular function.
2. Sign and symptom
A. S/S of HCM is variable, and there is not strong correlation between presence of LVOTO,
extent of LVH, and symptoms. Some patients with severe LVOTO remain asymptomatic
for many years, while others without LVOTO may have significant limitation.
B. While many patients with HCM are asymptomatic, others develop one or more of the
following symptoms.
i.
Dyspnea on exertion
ii.
Fatigue
iii.
Atypical or anginal chest pain
iv.
Presyncope and syncope, particularly during or immediately following exertion
v.
Palpitation
C.
Advanced heart failure symptoms of orthopnea, paroxysmal nocturnal dyspnea, and
edema are uncommon. The frequency of symptoms at diagnosis varies considerably
depending on whether population being studied is cross section of overall population or
patients at referral center.
D. In series of 320 patients from 3 referral centers, TTE was performed in all patients, with
subsequent stress UCG only in those whose LVOT gradient was < 50 mmHg at rest. The
following findings were noted.
i.
169 patients (59%) had NYHA Class II or greater dyspnea at presentation.
ii.
119 patients (37%) had resting LVOT gradient ≥ 50 mmHg, while 201 patients (63%)
had resting LVOT gradient < 50 mmHg (mean 4 mmHg). With exercise, 76 (24%)
developed LVOT gradient ≥ 50 mmHg, and 46 (14%) developed DOE.
iii.
E.
F.
G.
H.
I.
95 patients (30%) were asymptomatic with little or no gradient (≤ 30 mmHg) at rest
or with exertion.
In study of 277 outpatients from regional cohort (non-referral population) who were
followed for eight years, 90% were asymptomatic at presentation. During 8-year
follow-up, 69% remained asymptomatic or had only mild symptoms, and survival in
adults was similar to normal control age-matched population.
Thus, among patients referred for evaluation of HCM, both HF symptoms and outflow
gradients are common, although in many cases exercise testing may be necessary to
demonstrate these abnormalities.
The clinical presentation also may be affected by gender. In review of 969 consecutive
patients from the US and Italy, women were significantly older at presentation than
men (47 vs. 38 years), more symptomatic (NYHA class 1.8 vs. 1.4), and more likely to
have LVOTO (37 vs. 23%). At mean follow-up of 6.2 years, women had significantly
higher rates of progression to NYHA class III or IV and death from heart failure or stroke.
Symptoms can be induced by variety of mechanisms which may include LVOTO, impaired
myocardial function, brady- or tachyarrhythmias, or impaired filling due to diastolic
dysfunction. The importance of these mechanisms may change with time and stage of
disease. Some patients, for example, are initially symptomatic because of obstruction. As
myocardial disease worsens over time, heart may enlarge, obstruction lessens, and
symptoms are primarily due to systolic and/or diastolic dysfunction.
Relationship of symptom to age
i.
The age of patient at diagnosis and presence or absence of symptoms provide
important prognostic information. In general, patients diagnosed during childhood
or adolescence have more symptoms and poorer prognosis compared with those
diagnosed as adults.
J.
Relationship of symptom to pressure gradient
i.
A pressure gradient between LVOT and aorta is present in majority of HCM (75%),
either at rest or following provocation. Outflow tract gradients in HCM are dynamic,
characterized by spontaneous variability on day-to-day (or even hourly) basis, and
influenced by factors that alter myocardial contractility and loading conditions
(dehydration, ingestion of alcohol, or heavy meals). As such, for patients who do
not have evidence of LVOTO under resting conditions, attempt should be made at
provoking gradients as presence of LVOTO will affect management decisions.
Exercise (stress) UCG using standard symptom limited Bruce protocol is preferred
method as this mimics most closely conditions that patients would be experiencing
provocable gradients with daily activities. Alternatively, pharmacologic agents (amyl
nitrite, dobutamine, isoproterenol) and Valsalva maneuver can also be employed to
induce gradients, although these are non-physiologic maneuvers that may not
reflect true magnitude of outflow gradients experienced during daily activities.
ii.
However, despite presence of LVOTO, there is not predictable correlation between
degree of LVOTO and symptom. Some patients with severe LVOTO remain
asymptomatic for many years; at the other extreme, cardiac arrest or SCD may be
the initial presentation in those with or without obstruction.
K. Dyspnea
i.
DOE is the most common symptom in persons with HCM, occurring in over 90% of
symptomatic patients. Dyspnea can result from variety of mechanisms.
1. Diastolic dysfunction due to myocardial hypertrophy
2. Impaired left ventricular emptying due to LVOTO, resulting in increased LVEDP
3. Mitral regurgitation
4. Systolic dysfunction in patient with more extensive myocardial involvement
ii.
Paroxysmal nocturnal dyspnea and orthopnea are uncommon presentation.
L.
Chest pain
i.
Typical exertional chest pain (angina) occurs in 25 to 30% of patients with HCM,
ii.
usually in setting of normal coronary arteriogram. Some patients also complain of
prolonged episodes of atypical chest pain. This chest pain is commonly precipitated
or worsened by heavy meals.
Several of pathophysiologic features of HCM predispose to development of
microvascular angina, which may be induced by increase in myocardial oxygen
demand or reduction in myocardial blood flow and oxygen supply. Factors that
increase myocardial oxygen demand include myocyte hypertrophy and increased
muscle mass, myocyte disarray, LVOTO, and increased wall stress due to elevated
diastolic pressures. Factors that reduce myocardial blood flow in HCM, particularly
with exertion, include impaired vasodilator reserve, myocardial bridging with
systolic and early diastolic compression of intramural vessels, small vessel disease
and microvascular dysfunction, myocardial fibrosis, and increased capillary
separation and inadequate capillary density.
iii.
