Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
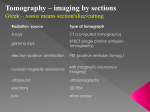
Optical Coherence Tomography and Advanced Fundus Imaging ©Gillian J. McLellan, BVMS, PhD, DECVO, DACVO, DVOphthal, MRCVS Assistant Professor in Comparative Ophthalmology University Of Wisconsin-Madison Objectives: 1) To provide an overview / review of the theoretical basis of confocal Laser Scanning Ophthalmoscopy (cLSO) and Optical Coherence Tomography (OCT) 2) To evaluate and discuss the practical clinical and research applications of cLSO and OCT in comparative ophthalmology I. Introduction: Advanced Imaging of the Ocular Fundus Confocal Laser Scanning Ophthalmoscopy (cLSO) and Optical coherence tomography (OCT) are non-invasive, non-contact optical imaging techniques capable of producing high resolution images of the retina and optic nerve head. These images provide information that is useful for following the progression and / or resolution of posterior segment disease longitudinally. Clinical investigation of disorders of the human fundus, including maculopathies and glaucoma, increasingly utilizes a “multimodal imaging” approach. While many of these advanced imaging techniques remain within the research domain in other species, as their cost progressively declines, veterinary ophthalmologists should be familiar with these technologies and their limitations. II. Confocal laser scanning ophthalmoscopy, first described in the 1980s, provides detailed, high resolution images of the fundus.[1] The laser is projected into the eye as a narrow beam, typically occupying just 1 mm of the pupil. As this leaves a large area of the pupil available for the reflected light from the fundus to pass through, imaging low light intensities is possible. Capturing images through a confocal aperture, essentially a “pinhole effect”, greatly enhances contrast. Such a narrow illumination beam can also be positioned to minimize the detrimental, lightscattering effect of opacities in the ocular media.[2] The laser is typically directed in a raster pattern (i.e. an x-y matrix of parallel lines), providing 2D images. The light is monochromatic and resulting images are also monochromatic, although pseudo-color mapping may be produced by instrument software. By varying the wavelength of the laser used, imaging can be carried out at those wavelengths that give most information on structures of interest, for example, by using an infrared laser to image structures deep in the fundus. When cLSO laser of very specific wavelengths (e.g. blue to excite fluorescein, or near infra-red for indocyanine green) are combined with specific barrier filters, it becomes possible to visualize fluorescent-labelled cells in the retina in vivo; angiographic studies are enhanced and fundus III. IV. auto-fluorescence can be documented in vivo (e.g. lipofuscin within the RPE or Bruch’s membrane).[3] Various modifications of cLSO technology have led to instruments (some combining multiple imaging modalities) that can provide different, often complementary, information about structure or physiologic properties of the fundus. The Heidelberg Retinal Tomograph (HRT) o provides detailed structural information that has been widely used to study optic nerve head topography longitudinally in human glaucoma patients.[4] Fundus Autofluorescence (FAF) o FAF imaging, first reported in the mid-1990s,[5] is now widely utilized in the investigation of macular diseases in human patients. o A blue laser optimally excites the autofluorescence of lipofuscin and is combined with a broad band pass barrier filter with short wavelength cut-off at about 520nm. o As in conventional fluorescein angiography, intrinsic fluorescence of the tapetum complicates cLSO imaging and auto-fluorescence detection. Presence of this highly reflective structure also impacts the quality of cLSO images by increasing back-scatter. o However, fundus autofluorescence imaging is still of value in tapetal species, as demonstrated by the ability of a prototype cLSO to detect and track the accumulation of autofluorescent lipopigment in dogs with vitamin E deficiency retinopathy,[6] o Imaging of FAF has also been applied to mouse models of retinal disease.[7]This modality is now often incorporated in commercially available fundus imaging platforms, e.g. the Heidelberg Spectralis HRA + OCT (see below).[8] o Additional modifications to cLSO technology include wide-field fundus imaging. In addition, a number of instruments (based on both cLSO and OCT platforms) are now available that incorporate the Doppler principle, allowing ocular blood flow to be studied. Optical Coherence Tomography (OCT) technology, first developed in the 1990s, now allows the acquisition of 3D data sets that provide exquisitely detailed cross-sectional images, approaching in vivo histopathology. [9-12] Modifications in OCT technology allow high resolution imaging of anterior segment structures as well, including the cornea and anterior chamber angle.