Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
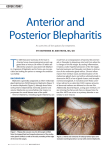
Dear Eye Care Professionals, We are writing to you today to bring to your attention a fact that is slowly and agonisingly ruining our lives. It is a fact that has led to undue pain, suffering, and debilitation for men and women all over the country. The simple fact is this: Treatment of dry eye (keratoconjunctivitis sicca) in Australia lags far behind the standards in much of North America and Europe. Eye care professionals in Australia are failing dry eye patients every single day by not adopting or pursuing the best-practice treatments currently emerging or established in the global medical community. This is not an opinion. It is a fact. Many of us have spent thousands of dollars visiting countless specialists who, after lengthy waiting periods, have often dismissed or ignored our symptoms and clinical picture, offering minimal, out-dated, ineffective treatments not specific to our condition. It’s depressing enough to suffer with such a chronic and embarrassing disease. To receive no sympathy, along with repeatedly hearing the line, ‘It’s all in your head’—it’s demoralising. We feel it is time to do something about it instead of sitting back, allowing our symptoms to worsen, and wasting valuable time and money with archaic treatments. We often find ourselves educating the doctors we pay to see, who then find it offensive that we know more about dry eye than they do. We say the above not to demean our eye specialists, but rather in the hope that it will send a message to all health care professionals that we need additional help—that there are more sophisticated treatment options than the usual ‘plug and drop’. As dry eye sufferers, we suffer from escalating anxiety and stress, debilitating physical pain, and an overall decrease in quality of life. It affects our ability to drive, use a computer, read, work outdoors, or do any fine detail work. This, in turn, affects our ability to support ourselves in employment or even enjoy basic recreational and social activities, which has a profoundly negative impact on our mental health. We understand that co-morbid diseases play a role in many cases and that there is no proven cure for each different type of ocular surface disease, but we believe there are better supportive treatments available to help us cope better on a day-to-day basis instead of suffering under constant duress. Many of us are members of the rapidly growing online dry eye support community. We have immersed ourselves in the many personal opinions, clinical reports, reviews, and well-received studies supporting the use of new, advanced, and even experimental treatments for dry eye. These treatments can help patients in Australia who are unresponsive or contraindicated to the conventional treatments in this country. We hope the following information will provide some valuable insight into the emerging and established treatments currently used in other countries, particularly the United States, with the hope that they may become available to us sooner rather than later. Every day that passes is a day we lose to this malady. We cannot delay this any longer, and we need your help. The Problem with Current Protocols Dry eye is a multi-factorial condition and must be treated as such. There is no one-size-fits-all treatment for us. Unfortunately, it seems very few doctors are willing to take a personal interest in managing the unique attributes of each of our specific cases, or do anything to help us research different therapies to improve our symptoms. We feel forgotten because our disease is not properly understood or extensively researched in this country. The consensus seems to be simply, ‘As long as you can see, then we can’t do anything more.’ This isn’t good enough—in fact, it is a dangerous and irresponsible practice. Many of us have also faced the problem of dry-eye-induced epiphora. Because of the lack of attention and consideration given to dry eye, the root of this epiphora can be (and has been) missed. This has led to DCR (dacryocystorhinostomy) surgeries being performed when they, in reality, should have been contraindicated. The result is the return of the original dry eye, compounded with the increased drainage caused by DCR—in other words, the most painful and severe dry eye imaginable. This is even worse if the puncta have been over-dilated. The problems with protocols for epiphora are another letter entirely, however. Current first-line treatments typically prescribed to dry eye patients in Australia are artificial tears, steroids, punctual plugs, basic lid hygiene, and (rarely) scleral lenses. While artificial tears may provide short-term relief, they do not address underlying pathophysiology, and in some cases can cause worsening of symptoms rather than improvement due to the lack of investigation into the original cause of the dry eye. In addition, many over-the-counter drops contain harmful preservatives, which patients are not instructed to avoid.1 Even if they are preservative-free, dosage of any drops in a chronic fashion can be detrimental rather than beneficial to the natural tear film structure and corneal epithelium. Prescription steroids and mass cell stablizers used to combat inflammation in vulnerable dry eye patients such as Flarex, FML, and Patanol are preserved with benzalkoniumchloride (BAK), a chemical used in detergents. BAK can puncture the corneal epithelium, denature corneal protein, and cause irreversible damage to the eye. Steroid drops are usually prescribed with little concern for their toxicity to the ocular surface, and can cause significant worsening of symptoms in some cases, even in the short term.2 There are many tests and equipment that can be used to evaluate a dry eye patient’s specific conditions and severity, such as fluorescein breakup time measurement, meibography, Schirmer’s test, TearLab osmolarity, evaluation of the lid margin, and bacterial analysis to determine staphylococcal/seborrhoeic dermatitis—most of which are not routinely performed in Australia. Meibomian Gland Dysfunction and Blepharitis Regardless of whether a patient has an aqueous tear deficiency (ATD) or not, complaints of dry eye symptoms are usually accompanied by mild, moderate or severe meibomian gland dysfunction (MGD), a common, under-diagnosed disease of the oil producing glands in the eyelid. Meibomian gland dysfunction can occur for various reasons, most commonly blepharitis.3 If there is an ATD, this prevents proper protection for the eyelids, causing a build up of bacteria on the lid margin. The result is a combination of both ATD and MGD, an unstable tear film culminating in dry eye syndrome (DES). As you hopefully already know, blepharitis takes on two forms: anterior, which occurs when a build-up of excess oil produced by the meibomian glands develops on the outer lids creating a breeding ground for bacteria; and posterior, which develops when the meibomian glands become inflamed and a thick paste-like meibum is secreted, or no oil is produced at all. This lack of oil on the tear film causes the middle aqueous layer to evaporate, resulting in a condition called ‘evaporative dry eye’. Each type requires different treatments, and only anterior blepharitis seems to be the focus in Australia. Posterior blepharitis is far more difficult to treat, but there are now new technologies available that are proving to combat it. Instructing patients with ATD and MGD to chronically dose themselves hourly (or up to four times an hour) with artificial tears and inserting punctal plugs isincorrect and potentially harmful. Retaining abnormal tears with high concentrations of pro-inflammatory cytokines can cause further inflammation.4 MGD must be treated vigorously first before punctal plugs are used. It is estimated that up to 80% of dry eye sufferers have some form of MGD on top of ATD, which begs the question, ‘Why are the majority of treatments only aimed at treating the aqueous layer?’ Many of us have been into numerous ophthalmologists suites, with high hopes and a price tag to match, only to find out they don’t even know what a meibomian gland is! This is absolutely appalling and entirely unacceptable. New Potential Solutions Meibomian Gland Related Treatments Current treatment options advised for blepharitis and meibomian gland dysfunction in Australia are lid hygiene, warm compress, eyelid massage, and oral supplementation of omega-3 fatty acids. While these may help patients with mild MGD, studies on omega-3s are largely equivocal. Patients with chronic MGD, moderate to severe evaporative dry eye, and even aqueous deficient patients can benefit from newer much more effective treatment options. LipiFlow: This is a thermal pulsation system that bypasses the tarsal plate to directly apply heat to the meibomian glands and their contents, allowing for easier flow of oil.5 Dr. Jim Kokkinakis at The Eye Practice in Sydney CBD rented the equipment on a trial basis in June 2012. Following this news, he immediately began taking frantic appointments from over 40 desperate patients, from all over Australia and even New Zealand, indicating our widespread desperation and the travel-burden required for better treatment.