Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
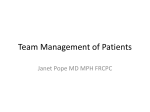
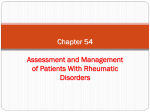
Poster Viewing Session 2 Conclusions: This CTC model has helped to shorten the referral lag time, as well as management lag time. The self-administered questionnaire has proved to be valid and comprehensible. Clinical tests for CTS are not reliable predictors of the diagnosis. There is a room for conservative therapy in the management of CTS. Miscellaneous Rheumatic Diseases 264. EARLIER MHC CLASS I OVER-EXPRESSION RESULTS IN A MORE SEVERE PHENOTYPE IN TRANSGENIC MODEL OF MYOSITIS Thursday 04 May 2006, 08:30–10:00 i111 Results: Two males and five females, age range 26 to 62 yrs (median age 47) disease duration from 5 months to 8 yrs, took part. Interviews produced rich descriptions. Issues related to bladder and bowel involvement emerged from the preliminary data and these themes were explored in more depth in later interviews. Most patients experienced frequency, urgency and pain similar to cystitis on micturition. When asked to describe these organs, they expressed the bladder and to a lesser extent the bowel, were enormous and felt a sense of the organs merging with their affected leg. One patient reported no dysfunction or distortion. Conclusions: Findings from this qualitative study indicate that CRPS patients do suffer from disturbances of visceral sensation and perception including pain, supporting our hypothesis. Some of whom had extensive urological investigations which were negative but without a diagnostic label. This has implications for clinical practice. Further research is required in this area. C. K. Li, B. Singh and L. R. Wedderburn 1 Rheumatology Unit, Institute of Child Health, UCL, London, United Kingdom and 2 Department of Pathology and Infectious Diseases, The Royal Veterinary College, London, United Kingdom 266. Background: Over-expression of Major Histocompatibility Complex (MHC) Class I on muscle fibres in inflammatory muscle diseases is a well-recognised phenomenon. Expression of MHC on normal muscle fibres is low. We have shown that in the most common paediatric form of myositis, juvenile dermatomyositis (JDM), this phenomenon is seen very early after presentation, and that it may be present in the absence of infiltrating inflammatory cells (Li et al. 2004). Methods: Using a double transgenic mouse model where MHC Class I expression on muscle cells is controlled by the withdrawal of the antibiotic doxycycline (Nagaraju et al. 2000), we modelled JDM by early over-expression of MHC class l at 3 weeks of age, simultaneous with weaning. Mating parents and pre-weaned female pups were kept on doxycycline. Mice in group 1 were taken off doxycycline at time of weaning, while those in group 2 were kept on doxycycline until 35 days. Age matched double transgenics left on doxycycline and single transgenics were kept as controls. Mice were regularly weighed and observed for behavioural changes, in particular for reduction of voluntary movement. Muscle strength was measured by timing the ability to maintain running on an accelerating rotating device (Rotarod). Skeletal muscles were frozen at the time of sacrifice. All procedures comply with United Kingdom Home Office guidelines and ethical approval. Mice were sacrificed at pre-defined time-points, or when deemed to be significantly disabled on a scoring system as advised by veterinary support. Results: Double transgenic mice had statistically significant reduction of strength/ stamina as assessed by Rotarod running when analysed in a regression model factoring in that double transgenic mice exhibit weight loss over time, compared to age-matched controls. Controls kept on doxycycline did not show significant weight loss or weakness (n ¼ 10). Mice from group 1 developed severe and fatal disease compared to the late group. 69% (24/35) died spontaneously or were deemed to have severe disease to be culled at 90 days of age (69 days after transgene activation), compared to group 2 where the same severity was not reached by 250 days. Histological analysis revealed muscle necrosis, fibre size variation, hyalinisation, loss of striations, attempted muscle regeneration and predominantly macrophagic inflammatory infiltration in both groups. A scoring system encompassing these features was devised and comparison of mice from the two groups (matched by transgene activation time) and age matched single transgenic controls was performed: the differences in the scores were statistically significant when comparing either double transgenic group to the control group (Kruskal Wallis, P ¼ 0.03), but did not show significant difference between the