[13-17] OCT Technology: The principle of operation of OCT, low coherence interferometry, is broadly comparable to ultrasonography, except that it uses light rather than sound. OCT uses the reflectivity of light waves to produce detailed cross-sectional images of ocular tissues. Unlike ultrasonography, which requires direct contact between probe and tissues or between probe, coupling medium and tissues, OCT does not require any contact with the eye (thus avoiding the potential for tissue compression and/or distortion) and it allows measurement of structures and distances on the sub- 10 micron scale, versus the 100micron scale of all but the highest-resolution ultrasonography. OCT systems combine an interferometer with a low coherence light source. The optical beam is split and sent to both the sample (i.e. tissue of interest) and a reference arm (typically a mirror). The light reflected by sub-surface features of the tissue is collected by an interferometer. Low coherence optical interferometry involves detection and evaluation of the interference pattern of light reflected from the reference arm interacting with backscattered, reflected light from the tissues of interest. The information obtained about depth and intensity of light reflected from a sub-surface feature is, in turn, utilized to determine spatial dimensions and location of structures within the tissue of interest. These intensity profiles (the axial or A-scans) are then laterally combined to create a transverse, detailed crosssectional image. [9, 11] The first widely used commercial OCT system was the Stratus OCT 3 (Carl Zeiss Meditec, Inc.). This system uses time domain (TD-OCT) technology in which the position of the reference mirror is changed and reflected intensity signals are detected from the sample at different depths, sequentially, based on “time of flight” / echo time delay. Since the signals gathered are time-encoded, the system is referred to as a time domain. Newer systems use broadband light sources and gather all backscattered frequencies simultaneously, using a spectrometer as the reference mirror remains stationary.[18-20]. The signal is then analyzed using Fourier analysis, a mathematical transformation in which spatial frequencies are processed to isolate individual components of compound waveforms. This method enables recognition of patterns and mapping of the form of objects, essentially expressing data as a frequency spectrum, with each frequency corresponding to a different tissue depth. These systems are referred to as spectral domain (SD-OCT) or Fourier domain (FD-OCT). Axial resolution and scan acquisition speed are both dramatically improved with SD-OCT. For example, TD-OCT systems may capture 512 A-scans in 1.28 seconds and provide an axial resolution of 10 microns. In contrast SDOCT systems generally capture many more A-scans in a fraction of a second (a rate of 20,000 - >70, 000 per second in the latest instruments) and have an axial resolution of ~ 2-5µm (transverse resolution is “only” ~ 10-15µm). The higher resolution and denser sampling of SD-OCT increase its diagnostic utility, allowing detection of smaller, more subtle morphologic changes and rapid collection of 3D data sets. The longer scan acquisition time of TD-OCT means that motion artifact can be a problem, even with relatively small ocular movements. Motion artifacts are still possible with SD-OCT but the faster scan time can reduce their frequency. In animal subjects, if quantitative measurement of tissue thicknesses are needed, heavy sedation or general anesthesia are generally required to ensure that the subject is adequately immobilized to limit motion artifact. In recent years, a number of different commercially available instruments have entered (and left) the market. These instruments are reviewed elsewhere [11, 12, 21]. Rapid developments in OCT technology mean that the list of available instruments is likely to change markedly over a relatively short span of just a few years. This rapid evolution may work in favor of veterinary clinicians! V. Pathology, Longitudinal studies and Reproducibility/ Reliability The distinct layers, visible as alternating bright-dark signals, in cross-sectional images of the retina obtained by OCT in vivo, can be correlated with retinal layers that are histologically identifiable on light microscopy.[12, 22-27] The number of distinct retinal “layers” that are routinely detectable on OCT images varies with species and instrument (cat retina shown below). Optical coherence tomography can provide valuable information regarding progression or resolution of diseases or injuries. The location, progression and/or resolution of retinal pathology can be followed longitudinally. Posterior segment lesions identified on ophthalmoscopy and/or fundus photography can be better characterized with OCT, which more clearly identifies which retinal layers are involved[28, 29]. Reproducibility and reliability are central to the use of OCT in longitudinal studies and have been demonstrated in a variety of macular and optic nerve indications in humans and in animal models [30-34] Reproducibility of results depends on understanding the nature of artifacts that can affect quantitative and qualitative assessment of the OCT data .[35] It is possible to acquire high quality scans in most species but the range of normal variation within differing species has not been well-defined and reproducibility of measurements must be determined for each subject population and instrument. VI. In longitudinal studies, the effects of age on thickness values must be taken into consideration. For example, in humans, RNFL thickness parameters decreased significantly with increasing age.