Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Sound localization wikipedia , lookup
Specific language impairment wikipedia , lookup
Evolution of mammalian auditory ossicles wikipedia , lookup
Auditory system wikipedia , lookup
Sign language wikipedia , lookup
Deaf culture wikipedia , lookup
Telecommunications relay service wikipedia , lookup
Video relay service wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Hearing loss wikipedia , lookup
Sensorineural hearing loss wikipedia , lookup
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
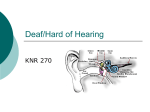
Hearing Loss, Deaf Culture and ASL Interpreters By Laura Jacobsen (4/2014) “Being deaf is a worse handicap than being blind because deafness separates people from people.” -Helen Keller Goals of the Newborn Hearing Screening: o Have all babies screened for hearing at birth, or by 1 month of age. o For all babies with hearing loss, have them diagnosed by 3 months of age and receiving appropriate early intervention services by 6 months of age. (“1-3-6”) o If they fail (“refer”) the first hearing screen (on either ear or both) then they need to be rescreened before 1 month of age. This just needs to be another ABR – there is currently no order for this. Call Christy “Chris” Randall at 966-1993, leave a message, or page at 216-6191. o May not have passed the initial screen due to: fluid in the middle ear, vernix in the ear canal, too much movement/crying during the test, etc. o If they fail (“refer”) the re-screen then they need referral to Pediatric Audiology for a full evaluation (before they are 3 months old). o If they are diagnosed with hearing loss then they need referral to CDSA/Early Intervention and will also be followed by ENT and Audiology. Exposure to LANGUAGE as early as possible is what matters (amplification devices, cochlear implants, oral language, cued speech, Sign English, American Sign Language… something)! Hearing Tests 1) ABR (Auditory brainstem response): analyzes the cochlea and auditory nerve response to sound from an earphone and receives the signals through electrodes on the head. Baby must be napping (quiet and still). 2) OAE (Otoacoustic emissions): sound is produced in an earphone causing the outer hair cells of the cochlea to vibrate producing a sound that echoes back to the probe in the ear. Need quiet environment. 3) Audiometry (or Pure-tone testing): tests the faintest tones (decibels) a person can hear at selected frequencies (Hertz) through earphones. Must be able to indicate that the sound was heard, and preferably which ear. @ birth (NC newborn hearing screen website: http://www.ncnewbornhearing.org) - UNC does ABR in the Newborn Nursery (either ABR or OAE can be done in the newborn period) @ ages 4, 5, 6, 8, and 10. - By age 4, child is able to respond to auditory stimulus (maybe not which ear) by Pure-tone Audiometry (Kindergarten forms) - Assess risk yearly (i.e. risk factorsⱡ, abnormal speech development) and screen as needed history, physical exam (otoscopy, tympanometry) Audiology referral if no signs of ear infection or fluid For deaf or hard-of-hearing children in schools: - Mainstream schools versus schools for the Deaf or residential schools - To be successful children need to be placed in appropriate classrooms based on their language, reasoning, conversational and social skills - The Individuals with Disabilities Education Improvement Act (IDEIA, 2004) mandates a "free and appropriate public education" in the "least restrictive environment" and this needs to be spelled out in the IEP (type of assistive devices, who cares for them, accommodations in class, etc.) with the help of teachers, administrators, Speech-Language Pathologists, Audiologists, and Pediatricians - Resources for families: ASHA http://www.asha.org/Publications/leader/2005/050927/f050927a.htm, Early Hearing Detection & Intervention (EHDI) Program http://www.ncnewbornhearing.org/ Deaf Culture Signing Exact English ASL Ways to communicate - Oral: encompasses speech, lip-reading, cued speech plus writing, gesturing and amplification devices as appropriate (FM systems in schools, hearing aids, cochlear implants) - Sign: includes Sign English to American Sign Language - Total communication uses both speech and signing to communicate 92% of deaf children are born into all hearing families. 