Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
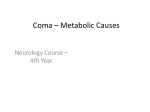
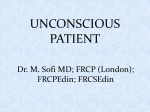
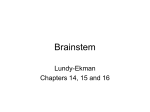
CHAPTER 16 Depressed Consciousness and Coma Benjamin S. Bassin and Jeremy L. Cooke PERSPECTIVE Epidemiology Depressed mental status represents an alteration in arousal and is a common presenting complaint in the emergency department (ED). This presentation can be the manifestation of a wide spectrum of diseases, with the degree of impairment ranging along a continuum from sleepiness to decreased alertness to frank coma. The differential diagnosis of stupor and coma is broad and diverse (Table 16-1) but can usually be categorized into metabolic and systemic, structural, or psychogenic causes. The majority of cases are caused by metabolic or systemic derangements, whereas the remainder are usually caused by structural lesions. Psychogenic presentations are much less common. The differential diagnosis for depressed level of consciousness often overlaps with that for confusion (see Chapter 17). Frequently, diagnosis and management occur simultaneously, and a structured systematic approach is used. A thorough grasp of the underlying pathophysiology leading to the acute depressed mental state will lead to timely diagnosis and treatment. Pathophysiology Consciousness is defined as the awareness of one’s self or sur roundings; it includes the properties of arousal and cognition. Alterations in arousal frequently are described as levels of consciousness, although they actually refer to dynamic points on a continuum ranging from fully alert to stuporous to comatose or complete unconsciousness. Conversely, cognition frequently refers to states of consciousness or awareness and is defined as the combination of orientation, the accurate perception of what is experienced; judgment, the ability to process input data to generate more meaningful information; and memory, the ability to store and retrieve information. There are many examples of medical states that alter cognition, including confusion, inattention, delusions, and dementia. However, these states do not depress the level of arousal and therefore are discussed in other chapters in this book. The ascending reticular activating system (ARAS) is the neuroanatomic structure primarily responsible for arousal and cortical activation. It is located in the paramedian tegmental zone in the dorsal part of the brainstem (Fig. 16-1). The input of somatic and sensory stimuli to the cerebral cortex is controlled by the ARAS and functions to initiate arousal from sleep. The brain’s cognition centers are located primarily in the cerebral cortex and serve to determine the content of consciousness. Insults to the cerebral cortex or brainstem can each independently cause depressed consciousness or coma. These structures 142 are vulnerable to metabolic derangements, toxins, or mechanical injury. Typically, both cerebral hemispheres need to be affected to induce coma, and this also depends on the size and speed of progression of the insult. Localized, unilateral lesions in the cerebral cortex usually do not induce depressed consciousness or coma even if other cognitive functions are impaired. In contrast, a completely intact brainstem is necessary for arousal. Small focal lesions in the brainstem can affect the ARAS. If the ARAS is impaired, the cerebral cortex cannot be aroused, and depressed consciousness or coma occurs. DIAGNOSTIC APPROACH Differential Considerations Potential causes of depressed consciousness can be divided into a few general categories. Metabolic or systemic causes of coma can include hypoxia, hypoperfusion, infection, toxic drug effects, or electrolyte disturbances. Hypoxia can be the result of congestive heart failure (CHF), pulmonary embolism, carbon monoxide poisoning, or severe pulmonary compromise such as occurs in chronic obstructive pulmonary disease (COPD), cystic fibrosis, and asthma. The various causes of shock can result in global hypoperfusion states leading to depression of consciousness. These include anaphylactic, septic, hypovolemic, cardiogenic, and neurogenic origins of shock. Each type of shock has its own unique characteristics, which are detailed in other chapters. Infection, both systemic (sepsis) and focal, can be another general cause of depressed consciousness. This is particularly true if central nervous system (CNS) structures are involved, as in meningitis, encephalitis, or CNS abscess. Toxic drug effects ranging from recreational drug use and intentional overdoses to therapeutic doses with adverse side effects are common general causes of depressed consciousness seen in the ED. In the elderly, adverse side effects from prescription medications are common. In addition, electrolyte and glucose abnormalities can be caused by multiple conditions, including diabetes, renal dysfunction, malignancy, and medication interactions or dosage errors. Head trauma, stroke, tumor, and infection are the most common structural causes of