Many studies have shown that, during pacing or pharmacologic stress, myocardial
blood flow is abnormal in patients with HCM and often associated with metabolic
evidence for myocardial ischemia. Myocardial perfusion in patients with HCM can
be assessed using exercise or pharmacologic stress testing.
M. Arrhythmia
i.
Both supraventricular arrhythmias, primarily Afib, and ventricular arrhythmias
occur in HCM. Patients with arrhythmia may present with palpitations, increasing
dyspnea, presyncope, or syncope, with occasional patients presenting with SCD due
to sustained ventricular arrhythmias.
ii.
The arrhythmias associated with HCM, as well as their treatment, are discussed
separately.
N. Syncope
i.
Approximately 15 to 25% of patients with HCM report at least one syncopal episode.
Another 20% complain of presyncope. Multiple mechanisms may lead to
inadequate cardiac output or abnormal peripheral vascular reflexes.
1. Atrial fibrillation
ii.
2. Conduction abnormalities and AVB
3. LVOTO
4. Ventricular baroreflex activation with inappropriate vasodilatation
5. Myocardial ischemia during exertion
Among the reported predictors of syncope in patients with HCM.
1. Age < 30 years
2. Small LVEDV and small LV cavity size (irrespective of obstruction and
hypertrophy)
3. Episodes of non-sustained VT on 72-hour ambulatory ECG monitoring
iii.
3.
Unexplained syncope (not related to neurocardiogenic/vasovagal causes) is
considered marker for increased risk of SCD, particularly when recent and when
occurring in young patient.
Physical examination
A. PE in patient with HCM may be normal or may reveal nonspecific abnormalities such as
fourth heart sound, systolic murmur, and/or left ventricular lift. Many of classically
described PE findings in patients with HCM are associated with LVOTO. Persons with
minimal or no LVOTO may have normal or nearly normal physical examination.
B. Systolic murmur
i.
Significant LVOTO, often due to combination of LV upper septal hypertrophy and
SAM, results in harsh crescendo-decrescendo systolic murmur that begins slightly
ii.
iii.
iv.
v.
vi.
after S1 and is heard best at apex and LLSB. The murmur may radiate to axilla and
base, but usually not into neck. It may reflect both aortic outflow obstruction and
MR in patients with large gradient.
SAM can lead to impaired leaflet coaptation and MR, usually with posteriorly
directed jet, which produces mid-late systolic murmur at apex. Centrally directed
MR, usually associated with primary mitral valve pathology, classically results in
holosystolic murmur heard loudest at apex which radiates to axilla. However, if
regurgitant jet is eccentrically directed, murmur can radiate toward base of heart
and may be confused with murmur of LVOTO.
The systolic murmur related to LVOTO in HCM is often similar to that of valvular AS
and subvalvular AS, and differentiating these conditions is difficult on routine
auscultation. However, patient can be asked to perform series of maneuvers and
position changes which can aid in making correct diagnosis. Maneuvers that affect
degree of LVOTO cause change in intensity of outflow tract crescendo-decrescendo
murmur (table 2).
An increase in intensity, due to enhancement of obstruction, is seen with the
assumption of upright posture from squatting, sitting, or supine position; Valsalva
maneuver; during more forceful contraction that follows compensatory pause after
VPC; and following administration of nitroglycerin.
A decrease in intensity, due to attenuation of obstruction, is heard after going from
standing to sitting or squatting, with handgrip, and following passive elevation of
legs.
The murmur in AS does not change substantially, or decreases slightly following the
Valsalva maneuver and usually radiates into neck, while murmur in subaortic
stenosis (most commonly seen in children) tends to decrease following Valsalva
maneuver.
C.
Other physical finding
i.
The first heart sound is typically normal. In patients without severe obstruction, the
ii.
iii.
iv.
v.
vi.
second heart sound splits normally; however, split may be paradoxic if there is
severe LVOTO.
S3 or S4 is common in young patients but rarely heard in later life.
The arterial or carotid pulse may be brisk in upstroke and bifid; this results from
sudden deceleration of blood due to development of mid-systolic obstruction to
blood flow and partial closure of aortic valve.
Inspection of neck veins may reveal prominent "a" wave.
There is often diffuse, forceful LV apical impulse.
A presystolic apical impulse may be felt, reflecting atrial systole.
vii.
A systolic thrill may be appreciated at apex or LLSB.
viii.
A parasternal lift suggests significant MR and/or pulmonary HTN.
DIAGNOSTIC EVALUATION
1. A variety of tests have been used in evaluation of patients with possible HCM. Appropriate
testing as indicated when diagnosis of HCM is being considered, or when suggestive clinical
signs or symptoms are present.
A. To establish diagnosis of HCM
B. To identify presence or severity of LVOTO
C. To identify presence or severity of MR
D. To assess risk for arrhythmia (both supraventricular and ventricular)
2.
3.
4.