two double transgenic groups. Conclusions: Our data suggest that pathological upregulation of expression of MHC Class I at a time point when muscle fibres are growing in early life, may have a different effect than the same process in adult mature fibres. Background: Minocycline, a semi-synthetic tetracycline used predominantly as a treatment for acne, has been recognised as a cause of a drug induced lupus since the early 1990s, with over 100 cases now reported in world literature. For an illness to be recognised as a drug induced lupus, symptoms should be induced only after exposure to the drug, and recur on rechallenge. In a series reported by Lawson et al. [1], oral rechallenge with minocycline induced an illness characterised by fever, polyarthralgia and myalgia with raised CRP, within a few hours of a single oral dose. This suggests a cytokine mediated process. The aim of our study was to produce an in vitro rechallenge with minocycline, in patients previously diagnosed with a likely minocycline induced lupus, and observe the response of TNF and other pro-inflammatory cytokines. Idiopathic lupus patients not previously exposed to minocycline were used as controls. Methods: PBMCs were isolated from 3 patients diagnosed with minocycline induced lupus, in whom minocycline had been withdrawn, and 3 patients with idiopathic lupus, meeting ACR criteria for diagnosis but with quiescent disease. PBMCs were then cultured with minocycline at 5 and 50 g/ml concentrations, with and without LPS stimulation. TNF mRNA production was measured by Realtime PCR, at 0, 4 and 18 hr. Results: In 1 patient with a severe minocycline induced illness consisting of fever, rash and a small joint polyarthritis starting within 3–4 weeks of commencing minocycline, a marked elevation in TNF mRNA production was seen after 18 hr of culture with 50 g/ml minocycline compared with the samples not cultured with minocycline, and the lupus controls (Fig. 1). The remaining patients, with less severe clinical presentations did not demonstrate a TNF response which differed from those with idiopathic lupus. Conclusions: This study has demonstrated a convincing TNF response to in vitro rechallenge with minocycline in a patient presenting with an acute illness 3 to 4 weeks after commencing minocycline, which resolved on withdrawal of the drug. This supports the hypothesis that a cytokine mediated mechanism underlies this illness. The lack of a similar response in the remaining patients, whose symptoms were milder, and occurred only after 12–18 months of minocycline use may reflect a different disease mechanism, a sub-threshold minocycline dose, or that the observed illness following in vivo rechallenge is the result of hepatic metabolism. We believe that this area is worthy of further study in a larger series, as the technique has the potential to be used as part of a diagnostic test for minocycline induced lupus. MINOCYCLINE INDUCED LUPUS – AN IN VITRO RECHALLENGE J. R. Maxwell, D. Mewar, E. M. Heath, A. L. Coote, M. Akil and A. G. Wilson Division of Genomic Medicine, The University of Sheffield, Sheffield, United Kingdom 265. COMPLEX REGIONAL PAIN SYNDROME IS ASSOCIATED WITH VISCERAL DISTURBANCE IN BLADDER AND BOWEL: A HYPOTHESIS H. E. Cohen1,2, J. S. Lewis1,3 and D. R. Blake1,2 1 Rheumatology, The Royal National Hospital for Rheumatic Diseases, Bath, Somerset, United Kingdom, 2School of Health, University of Bath, Bath, Somerset, United Kingdom and 3School of Health Professions and Rehabilitation Sciences, University of Southampton, Southampton, United Kingdom Background: Peripheral and central sensitisation of visceral afferent nerve fibres may occur in an analogous fashion to that demonstrated in sensory motor nerve fibres with chronic pain states. Lower limb visceral and sensory afferent nerve fibres travel together possibly generating sympathetic nociceptive expansion. This could cause increased awareness of visceral sensations that would be interpreted as painful. Similarly, neuroplastic cortical remapping may occur which could give rise to disturbances of autonomic visceral sensation. On this basis we would hypothesise that patients with complex regional pain syndrome (CRPS) would have disturbances of visceral sensation and perception including pain. Methods: Following informed consent, 7 consecutive patients with lower limb involvement who met the International Association of the Study of Pain CRPS classification were interviewed. Qualitative methods were used to explore participant experience and perceptions regarding their bladder and bowels. These semi-structured interviews were coded and analysed utilising a grounded theory approach and themes emerged