coma and depressed consciousness. Traumatic causes can include subdural and epidural hematomas, intraparenchymal or subarachnoid hemorrhage, or simply contusion or concussion. Strokes occur with embolic, thrombotic, or hemorrhagic mechanisms, but it is extremely unusual for ischemic (i.e., nonhemorrhagic) stroke to depress consciousness unless a massive insult to both hemispheres has occurred (e.g., diffuse severe cerebral edema after a massive infarct) or a high-grade basilar artery stenosis or occlusion is present.1 Depression of consciousness with CNS infections may be caused by mass effect and is common with Chapter 16 / Depressed Consciousness and Coma 143 Table 16-1 Differential Diagnosis ORGAN SYSTEM CRITICAL DIAGNOSES EMERGENT DIAGNOSES NONEMERGENT DIAGNOSES Neurologic or CNS Hemorrhage • Subarachnoid • Pontine • Cerebellar • Intracerebral Ischemic stroke Status epilepticus Acute hydrocephalus Subdural hematoma Epidural hematoma Acute hydrocephalus Primary brain tumor Metastatic disease Venous sinus thrombosis CNS vasculitis Pseudotumor cerebri Seizures (limited) Concussion or contusion Infectious Bacterial meningitis Encephalitis Septic shock Brain abscess Viral meningitis Sepsis from other sources Metabolic Hypoglycemia Hyperglycemia (DKA, HONK) Thiamine deficiency (Wernicke-Korsakoff syndrome) Hyponatremia or hypernatremia Hypocalcemia or hypercalcemia Hyperammonemia Myxedema coma Thyrotoxicosis Uremia Porphyria Hypophosphatemia Hypomagnesemia or hypermagnesemia Hypoparathyroidism or hyperparathyroidism Toxic Carbon monoxide Cyanide Heroin or opiates Beta-blockers Calcium channel blockers Cardiac glycosides (digoxin) Tricyclic antidepressant Alcohol Benzodiazepines Cocaine, amphetamines γ-Hydroxybutyrate (GHB) Isoniazid Organophosphates Acetaminophen Anticonvulsants Aspirin Lithium PCP SSRIs Marijuana LSD Mushrooms NSAIDs Environmental High-altitude cerebral edema Heat stroke Hypothermia Malignant hyperthermia Neuroleptic malignant syndrome Dysbarism Pulmonary, hypoxia Anaphylaxis Pulmonary embolus Asthma, COPD Cardiovascular Acute MI Aortic dissection Cardiogenic shock Cardiac tamponade Hypovolemic shock Hypertensive crisis Malignant arrhythmia Congestive heart failure Anemia CNS, central nervous system; COPD, chronic obstructive pulmonary disease; DKA, diabetic ketoacidosis; HONK, hyperosmolar nonketotic coma; LSD, lysergic acid diethylamide; MI, myocardial infarction; NSAIDs, nonsteroidal anti-inflammatory drugs; PCP, phencyclidine; SSRIs, selective serotonin reuptake inhibitors. severe bacterial meningitis, cerebral abscess or empyema, or parasitic mass. Malignancies, whether primary or metastatic, can cause depressed consciousness if the tumor mass elevates intracranial pressure (ICP) or reduces cerebral blood flow, or if surrounding edema develops rapidly. Special consideration should be given to specific populations of patients. The elderly, in particular, are susceptible to alterations in therapeutic medication dosage and drug-drug interactions. Even seemingly minor infections, such as urinary tract infections, upper respiratory infections, or viral gastroenteritis, may cause altered mental status (see Chapter 13), depressed consciousness, or coma. In addition, immunocompromised patients with acquired immunodeficiency syndrome (AIDS) or those undergoing chemotherapy treatments for transplants, and patients with malignancy or immunologic disease are vulnerable to a multitude of opportunistic infections not commonly seen in the general patient population. The clinical evaluation and stabilization of patients with depressed consciousness occur simultaneously with the diagnosis in the ED. The differential diagnosis of depression of consciousness is extensive but can be greatly simplified by focusing attention on the distinguishing characteristics of the available patient history and physical examination (Box 16-1).2 Approaching the patient’s presentation systematically, beginning with a broad differential diagnosis, usually allows development of a short list of likely diagnoses early in the encounter. 144 PART I ◆ Fundamental Clinical Concepts / Section Two • Cardinal Presentations Medial geniculate body Inferior brachium Optic tract Pulvinar Pineal body Optic commissure Superior colliculi Inferior colliculi Peduncle of cerebrum Frenulum veli Trochlear nerve Lateral lemniscus Superior peduncle Oculomotor nerve Pons Trigeminal nerves Middle peduncle Rhomboid fossa Acoustic nerve Facial nerve Abducent nerve Clava Figure 16-1. Brainstem anatomy. (Adapted Hypoglossal nerve Glossopharyngeal and vagus nerves from Adams J: Emergency Medicine. Philadelphia: Elsevier; 2008.) BOX 16-1 Structural Etiology of Altered Mental Status and Coma Trauma Subdural hematoma Epidural hematoma Cerebral concussion or contusion Stroke Syndromes Embolism Cardiac (atrial fibrillation, endocarditis) Paradoxical (fat embolus) Thrombosis Cerebral venous sinus thrombosis Hemorrhage Subarachnoid hemorrhage (SAH) Pontine hemorrhage Cerebellar hemorrhage Intracerebral hemorrhage Tumor