E. To assess overall left ventricular function
In addition to performing comprehensive cardiac history and physical examination and ECG,
cardiac imaging to identify LVH should be performed in all patients. Typically, presence or
absence of LVH can be satisfactorily identified using UCG, although another imaging modality
such as CMR may be necessary in persons with non-diagnostic or suboptimal quality UCG
In persons with ECG and echocardiographic (or CMR) evidence of HCM, ambulatory ECG
monitoring and exercise stress testing should be performed for additional prognostic
information and risk stratification purposes. Additional testing may not be necessary in
asymptomatic or mildly symptomatic patient; such patients may be discovered because of
positive family history or abnormal ECG obtained for some other reason. In contrast, more
thorough and detailed evaluation is necessary for symptoms such as syncope, or prior to and
following surgical myectomy or septal ablation.
Electrocardiography
A. ECG should be performed in all patients when considering diagnosis of HCM. ECG is the
most sensitive routinely performed diagnostic test for HCM, but ECG abnormalities are
not specific to HCM and should prompt further diagnostic evaluation, usually with UCG.
B. A normal ECG is uncommon, seen in < 10% of patients with HCM. In cohort of 2485
consecutive patients with HCM who were evaluated at single center, normal ECG was
seen in only 135 patients (5%).
C.
Typically, ECG is abnormal with localized or widespread repolarization changes.
Prominent voltages with repolarization changes are typical of HCM associated with
storage disease (Danon's disease), while prominent voltages in isolation are rare as an
ECG manifestation in HCM.
i.
ii.
iii.
iv.
5.
Prominent abnormal Q waves, particularly in the inferior (II, III, and aVF) and lateral
leads (I, aVL, and V4-V6). These changes reflect septal depolarization of the
hypertrophied myopathic tissue.
P wave abnormalities, reflecting LAE. The combination of LVH with RAE is strongly
suggestive of HCM.
Left axis deviation.
Deeply inverted T waves (so-called "giant negative T waves") may be seen in the
mid-precordial leads (V2 through V4) in patients with apical variant of HCM.
Echocardiography
A. Comprehensive TTE with two-dimensional, color Doppler, spectral Doppler, and tissue
Doppler imaging should be performed in all patients when considering diagnosis of HCM.
TTE can demonstrate cardiac morphology, systolic and diastolic function, presence and
severity of any LVOT gradient, and degree of MR.
B.
LV hypertrophy
i.
A clinical diagnosis of HCM is confirmed when unexplained increased LV wall
thickness ≥ 15 mm is imaged anywhere in LV wall. A wall thickness of ≥ 13 mm may
also be considered diagnostic of HCM, particularly when identified in patient whose
family member also has HCM. The most common location for LVH is basal anterior
septum in continuity with anterior free wall, with posterior septum (at mid-LV level)
the third most common location. Although LVH often involves substantial portion of
LV wall, important minority of HCM patients (10%) have increased wall thickness
confined to only 1 or 2 LV segments. Although typically asymmetric in distribution,
any pattern of LV wall thickening can be seen in HCM, including apical and
concentric LV hypertrophy in small minority (1%).
ii.
The distribution of LVH on UCG is assessed in variety of views but primarily in
parasternal short-axis plane. The presence and extent of LVH is evaluated in
diastole at level of mitral valve and papillary muscle. Parasternal long-axis, and
apical 2- and 4-chamber views are also used to integrate the information obtained
from short-axis image.
C. Systolic anterior motion of the mitral valve
i.
Patients with HCM frequently have SAM, which positions mitral valve within LVOT.
SAM of mitral valve may result in LVOTO when there is contact between mitral
valve and septum. The greater the duration of mitral-septal contact, the higher the
LVOTO. The presence of SAM is not requirement for diagnosis of HCM.
D.
LVOT obstruction
i.
UCG can be used to accurately measure non-invasively presence and magnitude of
LV outflow gradients using continuous-wave Doppler techniques. The apical
long-axis imaging window provides the best views to obtain Doppler estimates of
LVOT pressure gradient, and particular care must be taken to separate LVOT signals
from those due to MR. The aortic valve motion may display early-systolic closure
and "peak and dome" configuration of aortic pressure and velocity, which
corresponds to transient mid systolic obstruction and reduction in stroke volume.
ii.
Outflow tract gradients in HCM are dynamic, characterized by spontaneous
variability on day-to-day (or even hourly) basis, and are influenced by factors that
alter myocardial contractility and loading conditions (dehydration, ingestion of
alcohol, or heavy meals). Therefore, for patients who do not have obstruction
under resting conditions, provoking gradients for the purpose of management
decisions is crucial. Exercise (stress) UCG using standard symptom limited Bruce
protocol is the preferred method as this mimics most closely conditions that
patients would be experiencing on a daily basis. Alternatively, medication (amyl
nitrite, dobutamine, isoproterenol) and Valsalva can also been employed to induce
gradients, although these are non-physiologic maneuvers which may not reflect
true magnitude of outflow gradients experienced during routine daily activities.
iii.
iv.
6.
7.
A pressure gradient between LVOT and aorta is present in majority of patient with
HCM (75%) at rest or with provocation. As example, in cohort of 201 patients with
HCM and no resting LVOT gradient who underwent exercise testing, 106 (53%)
developed LVOT gradients ≥ 30 mmHg, including 76 of whom developed gradients ≥
50 mmHg. These findings suggest that patients with symptomatic HCM without
LVOTO at rest should undergo exercise UCG to assess for potential latent
obstruction since identification of such obstruction would provide therapeutic
target and may prompt more aggressive medical therapy and consideration of
septal reduction therapy.