from the data. FIG. 1. Reference 1. Lawson et al., Rheumatology 2001;40:329–335. i112 Thursday 04 May 2006, 08:30–10:00 267. ARTHROPATHY ASSOCIATED WITH HEPATITIS C VIRUS INFECTION A. A. Elbeialy1, S. M. Zaky2 and A. M. Bersy3 1 Rheumatology, Azhar Faculty of Medicine, Damietta, El Salvador, 2Enterology, Azhar Faculty of Medicine, Damietta, Egypt and 3Clinical Pathology, Azhar Faculty of Medicine, Damietta, Egypt Background: Arthropathy associating HCV is common, affecting up to 20% of HCV-infected individuals, and is commonly presented as rheumatoid-like, with symmetrical inflammatory polyarthritis involving mainly small joints, or, less commonly large joints, and is associated with a positive rheumatoid factor test. It is typically non-deforming, and not associated with articular bony erosions. This study was carried out to assess the incidence of rheumatoid like manifestations in association with HCV infection and its characterization. Methods: A cohort of 100 patients with clinically evident HCV infection, were examined for the presence of articular or musculoskeletal problems. Another 100 rheumatoid arthritis patients were screened for the presence of concomitant HCV infection. CBC, ESR, ALT and AST enzymes, serum uric acid, antinuclear, anti smooth muscle, antimitochondrial, and extractable nuclear antigen autoantibodies, serum rheumatoid factor, and mixed cryoglobulins were all measured. HCV antibodies were tested for all patients. HCV RNA sequences were determined in rheumatologically affected patients. Results: Polyarthropathy was reported in 25 HCV patients (25%), 2 of them had true RA. The other 23 patients had not fulfilled the ACR criteria, although they had polyarthropathy of hands and/or feet, small and large joints, and a positive rheumatoid factor. They had neither rheumatoid nodules, morning stiffness, nor diagnostic X-ray findings. On the other hand, HCV infection was detected in only 4% of RA patients. Rheumatoid factor autoantibody was detected in 100% of HCV patients with arthropathy vs 69% of those without arthropathy. ESR was significantly raised in patients with arthropathy than those without arthropathy, while haemoglobin was significantly lower in the arthropathy group. Arthropathy group significantly had viraemia (88%), which was of the moderate and low levels as referenced by the used kits. The arthropathy group had significantly longer duration of HCV infection (10.6±4.2 yrs) prior to complaining of joint problems. Conclusions: Rheumatological symptoms and autoimmune markers are common in HCV infection and are usually overlooked. Patients with unexplained joint pains or rheumatological symptoms of unknown origin should be screened for HCV, because treatment would be different, and the outcome of proper treating HCV arthritis would be excellent. 268. HUMAN IMMUNODEFICIENCY VIRUS-ASSOCIATED RHEUMATIC MANIFESTATIONS IN A WELL-DEFINED HIV-POSITIVE COHORT IN THE UK K. E. Walker-Bone1, M. Fisher2, D. Churchill2 and G. Dean2 1 Department of Rheumatology, Brighton & Sussex Medical School, Falmer, Brighton, East Sussex, United Kingdom and 2HIV/GUM, Royal Sussex County Hospital, Brighton, East Sussex, United Kingdom Background: Since the discovery of human immunodeficiency virus (HIV) in 1984, HIV has become a global pandemic. Soon after the virus was discovered, early case reports suggested that untreated HIV infection was associated with rheumatic manifestations such as spondyloarthropathies, psoriatic arthritis, Reiter’s syndrome, and a diverse range of connective tissue diseases and vasculitis. Now however, highly active antiretroviral therapy (HAART) has dramatically improved the morbidity associated with HIV infection and rates of survival have improved considerably. Currently unknown however, is what effect, if any, the advent of HAART has had on rheumatic syndromes associated with HIV infection. In Brighton, East Sussex, there is a high prevalence of HIV infection and patients have been studied prospectively for more than 10 yr. Currently, there is a well-defined cohort of 1100 patients undergoing regular follow-up and assessment. The objectives of this study was a prospective evaluation of rheumatic symptoms among any member of the cohort. Methods: In collaboration with the team of local HIV/GUM physicians, a dedicated rapid response rheumatology clinic has been set up adjacent to the premises of the HIV/GUM department. All HIV positive patients reporting symptoms or signs of rheumatic disease are referred for assessment by one Consultant Rheumatologist. Symptoms and signs are classified, where possible, according to recognised classification criteria and investigation and treatment plans initiated in collaboration with the HIV/GUM physician. Results: To date, 42 patients with HIV infection and musculoskeletal symptoms/ signs have been referred to the clinic since January 2005 (equivalent to 5% annual incidence): 34 men (81%) and 8 women (19%). The group was predominantly homosexual (71%). Arthralgia was common (5/42, 12%). Two cases of chronic Reiter’s syndrome (2/42, 5%) and three other cases of seronegative arthritis were diagnosed (one enteropathic associated with ulcerative colitis), and one psoriatic. 