Brainstem tumors Metastatic disease Angiomas Pituitary apoplexy Acute hydrocephalus Infection Subdural empyema or abscess Pivotal Findings History Chief complaints relating to depressed consciousness vary widely. Family members may report the patient as being more difficult to arouse from sleep or less interactive. Often, family members or friends have alerted emergency medical services after the patient is “found down” or unarousable even with vigorous stimulation. Often, information from alternate sources guides the diagnostic workup. Common sources of information include family members, neighbors, prehospital personnel, law enforcement, and nursing home staff.3 They may know of preceding symptoms such as headache, nausea, vomiting, or fever. Key historical information includes the rate of symptom onset, a history of trauma, exposure to drugs or toxins, or new medications or change in dosage. Rate of symptom onset is important, as an abrupt onset of decreased alertness may suggest structural phenomena or vascular insult, whereas a gradual onset would be more indicative of the slow, indolent course frequently seen with toxic, metabolic, or infectious causes. Family members usually have some knowledge regarding the patient’s past medical history, which may include diabetes, liver or renal disease, vascular disease such as hypertension, coronary disease, stroke or transient ischemic attacks, malignancy, seizures, immunocompromised states such as human immunodeficiency virus (HIV) infection, sickle cell disease, organ transplantation, or psychiatric illness. Family members may also be able to relay additional diagnostic clues such as rate of onset or waxing-waning characteristics of the patient’s symptoms. In addition, previous medical records should be reviewed whenever possible to augment or confirm the information provided. Items with the patient such as a card in the wallet containing lists of medical conditions and/or medications or a medical alert bracelet or necklace can provide valuable information. If the patient’s historical baseline mental status cannot be established, the current presentation is assumed to be an acute change.4 Causes of depression of consciousness vary with patient age (Box 16-2). The elderly are particularly vulnerable to infectious causes, medication changes, and alterations in their living environments. Young adults and adolescents are more likely to be affected after recreational drug use or trauma. Accidental toxic ingestions are often seen in younger children. In infants, infectious Chapter 16 / Depressed Consciousness and Coma 145 BOX 16-2 Common Age-Related Etiology of Altered Mental Status Infant Infection Trauma, abuse Metabolic Child Toxic ingestion Adolescent or Young Adult Toxic ingestion Recreational drug use Trauma Elderly Medication changes Over-the-counter medications Infection Alterations in living environment Stroke causes of depressed consciousness are most common; however, trauma secondary to physical abuse and metabolic derangements from inborn errors of metabolism can be seen.5 Physical Examination The severity of presenting symptoms dictates the speed needed for stabilization and diagnosis. After necessary stabilization measures have been instituted (e.g., intubation of the frankly comatose patient), a systematic physical examination is conducted. Level of consciousness is determined by the patient’s ability to speak in full, coherent sentences and to respond appropriately to the examiner. A rapid, directed neurologic screening examination can determine whether the patient has a significant focal motor deficit. The presence of a distinctive odor on the breath, although uncommon, can cue the examiner to the presence of alcohol, ketones (diabetic or alcoholic ketoacidosis), or bitter almonds (cyanide toxicity). Undressing the patient completely permits evaluation for signs of trauma or skin lesions suggesting overwhelming infection or needle track marks. Significant hypotension with depressed consciousness suggests shock with resultant cerebral hypoperfusion, and both causes and therapy should be addressed immediately. Hypertension can be seen as a result of subarachnoid hemorrhage or cerebral or brainstem infarction or may be secondary to any condition resulting in increased ICP. Late-stage, severe elevation in ICP can cause bradycardia and hypertension, also known as the Cushing reflex. This is an ominous sign and is seen most commonly in lesions affecting the posterior fossa and in children. Bradycardia is also seen in medication overdoses such as with beta-blockers, calcium channel blockers, cardiac glycosides, and clonidine. Myocardial conduction blocks may also cause severe bradycardia, hypotension, and subsequent stupor or coma. Tachycardia has a broad differential in the altered patient and can be the result of hypovolemia, fever, severe anemia, thyrotoxicosis, and drugs such as anticholinergics and stimulants. Both hypothermia and hyperthermia can result in altered mental status whether from infectious, structural, toxic