[36] This effect of age may be less of a concern in short term studies in laboratory animals. However, in clinical practice, as many of the animals that present with retinal or optic nerve disease are middle aged or order, age-matched control animals should be evaluated concurrently, if possible. Although no significant age-related decline in mean RNFL thickness value was identified within a cohort of 16 normal cats ranging in age from 6 months to 6 years,[37] the potential for an effect of aging should still be considered when conducting long-term longitudinal studies. Deriving quantitative measurements from OCT instruments is hindered by software algorithm errors in detecting the edges of the distinct retinal layers (segmentation). These segmentation errors occur in scans of human eyes as well in other species and arise with similar frequency with each of the different OCT instruments. Fortunately, most instruments have software features that allow these manual corrections to be made and several also have 3-D and en face visualization features to facilitate qualitative assessments. Manual segmentation methods to derive optic nerve head and other structural indices have been developed for several species, as have custom segmentation algorithms. Practicalities of Image Acquisition in Animals: Globe immobilization, alignment and pupil dilation o Movement artifact should be minimized. In addition, angle of scanning can impact scan quality and quantitative measures. Options to help maintain a central, immobile eye for scanning include neuromuscular blockade,[38] retrobulbar saline injections, or retrobulbar local anesthetic block. [39] Manual rotation and fixation of the globe to facilitate scanning may be achieved with forceps or atraumatic conjunctival clip electrodes. [40] A combination of ketamine and xylazine provides optimal scanning conditions in cats. o Some instruments’ software packages offer an “alignment tool” that can compensate for changes in blood vessel orientation. The latter is of great importance during longitudinal studies to detect changes in RNFL thickness values for different quadrants or sectors of the peripapillary region, particularly as retinal blood vessels tend to be colocalized with thicker bundles of ganglion cell axons.[41] o Although it may not be necessary for scanning in larger species, application of a mydriatic, such as 0.5-1% tropicamide, is generally recommended (and is necessary for rodents) Clear ocular Media o Even minimal cataract, corneal opacity, inflammatory cells, flare or hemorrhage within aqueous or vitreous can compromise the image quality, resulting in areas of signal drop-out. Remember that OCT VII. is an optical imaging technique, and opacity may even preclude image acquisition. Corneal Hydration o Corneal desiccation should be avoided as this will negatively impact optical clarity of the cornea and scan quality.[42] o Frequent application of a topical wetting agent (e.g. balanced salt solution, or 0.5% carboxymethylcellulose) is helpful. o When imaging multiple subjects of the same species, perhaps the best solution is to use plano, rigid gas permeable contact lenses that have been manufactured to conform to the approximate corneal curvature and diameter of the particular species to be imaged. Combination with other Test Procedures: o In studies that collect multiple structural and functional measures, e.g. ultrasonography, fundus or gonio- photography and electrophysiology, care should be taken during and between procedures to avoid any corneal drying or epithelial surface damage (see above). o Consider separating studies into different sessions depending on the compatibility of procedures. For example, as this is an optical imaging technique, any electrophysiological tests should be conducted prior to OCT imaging. However, the corneas could potentially be compromised by prior application of ERG contact lens electrodes or drying during the ERG procedure, and image quality can suffer. o When evaluating ONH parameters in glaucoma subjects, intraocular pressure (IOP) should be measured prior to and at the conclusion of the scanning session, taking into potential effects of mydriatics on IOP. [43] If possible, IOP should be within the normal range when scans are acquired to limit corneal edema and reversible “cupping” due to tissue compliance that can both confound quantification of ONH morphologic parameters. [44] Species-specific considerations: OCT scanning can be accomplished in a wide variety of animal species. However, each species presents its own challenges [12]: Dogs and cats o The presence of the reflective tapetum lucidum in these species may require adjustment of scan acquisition parameters to achieve even illumination, especially of the fundus reflectance image. o If a calm, quiet scanning environment is created, minimal use of sedation may be possible, limiting globe rotation. Anterior segment scans – e.g. for corneal pachymetry - may be acquired in unsedated dogs and cats but generally sedation or general anesthesia is required.[45-49] We have found that heavy sedation or general anesthesia has been necessary to acquire good quality fundus scans, free from motion artifact. Various strategies to maintain a stable, central eye position have been discussed previously. o Previous studies in dogs show that whole retinal thickness, RNFL thickness and photoreceptor layer thickness were all greater in the superior (tapetal) than in the inferior (non-tapetal) retina.