2 patients have presented with SLE, according to ACR criteria and one patient with Diffuse Idiopathic Lymphocytosis Sydrome (DILS). Two male patients have presented with gout. Two female patients fulfilled the ACR criteria for the diagnosis of fibromyalgia syndrome (5%). Soft tissue regional pain syndromes were also common, including: carpal tunnel syndrome, lateral epicondylitis, pre-patellar bursitis, shoulder pain and neck pain. Most patients had low viral loads and high CD4 cell counts at the time of presentation and the majority were taking HAART. To date, intra-articular injections have been undertaken in 5 patients under strict sterile technique. Two patients have been commenced on corticosteroids. Poster Viewing Session 2 Conclusions: Rheumatic symptoms were common among this HIV positive population. In comparison with the pre-HAART era, there appears to be a changing spectrum of rheumatic conditions. HAART may be associated with autoimmune rheumatic disease through the phenomenon of immune reconstitution. 269. AUTOLOGOUS STEM CELL TRANSPLANT IN STILL’S DISEASE H. V. Reddy1, V. V. Kaushik1, T. D. Kennedy1, P. J. Prouse2 and J. Thachil3 1 Rheumatology Department, Royal Liverpool University Hospital, Liverpool, United Kingdom, 2Rheumatology Department, North Hampshire Hospital, Basingstoke, Hants, United Kingdom and 3Haematology Department, Royal Liverpool University Hospital, Liverpool, United Kingdom Background: Still’s disease is a systemic disease characterised by polyarthritis, intermittent fever and a typical rash [1]; other clinical features include lymphadenopathy, hepatosplenomegaly, anaemia, leucocytosis and characteristically significantly raised inflammatory markers and ferritin. The first reported use of autologous Hematopoietic Stem Cell Transplant (HSCT) in juvenile idiopathic arthritis was in children with the most severe and longstanding systemic disease, with much irreversible erosive joint destruction [2]. We present 2 patients with Still’s disease successfully treated with HSCT. Methods: A 24-year-old woman was diagnosed with Still’s disease at the age of 14. Her disease was characterised by frequent flares with no significant joint damage and was steroid dependant. She failed to respond to traditional DMARDS, biologic therapies and IVIG. Based on previous reports of successful HSCT [2, 3, 4], she underwent this procedure in May 05. The post transplant period was complicated by persistent fever for 3 months, thought to be viral in origin. She also had 2 episodes of severe autoimmune haemolysis with frank haematuria associated with Kidd group antibodies. She recovered well and is currently in remission, with normal inflammatory markers. She is being gradually weaned off prednisolone (current dose 2.5 mg daily). The second report is a 34-year-old woman with the diagnosis, based on intermittent fever, rash, arthritis, leucocytosis, anaemia and raised inflammatory markers. She was steroid dependant and had significant erosive disease. She failed to respond to traditional DMARDS and biologic therapies. She underwent HSCT in early 2003. She responded very well and was in remission soon after with normalised inflammatory markers. She had a successful pregnancy in 2004 giving birth to a healthy baby boy in October and to date remains in remission. Results: Conclusions: Still’s disease accounts for 10–20% of patients with JIA. The pathogenesis is unknown and management includes NSAIDs, high dose corticosteroids and intravenous immunoglobulin courses. There are a number of reports showing moderate efficacy with the use of traditional DMARD therapy. However DMARD therapies appear to help the articular symptoms more than the systemic symptoms. With the advent of biologic therapies, these have been tried in a few patients with varying degrees of success. Based on our two patients and other published reports Hematopoietic Stem Cell Transplant (HSCT) appears to offer a viable alternative and hope for patients with recalcitrant Still’s disease. However the potential risks associated with the procedure should be weighed against its benefits before being offered to patients. More research is required into this before it can be recommended as a definitive management option. References 1. 