or metabolic, or environmental causes. Hyperventilation, Kussmaul’s or Cheyne-Stokes breathing, agonal breathing, apnea, or other alterations in respiratory patterns can suggest primary CNS abnormalities or toxic or metabolic derangements. Changes in respiratory patterns can be challenging for the clinician in an unresponsive patient, as they can represent the sequelae of a primary CNS insult or compensation for an underlying toxic or metabolic process. BOX 16-3 Glasgow Coma Scale Eye opening Verbal response Adult Pediatric Motor response Spontaneous To voice To pain None Oriented Confused Inappropriate words Incomprehensible words None Appropriate Cries, consolable Persistently irritable Restless, agitated None Obeys commands Localizes pain Withdraws to pain Flexion to pain Extension to pain None Score 4 3 2 1 5 4 3 2 1 5 4 3 2 1 6 5 4 3 2 1 Immediately after an assessment of the patient’s vital signs, a head-to-toe physical examination is performed.6 A methodical and complete head and neck examination is conducted, with particular emphasis on examination of the pupillary reflexes and eye movements (see later discussion) and any indications of head trauma, including hemotympanum, periorbital ecchymosis, Battle’s sign, scalp hematoma, or CSF otorrhea or rhinorrhea. The hydration of the mucous membranes may give clues to specific toxidromes. Laceration or bruising of the tongue may indicate a recent seizure. Examination of the neck should focus on evidence of meningismus, which can be seen in meningitis, subarachnoid hemorrhage, and some cases of herniation. The cervical spine should be immobilized if there are signs of neck trauma, such as cervical spine tenderness or evidence of blunt external trauma, or if the history indicates a potential mechanism for neck injury. Stridor indicates respiratory distress typically from infection, allergic reaction, or foreign body aspiration. Presence of a goiter may indicate underlying thyroid pathology. Cardiopulmonary examination should focus on respiratory effort, ventilatory patterns, presence of arrhythmia or murmurs, cardiac output, and the presence of injury. Potentially helpful abdominal findings include hepatosplenomegaly, pulsatile masses, ecchymosis, or sequelae of liver failure such as ascites, caput medusa, or spider angiomata. Gross blood, purulent drainage, or retained foreign bodies should be sought on genitourinary and rectal examination. In the absence or presence of signs of trauma, lesions on the skin such as rashes, signs of drug use (needle tracks or medication patches), or embolic phenomena can be differential clues. A systematic neurologic examination, with particular attention paid to the eyes, is the most useful tool in differentiating a structural from a systemic or metabolic cause of depressed consciousness or coma. A head-to-toe approach is a proven strategy. This should include evaluation of the patient’s Glasgow Coma Scale (GCS) score (Box 16-3), level of alertness, cranial nerves, strength, reflexes, and cerebellar functions with emphasis on gait, pronator drift, finger-to-nose, heel-to-shin, rapid alternating movements, and Romberg testing. The GCS measures the best motor and verbal responses and the degree of stimulus required to elicit eye 146 PART I ◆ Fundamental Clinical Concepts / Section Two • Cardinal Presentations opening and is measured serially, as level of consciousness frequently is dynamic after the initial insult and subsequent response to therapy. The GCS does not differentiate among causes of altered mental status or coma or assess cognition but is useful in monitoring changes in mental status when serial examinations are performed and serves as an objective reference for communicating with consultants.7 A change of two or more points in serial GCS testing represents a significant change. Discovery of a focal neurologic deficit is suggestive of a structural cause. Particular attention should be paid to a focused eye examination, during which a helpful amount of information can be obtained. Unilateral dilatation of a pupil (“blown pupil”) and loss of reactivity in a comatose patient are ominous signs of uncal herniation and necessitate immediate neurosurgical consultation and intervention. Papilledema, which may indicate increased ICP or retinal hemorrhages associated with trauma, can be identified on funduscopic examination. The eye examination should also include testing of eye movements, which are coordinated by the medial longitudinal fasciculus located in the brainstem and ocular centers located in the cerebral cortex. Cranial nerves III, IV, and VI are responsible for control of the extraocular muscles. Cranial nerve III paralysis results in a persistently abducted eye, whereas a persistently adducted eye is caused by paralysis of cranial nerve VI. In the setting of trauma, a unilateral third cranial nerve palsy suggests an ipsilateral compressive lesion such as seen with epidural hematoma. Cranial nerve VI palsies are often nonlocalizing, as the nerve has a long intracranial