Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
!"#$"$%
Mark Dunbar: Disclosure
Medical Management of
Ocular Surface Disease
! Optometry Advisory Board for:
" Allergan
" Carl Zeiss Meditec
" Regeneron
" Nicox
Mark T. Dunbar, O.D., F.A.A.O.
Bascom Palmer Eye Institute
University of Miami, Miller School of Medicine
Miami, FL
Mark Dunbar does not own stock in any of the above companies
&'()*+(,-./0) 12)3,/45.)*/.25,()678(58(
! 39(.45+)
:(-;((<)=.>)
(>(?):4(+'5.7-78
5<=)544(.@>
! 32-(<),1A(B78! 67227,/4-);'(<)
05C7<@)
-.(5-0(<-)
=(,7871<8)))
1.
1'-23-#
4'#5&"#67#
890
#$%
&'%
Mucous Fishing Syndrome
Cascading cyclic characterized by continuous
extraction of mucous strands
! Initiated by ocular irritation
! Ocular surface cells produce excess mucus, in
response to irritation
! Snow balling" cycle begins when the pt
extracts ("fishes") excess mucus from the
ocular surface
!
!"#$%&'()(*
4'#5&"#67#2:
./0
+""#',-
4'#5&"#67#
890
"
Causes further irritation and a more discharge
M.A. Lemp, oral presentation O SD Summit Meeting, 2008
Mucous Fishing Syndrome
! Treatment includes eliminating the initiating
element
! Educating the patient not to touch the eye
when extracting the excess mucus
! Artificial Tears - Mucolytic agent
! Antihistamine-mast cell stabilizer
The Triad
Dry Eye – Allergy - Blepharitis
! Difficult to separate
! Similar symptoms: tearing, burning, itching,
FBS
! Often vague symptoms
! Signs of inflammation are similar regardless
of disease cause
$
!"#$"$%
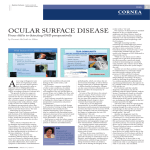
Overlap in Ocular Surface Disease
Opitz DL ARVO 2014 et al.
E1<8(,/-79()F5-7(<-8)E5-(@1.7G(=
! H1.054)
! IJ/(1/8)=(27,7(<-)=.>)(>(
! K95+1.5-79()=.>)(>(
! I44(.@7,),1<L/<,-797-78?)
Overlap in Ocular Surface Disease
! Allergic conjunctivitis most prevalent 42%
! Most common overlap: Mixed Dry Eye
" 86% of the subjects had one or more of these
conditions
! M7B(=)N01.()-'5<)1<()12)-'()-'.((O
6.>) K>()A M1.()-'5<)5<)I<<1>5<,(
!"#$%&#'()#$*+%(,-*.)%"(&/(.)/0
"P4/..(=) 97871<)
"6.>)5<=)@.7-->)8(<85-71<
"P/.<7<@)
"F'1-1+'1:75
"Q.(J/(<-):47<C7<@
"Q.(J/(<-)/8()12)5.-727,754)-(5.
Opitz DL, Kwan JT, Harthan J, et al. Prevalence of allergic conjunctivitis, ocular
surface disease subtypes, and mixed disease. Poster presented at: ARVO ;May 6,
2014;
F5-7(<-)&>+(8);7-')R7@')
S<,7=(<,()12)6.>) K>()678(58(
! T10(<)5@(=)UV)1.)14=(.$
! T10(<)/87<@)+18-0(<1+5/854)'1.01<()
.(+45,(0(<-)-' (.5+>D
! &'18();7-')1,/45.),101.:7=7-7(8 #
! E1<-5,-)4(<8);(5.(.8 #
! *01C(.8 W
! X8(.8)12)5.-727,754)-(5.8)Y)#)-70(8"=5>
( )*+,-./0123043,563!"#$#%&'(')*"+*, 788#6
7 )*+,-./0123043,563$!-!, 788(6
# 90.:63./!%#$, (;;'6
$ <-54=>):?@A?13)-1B0CAD3E@*63788$630'1# 2334# 5)**6(689#+:#;<9#=91#76::1<1<>,#788$6
F.(954(<,()12)6.>) K>()678(58($
! DU)074471<) I0(.7,5<8) 5.()(8-705-(=) -1):() 8/22(.7<@)2.10) 6.>)K>(D
! Z(8/4-8) 2.10)-'()DV$D) [544/+) +144) +.1L(,-) -'()</0:(.) 12)5=/4-8) ;'1) .(+1.-)
(B+(.7(<,7<@)6.>)K>()1<) 5).(@/45.):5878$\
4';<#7)#=2>';?)%2(62
@'#AB#6)2
1'-23-#2CBDD#'#'*2
E(62F(""(;6*G.
6.>) K>()M5.C(-)39(.97(;\)
!"#$%&#'()*+',-(-+').-(/)!"%0(-0#)122+"(3'-(4
! ]DU)M74471<)Americans suffer from dry eye disease
! 1234(5)..)&6(spent on dry eye symptom relief annually in the U.S. alone
! M18-)2.(J/(<-4>)(<,1/<-(.(=)=78(58()8-5-()by eye care professionals
3++1.-/<7->
29.1
26.4
1 0 .2 % g ro wth
2012
2022
F1?G0*4=?@A3?H3H10I-0@43 J1C3KC03A-HH0101A3 ,103*,5*-5,40L3/C3 ,::5C=@23=@*=L0@*03/C3,2034?3M)3N0@A-A3F?:-5,4=?@3
0A4=.,40A3=@30,*+3 ,20321?-:3 =@378(73,@L3 787763F1?G0*4=?@A3,AA-.03@?3 *+,@203=@3=@*=L0@*0350B05A3?B0134+03 @0O43
L0*,L063
P(--(. ,47<7,54)
1/-,10(8)21.)
+5-7(<-8)
F5-7(<-)Z(-(<-71<)
^)Z(2(..548
F.5,-7,()
[.1;-')
7 *890 %( !+& $ 0 ( : ; < 2 ( = & #$ 80 > 0 6 ')?0 ( @ 0$ & 8%( &6 ( %> 0( A.& B*.( C8"( D"0 ( E 8& F - +%'( 7 *890 %
1 . Th e Ga llu p Orga niza tio n, Inc. Th e 20 12 Gallup Stud y of Dry Eye S u ferers.. 2 01 2; 2. Mark et Sco pe Da ta, Allerg an , Inc. 20 11 .