[6,7] The use of LipiFlow to treat MGD is vastly superior to home remedies such as lid massage and warm compress, of which the latter can be dangerous due to potential overheating. Currently, only the Wilson Eye Center in Bundaberg, QLD offers LipiFlow for it's dry eye patients. Meibomian Gland Probing (MGP): Dr. Colin Chan at the Vision Eye Institute in Bondi, New South Wales, is one of the few doctors in Australia that offers MGP. The procedure and equipment were developed by Dr. Steven L. Maskin in Tampa, Florida.8 It has been proven to be highly successful as an initial treatment to unclog blocked meibomian glands along the lid margin. In chronic MGD patients, inflammation causes periductal fibrosis, and only an MG probe can ‘pop’ open these scars that wrap around the ducts, allowing oil to flow naturally.[9,10,11,12,13] This procedure is widely used across North America and Europe. It has become standard practice to help chronic MGD patients. There is a misconception that probing is ‘dangerous’ or ‘painful’, but, in fact, many patients with MGD find it extremely relieving. Maskin Probes are simple to use, inexpensive, and can be purchased from Rhein Medical or their Australian Distributor, Ellex.14 Meibomian Gland Expression: This is the easiest and most costeffective option to help patients with chronic MGD. As of this writing, we are not aware of any doctors in Australia that utilise meibomian gland expression in their toolbox of treatments for MGD patients. Dr. Malcolm McKellar from Christchurch, New Zealand, has performed this treatment in-office with great success. His eye centre website offers instructional information on how to perform the procedure. The idea is to massage the eyelids with forceps to express solidified contents in the meibomian glands, which will encourage production of newer, thinner secretions. In McKellar’s words: ‘It’s not sexy, but it does work.15 There are adjunct tools developed by doctors in the US such as the Mastrota Paddle and Gulden Expressor Kit, both of which are designed specifically for in-office expression, and are economical and uncomplicated to use. They recommend expression as a first-line, weekly treatment. Subsequent conventional treatments such as Omega-3 supplementation, warm compress, etc., can form part of a wider long-term strategy. Meibomian gland expression is also regularly practiced across North America and Europe. The technique can and should be adopted by all eye care professionals treating patients with MGD.[16,17,18,19] Haemotherapy Related Treatments Autologous Serum Drops: Serum drops are prepared from a patient’s blood and can be used in different solutions (20–100%). It should be prepared under sterile conditions in a certified laboratory unit. It contains several growth factors, vitamin A, and fibronectin, and also has an anti-inflammatory effect. Therefore, it has been beneficial in advanced and severe cases of dry eye.20 Serum drops are usually reserved for patients with significant corneal problems. This is a misguided approach, as many dry eye patients benefit from the non-allergic nature of the drops and also find the properties that help promote a healthy tear film, leading to a reduction in dry eye symptoms. Eye Platelet Rich Plasma (E-PRP): Goblet cell density is low in dry eye patients, particularly in cases of aqueous tear deficiency and cases with chronic inflammation.