2. 3. 4. Bull Rheum Dis 1972;23:712. Lancet, 353,550–3. Annals of the Rheumatic Diseases, 63;1318–26. Bone Marrow Transplant 2000;25:1307–10. 270. ADULT ONSET STILL’S DISEASE. CLINICAL COURSE AND OUTCOME; SOUTHEND EXPERIENCE D. Makkuni and B. Dasgupta Rheumatology, Southend General Hospital, Southend, Essex, United Kingdom Background: Adult onset Still’s disease(AOSD) is a rare systemic inflammatory condition of unknown aetiology. Diagnosis and treatment of this condition can be difficult due to the lack of diagnostic and management guidelines. The disease can have a variable course and outcomes with some patients presenting with recurrent systemic symptoms like fever and rash or others evolving into a chronic arthropathy with serious functional disability. The treatment options have improved with the advent of biological agents. Through this study we look into the local experience of the management of AOSD. Methods: Patient with an established diagnosis of AOSD, fulfilling the Yamaguchi criteria (Major-fever, arthralgia, rash and leucocytosis Minor-sorethroat, liver dysfunction, negative ANA and Rheumatoid factor, Lymphadenopathy) were identified through the Rheumatology data base at the Southend hospital. The clinical presentation, course of the disease and response to treatment were studied. Results: Eight cases of AOSD were identified, 5 female and 4 male patients. The age of presentation varied between 28–80 yr (only 3 patients above the age of 40 yr). The joints most commonly affected were wrists, ankles and knees (Table 1). Six patients had tenosynovitis and out of these 2 subsequently developed stenosing tenosynovitis needing orthopaedic intervention. Systemic signs apart from fever and rash were pleurisy, pericarditis, anemia, lymphadenopathy, hepatosplenomegaly, mild transaminitis and positive urine sediments. All patients initially received highdoses of steroids to control the disease (50–80 mg oral Poster Viewing Session 2 Thursday 04 May 2006, 08:30–10:00 prednisolone and 500–1 gm IV methylprednisolone) followed by methotrexate. Two patients went into complete remission 2 and 4 yr of treatment but the rest developed chronic polyarthropathy and these patients required a maintenance dose of 10–15 mg prednisolone along with 15–20 mg methotrexate. Three patients received biologic therapy (2 etanercept and 1 Anakinra) and showed very good response to therapy. Of the eight patients only two patients showed progressive articular damage. One patient underwent total knee replacement. Conclusions: The natural history of AOSD from this study has shown a significant tendency for chronicity. Six out of 8 patients developed chronic articular problems with poor functional outcome. Tenosynovitis of flexor and extensor tendons were seen at the time of presentation in majority of cases. All patients required high doses of steroids for inducing as well as maintaining the disease in remission in addition to therapeutic doses of methotrexate. Anti TNF drugs like etanercept and IL1 blocker Anakinra were found to be extremely useful in controlling the disease in a subset of patients with chronic active disease. In future an aggressive treatment strategy including early introduction of biologic agents should be tried in these patients. Articular distribution in AOSD Tenosynovitis Wrists Ankles Knee Others 6 6 3 3 2 i113 (DAS(4) ¼0.54*sqrt(RAI) þ 0.065* (swollen44) þ 0.33*Ln(ESR) þ 0.0072*GH; DAS(3) ¼ 0.54*sqrt (RAI) þ 0.065*(swollen44) þ 0.33*Ln(ESR) þ 0.22; DAS-4(crp) ¼ 0.54*sqrt(RAI)þ0.065*SJC44 þ 0.17*ln(CRP+1) þ 0.0072*GH þ 0.45; DAS3(crp) ¼ 0.54*sqrt(RAI)þ0.065*SJC44 þ 0.17*ln (CRP+1) þ 0.65; DAS28(4) ¼ (0.56*sqrt(t28) þ 0.28*sqrt(sw28)þ 0.70*Ln(ESR) þ 0.014*GH; DAS28(3) ¼ [0.56* sqrt(t28) þ 0.28*sqrt(sw28) þ 0.70*Ln(ESR)]*1.08 þ 0.16; DAS28-CRP(4) ¼ 0.56* sqrt(TJC28) þ 0.28*sqrt(SJC28) þ 0.36*ln(CRP+1) þ 0.014* GH þ 0.96; DAS28CRP(3) ¼ [0.56*sqrt(TJC28) þ 0.28*sqrt (SJC28) þ 0.36*ln(CRP+1)]*1.10 þ 1.15). All data are permanently stored and data retrieval for analysis in most format is possible (excell, access, spss . . .), as well as download of pre-existing data set. Results: I designed a software for easy DAS calculations however, with the unique ability to download pre-existing data, permanently store and retrieve data in most desired formats. The capture screen was designed to resemble the paper version of DAS calculation used in most research departments. All procedures are automatic and data entry is similar to what would be stored on paper records. There is no need to know the database language and procedures are simplified to the maximum. The computer and web-interface versions are available and the mobile phone and pocket computer versions are currently under further development. Conclusions: This new tool provides the opportunity for research departments to record DAS from any set up (computer, web-interface, pocket-PC or mobile phone) in a unique format that can be stored in a centralised departmental database. The software will be compatible with other clinical data storage systems currently under development. Others-MCPjoints. 