D
8/31/16
Dry Eye
As defined by the Dry Eye Workshop (DEWS)
- “is a multi-factorial disease of the tears and ocular
surface that results in symptoms of discomfort, visual
disturbance, and tear film instability, with potential
damage to the ocular surface. It is accompanied by
increased osmolarity of the tear film and
inflammation of the ocular surface.1”
Dry eye complaints are the most common
reason patients seek help from eye doctors
Patient Types with High
Incidence of Dry Eye Disease
• Women aged 50 or older1
• Women using postmenopausal hormone
replacement therapy2
• Those with ocular comorbidities3
• Contact lens wearers3
• Smokers4
• Users of artificial tears ≥ 3 times/day
1 Schaumberg
Traditional Dry Eye
• Age-related dysfunction of the lacrimal gland
• Lead to aqueous tear deficiency or tear film
instability
• Treatment aimed at lubricating and hydrating
the ocular surface
– Provided palliative, transient symptomatic relief
et al. Am J Ophthalmol. 2003.
et al. JAMA. 2001.
3 Lemp. CLAO J. 1995.
2 Schaumberg
[1 ] Defin itio n a nd cla ssifica tion o f d y
r ey e. Repo rt o fth e diag no sisa nd cla ssifica tion sub co mmitteeo f th e Dry Ey e Wo rk Sh op (DEWS ).Ocu a
l r S u rface
2 00 7; 5:75 -9 2 .[2] Beh ren sA, Do yle JJ ,S tern L, Ch u ck RS ,McDo nn ell PJ ,et al; Dy sfun ction al tea r sy nd ro me stu dy g ro up .Dy sfu n ctio na ltea r sy nd ro m
e:
a Delp h i a pp ro ach to trea tmen t reco mmen d ation s.Corn ea .20 06 S ep 2
; 5(8):9 00-7 .
4 Multi-Sponsor
Surveys, Inc. 2004. The 2004 Gallup Study of Dry Eye Sufferers. 2004.
Healthy Tears
• A complex mixture of
proteins, mucin, and
electrolytes
• Antimicrobial proteins:
Lysozyme, lactoferrin
• Growth factors & suppressors
of inflammation: EGF, IL1RA
• Soluble mucin 5AC secreted
by goblet cells provides
viscosity
– Membrane-bound mucins 1 & 4
help stabilize tear film
• Electrolytes for proper
osmolarity
Tears in Chronic Dry Eye (CDE )
• Lesser concentrations of
many proteins in CDE
– e.g. antimicrobial proteins
• Growth factor
concentrations decreased
• Cytokine balance shifted,
promotes inflammation
• Soluble mucin 5AC greatly
decreased
Artificial Tears
Normal
Healthy
Tears
Artificial
Tears
– Due to loss of goblet cells
– Impacts viscosity of tear film
• Activated proteases
– Degrade extracellular matrix
& tight junctions
• Increased electrolytes
• Artificial tears contain electrolytes –
But they lack the complex mixture of proteins, mucins &
other factors found in normal healthy tears
• Provide temporary, palliative relief
3
!"#$"$%
The Healthy Eye
Normal tearing
depends on a
neuronal feedback loop
_5,.7054
[45<=8
Neural Feedback Loop
It functions as an single integrated unit
! Controls tear and mucin production
*(,.(-101-1.)
H(.9()S0+/48(8
! Incites inflammation when there is an
imbalance in the feedback look
! This leads to a change in quantity and quality
of the normal tears
!"#$%&'())*$+&#,-&.#/,+#/,
01(2#$&'($3#1"
3,/45.) */.25,(
H(/.54)
*-70/45-71<
Stern et al. Co rn ea . 1 9 9 8 :1 7:5 8 4
E/..(<-) F(.8+(,-79()1<)6.>) K>(
Stable Tear Film Essential to Function
! &;1)+.705.>)21.08)12)=.>)(>(
Lacrimal
Gland
Aq ueous
" D?*$&8*%)?0(G.)$)F(F0/)+)06%(+*-'0F(B"(7ACH
! 3,,/.8);'(<)-'();5-(.)N1.)5J/(1/8O)7<)-(5.8)(95+1.5-(8)5-)5)258-(.).5-()-'5<)
<1.054
Meibo mian
Gland
Anatomical
Lip id
Mucin
" I,-0&-'(F0/)+)06%
Go blet Cells
Stable
Tear
Film
! 3,,/.8);'(<)5J/(1/8)@(<(.5-71<)2.10)-'()45,.7054)@45<=)78)7<8/227,7(<-)-1)
C((+)-'()(>(8)0178-
Latest research suggests that 86% of dry eye patients have
Evaporative Dry Eye1
Sensory
Motor
Lid B link ing
T ear
Clearance &
Sp read
Lid Clo sure
Evap oration
1. Lemp MA, et al. Dis tribution of aqueous defic ient and evaporative dry eye in a c linicbas ed patient c ohort: a retros pec tive s tudy. Cor nea. 2012:31(5):472-478
22
Clinical Findings Associated with Dry Eye
! Diffuse injection
! Punctate epithelial erosions (PEE) and
punctate epithelial keratitis (PEK)
! NaFl staining
! Rose Bengal/Lissamine green staining
! Reduced Schirmers
! Rapid tear break-up time (TBUT)
Assessments Currently Used to
Diagnose Dry Eye Disease
! Presence of patient
symptoms
! Aqueous tear production
" Schirmer tests
" Zone Quick
! Ocular surface disease
" Clinical examination
! Tear stability
" Tear breakup time
! Tear film osmolarity
! No test currently
evaluate the OS
inflammation…yet
" Dye staining
W
8/31/16
Tear Film Osmolarity
• A measure of the concentration of solutes
in the tear film
• Elevated in both evaporative and aqueous
deficient dry eye disease
• Tear film osmolarity has been proposed as
a biomarker that could be used to diagnose
and monitor dry eye disease
InvestOphthalmolVisSci.2006Oct;47(10):4309-15.