While the vast majority of patients with HCM exhibit increase or no change in LVOT
gradient with exercise, paradoxical decrease in LVOT gradient following exercise has
been reported in small cohort of patients with HCM. The exact mechanism and
clinical implications of this paradoxical decrease in LVOT gradient following exercise
are not known.
Ambulatory ECG monitoring
A. Ambulatory ECG monitoring should be performed for 24 to 48 hours in all patients
diagnosed with HCM (based on clinical and imaging findings) as part of risk assessment
for ventricular arrhythmias and risk for sudden death. In addition, in patients with
palpitations in whom the etiology is uncertain or if there is suspicion for atrial
fibrillation/flutter, ambulatory monitoring should also be considered.
B. Ambulatory ECG monitoring and continuous loop recorders can identify non-sustained
atrial and ventricular arrhythmias in patients with HCM and help to establish whether
arrhythmia is cause of palpitation or impaired consciousness. Non-sustained VT on
Holter monitoring is associated with increased risk for SCD, even in asymptomatic
patient.
Exercise testing
A. We proceed with exercise stress testing in all patients with known or suspected HCM
(based on clinical and imaging findings) as part of risk stratification (abnormal BP
response to exercise) and for assessment of LVOT gradient. Exercise treadmill testing is
preferred method of stress, rather than using pharmacologic stress agent, as maximal
treadmill or bicycle exercise stress test provides objective measurement of functional
capacity and information on integrity of vascular responses and risk of exercise related
ischemia, arrhythmia, and obstruction. In addition, results of exercise stress testing may
lead to change in patient management (inducible ventricular arrhythmias or inducible
LVOT gradient). The decision to add imaging modality such as UCG or myocardial
perfusion imaging to stress test should be based on usual indications for imaging during
stress testing (baseline ECG is uninterpretable). However, for assessment of LVOT
gradients, echocardiographic imaging should be performed in conjunction with the
stress test.
B.
Whenever feasible, initial exercise testing should be performed prior to institution of
therapy, although follow-up exercise testing on treatment may be indicated to assess
efficacy of particular treatment. During exercise, some patients, particularly those who
develop angina with marked ST segment changes, Afib, HoTN, or large (> 100 mmHg)
gradients, may be at risk of developing serious ventricular arrhythmia. However, the
incidence of sustained VT/VF during exercise testing appears to be very low.
C. Clinically important findings during exercise testing.
i.
Development of symptoms such as angina, dyspnea, palpitation, or presyncope
ii.
An increase in or development of LVOT gradient
iii.
Failure of BP to increase appropriately with exercise or exercise-induced HoTN
iv.
Clinically significant arrhythmias (Afib, VT) at maximum exercise or immediately
after exercise
v.
Severe STD during exercise may reflect myocardial ischemia, particularly if ST and T
of resting electrocardiogram are normal
vi.
An increase in, or development of, MR
D. Myocardial ischemia during exercise testing commonly occurs in absence of significant
CAD, and has been reported to be associated with future risk of adverse cardiac events.
The pathophysiology of myocardial ischemia is discussed in detail separately.
E. While majority of exercise testing with imaging will involve UCG or SPECT MPI, PET at
baseline and after infusion of coronary vasodilator dipyridamole is another method of
evaluating myocardial perfusion. The normal increase in myocardial blood flow in
response to dipyridamole is impaired in patients with HCM.
F. Cardiopulmonary exercise testing
i.
Cardiopulmonary exercise testing to assess between respiratory and circulatory
causes of exercise intolerance has no clear prognostic value and therefore is not
part of routine evaluation of HCM patients. However, cardiopulmonary exercise
testing may rarely be considered for those patients in whom etiology of dyspnea
remains uncertain.
ii.
Among the abnormalities that have been associated with HCM.
1. Reductions in peak oxygen uptake and anaerobic threshold, which are present
in most patients
2.
An impaired stroke volume response to exercise, which can be caused by
diastolic dysfunction, LVOTO, or systolic impairment
3. Chronotropic incompetence
G. BP response
i.
The normal blood pressure response to maximum upright exercise testing includes
at least 20 mmHg increase in systolic pressure from rest to peak exercise. However,
20 to 40% of patients with HCM fail to augment their baseline blood pressure
during exercise; in some of these patients, the blood pressure falls below baseline
values during or immediately following exercise.
ii.
8.
In most patients, abnormal exercise blood pressure is associated with appropriate
increase in CO and inappropriate peripheral vasodilatation. Occasionally, however,
abnormal BP response is due to failure to increase CO or development of global
myocardial ischemia or LVOTO.
iii.
The exact trigger for drop in BP during exercise is usually not known. However,
abnormal blood pressure response during maximal symptom-limited exercise test is
associated with an increased risk for SCD, particularly in patients < 40 years of age
and in those with family history of premature SCD.
Other tests
A. Cardiovascular magnetic resonance
i.
For assessment of anatomic structures, CMR may provide additional information
beyond that which is available from UCG. CMR may allow for identification of LVH
in segments not visualized well with UCG, better characterize structural
abnormalities of mitral valve and papillary muscles, and, when intravenous contrast
with gadolinium is used, allow for identification of myocardial fibrosis. We suggest
performing CMR for diagnostic purposes in selected patients in whom diagnosis of
HCM remains uncertain following UCG. It is reasonable to consider performing
CMR for additional risk stratification purposes in all patients with suspected or
diagnosed HCM if expense is not issue (as part of research protocol). In addition, in
patients with HCM being considered for invasive septal reduction therapy in whom
mitral valve and papillary muscle anatomy are not well defined with UCG, CMR can
ii.
be performed to clarify if patient is better suited for ASA or surgical myectomy.