271. AN EPIDEMIOLOGICAL STUDY OF CONNECTIVE TISSUE DISEASES PRESENTING AS FEVER OF UNKNOWN ORIGIN (FUO) OVER 5 YEARS DURATION F. I. Fahmy1, A. A. Elbeiay1, S. M. Zaky2 and A. M. Bersy3 1 Rheumatology, Azhar Faculty of Medicine, Damietta, Egypt, 2Tropical Medicine, Azhar Faculty of Medicine, Damietta, Egypt and 3Clinical Pathology, Azhar Faculty of Medicine, Damietta, Egypt Background: The diagnostic spectrum of fever of unknown origin (FUO) has changed since its original definition. The number of cases of FUO due to infectious diseases has declined and there has been a corresponding increase in the number of cases due to multisystem diseases, such as systemic lupus erythematosus, rheumatoid arthritis, and Still’s disease. Unfortunately, many of these rheumatic diseases presenting with FUO may remain undiagnosed for months, and reach the rheumatologist very late. This prospective study was devoted to point out the frequency of patients presenting with FUO associated with connective tissue diseases, over 5 yrs’ duration in our country. Methods: This study included a series of 578 patients, all had been attending Tropical Medicine Departments, al-Azhar University, and Abbasseya Fever Hospital, in Cairo, over 5 yrs duration, from 2000 to 2004. Each patient was subjected to complete evaluation and meticulous medical examination, followed by intensive laboratory studies, documented thoroughly with respect to past and present medical history. Each patient had fulfilled Petersdorf and Beeson criteria for FUO. Results: The most common causes of FUO were infectious diseases (294, 50.86%), connective tissue diseases (CTDs) (107, 18.51%), neoplasms (105, 18.17%), and other causes (72, 12.46%). SLE was the most common cause of CTDs associated with FUO (45.8%), followed by RA (19.6%), and Still’s disease (14.0%). Other CTDs were polymyositis (5.6%), dermatomyositis (2.8%), polyarteritis nodosa (1.9%), Behcet disease (1.9%), sclerodermia (2.8%), rheumatic fever (1.9%), mixed connective tissue disease (0.9%), inflammatory bowel disease (0.9%), psoriasis (0.9%), and eosinophilic fasciitis (0.9%). The study showed that most of the patients diagnosed as having CTD presented with fever were in the middle age group (30–40 yrs old), most of them were females (95.09%). Conclusions: These results give us a strong impression that we have not to neglect the increased incidence of CTDs from routine medical clerking of patients with FUO, and it is valuable to include a rheumatologist in the consultation of all patients with FUO. Together with a logical and disciplined approach, this might help early detection and diagnosis of CTDs presented with FUO. 272. AN ELECTRONIC TOOL TO CALCULATE AND STORE DAS SCORES P. Gente Software Designer, Paris, France Background: The need for rapid disease activity score calculations has been recognised in Rheumatology both clinically and for research purposes. However, some of the current calculators do not allow data retrieval or even long term storage. I have created a software with a single capture screen for DAS and DAS28 calculations with automatic download and storage of all individual component of the score into a database allowing data analysis in the long term. Methods: A new database language allowing the design of applications for computers, pocket-PC, mobile phones and a web-interface was used. A single screen for the capture of all data set (patient ID, date, visit number for followup, tender swollen joint count, ESR, CRP and patient’s global assessment of disease activity) was designed using a combination of free data entry fields, pre-set boxes and click-button. Different DAS calculations appear automatically FIG. 1. 