[21,22] Known as the ‘ball bearings’ of the tear film, it makes sense that, with a deficient goblet cell density, we experience a gritty sensation. Low goblet cell density is also associated with a mucin layer problem in the tear film. Artificial tears do not treat this layer of the tear film. Similar to autologous serum, E-PRP has shown to be highly effective in treating dry eye patients. Clinical studies report significant improvement on lachrymal meniscus and conjunctival hyperaemia and a decrease of corneal fluorescein staining. Post treatment, impression cytology reveals significant increases in conjunctival goblet cells.23 E-PRP has been extensively researched by Dr. Edward Jarka and Dr. John Crane, in St. Louis, Missouri, in the United States. Renowned Australian Optometrist Dr. Brian Holden has also worked with these doctors on this therapy.24 To obtain PRP for therapeutic use, a small amount of blood is collected from the patient. The sample is then centrifuged for several minutes to separate the red blood cells, platelets, and serum. The platelets are then removed and prepared for use in eye drop form. Importantly, when platelets are ‘activated’ (either by coming into contact with collagen, heating to body temperature, or mixing with thrombin), hundreds of antiinflammatory molecules are released into the local tissue environment. While the very complex mechanisms of interaction between these growth factors, cytokines, hormones and other molecules are just beginning to be elucidated, they are proving to work in concert to restore tissue homeostasis in cases of chronic inflammation.[25,26,27,28] In correspondence with Dr. Jarka, he stated: ‘We believe that the concentrated growth factors that are released when the platelets are activated on the ocular surface have the ability to restore the normal cellular structural architecture that may have changed from a number of environmental or internal factors that deplete these components over time. The result is a continuous intracellular and intercellular signalling that culminates into a chronic dry eye. ‘The procedure involves the collection of your blood and concentrating it in a cell separator. We use the Harvest Smart PReP System. We then prepare a concentrate into a solution form to be applied to the eye at least twice a day.29 ‘We have had enough success with this procedure that we now receive referrals from local physicians and ophthalmic surgeons. We have treated people from many states including Oklahoma, Arkansas, Virginia, and an American citizen currently working in Afghanistan. The cause of these dry eyes has usually been from many contributing factors.’ Amniotic Membrane Related Treatments Amniotic Membrane (AM) and ProKera: It is widely regarded that one common theme throughout all dry eye patients, regardless of the type, is that we all suffer from recalcitrant inflammation of the ocular surface. As such, anything that possesses anti-inflammatory actions could help us, and should be investigated. The use of amniotic membrane in ophthalmology dates back to the early 90s, where it was discovered that the foetal wound healing strategy could be applied to the eye to help reduce inflammation and minimize scarring.30 World renowned pioneer Dr. Scheffer Tseng in Miami, Florida, developed the use of AM to heal damaged ocular surfaces on patients with acute chemical burns, Stevens-Johnson Syndrome, and even pterygium removal with very high success rates. Due to this success, Dr. Tseng now treats moderate to severe dry eye patients with a selfretaining contact lens containing AM, called ProKera. ProKera is listed by the FDA as a Class II medical device.31 As per his correspondence, Dr. Tseng has successfully treated patients with dry eye using ProKera. He states: ‘Yes, ProKera can help dry eye patients in several ways. I have used it successfully for them. In short, its potent anti-inflammatory action can surpass steroids and Restasis and more importantly circumvent the potential side effect known to both of them. The membrane also contains abundant nerve growth factor that is known to promote innervations that may help correct the ocular surface deficit caused by dry eye and inflammation so that the neuronal reflex can be improved. The hydration of the membrane instantly helps maintain the preocular tear film stability. For those eyes where the eyelid blinking is incomplete, it also prevents exposure-induced dryness. Once improved, the patient will normally have a “prolonged” period of remission. Because the underlying causes of dry eye are multiple and may not be fully corrected, dry eye can return later on. Nonetheless, the treatment can be repeated.’ Dr. Allan Panzer of Houston, Texas, has also treated dry eye patients with ProKera, claiming it relieved their pain immediately. One of his long-term dry eye patients was interviewed by Fox News in the US, stating, ‘It felt like I took a pain pill.’32 Numerous other ophthalmologists have been using AM for many years to help dry eye patients, such as Dr. Steven Maskin of the Dry Eye and Cornea Treatment Center in Tampa, Florida; Dr. John Hovanesian of the Harvard Eye Associates; and Dr. M. Wang of the Wang Vision Institute in Nashville, Tennessee. While it may be difficult to ship cryopreserved AM from the US, the Centre For Eye Research (CERA) located at the Royal Eye & Ear Hospital in Melbourne has been distributing amniotic membrane tissue every year, primarily in corneal transplant patients.33 Attempting this type of treatment for dry eye is just a matter of harnessing the material for modification for a different purpose. If not used in a self-retaining contact lens, AM can be easily temporarily sutured with nylon stitches or fibrin glue to the eyelid margin for the same effect by covering the ocular surface as a ‘biological bandage’.34 We are excited to see that it appears CERA is organising a study for the development of a therapeutic contact lens to culture and deliver corneal epithelial cells, to be compared to AM transplantation. Amniotic Membrane Extract (AMX): AMX is a novel method of applying amniotic membrane to the eye without the need for surgery or contact lenses. Inventor Dr. Emliano Ghinelli, from Rome, patented the use of lyophilized amniotic membrane for topical application promoting the same biological factors, corneal epithelial regeneration, and inflammation suppression.35 AMX contains an abundance of growth factors, neurotrophins, interleukin antagonists, plus fibronectin and collagen. In correspondence with Dr. Ghinelli, he gave the following statement: ‘As inventor I would certainly recommend you AMX to increase your Conjunctival Goblet Cells Mucin secretion and in this way “hold tighter” the aqueous part of your few tears on your ocular surface. Regarding availability: FDA does not allows AMX to be on the US market yet. On the EU field, AMX its currently under evaluation to have the green light. Regarding ProKera: AM or PROKERA are both clever and innovative ways to approach the same diseases.’ Dr. Kenneth R. Kenyon from the Massachusetts Eye Infirmary has worked closely with Dr. Ghinelli, stating AMX has application in moderate to severe dry eye.[36,37,38,39,40] The use of AMX has also been clinically studied in the US by Dr. Hosam Sheha in Miami, Florida. His studies confirm that: ‘Although one may attribute AMX’s effect in relieving pain to its antiinflammatory action, we suspect that such a rapid action in pain relief might be mediated by a yet unknown anti-pain action that deserves further investigation. Ocular surface inflammation was markedly reduced in all cases after treatment. Although the exact action mechanism remains to be determined, the aforementioned effect may be associated with early delivery of AM’s anti-inflammatory active ingredients, which are retained in AMX.’ [41,42,43] Please view this video on Amniotic Membrane at the recent Hawaii Eye Convention, presented by Dr. Kenneth R. Kenyon. Other Treatment Options Tetracycline: Oral tetracycline exhibits antibacterial, anti-inflammatory and anti-angiogenic properties, and can be used systematically.44 The dosing varies between 20 and 100 mg/day and usually lasts for three months in an intermittent modality. Studies confirm that low dose doxycycline improves Schirmer’s and Tear Break-Up Time Scores (TBUT).45 A common side effect is stomach pain, but many patients have claimed this to be far less than the pain experienced from their dry eye.46 AzaSite: The use of AzaSite (topical azithromycin) has been proven to treat eyelid inflammation in both anterior and posterior blepharitis patients, with results indicating more than 50% effectiveness over conventional lid hygiene and warm compresses therapy.47 The presence of lid margin telangiectasias is commonly overlooked leading to further mis-diagnosis. Many eye doctors do not even perform basic lid eversion tests. AzaSite as well as Lotemax (loteprednol) have also shown to reduce the inflammation in lid