course and compressive forces from intracranial mass effects (e.g., tumor, traumatic hematoma, increased ICP) may compromise cranial nerve function anywhere in its course. Horizontal disconjugate gaze is an important finding and is commonly seen in patients who are sedated, drowsy, or intoxicated. Disconjugate gaze found in the vertical plane is usually more serious and suggests cerebellar or pontine dysfunction. Normal ocular motility suggests that a significant portion of the brainstem remains intact. Oculocephalic (doll’s eyes) and oculovestibular reflex testing are useful in looking at the functional integrity of the brainstem. These tests, if results are negative, make structural lesions in the brainstem very unlikely as the source of the patient’s altered mental status. If there are no contraindications, such as suspected cervical spine injury, oculocephalic testing is accomplished by observing the patient’s eye movements while the head is turned from side to side. Patients who exhibit a maintained forward gaze despite head turning (doll’s eye reflex) are unlikely to have a brainstemmediated cause of coma. If the eyes remain in a fixed position within the orbits, turning in unison with the head, brainstem dysfunction is suggested. Oculovestibular or “cold water caloric” testing is a more sensitive test for brainstem involvement and cannot voluntarily be resisted (Fig. 16-2). After elevation of the patient’s head to 30 degrees (this can be done in patients whose cervical spine is not cleared by placing the bed in the reverse Trendelenburg position), 10 to 30 mL of ice water is used to irrigate the external auditory canal. Tympanic membrane perforation and cerumen impaction should be ruled out before this test is performed. In patients who have an intact brainstem, the response is a slow conjugate deviation of gaze toward the side of the cold water stimulus for 30 to 120 seconds. The reflex is short-lived and followed by corrective fast beats of nystagmus toward the midline. This corrective nystagmus is described by the mnemonic COWS, which stands for “cold-opposite, warm-same.” If there is no response to the irrigation, brainstem dysfunction is possible. Recently, literature on the phenomenon of basilar artery stenosis or occlusion manifesting as depressed consciousness or coma has increasingly been published. A review of the Lausanne Stroke Registry showed that 100% of patients with poor outcome from high-grade basilar stenosis or occlusion had either stupor or Ice water irrigation right ear Alert wakefulness (nystagmus with rapid movement opposite side of cold stimulation) Bilateral cerebral hemisphere dysfunction Left MLF dysfunction Brainstem dysfunction Left oculomotor nerve dysfunction Figure 16-2. Oculocephalogyric (caloric) responses to various central nervous system pathologic conditions. MLF, medial longitudinal fasciculus. coma or the triad of pupillary abnormalities, dysarthria, and bulbar findings on presentation.1 Ancillary Testing (Refer to Table 16-2) Laboratory Studies Bedside glucose testing definitively confirms or excludes hypoglycemia and can frequently limit further extensive metabolic testing in diabetic or intoxicated patients. Serum electrolytes and renal function measurement identify the presence of a metabolic acidosis, anion gap, uremia, or derangements in sodium or potassium. Changes in serum calcium can be a marker for metastatic disease, and severe hypercalcemia can cause altered mental status. Arterial blood gas analysis rapidly assesses acid-base status and the presence of hypercarbia or hypoxia and allows calculation of arterialalveolar gradient in conditions in which shunting is suspected. Carbon monoxide (CO)–oximetry can be added to confirm methemoglobinemia or carbon monoxide exposure. A urine dip test is a quick way to screen for the presence of ketones, the spilling of glucose as seen in hyperosmolar states, or infection, which can frequently precipitate changes in mentation, especially in the elderly. Urinalysis itself provides valuable information regarding hydration status (specific gravity) and the possible presence of calcium oxalate crystals in the setting of ethylene glycol ingestion. Urine drug testing may confirm a suspected ingestion or be helpful if another cause is not readily apparent. Chapter 16 / Depressed Consciousness and Coma 147 Table 16-2 Ancillary Testing in the Altered Patient TEST FINDING POTENTIAL DIAGNOSIS Hypoxemia Hypercarbia Metabolic vs. respiratory acidosis Pulmonary embolus, intracranial event, central hypoventilation, CHF Laboratory ABGs A-a Gradient Obstructive or restrictive pulmonary condition, high altitude cerebral edema, intracerebral process Multiple—DKA, toxic ingestion, sepsis, respiratory failure Pulmonary embolus Electrolytes Carboxyhemoglobin—elevated Sodium—increased Sodium—decreased Carbon monoxide exposure (consider cyanide in inhalational exposure) Dehydration, diuretic overuse, diabetes insipidus, osmotic diuresis Adrenal insufficiency, CHF, cirrhosis, DKA, infant formula