[38] These authors reported that the thickness measurements on the linear scans often required manual correction and although the RNFL was correctly delineated in approximately 60% of the peri-papillary scans with the automatic software algorithm, the remaining 40% of these scans had inadequate RNFL delineation. The most common clinical application for posterior segment OCT with companion animal species is to assist in the diagnosis and documentation of treatment efficacy or progression of spontaneous or genetic retinal disease, as well as glaucoma. Optical coherence tomography has been used in both dogs and cats in a clinical and research setting to visualize subretinal implants [50-52]; evaluate disease progression and response to therapies in retinal degeneration models and patients , [53-56] and to evaluate the retina and optic nerve head in glaucoma models. [37, 57, 58] Rabbits o The unique ocular anatomy of rabbits poses a challenge in positioning, as the optic nerve head and medullary ray are both situated superiorly. o The rabbit optic nerve head is quite wide and has a very deep central cup. Both can be at or near the maximum size capable of fitting in the scan axial and lateral field of view. o Using software programs designed for human eye structures will likely result in unreliable quantitative values, especially for the RNFL, but most instruments have software features that allow adjustment of segmentation lines and scan circle placement. [44] o Custom measurements can be made using caliper features. o Fewer retinal structures / layers are demarcated by OCT in rabbits, which may in part relate to optical aberration. o The merangiotic vascular pattern of the rabbit fundus limits the number of available landmarks to assist in location of sequential scans in longitudinal studies, [45] due to an absence of retinal blood vessels, except for within the region of the medullary rays. [46] Horses o The equine subject presents many practical challenges to scanning. A portable instrument with a hand-held scan-head will enable scan acquisition in standing, sedated horses. [59, 60] o Globe size may preclude high quality image acquisition using some instruments o At the time of writing, proprietary segmentation algorithms have not yet permitted automated segmentation of equine OCT scans and measurements of anterior and posterior tissue thicknesses have been VIII. conducted manually using the OCT-software caliper function, which can prove very laborious. o Qualitative evaluation of ocular lesions may be valuable in a clinical setting. Rodents o While challenging to scan, the proliferation of mouse models of ocular disease dictates an increasing need for documentation of retinal and optic nerve disease and drug effects in the mouse and rat eye. o The small size of mouse eyes may require use of a corrective lens to compensate for the small eye and extremely short focal length. Several commercially available instruments have specific rodent attachments for just this purpose. For other instruments, a +ve Diopter trial lens can be affixed in front of the scan head, although this may not prove necessary for rats. o Rodents should be anesthetized and positioned in a tube (mice) or on a customized platform or microscope stage. o Duration of the scanning procedure should be minimized as safety of anesthesia may be a concern. Reversible cataract formation may impact outcome if the animal is hypothermic and corneal hydration not diligently maintained by very frequent irrigation with balanced salt solution, or application of a methylcellulose based ophthalmic demulcent together with an appropriately sized plano contact lens or coverslip. [24, 25, 34] Pigs o Use of OCT has been reported previously in this species. [61] o Positioning can be particularly difficult with pigs, including minipigs, given their size, limited neck mobility and ocular conformation, that includes small, deep-set eyes and thick eyelids. However, high quality scans for diagnostic purposes can be acquired. o As with rabbits, the anatomy of the pig eye is sufficiently different from that of humans that instrument analysis software may not accurately detect retinal layers, in ONH scans in particular. Scans must be carefully examined for errors before tabulating quantitative data. Challenges/limitations of OCT Segmentation o Recognition and segmentation of retinal layers is an ongoing issue in OCT image analysis. Each instrument comes with a proprietary segmentation algorithm that delineates retinal layers in a slightly different way and uses different layers to calculate macular thickness values. Thus, instruments cannot necessarily be used interchangeably. Thickness values generated by the software cannot often be compared across instruments or even between different iterations of OCT instruments made by the same company.