• A meta-analysis by Tomlinson et al reviewed
osmolarity values in patients with and
without dry eye disease and suggested a
value of > 316 mOsmol/L as being diagnostic
of dry eye disease
InflammaDry
§ DetectselevatedlevelsofMMP-9intearfluid
§ 10minutein-officeresults
§ Easytouse– canbeperformedbytechniciansor
nurses
§ Disposable– noadditionalequipmentrequired
Limit of Detection: the normal level of MMP-9
in human tears ranges from 3-41 ng/ml
§Positive test result = MMP-9 ≥ 40 ng/ml
§Negative test result = MMP-9 <40 ng/ml
Archives Ophthalmol Jan 2013
5
!"#$"$%
Treatment Options for Dry Eye
InflammaDry Clinical Trial
Clinical Criteria
+
–
N = 206
+
121
4
–
22
59
InflammaDry
Sensitivity
85% (121/143)
Specificity
94% (59/63)
Overall Agreement
87% (180/206)
! Control environmental
factors
! Lid hygiene
! Artificial tears
! Punctal plugs
! Steroids
! Restasis
! Xiidra
! OMG3
Treatment of Dry Eye
! Anti-inflammatory treatment
" Restasis (Cyclosporin)
" Xiidra (Lifitagrast)
! FDA approved June 2016
" Topical steroid
" Doxycycline if MGD
" ? Omega 3 fatty acids
e77=.5 [email protected]
3FX*A#)
! _5-(8-)=.>)(>()=./@)5++.19(=):>)Q6I)21.)-'()
-.(5-0(<-)12):1-')87@<8)5<=)8>0+-108)
! I++.1954):58(=)1<)W)0/4-7,(<-(.) ,47<7,54)-.754
! P7=)=187<@
! e77=.5 '5=)5)8-5-78-7,544>)87@<727,5<-),47<7,54)
70+.19(0(<-)7<)87@<8)N,1.<(54)8-57<7<@O)5<=)
8>0+-108)N(>()=.><(88O),10+5.(=);7-')
+45,(:1)N3+/8)8-/=7(8O
E10+5.(=)*>0+-108\
! #UU)+5-7(<-8)1<)e77=.5 5<=)#U%)1<)+45,(:1
! e77=.5 '5=)5)'7@'4>)8-5-78-7,54)70+.19(0(<-)5-)
=5>)!W)N+fV`VVVbO?)=5>)WD)N+gV`VVV$O)5<=)5-)
$W)=5>8)52-(.)7<7-75-7<@)-'(.5+>)N+gV`VVV$O`
%
!"#$"$%
M3I)12)_727-(@.58! *0544)014(,/4()7<-(@.7<)5<-5@1<78-)-'5-):41,C8)
:7<=7<@)12)SEIMA$)-1)_QIA$)1<)-'()&A,(44)
8/.25,(?)7<'7:7-7<@)&A,(44).(,./7-0(<-) 5<=)
5,-795-71<)5881,75-(=);7-')6K6)7<245005-71<
&'()3,/45.)*/.25,()7<)6.>)K>(
! 39(.A(B+.(8871<)12)5)47@5<=)C<1;<)58)7<-(.,(44/45.)
5='(871<)014(,/4(A$)NSEIMA$O
" &' (8()5.()27<@(.47C()+.1L(,-71<8)1<)-'()(+7-'(47/0)5<=)
(<=1-'(47/0)'59():7<=7<@)87-(8)21.)&A4>0+'1,>-(8
! &' () 8+(,727,):7<=7<@)1,,/.8)975)-'()_QIA$)7<-(@.7<
! _QIA$)78)1<)-'()[email protected]<@)&A4>0+'1,>-() 5<=):7<=8)-1)SEIMA$`)
" &' ()7<-(.5,-71<)12)_QIA$)5<=)SEIMA$)78)<1-)1<4>)
70+1.-5<-)21.)&A,(44)5='(871<?):/-)5481)[email protected]<?)
+.1472(.5-71<)5<=),>-1C7<().(4(58()5-)87-(8)12)
7<245005-71<
RESTASIS®
(cyclosporine ophthalmic emulsion)
0.05%
E>,418+1.7<()3+'-'5407,)K0/4871<)V`VUh))
Z(8-5878i
! F10B0@4A3P3*0553,*4=B,4=?@#'
" Q* 4=B ,40L3P3* 055A 3:1?L-* 03=@H5,..,4?1C 3* C4?R =@0A 34+,4350,L34?S( (
!
P=AA-03 L,.,20
!
T0*1-=4.0@43 ?H3 P3 *055A
!
F1?L-*4=?@3 =@H5,..,4?1C3 A-/A4,@*0A
! J0*10,A0A3,:?:4?A=A3?H35,*1=.,5325,@L34=AA-0#'
! E@*10,A0A3*?@G-@*4=B,5 2?/5043*0553L0@A=4C#&
! E.:1?B0A3*?1@0,53/,11=013H-@*4=?@#U
K8-5:478'(=)852(->) +.1274(#U?#bAWV)m)#`c)074471<)+5-7(<-8)-.(5-(= kW$
k&1 -54 ) + 5-7 (< -8) -.(5-(= ) 2.1 0) l5< /5.>) D VV #) -1) *(+ -(0: (.) DV$ D`
$$` ) *- (. <)M K?) P(/(. 0 5<) ZT ?) Q1B) ZS ?) (- ) 54̀ ) &'() +5- '141@>) 12 )=. >) (>(\ ) - '() 7<- (. 5,- 71<) :(- ;((<) - '()1,/45. ) 8 /. 2 5,() 5<=) 45,. 70 54) @45<=8 ` ) E1. <(5) $cc!a $bN %O \ U!WdU!c` ) ) #U` )ZK*&I*S * i F. 1=/,- ) M 1<1@. 5+'?) I44(. @5<)
S <,` )3,- 1:(. ) #?) DV$D` ) #%` ) j/<(. - *) "+  & [1:4(- ) ,(44) </0 :(. 8 ) 5<=) (+7- '(4754)
+. 1472 (. 5- 71<) 7<) - '() ,1<L/<,- 79 5) 12 ) +5- 7(<- 8 ) ;7- ') =. >) (>() 8 ><=. 10 () - . (5- (=) ;7- ') ,>,418 +1. 7<(` :$ 16& 0)6+ 6#27 *2*;<
DVVDa $DV\ ##Vd
##b` ) #b` )* 544 j?) M /<=1. 2 &j?) Z(78 ) P_) 5<=) - '() E8 I F'58 () #) *- /=>) [. 1/+` ) &;1) 0 /47, (<- (. ?) . 5<=10 7G (=) 8 - /=7(8 ) 12 ) - '() (2 2 7, 5,>) 5<=) 8 52 (- >) 12 ), >,418 +1. 7<()
1+'- '540 7, ) (0 /48 71<) 7<) 0 1=(. 5- () - 1)8 (9(. () =. >)(>()
=78 (58 (` ) 0)6+ 6#27 *2*;<
DVVVa $VbN WO \ %#$d%#c` ) #!` )EIH6I\ ) *(,- 71<) !` %` $#)&5:4() U` W) S <- (@. 5- (=) */0 0 5. >) 12 )K2 2 7, 5,>?) $ccc` ) #c` ) 65- 5) 1<) 2 74(` ) E47<7, 54)
*- /=>) Z(+1. - ) $cD#b$A VVD` ) $ccc` ) ) WV` ) 65- 5) 1<) Q74(` ) E47<7, 54)
*- /=>) Z(+1. - ) $cD#b$A VV#` WV` ) 65- 5) 1<) 2 74(` ) I44(. @5<?) S <,`
Cyclosporine: Treatment for
Dry Eye Disease
! Cyclosporine ophthalmic emulsion contains the
immunomodulator cyclosporine
" Immunomoduator = immunosuppressive -?