96% of those parents are not able to communicate with their own deaf children. Deaf communities gather around deaf schools: http://www.csdf.k12.ca.us/deafschools/site/main_site.htm Interaction - Get deaf patient or family member’s attention: walk slowly into eye line, flip light switch once from door Do not: stamp on floor or wave hands in front of face. Try to avoid touching deaf person - Ask their preference for communicating: lip reading, sign language interpreter, writing, etc. - In a pinch write notes, text on phones - The ADA (Americans with Disabilities Act) requires the use of a certified interpreter (not a family member). - As with all interpreting, face your client so they can see your mouth, ignore the interpreter - Do not speak loudly or exaggerated, just speak clearly and without covering your mouth or too much extraneous movement (decrease distractions) “Deaf and dumb” Interpreters Deaf vs. deaf UNC - Chapel Hill A Sign Language interpreter is available via a laptop in Patient Relations which is located on the ground floor of the Women’s Hospital. Call 966-5006, available most hours (even at night); if unavailable extra laptop in Adult ED. To request a live ASL interpreter (need 24-48hrs notice) email [email protected] and provide the following information: Patient name, MRN, date, type of language (ASL), how long will request be for, location/address, reason for appointment. Wake Med They have "On Demand" interpreters for MANY languages available on laptops-on-wheels at Wake Med. It is available in the ER, Clinic and inpatient units. Just ask nurse for the interpreter computer if you cannot find one. Click "Sign Language" and have the MRN ready. To schedule a physical Sign Language interpreter you page the interpreting service at Wake Med at 5124 (via SmartWeb paging) or call them at 791-6810. They will ask for information such as the MRN, where to go and how long the interpreter will be needed for. It will likely take 1-2 days to schedule an actual person. This could be used for scheduled family meetings or very in-depth discussions. Moses Cone Hospital: To schedule a Sign Language interpreter call through the Clinical Social Work Department at 336-8320145. For urgent interpreters call their office at 336-275-8878. During business hours use extension #2; for after-hours use extension #1 and the on-call person will be paged. Cone Health Center for Children at Wendover: front office staff are made aware of the need for sign language interpreters when an appointment is made and has a contract with a local company to supply interpreters for clinic visits. ⱡ TABLE 3 American Academy of Pediatrics Joint Committee on Infant Hearing Year 2007 Position Statement: Risk Indicators Associated With Permanent Congenital, Delayed-Onset, and/or Progressive Hearing Loss in Childhood 1 Caregiver concern regarding hearing, speech, language, or developmental delay. 2 Family history of permanent childhood hearing loss. 3 Neonatal intensive care of more than 5 days or any of the following regardless of length of stay: ECMO, assisted ventilation, exposure to ototoxic medications (gentamicin and tobramycin) or loop diuretics (furosemide/Lasix), and hyperbilirubinemia that requires exchange transfusion. 4 In utero infections such as CMV, herpes, rubella, syphilis, and toxoplasmosis. 5 Craniofacial anomalies, including those that involve the pinna, ear canal, ear tags, ear pits, and temporal bone anomalies. 6 Physical findings, such as white forelock, that are associated with a syndrome known to include a sensorineural or permanent conductive hearing loss. 7 Syndromes associated with hearing loss or progressive or late-onset hearing loss, such as neurofibromatosis, osteopetrosis, and Usher syndrome; other frequently identified syndromes include Waardenburg, Alport, Pendred, and Jervell and Lange-Nielson. 8 Neurodegenerative disorders , such as Hunter syndrome, or sensory motor neuropathies, such as Friedreich ataxia and Charcot-Marie-Tooth syndrome. 9 Culture-positive postnatal infections associated with sensorineural hearing loss, including confirmed bacterial and viral (especially herpes viruses and varicella) meningitis that requires hospitalization. 10 Head trauma, especially basal skull/temporal bone fracture. 11 Chemotherapy 12 Recurrent or persistent otitis media for at least 3 months. Reproduced with permission from: American Academy of Pediatrics, Joint Committee on Infant Hearing. Pediatrics. 2007; 120(4):898 –921. www.asl.ms