CMR, with its high spatial resolution and tomographic imaging capability, has
emerged as technique particularly well suited to characterizing diverse phenotypic
expression of HCM. CMR can identify areas of segmental LVH (anterolateral wall or
apex) not reliably visualized by UCG (or underestimated in terms of extent). In study
of 48 patients with suspected or confirmed HCM diagnosis who underwent both
UCG and CMR, maximal LV thickness was similar with both techniques, but CMR
identified areas of thickening in anterolateral LV free wall in 3 patients (6%) in
whom UCG showed no areas of LVH, thereby making new diagnosis of HCM.
iii.
iv.
v.
vi.
vii.
In addition to its ability to identify additional regions of LVH not seen with UCG,
CMR is helpful in characterizing structural abnormalities of mitral valve
(elongation leaflets) and papillary muscles (accessory and apically displaced or
anomalous insertion into mitral valve leaflet) and can more precisely identify the
mechanisms responsible for LVOTO. Because of importance of mitral valve and
papillary muscle anatomy in patients with LVOTO who are being considered for
invasive septal reduction therapy, CMR should be performed as part of evaluation.
With intravenous injection of gadolinium, areas of hyper-enhancement (late
gadolinium enhancement [LGE]) representing myocardial fibrosis within
myocardium can be identified with contrast-enhanced CMR. The amount of LGE can
be quantified as percent of total LV mass. Approximately half of HCM patients
demonstrate LGE, with diverse pattern and location (not related to coronary
vascular distribution), although most commonly involving hypertrophied segments
of LV wall and at the junctions of ventricular septum and right ventricular free wall.
In prospective multicenter cohort of almost 1300 patients with HCM who
underwent quantitative contrast-CMR, extensive LGE was independent predictor
of sudden death, with ≥ 15% of LV mass conveying 2-fold increase in SCD risk, even
among those patients with HCM who do not have conventional SCD markers.
Observational studies have also suggested that patients with HCM and LGE were at
greater risk for ventricular tachyarrhythmias on ambulatory 24-hour Holter ECG
compared with those without LGE, suggesting that myocardial fibrosis may
represent structural nidus responsible for generation of potentially lethal reentry
ventricular tachyarrhythmia.
The independent predictive value of LGE in identifying patients with HCM who are
at risk for SCD is still debated among experts, and therefore management decisions
about ICD for primary prevention should not be made based solely on results of
CMR study. However, substantial LGE also has potential to resolve complex ICD
decision making, acting as arbitrator in selected patients for whom SCD risk remains
ambiguous even after standard risk stratification, while absence of LGE is associated
with lower risk for adverse events and may provide measure of reassurance to
patients. In addition, preliminary data suggest that prevalence and extent of late
gadolinium enhancement appears similar in children as adults and may also identify
young patients at increased risk for adverse disease-related events, although
additional studies are necessary to confirm these observation.
In addition to detecting LVH and myocardial fibrosis, CMR can provide additional
information in patients with HCM.
1. Identification and quantification of RVH
2. Evidence of microvascular dysfunction
3. Assessment of regional myocardial function
4. Assessment of diastolic function
B.
Cardiac catheterization
i.
We typically reserve hemodynamic assessment using cardiac catheterization for
patients with suspected HCM and one or more of the following situations.
1. Persons in whom additional diagnosis of RCMP or constrictive pericarditis is
being considered.
2. Persons in whom invasive coronary angiography is being performed for
evaluation of obstructive coronary disease.
3. Persons in whom suspicion for LVOTO is present but clinical and imaging data
are discrepant.
4. Persons in whom EMB is indicated to exclude non-sarcomeric disease (Fabry
disease, amyloidosis, Danon disease).
5. Pre-cardiac transplantation evaluation.
ii.
Cardiac catheterization is rarely required for diagnosis or clinical evaluation of HCM.
In most patients, UCG provides sufficient information regarding CO, LV filling
pressure or left atrial pressure, and LVOT pressure gradient such that cardiac
catheterization is not necessary.
C. Coronary angiography
i.
Coronary angiography should be performed in patients with apparent anginal chest
pain when knowledge of coronary anatomy may affect therapy or when cardiac
surgery is planned. Although epicardial coronary arteries are usually large and
normal in patients presenting with angina, CAD may coexist with HCM and must be
ruled out. In absence of obstructive epicardial CAD, angina may be due to regionally
impaired coronary flow and altered coronary flow reserve.
D. Genetic testing
i.
As of 2012, over 1400 mutations in 13 genes of cardiac sarcomere have been
associated with HCM. Due to this substantial genetic heterogeneity, clinic genetic
testing can identify disease-causing sarcomere protein mutation in substantially less
than half of patients with phenotype of HCM, and disease expression among
first-degree family members with HCM can be dramatically different. In addition,
identifying HCM patients at risk for adverse disease-related events including sudden
death cannot be predicted based on specific mutations, and specific HCM
ii.
phenotypes have diverse mutations associated with them, suggesting it is not
possible to predict phenotype based on specific mutation. As result, management
decisions such as ICD for primary prevention cannot be made solely based on
results derived from genetic testing.
For these reasons, routine genetic testing is not recommended for diagnostic
purposes, unless clinical evaluation raises suspicion for another genetic condition
known to cause LV hypertrophy (ie, Fabry disease, lysosomal storage diseases, etc.).