! Cyclosporine is a prescription therapy for
patients with dry eye due to decreased tear
production
! Cyclosporine is believed to treat and may prevent
progression of the disease by treating the
underlying cause - inflammation
b
!"#$"$%
Cyclosporine Pivotal Trial
Results
! Superior Schirmer scores
!
!
!
!
Reduced reliance on artificial tears
Reduced corneal staining
Symptom relief
Increased goblet cell density
Summary of Laboratory
Efficacy Measures
! Restasis™ decreased inflammatory markers
! Reversal of inflammation
! Underlying immune-mediated pathology of dry
eye disease addressed
! 0.05% CsA normalizes the ocular surface
" Permits return of a stable, healthy tear
Dysfunctional Tear Syndrome (DTS):
Pathophysiology
! Most DTS cases have inflammatory basis
" Triggers or maintains condition
" Sometimes difficult to clinically observe
inflammation
! Presence of clinically apparent inflammation
affects treatment choices
<*J?@@0553 043 ,5,# QTVW,#788$6
E1<8(<8/8) &.(5-0(<-) [email protected]'0)
[/7=(47<(8
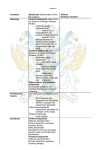
Severity Level 1
Symptoms
! Mild to moderate
symptoms and no
signs
! Mild to moderate
conjunctival signs
If no improvement – add level 2
X0 + 10 @ A 30 43, 5 63.+<? 1 ) ,7 8 8& 6
Treatment
" F5-7(<-),1/<8(47<@
" F.(8(.9(=)-(5.8
" K<97.1<0(<-54)
05<5@(0(<-)
" E1<-.14)I44(.@7(8
" X8()12)'>+1544(.@(<7,)
+.1=/,-)
" T5-(.)7<-5C(
DTS Study Group
!
!"#$"$%
Severity Level 2
Treatment
Symptoms
! M1=(.5-()-1)
8(9(.() 8>0+-108)
! &(5.)2740)87@<8
! M74=),1.<(54)
+/<,-5-( 8-57<7<@
! E1.<(54)8-57<7<@
! n78/54)87@<8
6&*) *-/=>)[ .1/+
! X<+.(8(.9(=)-(5.8?)
@(48?)17<-0(<-8
! E>,418+1.7< I)NZ(8-5878O
! [email protected] NB77=.5O)
! &1+7,54)8-(.17=8)
! H/-.7-71<54) 8/++1.-)
N245BA8((=)174O`
If no improvement – add level 3
Severity Level 3
Symptoms
! *(9(.()8>0+-108)
! M5.C(=),1.<54
8-57<7<@
! E(<-.54),1.<(54)
8-57<7<@
! Q7450(<-5.>)C(.5-7-78
(6 F10A01B,4=B0>H1003 5-/1=*,@4A3 [email protected]@4A[
76 \-41=4=?@,53 A-::?143 Y0AA0@4=,53 H,44C3,*=LAD30626D3W.02,>#[
#6 P?:=*,53 ,@4=/=?4=*3 YA+?143401.3?@5C[
$6 NC*5?A:?1=@03 Q
'6 P?:=*,53 A401?=LA3 Y5?]>L?A03 F10L <=5L^Z_<9^[
&6 )CA40.=*34041,*C*5=@0A YL?OC*C*5=@0Z.=@?*C*5=@03 (88 .23?13
,`=4+1?.C*=@Z*5,1=4+1?.C*=@3 7'83 .237OZ]R[
U6 9,*1=A014
a6 F-@*4,5 :5-2A3 Y40.:?1,1CZ:01.,@0@4[
! Tetracyclines
! Punctal plugs
If no improvement –
add level 4
6&* *-/=> [ .1/+
&.(5-0(<-)d _(9(4)D)^)#
K#5#"2 82L2/2M
82L2/2M N;=#'&)#2 );2 N;=#'&)#"-2 C#5#'#(D#
Treatment
Severity Level 4
Symptoms
! *(9(.()8>0+-108)
! *(9(.(),1.<(54)
8-57<7<@
! K.1871<8
! E1<L/<,-7954
8,5..7<@
;6 <?=A4-10>104,=@=@23 0C03]0,1
Treatment
! Systemic antiinflammatory therapy
! Oral cyclosporine
! Moisture goggles
! Acetylcysteine
! Punctal cautery
! Surgery
$` )&'() &(5. ) Q740 ) ^) 3,/45. ) */. 2 5,() *1,7(- >` ) DVVb) . (+1. - ) 12 ) - '() S <- (. <5- 71<54) 6. >) K>() T 1. C*'1+) N 6KT *O ` ) *+(,754) S 8 8 /(` )!6"& 01(2#$ & '($ 3 #1" DVVba UN DO \ %bdDVW` )
#` )l 5,C8 1<) T P\ )M 5<5@(0 (<- ) 12 ) =>8 2 /<,- 71<54) - (5. )8 ><=. 10 (\ ) 5)E5<5=75<) ,1<8 (<8 /8 ` ) =#,& > &0)6+ 6#27 *2
DVVca WW\ #!Ud#cW` )
6&*) *-/=>)[ .1/+
3,/4(9(
H(/.18-70/45-71< 12)-'()45,.7054)<(.9(
c
!"#$"$%
Diagnosis
! Anterior/Posterior blepharitis
Treatment Options:
! Lid hygiene
! Oral Doxycycline 100 mg/day for 1 wk, 50
mg/day X 6-8 wks
" Perostat (Doxy 20 mg)
! AzaSite bid X 2 days, qhs X 1 mo
Diagnostic and Therapeutic
Challenges with Blepharitis
Blepharitis
Staphyloccal
)0B 01,534C :0A
,@L3 A-/4C:0A
]=4+3 ?B015,::=@2
A=2@A3 ,@L3 AC.:4?.A
Chronic Red Eye
X50:+,1=4=A
N5=@=*,53 F10A0@4,4=?@
\?3L0H=@=4030@L3
:?=@43* -10
N?.:50O3=@401,*4=?@
?H3=@H5,..,4=?@D
E@H0*4=?@D3,/@?1.,5
<b3A0*104=?@A3,@L3
LCAH-@*4,5
40,13H=5.