[35, 6266] Segmentation errors and other errors impacting thickness calculations o The most common segmentation error in animal models is misidentification of the outer retinal layers, whereby the softwaregenerated segmentation line does not follow the contour of the RPE. o Inner retina misidentification is much less common but can occur when debris in the vitreous is reflective enough to be identified as the inner limiting membrane (ILM). o The percentage of scans with segmentation errors is likely to be greater in subjects with a relative lack of pigment in their RPE and choroid. These errors seem to occur with greater frequency in macular cube scans and are an important consideration as subalbinotic and albino animals are commonly utilized in laboratory studies. These errors may in part be due to enhanced visualization of choroidal structure (leading to visualization of additional surfaces) or to increased back-scatter of light. [67] o Off -center fixation, a source of segmentation artifact in humans [35], can occur in animal imaging as a byproduct of eye movement and often results in inaccurate thickness measurements of the area centralis or fovea. In animal subjects operator skill is required to compensate for lack of fixation. o In addition, the circle defining the optic nerve head may not be centered and the line signifying the RNFL layer may be inaccurately drawn. o Different instruments also have different methods of compensating for segmentation errors and other software inaccuracies. While most instruments allow manual segmentation of the line delineating the RPE and RNFL, the time required might be prohibitive. The scan angle should also be evaluated, as tilted rather than “flat” scans indicate that the retinal or ONH surface was not perpendicular to the scanning beam, as is assumed in thickness calculations. [68] All of these image problems affect the numeric thickness values, so if quantitative data is important, inclusion / exclusion criteria need to be defined and each scan carefully evaluated. o While artifacts such as RPE and ILM layer segmentation errors and decentration can often be overcome using the manual adjustment features present in most SD-OCT software, artifacts such as scan registration errors still demand operator skill to identify so that scans can be re-acquired.[69] Most OCT instruments have a circular scan designed to measure RNFL thickness around the optic nerve head. The fixed size (3.4-3.5mm diameter) and round shape of the circle scan is designed for humans and it may not accurately reflect the RNFL anatomy of other species. o Even if the circle is not sized appropriately for the subject species, the images may still allow qualitative assessment and may still be useful for assessing longitudinal change. II. o Thickness values for the RNFL are dependent on the location of the OCT scan circle so registration of scans is essential for thickness measurement reproducibility and longitudinal examination.[70, 71] Opacities in the ocular media, including cataract and corneal lesions can have a profound effect on signal strength and contribute to areas of signal dropout that are often associated with errors in segmentation. Myopia and globe axial length can also affect the incidence of scan artifacts as well as reducing RNFL thickness values and altering thickness sectoral distribution in humans. [72-74] General scan quality, reproducibility and segmentation accuracy may be negatively impacted by ocular diseases such as glaucoma or uveitis. [75] Although in many cases this impact is minor and can be overcome by operator skill so that OCT images of diagnostic quality may still be obtainable, the resulting images should be evaluated carefully for the presence of artifacts and segmentation errors before accepting quantitative data derived from them. Segmentation algorithms o Proprietary segmentation algorithms are subject to ongoing refinement for all of the OCT instruments and a number of research groups are also working on enhancing segmentation algorithm accuracy and thus quantitative analysis via computer-aided grading/ retinal boundary detection methodologies. [76-78] o In some situations, the implications/nuances of the data are better captured by creation of a unique, custom algorithm or manual system of measurement. [79-82] o Manual segmentation, although more subjective and laborious, can be carried out using freely available image analysis software. Significant inter-observer variability generally mandates evaluation of scans by a single, consistent observer. Scan quality o Each OCT instrument has a unique method of assessing scan quality. o Most use a combination of intensity level of the signal along with the uniformity of the signal within a scan. o Scans should be evaluated by the operator during the scanning session, to ensure that scans at least meet pre-determined requirements for signal strength and absence of areas of signal drop out. o Similar to the situation in human glaucoma patients, we have found that mean RNFL thickness in cats is significantly affected by scan signal strength, and this effect should be taken into account when comparing numeric values between scans of different quality.[83, 84] Adaptive Optics Adaptive optics systems, first applied to retinal imaging in the late 1990s,[85] provide the highest resolution images of fundus structures. Using wavefront sensing techniques, similar to that used in astronomy, the aberrations of the eye are measured and can be corrected for using a complex system of lenses and deformable mirrors. With <2µm lateral resolution, these systems make it possible to visualize, in vivo, the photoreceptor mosaic, nerve fibers and flow of blood cells within retinal capillaries. With the use of adaptive optics, it is possible to improve the resolution of a scanning laser ophthalmoscope. Roorda et al (2002) described the first SLO to use adaptive optics to measure and correct the higher order aberrations of the eye.