wipers commonly seen in patients with lid margin disease.48 Testosterone Eyelid Cream and Drops: This has been studied for over a decade in the US by Dr. David A. Sullivan, Dr. Charles G. Connor, and the now retired Dr. Charles Haines. Transdermal application of 3% testosterone to the eyelid twice a day promotes both tear production and reductions in meibomian gland dysfunction, leading to improved tear film stability. The research has found that testosterone regulates both lacrimal and meibomian glands and direct application to the eyelids allows for direct treatment of both glands.49 When ineffective as an eyelid cream, testosterone can be delivered as an eye drop or even as a sublingual drop.50 Not currently FDA approved, testosterone cream is only used off-label in the US with impressive results in Schirmer’s tests, Ocular Surface Disease Index (OSDI), and contact lens wearing time. Many doctors in the US currently prescribe this cream for their patients, including the renowned Dr. Boxer Wachler in Los Angeles, California, and Dr. Allan Panzer in Houston, Texas.[51,52] Dehydroepiandrosterone (DHEA): Administered in drops, DHEA works along similar principles as testosterone, since we know that androgens play a role in the function of lacrimal and meibomian glands.[53,54] Although DHEA has substantially less androgenic activity than testosterone, a study by C.G. Connor and J. Fender demonstrated that 1% DHEA drops produced improvement in TBUT and Schirmer’s test results. In fact, participants felt that the DHEA drops were more effective at relieving symptoms than either plain artificial tears or 1% testosterone drops.55 Although it’s not registered with the TGA, we can use a compounding pharmacy to produce the medicine for us as long as a prescription is provided. While we’re aware of the potential risks of using a compounding pharmacy, we believe that as long as we choose our pharmacy with care (with the help of our doctors), we can get safe, effective medicine. Lacritin: Early studies into Lacritin as a potential dry eye therapy have been promising. Lacritin is produced by the lacrimal gland, cornea and conjunctiva of the eye as a tear protein that appears to be selectively downregulated in dry eye. Although a tear protein, it helps stimulate creation of the protective three-layer tear film as it flows through tear ducts onto the surface of the eye. It also acts as a shield against inflammation-associated cell death by promoting the health of the ocular surface. Lacritin can be easily and safely produced. The growing research on lacritin is notable for the detail by which lacritin's mechanisms have been explored, and by the collaborative 'Lacritin Consortium' of investigators that have contributed. Researcher Dr. Gordon Laurie of the University of Virginia, Cell Biology department states "New exciting studies from Nancy McNamara's lab at UCSF revealed that lacritin is also effective in dry eye. In a mouse dry eye model, lacritin stimulated tearing, and both reduced inflammation of the lacrimal gland and ocular surface staining. Thus Lacritin appears to address the disease upstream of inflammation". Currently seeking $3 million in funding for human clinical trials. Corporate interest in this research could transcend dry eye treatment around the world forever and provide incomparable profits for investors. In Closing, a Solemn Plea This writing is the culmination of years of experience and research from many individuals, sufferers and advocates alike. We are pleading that you take the time to read our references, gain an understanding into the collective mind of dry eye patients first hand, connect with each other, and bring much needed attention to our plight. We cannot treat ourselves at home. We need your help to have a chance at getting our lives back. None of the aforementioned treatments are regularly practiced in Australia, and we believe they should be. We cannot afford to travel overseas for treatment, as we are already under huge financial pressure because of our horrible dry eye symptoms. Australia has great scientific and medical capacity, and we can overcome any bureaucratic or technological stumbling blocks through the focus, ingenuity, and support of our eye care professionals. The Digital Revolution seems to have caused a new epidemic of Dry Eye