The role of genetic testing in assessing for family members at risk for developing
HCM is discussed in greater detail elsewhere.
E.
Electrophysiology study
i.
Syncope and presyncope in patients with HCM may be due to arrhythmias, LVOT
obstruction, or inappropriate vasodilatation despite adequate cardiac output.
However, invasive EP rarely identifies underlying mechanism and is not indicated to
determine need for ICD therapy for primary prevention of SCD.
F. Plasma BNP
i.
The range of values associated with plasma BNP and NT pro-BNP is quite broad and
does not correlate well with heart failure symptoms in patients with HCM. As result,
we do not order this test as part of diagnostic or prognostic evaluation of patients
with suspected HCM.
DIAGNOSIS
1.
2.
In individual patient, diagnosis of HCM may be suspected based on the following: family
history of HCM, unexplained symptoms (dyspnea, chest pain, fatigue, palpitations), systolic
ejection murmur, and abnormal 12-lead ECG or syncope (or presyncope). The presence of one
or more of these clinical findings may prompt further testing with UCG and/or CMR imaging
to confirm diagnosis. The presence of increased LV wall thickening ≥ 15 mm anywhere in LV
wall in absence of any other identifiable cause such as HTN or VHD is consistent with
diagnosis of HCM. Other common findings such as SAM or hyperdynamic LV are not obligatory
for HCM diagnosis.
Because of advances in non-invasive imaging, invasive assessments to make diagnosis of HCM
are rarely necessary. On occasion, however, invasive hemodynamic assessment using cardiac
catheterization may identify LVOT gradient which could not be confirmed using non-invasive
techniques and may be necessary to exclude CAD.
3. While presence of pathogenic sarcomeric mutation may be helpful for determining if family
members are at risk for developing HCM, genetic testing for HCM should not be performed
routinely for diagnostic purposes.
DIFFERENTIAL DIAGNOSIS
1. Differential diagnosis of LVH
A. In patient presenting with LVH, HCM must be distinguished from acquired causes of
cardiac hypertrophy. The most common causes are HTN and AS; in minority, HCM may
coexist with either.
B.
A rare cause of cardiac hypertrophy is Fabry disease, XR glycolipid storage disease.
Although classic multisystem Fabry disease is rare, isolated cardiac involvement may be
relatively common in patients with otherwise unexplained concentric LVH (up to 5%).
C. Hypertension
i.
Long-standing systemic HTN is the most common cause of LVH, particularly when it
has been untreated or incompletely treated. Most persons with HTN as cause of
LVH will be beyond adolescence, when HCM is most commonly identified. The
hypertrophy seen in HTN, however, rarely leads to wall thicknesses > 1.5 cm.
ii.
Additionally, HTN is usually suspected in persons with extended history of elevated
blood pressures (10 or more years), particularly in those with other evidence of
end-organ damage due to HTN (retinopathy, nephropathy).
D. Aortic stenosis
i.
Valvular AS due to stenosis of congenital bicuspid AV is more common in younger
persons (< 50 years of age), while in those > 50, valvular AS is typically due to
atherosclerotic narrowing of valve. In both situations, concentric LVH develops,
which is different than eccentric hypertrophy seen in HCM. Valvular AS can usually
be distinguished from other causes of LVH by UCG or invasive cardiac
catheterization, which allow for visualization of restricted leaflet motion.
ii.
Valvular AS also causes increased pressure gradient between LV and aorta.
E.
Athlete's heart
i.
Highly trained athletes can also develop cardiac hypertrophy (sometimes called
"athlete's heart"), resulting in wall thickness measurements in range that can
overlap with those seen in patients with HCM (wall thickness "grey zone" of 13 to
15 mm). As result, number of noninvasive measures has been proposed to help
differentiate athlete's heart from HCM.
ii.
iii.
Various exercise training disciplines appear to have qualitatively and quantitatively
different effects on cardiac structure and function. While both endurance and
strength training induce increases in left ventricular mass, strength training
generally leads to greater hypertrophy. Since athletes with cardiomyopathy can be
at risk of arrhythmias during physical exertion, it is important to exclude such
disorders before attributing cardiovascular, electrophysiological, or structural
changes to athletic training.
Criteria to distinguish HCM from athlete's heart
1. In individuals with possible diagnosis of athlete's heart vs. HCM, family history,
ECG, and LV cavity dimensions may help distinguish HCM from cardiovascular
adaptation in athlete. The evidence associated with these findings is discussed
2.
3.
4.
5.
6.
in detail separately.
ECG –ECG changes that develop as part of cardiovascular adaptation in
endurance athlete include SB, increased QRS voltage, tall peaked T wave, J
point elevation, and U waves. Pathological Q waves, LAD, and TWI, however,
strongly favor diagnosis of HCM.
Extent and pattern of LVH – As noted above, magnitude of expected LV wall
thickening varies with degree and type of athletic training. A finding of greater
degree of LVH than expected for degree and type of athletic training favors
diagnosis of HCM. In this regard, only high-level endurance training has been
associated with LVH of 13 to 15 mm. Of note, maximal LV wall thickness
achieved by women athletes almost never exceeds 14 mm.
Left ventricular cavity size – In study comparing 28 athletes with 25 untrained
patients with HCM, athletes had significantly larger LV cavities (end-diastolic
measurement of 60 vs. 45 mm), with LVEDD < 54 mm distinguishing HCM vs.
athletes heart with 100% sensitivity and specificity in this study.