dilution, myxedema coma, renal failure, SIADH BUN, creatinine, glucose Complete blood count Bicarbonate—decreased Calcium—elevated BUN, creatinine-elevated Glucose-elevated Decreased WBCs—elevated WBCs—decreased Hgb and Hct—elevated Hgb and Hct—decreased Platelets—elevated Platelets—decreased Metabolic acidosis—multiple causes (anion vs. non–anion gap) Malignancy, hyperparathyroidism, thyrotoxicosis Acute renal failure, uremia DKA, hyperosmolar hyperglycemic state (HHS) Alcohol abuse, cirrhosis, insulin overdose, sepsis Nonspecific—infection, inflammation, steroids, stress Immunocompromised—malignancy, drug, alcohol, or viral marrow suppression Polycythemia Severe anemia Hereditary thrombocytosis, acute phase reactant Sepsis, DIC, intracranial hemorrhage Coagulation ammonia PT and INR—elevated Elevated Bleeding dyscrasias, liver disease, warfarin use Hepatic encephalopathy, valproic acid toxicity, inborn errors of metabolism Thyroid studies Elevated Decreased WBCs—elevated Thyrotoxicosis Myxedema coma Meningitis Cerebrospinal fluid RBCs—elevated Specific gravity—elevated Subarachnoid hemorrhage Dehydration Urinalysis WBCs, leukocyte esterase, nitrites RBCs—elevated Glucosuria Calcium oxalate crystals Urinary tract Infection Retroperitoneal hemorrhage DKA, HHS Ethylene glycol ingestion Ingestion Urine drug screen Multiple possibilities Imaging Head CT—non-contrast Head CT—contrast CT angiography or venography MRI Chest radiograph Ultrasound Other Studies ECG EEG Blood Enlarged ventricles Mass or edema Mass or edema Ring-enhancing lesion Vascular clot Vascular dilation Hypoperfusion Mass Meningeal enhancement Consolidation or mass Pulmonary edema Radiolucency, mediastinal shift Widened mediastinum Hampton’s hump, Westermark’s sign Intra-abdominal blood ST segment changes, Q waves T wave inversions Abnormal intervals Osborne wave (J wave) Right-sided heart strain Multiple findings Intracerebral hemorrhage, epidural hematoma, subdural hematoma, subarachnoid hemorrhage, hemorrhagic stroke Obstructive hydrocephalus, shunt malfunction Ischemic stroke, tumor, or metastatic disease Tumor, metastatic disease Abscess Basilar or vertebral artery occlusion or stenosis, venous sinus thrombosis Aneurysm, arteriovenous malformation, Ischemic stroke, basilar or vertebral artery occlusion or stenosis, venous sinus thrombosis Tumor, metastatic disease, abscess (superior to CT for posterior fossa lesions) Meningitis, encephalitis, neurosarcoidosis, carcinomatosis, post–lumbar puncture Pneumonia, tumor, foreign body CHF, cardiogenic shock Pneumothorax Aortic dissection Pulmonary embolus Ruptured abdominal aortic aneurysm; spleen, kidney, or liver laceration (trauma) Ischemia or infarction Ischemia, intracerebral hemorrhage Conduction blocks, drug ingestion, electrolyte abnormality Hypothermia Pulmonary embolus Status epilepticus (convulsive or nonconvulsive) ABGs, arterial blood gases; BUN, blood urea nitrogen; CHF, congestive heart failure; CT, computed tomography; DIC, disseminated intravascular coagulation; DKA, diabetic ketoacidosis; ECG, electrocardiogram; EEG, electroencephalogram; Hct, hematocrit; Hgb, hemoglobin; INR, international normalized ratio; MRI, magnetic resonance imaging; PT, prothrombin time; RBCs, red blood cells; SIADH, syndrome of inappropriate antidiuretic hormone secretion; WBCs, white blood cells. 148 PART I ◆ Fundamental Clinical Concepts / Section Two • Cardinal Presentations A complete blood count can be useful. Although an elevated white blood cell count can be a marker for infection, it is nonspecific and rarely helpful in discerning a toxic or metabolic cause. An abnormally low white blood cell count, however, suggests an immunocompromised state and should urgently direct clinical investigation toward an infectious cause. Profound anemia may be seen from witnessed or occult blood loss. Thrombocytopenia can be a marker for sepsis, intracranial hemorrhage, or disseminated intravascular coagulation. Elevated results from serum coagulation studies can be a marker for bleeding dyscrasias, liver disease, or supratherapeutic levels of anticoagulation drugs. Both platelets and coagulation studies should be checked before invasive procedures are performed at noncompressible sites such as lumbar punctures and central venous access, if the patient’s condition allows. Serum ammonia levels are controversial and have not been shown to be a reliable marker for the cause of depressed consciousness. Although usually associated with severe liver disease, ammonia levels can be elevated in other conditions such as valproic acid toxicity and inborn errors of metabolism and can be normal in patients with hepatic encephalopathy.8 Thyroid function studies can help confirm myxedema coma or thyrotoxicosis. When CNS pathology such as infection or hemorrhage is suggested but not seen on neuroimaging studies, cerebrospinal fluid analysis is undertaken. Imaging Studies Noncontrast computed tomography (CT) of the brain is the initial imaging modality of choice in the setting of depressed