Although Anterior Blepharitis and
Posterior Blepharitis (MGD) are
distinct entities, they often coexist
Anterior
Blepharitis
Mixed
F?A401=?13
X50:+,1=4=A
Y<bJ[
Dry Eye
N?0O =A 4A 3]=4+3
B ,1=?-A 3
L01.,4?5?2=* 3
* ?@L=4=?@A
&'()*+(,-./0)12)_7=)
M5.@7<)678(58(
Spectrum of Lid Margin Disease
MGD
F18-(.71.
Anterior
N?.?1/=L=4C
]=4+3L1C 30C 0
,@L3?4+013W)J
N+1?@=* 3* ?@L=4=?@
]=4+30O ,* 01/,4=?@A
,@L310.=A A =?@A
Seborrheic
Marginal Ulcer
Phlyctenules
Anterior Blepharitis
Crusting of lids (am)
Loss of lashes
Collarettes
! Scales that encircle
lash
! Lid margin redness
! Conj hyperemia
! Inflammation
!
!
!
Most
Common
$V
!"#$"$%
Posterior Blepharitis
Pathophysiology of Anterior
Blepharitis
Meibomian Gland Disease (MGD)
! Inflammation is caused by the impact of
bacterial exotoxins and/or delayed
hypersensitivity to antigens
! Staphylococcal infection can be purulent or
ulcerative and often causes angular blepharitis,
a focal infection in the skin of the
lateral canthus
Involves a change
in composition of
meibomian gland
secretions
! Leads to
inflammation,
irritation and an
altered tear film
!
c , * R A ? @ 3dX63.)? #$ %
# & ' (' )* "+ * 6378 8 ae$ # S( U 8>( U ;e3).= 4+ 3TKD3_5? ]0 1A3Nd3c 163./ !%#$ 63(; ; ' e7 ( S78 8 >78 U e3_ ? - 5R A b\63X5 0 : +,1= 4= AS3
9 = L 3., 12 = @ 3L = A 0 ,A 0 3, @ L34+ 03? *- 5 , 13A - 1H, * 063E@ S3 f? 5 5 ,@ L 3Kc D3<, @ @= A <c D30 LA 63%@ 6* ) <#76 <:) @1 #;A >1 ) >1 B#-1 8 A @ )* #)? 8 #76<C A @) * #
-) ? ) C 1 "1 ? (,#\0 ]3g? 1R D3\gS3): 1= @2 0 1>V015 , 2 e3 7 8 87 e#; >$ a 6
MGD Can Lead to a
Downstream Cycle of Inflammation
S
Y
M
P
T
O
M
S
Pathophysiology of Posterior Blepharitis
and Its Role in Ocular Disease
+")#' #=2
"($(=*
!&7)#' (&"2
"($&*#
SYMPT OMS ST AR T
Critical intervention
p oint
I
N
C
R
E
A
S
E
Visib le/nonvisib le
+,#
P6D"&F F &)(;6
Q54010L3N?.:?A=4=?@3
?H3<0=/?.=,@3b5,@L3
)0*104=?@A
F1?>=@H5,..,4?1C3 ,@L3 =11=4,4=B0 0HH0*4A3
?H3 ,54010L3 .0=/-.
OCULAR CHANGES
Potential long-term
damage
I;' F ;6#
(F O&"&67#
J0A4,/=5=`,4=?@3 ?H3 40,13 H=5.
KB,:?1,4=B03 L1C3 0C0
E11=4,4=?@ZE@H5,..,4= ?@3 ?H3 5=L3.,12=@3
,@L3 ?*-5,13 A-1H,*0
W*-5,13 A-1H,*03 =@H5,..,4=?@ZL,.,2 0
F (..>) R6`) 6.>) (>() = 7 8(58(\) ) + 5-'1+ '>87 1 41 @>?),4 5887 27 ,5-7 1< ?) 5< =) =7 5@< 187 8`) :
) 7& >&.# ,# ; E5.(`) DV V! a) $W \) *b cA*!b `
*' 7 05G5C7 l?) (-) 54 `) 3,/ 4 5.) 8/ .25,() ,'5< @(8) 5< = )= 78,1 021 .-)7 <) +5-7 (< -8) ;7-')0(7 : 107 5< @4 5< = )= >82/< ,-71 <`) :$16 &0) 6+6# 27* 2 `) $c cUa$ $#N$V O\$ D% %A$D bV`
H7 ,' 1 4 8) j j ?) (-) 54 `) &' () 7< -(.< 5-71 <54 ) ;1.C8' 1 +) 1< 0
) (7 : 107 5< @4 5< = )= >82/< ,-71 <\) (B(,/ -7 9() 8/ 005.>`) 4,5"%+& 0)6 +6#2 7* 2& 8/ %& '1/ `)D V$$ )a #V aU DNWO\$c DD A$ cVc `
Meibomian Gland Function
M[)8(,.(-71<8)05>):()01=727(=):>).)$*'0'(
$8&F-+0F(B"(&+-.*8(B*+%08)*(
! P5,-(.75)05>)=(@.5=()-'()47+7=8);'7,')4(5=)
-1)5<)/<8-5:4()-(5.)2740)5<=)7..7-5-7<@) 2.(()
25-->)5,7=8
! R1.01<54)70:545<,(8)05>)54-(.)47+7=)+.1274(8)
-1)=(8-5:747G()-'()-(5.)2740)5<=)+.1=/,()
(95+1.5-79()=.>)(>(
Because Not All MGD Is Obvious,
Active Disease Identification Is Crucial
!