Doppler and tissue Dopper echocardiography – Depressed Ea velocities found
in patients with HCM contrast with normal or above normal Ea velocities seen
in trained athletes who may also have LVH, although Ea velocities for these
populations have not been directly compared within study.
CMR – CMR can most accurately compare maximal LV wall thickness
measurements before and after period of systematic deconditioning. Patients
in whom wall thickness regresses > 2 mm supports diagnosis of athlete's heart,
while hypertrophy that remains unchanged suggests HCM. It does not appear
that competitive athletes demonstrate late gadolinium enhancement (LGE,
which suggests myocardial fibrosis), and therefore presence of LGE may also
provide additional information to confirm diagnosis of HCM.
7.
8.
2.
Functional exercise testing – Lower than expected levels of peak oxygen
consumption (VO2peak) may aid in differentiation between HCM and
physiologic LVH in athlete. In study that compared 8 athletic men with
genetically proven HCM and mild LVH to 8 matched elite athletes with same LV
wall thickness, elite athletes without HCM had significantly greater peak VO2,
anaerobic threshold (percent of predicted peak VO2), and oxygen pulse
(mL/beat) than patients with HCM. A peak VO2 > 50 mL/kg per min or > 20%
above predicted VO2max, O2 pulse > 20 mL/beat, or anaerobic threshold > 55%
of predicted VO2max were indicators of physiologic LVH rather than HCM.
Genetic testing for HCM can also be considered. The identification of
disease-causing sarcomere mutation in athlete with maximal LV wall thickness
in "grey zone" would provide definitive diagnosis of HCM.
Differential diagnosis of increased LV to aortic gradient
A. Other than dynamic subaortic LVOTO seen in HCM, several other anatomic and
physiologic abnormalities can be associated with increased pressure gradients between
LV and aorta.
B. Volume depletion
i.
Patients with significant volume depletion in setting of normal LV systolic function
will often develop hyperdynamic ventricular function in effort to maintain CO.
Hyperdynamic LV function results in more vigorous ejection of blood from heart at
higher velocity than normal, leading to intracavitary gradient which may be
mistaken for increased LVOT gradient. An intracavitary gradient is usually suspected
from clinical scenario (HoTN, tachycardia, other signs of hypovolemia) and almost
always disappears following fluid resuscitation.
C. Subaortic stenosis
i.
Fixed subvalvular AS is congenital abnormality typically caused by thin membrane
of tissue in LVOT which is typically seen on UCG as well as both color and spectral
Doppler UCG. Fixed subaortic stenosis can usually be distinguished from HCM and
valvular AS by UCG or invasive cardiac catheterization.
ii.
Unlike dynamic LVOTO seen in persons with HCM, there is typically no evidence of
SAM, and ventricular wall thickness is normal (although long-standing LV HTN due
to significant gradient across membrane can lead to concentric LVH). Unlike valvular
AS, aortic valve leaflets are usually normal (although long-standing high-velocity
turbulent flow across membrane over years to decades may result in AV damage).
D. Valvular aortic stenosis
i.
In addition to potentially causing LVH, narrowing of aortic valve opening can lead to
significant pressure gradient between LV and aorta. As with subaortic stenosis,
valvular AS can usually be distinguished from other pathology by UCG or invasive
cardiac catheterization.
GENOTYPE POSITIVE/PHENOTYPE NEGATIVE HCM PATIENT
1. With the use of genetic testing, HCM family members who carry disease-causing sarcomere
2.
mutation but without LVH can now be identified (so-called genotype positive/phenotype
negative patients). In about 50% of these individuals, ECG will be abnormal. Although these
patients have no increased wall thickness, a number of observations have suggested that
myocardium may still not be structurally normal. For example, abnormalities such as
myocardial fibrosis by contrast-CMR, collagen biomarkers, mitral leaflet elongation, diastolic
dysfunction, and blood-filled myocardial crypts have all been shown to occur in gene carriers.
The likelihood of developing clinical evidence of HCM with LVH in family members who have a
sarcomere mutation is uncertain. However, clinical follow-up with longitudinal screening
should continue based on the current screening recommendations.
3.
The risk of SCD in gene carriers is also unknown but considered to be very low, and therefore
consideration for prophylactic ICD should be resolved on individual case basis. However,
current society guidelines do not recommend excluding genotype positive/phenotype
negative HCM family members from participating in organized competitive sport.
SCREENING OF FIRST-DEGREE RELATIVES
1. HCMP is AD disorder, and most mutations have a high degree of penetrance. As a result,
first-degree family members of an affected individual should be evaluated for possible
inheritance of the disease. We agree with the recommendations of others that the
components of family screening should include Hx, PE, ECG, and UCG. We do not recommend
routine genetic screening of first-degree relatives unless definite HCM-causing mutation has
2.
3.
been identified in the index case.
Among first-degree adult relatives of patients with HCM, otherwise unexplained
echocardiographic and ECG abnormalities identified during screening examinations have a
high probability of reflecting the expression of HCM. Screening is not routinely recommended
before the age of 12 unless the child has clinical manifestations of HCM, high-risk family
history, or is participating in intense competitive sports.
Family members who have a normal evaluation should not necessarily be assumed to be free
of risk.
A. Because hypertrophy usually develops during adolescence, clinical evaluation should be
repeated annually from 12 to 18 years of age.