consciousness and coma. In the majority of ED settings, it is available and quickly obtained, and this makes CT more suitable than other imaging tests for the patient with borderline hemodynamic instability. Brain CT is sufficiently sensitive to detect most intracranial hemorrhages that are large enough to cause coma. In addition, the presence of hydrocephalus can quickly be assessed. Despite its utility, linear artifacts created by the thick skull base can limit the view of the posterior fossa on CT. In this case, magnetic resonance imaging (MRI) of the brain is generally much better for identifying structural lesions in this region. However, this modality is less practical in most ED settings because of its cost, limited availability, and duration of acquiring each study, which consequently limits the ability to monitor or access the unstable patient.4 Contrast-enhanced CT may be used if a tumor, metastatic disease, or intracerebral infection is suspected. CT or magnetic resonance angiography or venography may be available in larger tertiary care centers for use in the diagnosis and/or treatment of intracerebral aneurysms, arteriovenous malformations, cerebral venous sinus thrombosis, or basilar or vertebral artery stenosis or occlusion. Plain radiography may identify severe pneumonia or acute respiratory distress syndrome. In ingestions, it may rarely reveal specific types of heavy metals such as mercury, iron, or lead in the pediatric population or packages of ingested illicit substances in body packers or stuffers. Additional Testing Electrocardiograms (ECGs) can reveal cardiac ischemia, conduction blocks, or arrhythmia or can help corroborate certain ingestions (tricyclic antidepressants), electrolyte abnormalities (e.g., potassium, calcium), or hypothermia. If nonconvulsive status epilepticus is suggested, or if a patient with status epilepticus has required neuromuscular blockade, continuous electroencephalographic monitoring, if available, can provide key information about the patient’s status and guide therapy. DIAGNOSTIC ALGORITHM Critical diagnoses to consider are listed in Table 16-1. Information gathered from the history and physical examination of the patient with depressed consciousness is used to direct the approach to diagnostic testing. Most often, this information points toward a systemic or metabolic cause rather than a structural cause. Neuroimaging studies are performed early in patients with suspected structural causes but should not precede treatment of quickly reversible conditions such as opioid overdose or hypoglycemia. Systemic or metabolic causes of depressed consciousness and coma are most often found on analysis of laboratory studies. Consequently, in the undifferentiated patient, diagnostic tests should be performed in parallel whenever possible to avoid unnecessary delays in initiation of treatment. Similarly, owing to the severe morbidity and mortality associated with many causes of depressed consciousness and the ability for rapid reversal of several conditions, initial stabilization, treatment, and assessment are performed simultaneously. A logical approach to the history, physical examination, and diagnostic testing is presented in Figure 16-3. EMPIRICAL MANAGEMENT Initial establishment of airway, breathing, and circulation (ABCs) is of primary importance in stabilizing the patient with altered mental status. Initiation of intravenous access combined with the administration of oxygen and continuous telemetry monitoring should happen concomitantly within the first few minutes of the patient’s arrival.2 In patients with a GCS score lower than 8, intubation is indicated unless the coma is readily reversible, such as that caused by hypoglycemia or opioid overdose (see Chapter 1). All patients should receive a thorough neurologic examination before sedation and chemical paralysis for intubation. Trauma patients require spinal immobilization in addition to indicated fluid resuscitation. Reversible causes of the patient’s condition should be sought concomitantly with initial stabilization. Administration of the components of the “coma cocktail,” which include dextrose, naloxone, and thiamine, can quickly reverse the alterations in mental status caused by hypoglycemia, narcotic overdose, and thiamine deficiency, respectively, and can substantially narrow the differential diagnosis. Bedside capillary blood glucose, blood, and urine studies should be sent while ECG and emergent noncontrast head CT are ordered. Further therapy and workup will be dictated by the patient’s history and physical examination. Specific attention should be given to identifying the focal neurologic abnormalities, including pupillary reflexes and pathologic eye movements that suggest mass effect or depressed brainstem function, prompting neuroimaging and evaluation by a neurosurgeon. Empirical administration of mannitol and elevation of the head of the bed are indicated when there is clear evidence of transtentorial herniation (see Chapters 41 and 101). In patients