Syndrome across the developing globe. An estimated 50 million people in the US alone suffer with dry eye of varying severity and estimates put Australia at around 200,000 sufferers. The potential market for proper dry eye treatments is vast, and most of us are willing to spend whatever it takes and to risk ourselves as guinea pigs in the hope a particular new treatment can provide relief from the agony. If we have this open mind about treating ourselves, why shouldn't our eye care professionals allow us to pursue it? As of October 2012, a very promising drug called Lifitegrast had just completed a Phase III study in the US.56 A small-molecule integrin antagonist designed specifically for the treatment of dry eye, Lifitegrast improved corneal staining scores and the mean discomfort and dryness scores in the 588 patients involved in the study.57 If this type of research was being conducted in Australia, we could have had the opportunity to be among the 588 patients involved in this exciting study, and could be seeing results. We want these opportunities. In Australia, the only promising treatment for blepharitis is being developed by Dr. Stephanie Watson and Dr. Kenneth Ooi at the Save Sight Institute, University of Sydney. Using topical Atorvastatin, studies have shown significant improvement's in symptoms and inflammation. They are currently looking for commercial funding to enable their treatment to become available for sufferers of blepharitis and are hoping to formulate the treatment into a topical eye drop and/or lid cleaning solution. For pharmaceutical companies, the market value for better Dry Eye treatment is worth billions. At this point in time, the only prescription drug available for dry eye patients is Restasis, and in it's first 5 years on the US market (since 2003) sales reached $1.5bn. Unfortunately, many Restasis users have reported side effects, worsening of symptoms and the few that have success only report minimal improvements after 6 months. Many researchers have found more effective methods to treat dry eye, and we are urging our pharmaceutical partners to recognise this unique monopoly market opportunity, to support these new developments through the clinical pipiline and into dry eye patients hands as soon as possible. The severe impact of dry eye is very real to us, not theoretical. It impacts our lives as much as other, better-studied ophthalmological conditions. We want some recognition, and we want the best help available. We’re tired of reading about patients in other countries with easy access to these treatments, fantasizing about the possibilities. The US and Europe are leading the way in helping dry eye patients.58 We must adopt the same strategies, and even form our own innovative methods to counteract this disease before it leads to a spike in mental health problems and disabilities like blindness down the road. We might consider the formation of specialised ‘Dry Eye Clinics’ (similar to Dr. Colin Chan in Bondi or the Dry Eye Center of Arizona), located in each capital city. In this setting, doctors would have access to the correct tear film diagnostic equipment on a regular basis and thus would be able to help patients attain the latest best-practice treatments. Even if it is an intermittent clinic that operates once a month, this is still better than nothing. We would gladly pay to have a few professionals taking an interest in us, helping us try newer more advanced options and monitoring our progress. For further education on Dry Eye, please watch this video recorded at the recent Hawaii Eye Convention 2013.59 If there are any ophthalmologists, optometrists, oculoplastic surgeons, or general practitioners that would be able to help dry eye sufferers try any of these treatment options, please contact us: [email protected]. There are many of us who suffer together, and we rely on each other for hope, support, and solutions. Let us rely on you, too. Thank you for your time and your help, —Dry Eye Sufferers of Australia To Download a Hard Copy of this Letter, please click here. References 1 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2958436/ 2 http://www.ncbi.nlm.nih.gov/pubmed/22529703 3 http://www.iovs.org/content/52/4/2006.full 4 http://www.eyeworld.org/article.php?sid=3059 5 http://www.ncbi.nlm.nih.gov/pubmed/22222996 6 