273. RISK FACTORS FOR OSTEOPOROSIS IN SUBJECTS WITH BENIGN JOINT HYPERMOBILITY SYNDROME (BJHS): COMPARISON TO POPULATION BASED CONTROLS A. Stewart1, A. J. Black2 and D. M. Reid1 1 Department of Medicine and Therapeutics, University of Aberdeen, Aberdeen, United Kingdom and 2Department of Rheumatology, NHS Grampian, Aberdeen, United Kingdom Background: Previous studies have shown that those with joint hypermobility are at greater risk of osteoporosis. These studies examined patients suffering from Ehlers-Danlos syndrome or benign hypermobility. These studies involved a variety of techniques to measure bone mass. The aim of our study is to examine osteoporosis risk factors, bone mass and bone turnover markers in subjects with BJHS and controls. Methods: Individuals with diagnosed BJHS were identified using an electronic diagnostic database, with a total of 54 subjects identified. Of these 50 were invited to take part. Our response rate was 70% with 35 individuals responding positively and of these 30 attended for their appointments. To date the bone mass has been measured in BJHS cases only. Age-matched controls (n ¼ 120) are part of a population-based study (OPUS) in whom data are available on risk factors for osteoporosis and historical, but not current, bone mass. A medic examined the joints to provide a Beighton score to test whether the Brighton criteria for BJHS were met. A questionnaire used in the OPUS study was completed by both cases and controls. 2 analysis was used to detect differences in prevalence of risk factors. Results: The average age of both cases and controls was 37 yrs, and largely premenopausal (86.7% of cases, 74.2% of controls, P ¼ 148). Of the cases 25 (83.3%) fill the criteria for hypermobility syndrome as set by the Brighton criteria. We assessed differences in osteoporosis risk factors. There were no significant differences between cases and controls for age (P ¼ 0.818), height (P ¼ 0.376) or weight (P ¼ 0.694). Differences were found for self-reported osteoporosis risk factors. Significantly higher prevalence was found in cases compared to controls for the following risk factors; previous fracture (P ¼ 0.007, cases 60%, 33.3%): family history of osteoporosis (P ¼ 0.012, cases 33.3%, controls 13%): oral corticosteroid use (P ¼ 0.012, cases 13.3%, controls 2.5%). We asked about osteoporosis medications and the cases indicated a higher prevalence (P ¼ 0.011) of ever taking calcium (16.7%) in comparison to the controls (3.3%), but i114 Thursday 04 May 2006, 08:30–10:00 no differences in other forms of treatment. No differences were found for smoking, alcohol intake or exercise, but the cases did record significantly reduced days of current intake of yoghurt (P ¼ 0.004), milk (P ¼ 0.027), milk products (P ¼ 0.007). Back pain was high in both groups, but significantly higher in the cases (P ¼ 0.009, cases 86.7%, controls 61.7%). However cases graded their general health better than controls (P ¼ 0.002). Conclusions: Subjects with BJHS may be at higher risk of osteoporosis due to an increased prevalence of previous fracture, family history of osteoporosis, corticosteroid use, and a decreased intake of calcium based foods. Bone mass has been measured in the BJHS subjects and will be compared to the controls in whom bone mass will be reassessed in the next few months. This will indicate whether the increased risk factors translates into lower bone mass. 274. MRI APPEARANCES IN LÖFGREN’S SYNDROME; IS ANKLE SWELLING CAUSED BY ARTHRITIS, TENOSYNOVITIS OR PERIARTHRITIS? J. D. Rees, P. Peterson and B. E. Bourke Department of Rheumatology, St George’s Hospital, London, United Kingdom Background: The rheumatological presentations of sarcoidosis are diverse. In the acute form of arthritis seen in Löfgren’s syndrome features include a variable inflammatory picture, sometimes mimicking either a reactive arthritis or rheumatoid arthritis. Features of periarticular soft tissue swelling, synovitis and tenosynovitis may be present clinically and are often associated with severe disability. Methods: We present MRI findings in two typical cases of acute sarcoidosis. Both cases occurred in young adult Caucasians who presented with acute and disabling symptoms. Both patients had bilateral hiliar lymphadenopathy on chest X-Ray, elevated serum ACE levels and bilateral lower leg swelling. Results: MRI findings in the two cases were very different as was clinical outcome. Case One In the first case the MRI confirmed a periarthritis rather than a true inflammatory arthritis. The main abnormalities demonstrated were of subcutaneous oedema, an effusion within the ankle joint and oedema within the sinus tarsi (Fig. 1). The patient was treated with NSAIDs alone and there was a rapid resolution of the symptoms and signs. Poster Viewing Session 2 Conclusions: We describe the features of acute sarcoidosis of the ankle joints in which have been investigated acutely with MRI scanning. The MRI has been able to define accurately the periarticular vs articular nature of the acute manifestations of the arthritis seen in Löfgren’s syndrome. We suggest that an early MRI may give prognostic information regarding the course of the