NOMGD with recalcitrant ob struction
d esp ite forceful exp ression
NOMGD yield ing secretion
with forceful exp ression
P 4 5,C7 () E I?) (-) 54 `) H1 < 1 : 97 1 / 8) 1: 8-./ ,-7 9()0(7 : 1 07 5< @4 5< = ) =>82/ < ,-7 1< `) =* $,"# 9 DV $V aDc \$# ## A$ #W U`
$$
!"#$"$%
<bJ3KO:10AA=?@3E@3WHH=*0
Meibomian Gland Evaluation
Diagnostic
Expression
Meibography
“Korb” Meibomian Gland Evaluator
Additional Manual Expression
! Standardized method for assessing meibomian
gland functionality
! Consistent, gentle pressure " deliberate blink
(1g/mm2 )
o&'()0(5<) </0:(.) 12)
0(7:1075<) @45<=8) >7(4=7<@)
47J/7=) 8(,.(-71<) 7<) -'()41;(.)
(>(47=) 78) ,1..(45-(=) ;7-') =.>)
(>()8>0+-108?)
(>()
8>0+-108?) +)f) V`VVVDp
? * $@ & A& B 2 # 1C/ "D& = * $, "# D& E FF G &
H"IJ&3+'-'5407,)*/.@7,54)S<8-./0(<-8
!"#$%&$"' '
("))*+
,"+-"% (*"$+./&)010+)' 23' '
!4' 56$0+%%+78' 9:
MGD Complications
Collins Expressor Forceps (Item 98610)
Fo r ag g ressiv e ex p ression o f th e Meib o mian g lan d.
Livengood Expressor Paddles
Angled (Item 9 8 6 2 0 ) & Flat (Item 9 86 30 )
Fo r mild o r g en tle ex p ressio n of th e Meib o mian g lan d.
! Chronic blepharoconjunctivitis
! Keratitis
" Neovascularization
" Ulceration
" Scarring and thinning
! Chronic pain
! Loss of vision
$D
!"#$"$%
Ocular Rosacea Findings
! Meibomian gland Dz
Ocular Rosacea Findings
! Corneal
vascularization
! Sterile corneal
infiltrates
! Corneal ulceration
! Corneal perforation
! Episcleritis
! Scleritis
! Iritis
" Foamy tears
! Recurrent chalazia
! Chronic blepharitis
" Staph blepharo- conjunctivitis
" Lid margin telangiectasia
! Papillae, follicules
! Hyperemia
Rosacea Keratitis
! Represents more significant clinical problem
! Cutaneous rosacea:
" 5-30% corneal involvement
! Ocular rosacea:
" 75-85% corneal involvement
! Inferior cornea usual site
! Characteristic spade-shaped infiltrates
'--+\"";;;`7198`1.@"
S3n*)M5.,')DV$$
IOVS March 2011
! Involved more than 50 leading clinical and basic research
experts from around the world
! Completed 2010: based on more than 2 years or work
! Participants were assigned to subcommittees, reviewed
published data and examined the levels of supporting evidence
! The report has also been translated, at least in part, into
Chinese, Dutch, French, German, Greek, Italian, Japanese,
Polish, Portuguese, Spanish, Russian and Turkish; these
translations are available on the TFOS website.
$#
8/31/16
Tests to Diagnosis MGD
MGExpression– mostimportant!
❖Theapplicationofmoderatedigitalpressureto
thecentrallowerlid
◆Asymptomaticadults
❖Itisappropriatetoincludeglandexpression
❖AdiagnosisofMGDmayrequirethatthepatient
befurtherassessedforocularsurfacedamage
anddryeye,usingappropriatediagnostic
techniques
Diagnosis/TreatmentofStage1
• No symptoms of
ocular discomfort,
itching, or
photophobia
• Clinical signs of
MGD based on gland
expression
• Minimally altered
secretions: grade >
2–4 Expressibility:
• No ocular surface
staining
u
Inform patientabout
MGD,
u The potentialimpactof
diet,andthe effect of
work/home
environments ontear
evaporation, andthe
possibledryingeffect of
certain systemic
medications
u
Consider eyelidhygiene
including warming/
expression
Diatnosis/Treatment of Stage 3
◆ Moderatesymptomsof
oculardiscomfort,
itching,orphotophobia
withlimitationsof
activities
◆ ModerateMGDclinical
signs
❖ Lidmarginfeatures:
plugging,vascularity
❖ Moderatelyaltered
secretions:grade>8to<
13Expressibility:2
❖ Mildtomoderate
conjunctival and
peripheralcorneal
staining,ofteninferior
All the above, plus
u Oral tetracycline derivatives
(+)
u Lubricant ointment at bedtime
(+)
u Anti-inflammatory therapy for
dry eye as indicated (+)
Tests for Diagnosing MGD
• Administration of a symptom questionnaire
• Measurement of the blink rate and calculation
the blink interval
• Measurement of lower tear meniscus height
• Measurement of tear osmolarity (if available)
• TBUT and Ocular Protection Index (OPI)
• Grading of cornea/conj stain
• Schirmer’s or alternate (phenol red thread test)
Diagnosis/Treatment of Stage 2
◆ Minimaltomild
symptomsofocular
discomfort, itching,or
photophobia
◆ MinimaltomildMGD
clinicalsigns
◆ Scatteredlidmargin
features
❖ Mildlyalteredsecretions:
grade>4– <8
❖ Expressibility:1
◆ Nonetolimitedocular
surfacestaining
u Advisepatient onimproving
ambienthumidity;
optimizingworkstationsand
increasing dietary omega-3
fatty acidintake (+)
u Institute eyelidhygiene with
eyelidwarming (aminimum
of4min,1-2X/day)followed
bymoderate tofirm
massage andexpression of
MG secretions (+)
u All theabove,plus(+)
u Artificiallubricants(forfrequentuse,
non-preservedpreferred)