B.
Due to the possibility of delayed-onset hypertrophy, it is recommended that adult family
members with normal ECG and UCG who are over the age of 18 be reevaluated
approximately every five years. There may be a role for tissue Doppler echocardiography
in such patients, where abnormalities in contraction and relaxation velocities can
suggest pre-clinical myocardial dysfunction. However, these abnormalities are not
considered diagnostic for HCM and rarely precede development of ECG abnormalities.
C.
The identification of gene mutations for HCM has led to interest in the development of
DNA-based testing of patients with HCM and screening of family members. Genetic
screening may accurately define the risk of disease development, but it is not universally
available and presents additional possible concerns. Additionally, not all persons with a
genotype-positive mutation will have the HCM phenotype identified by ECG or
echocardiography. The issue of genetic testing and screening for HCM with genetic
testing is discussed in greater detail separately.
SUMMARY AND RECOMMENDATION
1. HCM is genetic cardiomyopathy caused by mutations of the cardiac sarcomere, resulting in
heterogeneous phenotypic expression with respect to the extent, location, and distribution of
left ventricle (LV) wall thickening as well as a diverse clinical course including sudden death,
2.
3.
4.
5.
6.
7.
heart failure, and stroke. The prevalence of HCM in general population is 1 in 500 adults.
Histopathology in patients with HCM reveals disorganized myocyte architecture, including
hypertrophied myocytes in a disarray pattern with bizarre-shaped nuclei, abnormal
intramural coronary arteries, and interstitial as well as replacement fibrosis.
While many patients with HCM remain asymptomatic, it is not uncommon for patients to
develop one or more of the following symptoms: dyspnea on exertion, orthopnea,
paroxysmal nocturnal dyspnea, chest pain, palpitations, presyncope/syncope, postural
lightheadedness, fatigue, or edema.
The physical examination in HCM may be normal or may reveal nonspecific abnormalities
such as a fourth heart sound, systolic murmur, and/or left ventricular lift. Patients with LVOT
obstruction may have harsh crescendo-decrescendo systolic murmur, which develops slightly
after S1 and is heard best at the apex and lower left sternal border. Several physical exam
maneuvers can affect degree of obstruction, resulting in change in murmur intensity.
The evaluation for HCM in an individual patient may be prompted by a family history of HCM,
systolic ejection murmur, abnormal 12-lead electrocardiogram showing otherwise
unexplained evidence of left ventricular hypertrophy, and clinical symptoms including
syncope. In addition to performing a comprehensive cardiac Hx and PE and ECG in all patients
with suspected HCM, cardiac imaging to identify LVH should be performed.
Although the ECG is abnormal in 90% of HCM patients, no specific pattern is diagnostic.
Typically, the ECG shows repolarization abnormalities but also may include prominent
abnormal Q waves, P wave abnormalities, left axis deviation, and deeply inverted T waves.
Two-dimensional echocardiography can be used to reliably diagnose patients with HCM when
an area of increased LV wall thickness is imaged anywhere in the LV wall in the absence of
another cause. Echocardiographic findings suggestive of HCM include LVH (particularly when
asymmetric and involving the septum or anterolateral wall), an increased LVOT gradient, and
systolic anterior motion of the mitral valve leaflets, particularly when associated with an
increased LVOT gradient. In addition, CMR can be used to clarify a diagnosis of HCM or the
extent of wall thickness in those patients in whom LV wall thickness measurements remain
uncertain with two-dimensional echocardiography.
8.
9.
The majority of patients with HCM have LVOT obstruction under resting conditions or
following exercise. Because of this, we proceed with exercise stress testing in all patients with
known or suspected HCM as part of the risk stratification process. Exercise should be
performed as the stress agent rather than using a pharmacologic stress agent, as a maximal
treadmill or bicycle exercise stress test provides an objective measurement of functional
capacity and information on the integrity of vascular responses and the risk of exercise
related ischemia, arrhythmia, and obstruction.
Genetic testing is available for clinical use but is predominately reserved for identifying
patients who may have disease which appears phenotypically similar to sarcomere HCM, such
as Fabry disease or lysosomal/glycogen storage disease, or to help identify family members
who may be at risk of developing HCM.
10. The diagnosis of HCM can usually be made following echocardiography and/or CMR imaging,
and invasive diagnostic assessments are rarely necessary. We typically reserve invasive
hemodynamic assessment using cardiac catheterization for patients with suspected HCM to
exclude obstructive coronary artery disease, distinguish pericardial constriction from severe
restrictive physiology, to perform endomyocardial biopsy to exclude non-sarcomeric causes
of HCM, or for pre-cardiac transplant assessment.
11. In the patient presenting with LVH, HCM must be distinguished from acquired causes of
cardiac hypertrophy, including hypertension, aortic stenosis, and athlete's heart. Other than
the dynamic subaortic (LVOT) obstruction seen in HCM, several other anatomic and
physiologic abnormalities can be associated with increased pressure gradients between the
LV and the aorta, including volume depletion, subaortic stenosis, and valvular aortic stenosis.
12. HCM is an autosomal dominant disorder, and most mutations have a high degree of
penetrance. As a result, first-degree family members of an affected individual should be
evaluated for possible inheritance of the disease. The components of family screening should
include history, physical examination, ECG, and UCG. We do not recommend routine genetic
screening of first-degree relatives unless a definite HCM-causing mutation has been identified
in the index case.