[86] Although mainly restricted to research applications, adaptive optics systems are now available commercially and applicability of a flood-illumination, fundus camera adaptive optics system in cats has been reported in the veterinary literature. [40] Detailed References and Further Reading 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. Webb, R.H. and G.W. Hughes, Scanning laser ophthalmoscope. IEEE Trans Biomed Eng, 1981. 28(7): p. 488-92. Sharp, P.F., et al., The scanning laser ophthalmoscope--a review of its role in bioscience and medicine. Phys Med Biol, 2004. 49(7): p. 1085-96. Seeliger, M.W., et al., In vivo confocal imaging of the retina in animal models using scanning laser ophthalmoscopy. Vision Res, 2005. 45(28): p. 3512-3519. Ferreri, F., P. Aragona, and G. Ferreri, Scanning laser polarimetry and confocal scanning laser ophthalmoscopy: technical notes on their use in glaucoma. Prog Brain Res, 2008. 173: p. 125-38. von Ruckmann, A., F.W. Fitzke, and A.C. Bird, Distribution of fundus autofluorescence with a scanning laser ophthalmoscope. Br J Ophthalmol, 1995. 79(5): p. 407-12. McLellan, G.J., A.S. Halfyard, and F.W. Fitzke. Non-invasive fundus autofluorescence imaging in canine retinal pigment epithelial dystrophy. in Proceedings of the 1997 joint meeting of Br Assoc Vet Ophthalmol, Eur Soc Vet Ophthalmol, Eur Coll Vet Ophthalmol and Internat Soc Vet Ophthalmol. 1997. Charbel Issa, P., et al., Optimization of In Vivo Confocal Autofluorescence Imaging of the Ocular Fundus in Mice and Its Application to Models of Human Retinal Degeneration. Invest Ophthalmol Vis Sci, 2012. 53(2): p. 1066-1075. Castro Lima, V., et al., Simultaneous confocal scanning laser ophthalmoscopy combined with highresolution spectral-domain optical coherence tomography: a review. J Ophthalmol, 2011. 2011: p. 743670. Huang, D., et al., Optical coherence tomography. Science, 1991. 254(5035): p. 1178-81. Hee, M.R., et al., Optical coherence tomography of the human retina. Arch Ophthalmol, 1995. 113(3): p. 325-32. Gabriele, M.L., et al., Optical coherence tomography: history, current status, and laboratory work. Invest Ophthalmol Vis Sci, 2011. 52(5): p. 2425-36. McLellan, G.J. and C.A. Rasmussen, Optical Coherence Tomography for the Evaluation of Retinal and Optic Nerve Morphology in Animal Subjects: Practical Considerations. Veterinary Ophthalmology, 2012. Izatt, J.A., et al., Micrometer-scale resolution imaging of the anterior eye in vivo with optical coherence tomography. Arch Ophthalmol, 1994. 112(12): p. 1584-9. Doors, M., et al., Value of optical coherence tomography for anterior segment surgery. J Cataract Refract Surg, 2010. 36(7): p. 1213-29. Konstantopoulos, A., P. Hossain, and D.F. Anderson, Recent advances in ophthalmic anterior segment imaging: a new era for ophthalmic diagnosis? Br J Ophthalmol, 2007. 91(4): p. 551-7. Mireskandari, K., et al., Anterior segment imaging in pediatric ophthalmology. J Cataract Refract Surg, 2011. 37(12): p. 2201-10. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. Almazan, A., et al., Iridocorneal angle measurements in mammalian species: normative data by optical coherence tomography. Veterinary Ophthalmology, 2013. 16(2): p. 163-166. Wojtkowski, M., et al., In vivo human retinal imaging by Fourier domain optical coherence tomography. J Biomed Opt, 2002. 7(3): p. 457-63. Wojtkowski, M., et al., Real-time in vivo imaging by high-speed spectral optical coherence tomography. Opt Lett, 2003. 28(19): p. 1745-7. Townsend, K.A., G. Wollstein, and J.S. Schuman, Imaging of the retinal nerve fibre layer for glaucoma. Br J Ophthalmol, 2009. 93(2): p. 139-43. Kiernan, D.F., W.F. Mieler, and S.M. Hariprasad, Spectral-domain optical coherence tomography: a comparison of modern high-resolution retinal imaging systems. Am J Ophthalmol, 2010. 149(1): p. 18-31. Drexler, W. and J.G. Fujimoto, State-of-the-art retinal optical coherence tomography. Prog Retin Eye Res, 2008. 27(1): p. 45-88. Ruggeri, M., et al., In vivo three-dimensional high-resolution imaging of rodent retina with spectraldomain optical coherence tomography. Invest Ophthalmol Vis Sci, 2007. 48(4): p. 1808-14. Huber, G., et al., Spectral domain optical coherence tomography in mouse models of retinal degeneration. Invest Ophthalmol Vis Sci, 2009. 50(12): p. 5888-95. Knott, E.J., et al., Spatial correlation of mouse photoreceptor-RPE thickness between SD-OCT and histology. Exp Eye Res, 2011. 92(2): p. 155-60. Yamauchi, Y., et al., Biological activity is the likely origin of the intersection between the photoreceptor inner and outer segments of the rat retina as determined by optical coherence tomography. Clin Ophthalmol, 2011. 5: p. 1649-53. Spaide, R.F. and C.A. Curcio, Anatomical correlates to the bands seen in the outer retina by optical coherence tomography: literature review and model. Retina, 2011. 31(8): p. 1609-19. Rodarte-Almeida, A.C.V., et al., Retinal dysplasia in American pit bull terriers – phenotypic characterization and breeding study. Veterinary Ophthalmology, 2016. 