u Topicalazithromycin
u Topicalemollientlubricantorliposomal
spray
u Consideroraltetracyclinederivatives
Diagnosis/TreatmentofStage4
◆ Markedsymptomsofocular
discomfort,itchingor
photophobiawithdefinite
limitationofactivities
◆ Severe MGDclinicalsigns
❖ Lidmarginfeatures:
• Dropout,displacement
❖ Severelyalteredsecretions:
grade >13
❖ Expressibility: 3
All the above, plus
u Anti-inflammatory therapy for
dry eye (+)
◆ Increasedconjunctival and
cornealstaining,including
centralstaining:
◆ é Signsofinflammation:
❖ Moderateconjunctival hyperemia,
phlyctenules
14
!"#$"$%
Traditional Treatments
Commercial Lid Scrups
! Lid Hygiene
" Baby shampoo
" Hot compresses
! Poor compliance
Blepharitis Treatment: Beyond
Lid Hygiene
! Oral Doxycycline
Beyond Lid Hygiene
"100 mg/day for 1 wk, 50 mg/day X 68 wks
"Low dose doxycycline
! Perostat (Doxy 20 mg) bid
! AzaSite: topical azithromycin
The Effect of Low-Dose Doxy in
Chronic MGD
The Main Problem with Oral
Therapy (Doxycycline) is
Side-effects
! Evaluate the effect of low dose doxycycline (20 mg)
therapy in patients with chronic MGD that were
refractory to conventional therapy
! Randomized prospective study enrolled 150 patients
(300 eyes) w MGD who didn't respond to lid hygiene
and topical therapy for more than 2 months
! Patients randomized to:
" High dose group (doxycycline, 200 mg, twice a day)
" Low dose group (doxycycline, 20 mg, twice a day)
" Control group (placebo)
h?10,@3c3W:+4+,5.?563788'3J0*e(;Y$[S7'a>
$U
!"#$"$%
The Effect of Low-Dose Doxy
in Chronic MGD
! At 1 Mo: Both the high and low dose group
showed statistically significant differences after
treatment in TBUT, Schirmer test, the number of
symptoms reported and the degree of
improvement vs control
! No statistically significant difference between the
high and low dose groups
! The high dose group (18 patients, 39.13%) had
more side effects than did the low dose group (8
patients, 17.39%)
The Effect of Low-Dose Doxy in
Chronic MGD
CONCLUSIONS:
! Low dose doxycycline (20 mg twice a day)
therapy was effective in patients with chronic
MGD that were refractory to conventional
therapy
h?10,@3c3W:+4+,5.?563788'3J0*e(;Y$[S7'a>&#
h?10,@3c3W:+4+,5.?563788'3J0*e(;Y$[S7'a>&#
Low Dose Doxycycline
J0*8!+)06+0K
! Provides antiinflammatory results
! Lower dose
minimizes side effects
and eliminates antibacterial resistance.
Cost: ~ $1600 for both eyes
Instrument costs $99,000
E5<)+/.,'58() _7+1241; 21.)sDU?VVV
N;7-' 1/-)-' () _7+797(;O
E18-)<1;)t)s$VVV
Assess the Tear Film With LipiView®
LipiView
_7+7n7(;) /8(8) 5=95<,(=)7<-(.2(.10(-.7, -(,'<141@>) 5<=) ,5+-/.(8) =(-574(=) =7@7-54)
705@(8) 12)-'() (>(u8) -(5.)2740) -1) ,5+-/.(?) 5.,'79(?) 05<7+/45-(?) 5<=)8-1.()
-'() 174>) 47+7=) 45>(.)12) -(5.
_7@' -)81/.,(\
-' ()744/07<5-1.
LipiView® Output
&1/,' A8,.((<)
,1<-.14)+5<(4
E' 7<).(8E50(.5?) ,10+/-(.)
5<=)=.79(.8)5.()
'1/8(=):>)-'()=(97,(
M(58/.(0(<-)-70(\
DV)8(,1<=8)+(.)(>(
! Produces a measurement called
the Ocular Index of Lipid
Interferometric Color Unit (ICU)
! Calculated on a frame-by-frame
basis and plotted for
~1 billion data points per eye
! The results are then displayed
and are available for printout
$%
!"#$"$%
Conclusions
M7P1 Q41;
M(5<)70+.19(0(<-);58)1:8(.9(=);7-')_7+7Q41;i)2.10):58(47<()-1)
+18-A-.(5-0(<-)7<)M(7:1075<)@45<=)8,1.(?)-(5.)2740):.(5CA/+)-70(?)5<=)*FKK6)5<=)
3*6S)6.>)K>()8>0+-10)J/(8-71<<57.(8
_7+7Q41; @.1/+)'5=)5)8-5-78-7,544>)87@<727,5<-)@.(5-(.)70+.19(0(<-)7<)</0:(.)12)
M(7:1075<)@45<=8)8(,.(-7<@),4(5.)47J/7=)58),10+5.(=)-1);5.0),10+.(88),1<-.14)
-'(.5+>
*70745.)70+.19(0(<-)7<)(22(,-79(<(88)-.(<=8)1:8(.9(=)52-(.),.18819(.)2.10);5.0)
,10+.(88)-'(.5+>)-1)_7+7Q41; -.(5-0(<-
39(.544)852(->)+.1274()12)-'()_7+7Q41; 8>8-(0).(24(,-8)5)41;)1,,/..(<,()12)<1<8(.71/8?)
-.5<87(<-)87=()(22(,-8a)<1)8(.71/8)5=9(.8()(9(<-8).(45-(=)-1)-'()=(97,(
Dunbar Treatment Recommendations
A Stepwise Approach
! Step 1 – Lid Hygiene: LS, HC, AT
! Step 2 – Topical Medications
" Steroids (FML, Lotemax, PF)
" Steroid/antibiotic combinations
" Antibiotic ointment (Erythromycin)
" AzaSite
6(01=(B)'58).(,(79(=)5)41-)12)
5--(<-71<)19(.)-'()+58-)2(;)>(5.8
! Step 3 – Systemic antibiotics
" Tetracycline/Erythromycin
" Doxycycline
" Azithromycin
6(01=(B
! &7<>)+5.587-7,)07-(8)-'5-)
479()7<)1.)<(5.)'57.)21447,4(8)
12)0500548
! I.1/<=)%U)8+(7(8)12)
K"7*-"L
6(01=(B
! S<,7=(<,()!Wh)5@(8)%V?)$VVh)
14=(.)-'5<)bV
! _72(8+5<)78)$cAD#)=5>8
! M5-()5<=),1<-7</()-1)@.1;
! &(5)-.(()174)78),/..(<-4>)-'()
:(8-)-.(5-0(<-
" D)8+(,7(8)479()7<)'/05<8\))
21447,/41./0)5<=):.(978)d
,1001<4>)8((<)7<)-'()458'(8
$b
!"#$"$%
R7@' )I@(A=(+(<=(<-)F.(954(<,()12)
01(2#$&K"7*-"L&S<2(8-5-71<
!