http://www.theeyepractice.com.au/_blog/OptometristSydney/post/LIPIFLOW_Our_First_Impressions_with_treating_Dry_Eye s/ 7 http://eyeworld.org/article.php?sid=6279 8 http://www.modernmedicine.com/modernmedicine/article/articleDetail.js p?id=741058 9 http://www.dryeyezone.com/talk/showthread.php?16457-MeibomianGland-Dysfunction-and-Chalazia-Cured&highlight=probing 10 http://www.eyeworld.org/article-new-devices-for-ocular-surfacedisease 11 http://eyeworld.org/article.php?sid=6212 12 http://eyeworld.org/article.php?sid=5897 13 http://www.healio.com/Optometry/Cornea-ExternalDisease/news/print/primary-care-optometry-news/%7BCF8C52E37DB9-4574-805B-6F09D78B7E05%7D/Aggressive-treatmentsdeveloped-for-meibomian-gland-dysfunction 14 http://www.ellex.com/australia 15 http://www.drmalcolmmckellar.co.nz/meibomian-glandexpression1.html 16 http://www.guldenophthalmics.com/images/MG%20Expressor3.pdf 17 http://bmctoday.net/advancedocularcare/2010/10/article.asp?f=anew-paradigm-for-treating-dry-eye-patients 18 http://www.ocusoft.com/for-eye-care-professionals/surgical/miscsurgical-instruments/mastrota-meibomian-paddle.html 19 http://www.revoptom.com/content/d/therapeutics/c/36087/ 20 http://www.ncbi.nlm.nih.gov/pubmed/18813071 21 http://www.ncbi.nlm.nih.gov/m/pubmed/1123285/ 22 http://m.iovs.org/content/43/4/1004.short 23 http://content.karger.com/ProdukteDB/produkte.asp?Aktion=ShowAbstr actBuch&ArtikelNr=100933&ProduktNr=233014 24 http://www.evrgstl.com/Doctors/WhatWeDo.html 25 http://www.ncbi.nlm.nih.gov/m/pubmed/17146574/ 26 http://www.iovs.org/content/52/9/6066.full.pdf 27 http://www.tshservices.com/autologous_prp_eye_drops.html 28 http://www.ncbi.nlm.nih.gov/m/pubmed/17374962/ 29 http://www.harvesttech.com/products/smartprepmain.html 30 http://www.revophth.com/content/d/cornea-anterior_segment/c/28667/ 31 http://www.biotissue.com/Patients/patients-prokera.aspx 32 http://www.myfoxhouston.com/story/19450901/2012/09/04/newbornbabies-help-patients-with-dry-eyes?clienttype=printable 33 http://www.health.vic.gov.au/news/corneal_transplants.htm 34 http://www.osref.org/medical-education-materials/acute-treatment-ofsevere-ocular-inflammation.aspx 35 http://www.emilianoghinelli.com/Amniotic-Membrane-eXtract.html 36 http://www.eurotimes.org/10December/novelamnion.pdf 37 http://www.pharmcast.com/Patents200/Yr2011/Jan2011/011811/78716 46_Amniotic011811.htm 38 http://www.healio.com/ophthalmology/cornea-externaldisease/news/online/%7B8a880b8c-0fb9-4b50-a3db09b74213f34e%7D/amniotic-membrane-extract-shows-efficacy-intreating-persistent-corneal-epithelial-defects 39 http://www.healio.com/ophthalmology/cornea-externaldisease/news/print/ocular-surgery-news/%7B29ff115c-eb9d-4db7-9b2d5b0980ab4a15%7D/amniotic-membrane-embraced-as-versatiletreatment-for-ocular-surfacedisease 40 http://www.healio.com/ophthalmology/cornea-externaldisease/news/print/ocular-surgery-news-europe-edition/%7B11e2d0b22d70-40e2-9fc8-ca63b47154b2%7D/amniotic-membrane-extractshows-promise-in-treatment-of-corneal-epithelial-defects 41 http://www.jofamericanscience.org/journals/amsci/am0611/73_3943am0611_427_433.pdf 42 http://www.ncbi.nlm.nih.gov/pubmed/20092594 43 http://www.ophthalmologymanagement.com/articleviewer.aspx?articleID =107482 44 http://www.ncbi.nlm.nih.gov/m/pubmed/16491814/ 45 http://www.ncbi.nlm.nih.gov/m/pubmed/22668581/ 46 http://www.ncbi.nlm.nih.gov/m/pubmed/8328549/ 47 http://www.eyecareeducators.com/site/new_treatment_for_meibomian_ gland_dysfunction.html 48 http://www.revoptom.com/content/d/cornea/c/14606/ 49 http://abstracts.iovs.org/cgi/content/abstract/44/5/2450 50 http://jeffreydach.com/2010/03/19/testosterone-for-dry-eyes-byjeffrey-dach-md.aspx 51 http://eyeworld.org/printarticle.php?id=5448 52 http://www.argentisrx.com/media/press/2006-08-07-MemphisBioWorks.pdf 53 http://abstracts.iovs.org/cgi/content/abstract/43/12/66 54 http://ukpmc.ac.uk/abstract/MED/16974129 55 http://abstracts.iovs.org/cgi/content/abstract/43/12/66 56 http://www.empr.com/phase-3-study-update-of-lifitegrast-for-dryeye/article/264885/ 57 http://www.prnewswire.com/news-releases/sarcode-bioscienceannounces-positive-topline-results-from-phase-3-dry-eye-study-oflifitegrast-175379431.html 58 http://www.revophth.com/content/i/1353/c/25861/ 59 http://video.healio.com/video/Lids-Lipids-and-DryEyes;search%3Atag%3A%22ophthalmology-cornea-externaldisease%22