19(1): p. 11-21. Rauscher, F.G., et al., Optical Coherence Tomography as a Diagnostic Tool for Retinal Pathologies in Avian OphthalmologyOCT for Diagnosis of Avian Retinal Pathologies. Investigative Ophthalmology & Visual Science, 2013. 54(13): p. 8259-8269. Mwanza, J.C., et al., Reproducibility of peripapillary retinal nerve fiber layer thickness and optic nerve head parameters measured with cirrus HD-OCT in glaucomatous eyes. Invest Ophthalmol Vis Sci, 2010. 51(11): p. 5724-30. Chin, E.K., et al., Reproducibility of Macular Thickness Measurement Among Five OCT Instruments: Effects of Image Resolution, Image Registration, and Eye Tracking. Ophthalmic Surg Lasers Imaging, 2012. 43(2): p. 97-108. Leung, C.K., et al., Retinal Nerve Fiber Layer Imaging with Spectral-Domain Optical Coherence Tomography A Prospective Analysis of Age-Related Loss. Ophthalmology, 2012. Chiu, S.J., et al., Validated automatic segmentation of AMD pathology including drusen and geographic atrophy in SD-OCT images. Invest Ophthalmol Vis Sci, 2012. 53(1): p. 53-61. Gabriele, M.L., et al., Reproducibility of spectral-domain optical coherence tomography total retinal thickness measurements in mice. Invest Ophthalmol Vis Sci, 2010. 51(12): p. 6519-23. Ho, J., et al., Assessment of artifacts and reproducibility across spectral- and time-domain optical coherence tomography devices. Ophthalmology, 2009. 116(10): p. 1960-70. Sung, K.R., et al., Effects of age on optical coherence tomography measurements of healthy retinal nerve fiber layer, macula, and optic nerve head. Ophthalmology, 2009. 116(6): p. 1119-24. Seo, K., et al. SD-OCT Imaging of the Retina and Optic Nerve in Normal and Glaucomatous Cats in 2010 Annual Meeting Assoc Res Vis Ophthalmol 2010. Fort Lauderdale, FL. Hernandez-Merino, E., et al., Spectral domain optical coherence tomography (SD-OCT) assessment of the healthy female canine retina and optic nerve. Vet Ophthalmol, 2011. 14(6): p. 400-5. Schuman, J.S., et al., Optical coherence tomography and histologic measurements of nerve fiber layer thickness in normal and glaucomatous monkey eyes. Invest Ophthalmol Vis Sci, 2007. 48(8): p. 364554. Rosolen, S.G., et al., Cellular-resolution in vivo imaging of the feline retina using adaptive optics: preliminary results. Vet Ophthalmol, 2010. 13(6): p. 369-76. Hood, D.C., et al., Blood vessel contributions to retinal nerve fiber layer thickness profiles measured with optical coherence tomography. J Glaucoma, 2008. 17(7): p. 519-28. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. Stein, D.M., et al., Effect of corneal drying on optical coherence tomography. Ophthalmology, 2006. 113(6): p. 985-91. Gomes, F.E., et al., Effects of unilateral topical administration of 0.5% tropicamide on anterior segment morphology and intraocular pressure in normal cats and cats with primary congenital glaucoma. Vet Ophthalmol, 2011. 14 Suppl 1: p. 75-83. Strouthidis, N.G., et al., Effect of acute intraocular pressure elevation on the monkey optic nerve head as detected by spectral domain optical coherence tomography. Invest Ophthalmol Vis Sci, 2011. 52(13): p. 9431-7. Alario, A.F. and C.G. Pirie, A spectral-domain optical coherence tomography device provides reliable corneal pachymetry measurements in canine eyes. Veterinary Record, 2013. 172(23): p. 605. Alario, A.F. and C.G. Pirie, Central corneal thickness measurements in normal dogs: a comparison between ultrasound pachymetry and optical coherence tomography. Veterinary Ophthalmology, 2014. 17(3): p. 207-211. Alario, A.F. and C.G. Pirie, Intra and inter-user reliability of central corneal thickness measurements obtained in healthy feline eyes using a portable spectral-domain optical coherence tomography device. Veterinary Ophthalmology, 2013. 16(6): p. 446-450. Tsai, S., et al., The effect of topical latanoprost on anterior segment anatomic relationships in normal dogs. Veterinary Ophthalmology, 2013. 16(5): p. 370-376. Famose, F., Assessment of the use of spectral domain optical coherence tomography (SD-OCT) for evaluation of the healthy and pathological cornea in dogs and cats. Veterinary Ophthalmology, 2014. 17(1): p. 12-22. Volker, M., et al., In vivo assessment of subretinally implanted microphotodiode arrays in cats by optical coherence tomography and fluorescein angiography. Graefes Arch Clin Exp Ophthalmol, 2004. 242(9): p. 792-9. Güven, D., et al., Implantation of an inactive epiretinal poly(dimethyl siloxane) electrode array in dogs. Exp Eye Res, 2006. 82(1): p. 81-90. Gekeler, F., et al., Assessment of the posterior segment of the cat eye by optical coherence tomography (OCT). Vet Ophthalmol, 2007. 10(3): p. 173-8. Lheriteau, E., et al., The RPGRIP1-deficient dog, a promising canine model for gene therapy. Mol Vis, 2009. 15: p. 349-61. Cideciyan, A.V., et al., In vivo dynamics of retinal injury and repair in the rhodopsin mutant dog model of human retinitis pigmentosa. Proc Natl Acad Sci U S A, 2005. 102(14): p. 5233-5238. Beltran, W.A., et al., Gene therapy rescues photoreceptor blindness in dogs and paves the way for treating human X-linked retinitis pigmentosa. Proceedings of the National Academy of Sciences, 2012. 109(6): p. 2132-2137. Hoffmann, I., et al., Canine multifocal retinopathy in the Australian Shepherd: a case report. Veterinary Ophthalmology, 2012. 