K>(458' (8) 2.10)W#U)+(1+4();7-' )5@(8) 2.10)D)-1)c%)>(5.8) ;(.() (B507<(=) /<=(.) 5)47@' -)
07,.18,1+(` K"7*-"L 7<2(,-71<) ;58) ,4588727(=) 1<)-'() :5878) 12)+.(8(<,() 12)05-/.() 5<=)
45.954) 21.08)1. 52-(.) 1:8(.97<@) ,' 7-7<1/8 (B/975( N,>47<=.7,54) =5<=./22O)5227B(=)-1)-'()
8/:L(,-8) (>(458' (8`
$#h)7<)#)-1)$U)>(5.A14=
#Wh)7<)$c)-1)DU)>(5.A14=
%ch)7<)#$)-1)UV)>(5.A14=
!bh)7<)U$)-1)bV)>(5.A14=
cUh)7<)b$)-1)c%)>(5.A14=)
!
P(,5/8() 12)+.1-(,-79() :1<>)+.1-./871<?)1,/45.) K"7*-"L 78)' 5.=) -1)(.5=7,5-()
6(01=(B)M7-(8
! 6(01=(B) :4(+' 5.7-78) 78) -' ()
018-),1001<) :/-)19(.411C(=)
(B-(.<54) =78(58() +.1:4(0?)
,5/87<@) 1,/45.) 8/.25,()
7<245005-71<`)
! 3,/45.) 6(01=(B) 7<2(8-5-71<) 78)
' 5.=)-1)(.5=7,5-(`
! 6(01=(B ,5<) (B5,(.:5-() 05<>)
+.(A(B78-7<@) 1,/45.) 8/.25,()
,1<=7-71<8?) 47C() =.>) (>() 5<=)
+-(.>@7/0`) )
!"#$%"& ,$--*./-$(/#
!"#$%"& '(")*+
! H/0(.1/8) +/:47,5-71<8) '59()
8'1;<)-'5-)6(01=(B 12-(<)
+45>8) 5) .14() 7<):4(+' 5.7-78
Czep ita et a l (2 0 05 ) Kli n Oczn a ;1 07 :80 -2
Ru fli eta l (1 9 8 1 ) d erma to lo g ica ; 1 6 2 : 1 -11
Liu eta l (2 0 1 0 ) Cu rr Op in Allerg y Clin Immu n o l; 1 0 :5 0 5 -1 0
Z(878-5<-)-1)M5<>)E1<9(<-71<54)&.(5-0(<-8?):/-)
618(A=(+(<=(<-4>)j744(=):>)&&3
6(01=(B)&.(5-0(<-
! E5<<1-):()C744(=):>)B#@<&%6#7)**
! E5<<1-):()C744(=):>)MFN&O$*)/-*,"/*-/,"
! _58')=(:.7=(0(<-v))
" S<7-754)-.(5-0(<-\))=(:.7=()-'()458'(8)5<=)(>(:.1;8);7-')5)
,1--1<)-7+)5++47,5-1.)815C(=)7<)DVh)-1)UVh)-(5)-.(()174`
! E5<<1-):()C744(=):>)PQN*6*2
! E5<<1-):()C744(=):>).#1$*2/-"% 8/,')58)(.>-'.10>,7<
! &(5) -.(()174\))(B,(44(<-),1<,(<-.5-71<A=(+(<=(<-)
6(01=(BAC7447<@)+.1+(.-7(8
! E5<<1-):()C744(=):>)."+$*,/-#R*2"
! E5<<1-):()C744(=):>)SN&O/2*1#$)/,"
" $VVh)-(5)-.(()174)814/-71<)78)9(.>)7..7-5-7<@)5<=)8'1/4=):()
=74/-(=
" 3<(),5<)+.(+5.()5)07B-/.()12)UVh)-(5)-.(()174):>)=74/-7<@)
-'()-(5)-.(()174)7<)(7-'(.)05,5=5075)1.);54</-)174`
! j744(=)=18(A=(+(<=(<-4>):>)!"#&!$""&0/2&T!!0U
Gao et al, Br J Ophthalmol, 2005.
E47.5=(Bi
!
$),5.-1<)12)E47.5=(Bi) ,1<-57<8) DW)-1;(4(--(8
!
$),58() 12)E47.5=(Bi) ,1<-57<8) DV),5.-1<8)
Z(,100(<=(=)X85@(\
! K>()47="25,754),4(5<8(.
! &5.@(-8)=(01=(B
! E1<-57<8)oM(454(/,5)
I4-(.<721475p
" I)8+(,754)95.7(->)12)-(5)-.(()174)
;7-' )WA-(.+7<(14
!
Sy mpto m Sev erity
Frequency o f Use
Dura tio n
Clira dex ® Ca rtons
Per Indiv idua l
Mild - Mo dera te
1 x d aily
6 -8 week s
2 carto n s
Mo dera te - Sev ere
2 x d aily
6 -8 week s
4 carto n s
PD2;'2 ?%#62*-F$);F*2&'#2#'&=(7&)#=Q2
F&(6)#6&67#2(*2"#D )2);2)%#2=(*7'#)(;62;D 2)%#2
=;7);'R
$!
8/31/16
OcuSoft:Demodex ConvenienceKit
Demodexforthe
PrimaryCareEyeCareProvider
◆ Doesitwarrantthehype?
◆ Howdoyoudiagnoseit?
❖ Doyouneedmicroscopicconfirmation
◆ Whendoyoutreat?
Conjunctivochalasis
• Referstoachronic degenerativeloosening
andredundancyoftheconjunctiva
ConjunctivalChalasis
• Seenwithageingoftheocularsurface
• Mayalsoresultfromprolongedconjunctival
edemaasoccurswiththyroideyedisease,
ocularallergicconditionsandsomeorbital
tumours.
Conjunctivochalasis
• Almostallcasesofconjuctival chalasis
occurinthetemporalconjuctiva
• Advancedcasesofchalasis canresultin
exposureproblems
Symptoms
• Epiphorasecondarytoredundant
conjunctivalpreventionoftearflowtothe
punctum
• OftencoexistenceofdryeyeandCCh
– Dryeyesymptomsoftenexacerbated
– Makingthedistinctionb/wthe2canbedifficult
19