with compromised brainstem function who lack evidence of herniation, investigation of possible exposure to toxins or metabolic imbalances should proceed with consideration of basilar artery or bilateral vertebral artery occlusion requiring CT or magnetic resonance angiography. Basilar stenosis or occlusion is one of the few stroke syndromes that can manifest as stupor or coma, and administration of antiplatelet, anticoagulation and thrombolytic agents should be considered in consultation with a neurologist or stroke team. In patients who demonstrate normal brainstem function, the workup proceeds as supportive care is provided. When an infectious cause is suggested, empirical administration of a broadspectrum antibiotic should not be delayed for lumbar puncture or other diagnostic tools.9 Lesions or masses found on brain Chapter 16 / Depressed Consciousness and Coma 149 Initial assessment: Vital signs Airway, breathing, circulation IV, oxygen, monitor Bedside glucose Narcan No gag reflex, GCS < 8 RSI History/suggestion of trauma? Yes No History/suspicion of infection? C-spine immobilization Yes Signs of impending herniation? • Cushing’s response (↑ BP, ↓ HR) • Unilateral blown pupil Yes No IV antibiotics Consider steroids Toxic/metabolic workup ECG CT CT Toxic/metabolic etiology? No Elevate head Neurosurgery consult ↑ RR (PCO2 ~ 35 mm Hg) Mannitol Craniotomy/ventriculostomy CT/OR CT Yes Lesion on CT? Lesion on CT? Yes Yes No Neurosurgery consult OR Neurosurgery consult OR Toxic/ metabolic etiology? Yes Treat appropriately No Treat appropriately Lumbar puncture Yes Continue antibiotics Admit to ICU Neurology consult Lesion on CT? Yes Lumbar puncture No Neurosurgery consult OR Infection? No No Hemorrhage? No Toxic/ metabolic workup Lumbar puncture Yes Neurosurgery consult Angiography OR No Anoxia CVA MRI Neurology consult Figure 16-3. Algorithm for diagnostic approach to altered mental status and coma. BP, blood pressure; C-spine, cervical spine; CT, computed tomography of brain; CVA, cerebrovascular accident; HR, heart rate; ICU, intensive care unit; IV, intravenous; OR, operating room; RR, respiration rate; RSI, rapid sequence intubation. (Adapted from Adams J: Emergency Medicine. Philadelphia: Elsevier; 2008.) 150 PART I ◆ Fundamental Clinical Concepts / Section Two • Cardinal Presentations imaging should prompt evaluation by a neurosurgeon and, if indicated, early operative intervention. In patients in whom a toxic ingestion is possible, activated charcoal is of little benefit in most cases. Specific toxin antidotes, if indicated, can be given, with consultation with a local or regional poison center when required. Early hemodialysis after consultation with a nephrologist should also be considered in patients who have toxic or metabolic abnormalities amenable to this therapy. DISPOSITION Patients with structural lesions on imaging require immediate neurosurgical consultation and frequently will require operative intervention. Patients are urgently transferred to a center with neurosurgical capabilities once hemodynamically stabilized if these services are not available at the site of initial patient presentation. The vast majority of patients with depressed consciousness or coma require admission to the hospital for further treatment and workup. Some patients who have returned to their baseline mental status after reversal of hypoglycemia or opioid overdose may be suitable for discharge directly from the ED or ED observation unit after a period of observation. Patients with alcohol or recreational drug intoxication and no other discernible cause of altered mental status can be discharged when they are clinically sober. The references for this chapter can be found online by accessing the accompanying Expert Consult website. Chapter 16 / Depressed Consciousness and Coma 150.e1 References 1. Devuyst G, et al: Stroke or transient ischemic attacks with basilar artery stenosis or occlusion: Clinical patterns and outcome. Arch Neurol 2002; 59:567-573. 2. Hoffman RS, Goldfrank LR: The poisoned patient with altered consciousness. Controversies in the use of a “coma cocktail.” JAMA 1995; 274:562-569. 3. Kanich W, et al: Altered mental status: Evaluation and etiology in the ED. Am J Emerg Med 2002; 20:613-617. 4. American College of Emergency Physicians: Clinical policy for the initial approach to patients presenting with altered mental status. Ann Emerg Med 1999; 33:251-281. 5. Kirkham FJ: Non-traumatic coma in children. Arch Dis Child 2001; 85:303-312. 6. Bateman DE: Neurological assessment of coma. J Neurol Neurosurg Psychiatry 2001; 71(Suppl 1):i13-i17. 7. Koita J, Riggio S, Jagoda A: The mental status examination in emergency practice. Emerg Med Clin North Am 2010; 28:439-451. 8. Elgouhari HM, O’Shea R: What is the utility of measuring the serum ammonia level in patients with altered mental status? Cleve Clin J Med 2009; 76:252-254. 9. Brouwer MC, et al: Nationwide implementation of adjunctive dexamethasone therapy for pneumococcal meningitis. Neurology 2010; 75:1533-1539.