15: p. 134-138. Schallek, J.B., et al., Retinal Intrinsic Optical Signals in a Cat Model of Primary Congenital Glaucoma. Invest Ophthalmol Vis Sci, 2012. Grozdanic, S.D., et al., Recovery of canine retina and optic nerve function after acute elevation of intraocular pressure: implications for canine glaucoma treatment. Vet Ophthalmol, 2007. 10 Suppl 1: p. 101-7. Pirie, C.G., et al., Manual corneal thickness measurements of healthy equine eyes using a portable spectral-domain optical coherence tomography device. Equine Veterinary Journal, 2014: p. n/a-n/a. Pinto, N.I. and B.C. Gilger, Spectral-domain optical coherence tomography evaluation of the cornea, retina, and optic nerve in normal horses. Veterinary Ophthalmology, 2014: p. n/a-n/a. Gekeler, F., et al., Compound subretinal prostheses with extra-ocular parts designed for human trials: successful long-term implantation in pigs. Graefes Arch Clin Exp Ophthalmol, 2007. 245(2): p. 23041. Savini, G., et al., Comparison of Optic Nerve Head Parameter Measurements Obtained by Timedomain and Spectral-domain Optical Coherence Tomography. J Glaucoma, 2012. Sung, K.R., et al., Comparison of retinal nerve fiber layer thickness measured by Cirrus HD and Stratus optical coherence tomography. Ophthalmology, 2009. 116(7): p. 1264-70, 1270 e1. Knight, O.J., et al., Comparison of retinal nerve fiber layer measurements using time domain and spectral domain optical coherent tomography. Ophthalmology, 2009. 116(7): p. 1271-7. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. 82. 83. 84. 85. 86. Leung, C.K., et al., Retinal nerve fiber layer imaging with spectral-domain optical coherence tomography: a variability and diagnostic performance study. Ophthalmology, 2009. 116(7): p. 125763, 1263 e1-2. Sull, A.C., et al., Comparison of spectral/Fourier domain optical coherence tomography instruments for assessment of normal macular thickness. Retina, 2010. 30(2): p. 235-45. Chong, G.T., et al., Abnormal foveal morphology in ocular albinism imaged with spectral-domain optical coherence tomography. Arch Ophthalmol, 2009. 127(1): p. 37-44. Hong, S., C.Y. Kim, and G.J. Seong, Adjusted peripapillary retinal nerve fiber layer thickness measurements based on the optic nerve head scan angle. Invest Ophthalmol Vis Sci, 2010. 51(8): p. 4067-74. Han, I.C. and G.J. Jaffe, Evaluation of artifacts associated with macular spectral-domain optical coherence tomography. Ophthalmology, 2010. 117(6): p. 1177-1189 e4. Gabriele, M.L., et al., Optical coherence tomography scan circle location and mean retinal nerve fiber layer measurement variability. Invest Ophthalmol Vis Sci, 2008. 49(6): p. 2315-21. Vizzeri, G., et al., Effect of signal strength and improper alignment on the variability of stratus optical coherence tomography retinal nerve fiber layer thickness measurements. Am J Ophthalmol, 2009. 148(2): p. 249-255 e1. Ho, J., et al., Clinical assessment of mirror artifacts in spectral-domain optical coherence tomography. Invest Ophthalmol Vis Sci, 2010. 51(7): p. 3714-20. Kang, S.H., et al., Effect of myopia on the thickness of the retinal nerve fiber layer measured by Cirrus HD optical coherence tomography. Invest Ophthalmol Vis Sci, 2010. 51(8): p. 4075-83. Rauscher, F.M., et al., Myopia affects retinal nerve fiber layer measurements as determined by optical coherence tomography. J Glaucoma, 2009. 18(7): p. 501-5. Asrani, S., et al., Optical coherence tomography errors in glaucoma. J Glaucoma, 2010. 19(4): p. 23742. Yang, Q., et al., Automated layer segmentation of macular OCT images using dual-scale gradient information. Opt Express, 2010. 18(20): p. 21293-307. Hu, Z., et al., Automated segmentation of 3-D spectral OCT retinal blood vessels by neural canal opening false positive suppression. Med Image Comput Comput Assist Interv, 2010. 13(Pt 3): p. 3340. Debuc, D.C., et al., Improving image segmentation performance and quantitative analysis via a computer-aided grading methodology for optical coherence tomography retinal image analysis. J Biomed Opt, 2010. 15(4): p. 046015. Strouthidis, N.G., et al., Longitudinal change detected by spectral domain optical coherence tomography in the optic nerve head and peripapillary retina in experimental glaucoma. Invest Ophthalmol Vis Sci, 2011. 52(3): p. 1206-19. Roberts, M.D., et al., Correlation between local stress and strain and lamina cribrosa connective tissue volume fraction in normal monkey eyes. Invest Ophthalmol Vis Sci, 2010. 51(1): p. 295-307. Sigal, I.A. and C.R. Ethier, Biomechanics of the optic nerve head. Exp Eye Res, 2009. 88(4): p. 799807. DeBuc, D.C., A Review of Algorithms for Segmentation of Retinal Image Data Using Optical Coherence Tomography, in Image Segmentation, P.-G. Ho, Editor 2011, InTech. p. 15-54. Wu, Z., et al., Factors Associated with Variability in Retinal Nerve Fiber Layer Thickness Measurements Obtained by Optical Coherence Tomography. Ophthalmology, 2007. 114(8): p. 15051512. Sung, K.R., et al., Scan quality effect on glaucoma discrimination by glaucoma imaging devices. Br J Ophthalmol, 2009. 93(12): p. 1580-4. Liang, J., D.R. Williams, and D.T. Miller, Supernormal vision and high-resolution retinal imaging through adaptive optics. J Opt Soc Am A Opt Image Sci Vis, 1997. 14(11): p. 2884-92. Roorda, A., et al., Adaptive optics scanning laser ophthalmoscopy. Opt. Express, 2002. 10(9): p. 405412.