arthritis. Patients with a periarthritis rather than a true inflammatory arthritis are likely to have a more favourable clinical outcome. Paediatric and Adolescent Rheumatology 275. NEUROMUSCULAR IMPAIRMENTS IN CHILDREN DIAGNOSED WITH HYPERMOBILITY SYNDROME: A PRELIMINARY STUDY F. A. Fatoye1, F. Macmillan1, S. Palmer2, P. Rowe3 and S. Wilkinson4 1 Physiotherapy Subject Area, Queen Margaret University College, Edinburgh, United Kingdom, 2Faculty of Health & Social Care, University of the West of England, Bristol, United Kingdom, 3Bioengineering Unit, University of Strathclyde, Glasgow, United Kingdom and 4Physiotherapy Department, Royal Hospital for Sick Children, Edinburgh, United Kingdom Background: Impaired joint proprioception has been found in association with hypermobility syndrome (HMS) (Mallik et al. 1994; Hall et al. 1995). However, it is uncertain if other neuromuscular indices in children with HMS are impaired. Therefore, this study investigated a range of neuromuscular impairments in healthy children and those diagnosed with HMS. Methods: Seventeen healthy girls (mean age 11.3±S.D. 2.5 yr) and 13 girls diagnosed with HMS (mean age 11.8±S.D. 1.3 yr) participated in this investigation. The study was approved by the Education Department, City of Edinburgh Council, and the QMUC and NHS Lothian Local Research Ethics Committees. Informed written consent was obtained from the participants and their parents. Knee joint kinaesthesia (KI) was assessed at 60 degrees of knee flexion and joint position sense (JPS) was examined at both 25 and 10 degrees of knee flexion using a motorised proprioception measuring device. Absolute angular error (AAE) was calculated as the difference between the target and perceived angle for JPS tests. Quadriceps and hamstrings muscle torque was measured in high sitting with the test knee in 90 degrees using a digital myometer. Muscle torque was normalised to body weight. Mann-Whitney U tests were used to compare the variables between the two groups. Results: The results of this study are presented in table 1 below: Conclusions: The knee joint proprioception outcome measures were significantly different in children with HMS and they also showed weaker quadriceps muscles than the healthy controls. However, there was no hamstring muscle strength deficit between the two groups. Clinicians should be aware of these identified impairments in children with HMS, and a programme of proprioception and muscle strengthening exercises may be indicated. TABLE 1. The mean (S.D.) for joint proprioception and muscle torque Proprioception ( ) Group FIG. 1A. Case Two In the second case the MRI confirmed a true inflammatory arthritis with a marked synovitis affecting the ankle joint. Additionally there were effusions of numerous tendon sheaths (tibialis posterior, flexor digitorum longus and flexor hallucis longus). The patient is still symptomatic two years following onset despite treatment that has included NSAIDs, corticosteroids, hydroxychloroquine and most recently methotrexate. Healthy HMS P-values Muscle torque (Nm/kg) KI at 60 AAE at 25 AAE at 10 Quadriceps Hamstrings 1.90 (0.83) 3.15 (1.91) 0.030* 4.56 (2.94) 7.39 (3.69) 0.045* 2.33 (2.89) 4.92 (2.53) 0.011* 1.49 (0.24) 1.16 (0.30) 0.002* 0.86 (0.48) 0.63 (0.21) 0.161 *Statistically significant at < 0.05. References 1. Hall et al. British Journal of Rheumatology 1995;34:121–25. 2. Mallik et al. British Journal of Rheumatology 1994;33:631–37. 276. GENERATION OF TOLEROGENIC DC FROM PATIENTS WITH JUVENILE IDIOPATHIC ARTHRITIS E. Sala Soriano, K. R. Newton, S. Burns and L. R. Wedderburn Rheumatology Unit, Institute of Child Health, University College London, London, United Kingdom FIG. 1B. Background: Juvenile Idiopathic Arthritis (JIA) is one of the most common rheumatic diseases in children. There are various subtypes of JIA, with major differences in both severity and outcome. Both T cells and Dendritic Cells (DC) are key cell types contributing to the pathology of JIA. We have found CD4+CD25þ regulatory T cells (Treg) in the synovial fluid (SF) of children with JIA, and DC in a semi-mature state in the synovium. We have adapted a method previously developed in our laboratory to investigate the interactions of DC and T cells in JIA. Methods: Human monocyte derived DC grown from SF from children with JIA or peripheral blood of healthy controls, were infected with adenoviral constructs (E1E3-deleted) and then matured. CFSE- labelled T cells were cultured with either autologous DC (adenoviral infected or control) and stimulated with plate bound anti-CD3 or PHA, or were seeded with allogeneic DC. T cell proliferation was measured by CFSE dilution using flow cytometry.