Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
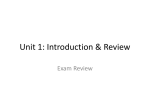
Copyright Eur J Oral Sci 2004 Eur J Oral Sci 2004; 112: 424–428 Printed in UK. All rights reserved European Journal of Oral Sciences Protective effect of salivary nitrate and microbial nitrate reductase activity against caries J. J. Doel1, M. P. Hector2, C. V. Amirtham2, L. A. Al-Anzan2, N. Benjamin3, R. P. Allaker1 1 Oral Microbiology Unit and 2Department of Oral Growth and Development, Barts and The London, Queen Mary's School of Medicine and Dentistry, London, UK; 3Peninsula Medical School, St Luke's Campus, Exeter, UK Doel JJ, Hector MP, Amirtham CV, Al-Anzan LA, Benjamin N, Allaker RP. Protective effect of salivary nitrate and microbial nitrate reductase activity against caries. Eur J Oral Sci 2004; 112: 424–428. Eur J Oral Sci, 2004 To test the hypothesis that a combination of high salivary nitrate and high nitratereducing capacity are protective against dental caries, 209 children attending the Dental Institute, Barts and The London NHS Trust were examined. Salivary nitrate and nitrite levels, counts of Streptococcus mutans and Lactobacillus spp., and caries experience were recorded. Compared with control subjects, a significant reduction in caries experience was found in patients with high salivary nitrate and high nitratereducing ability. Production of nitrite from salivary nitrate by commensal nitratereducing bacteria may limit the growth of cariogenic bacteria as a result of the production of antimicrobial oxides of nitrogen, including nitric oxide. Dental caries is the most common disease found within the oral cavity. Although there has been a steady decrease in the prevalence of coronal caries in many populations in the industrialized world over the last 20–30 yr, Ôhigh-riskÕ groups still exist within such populations. In the UK, these high-risk groups tend now to be limited to deprived inner city populations, ethnic minority groups and recent immigrants. In some developing countries an overall increase in the prevalence of dental caries is observed particularly where large numbers of people move from a predominantly rural to an urban environment and, at the same time, radically change their dietary habits (1). Dental caries is an infective condition and is initiated by an acid attack of tooth enamel, arising largely from the metabolism of sugars by bacteria such as Streptococcus mutans and Lactobacillus spp. (2). Individuals with high levels of these bacteria in saliva, i.e. > 106 colony-forming units (CFU) ml)1 of saliva, are believed to be at high risk for dental caries. S. mutans produces strong acids, such as lactic acid and acetic acid, that can reduce the pH of saliva below the critical value of 5.5 for acid demineralization (3). Although nitrate has historically been associated with deleterious effects in humans, such as infant methaemoglobinaemia (4), recent evidence has suggested a beneficial, antimicrobial role for inorganic nitrate in several systems in humans, including the gastrointestinal tract, oral cavity and skin (5–7). In relation to the oral cavity, inorganic nitrate is present in saliva in high concentrations. Dietary nitrate, present in large quantities in foods such as leafy green vegetables, is absorbed from the small intestine into the bloodstream. Nitrate is then actively concentrated by the salivary glands, so that salivary nitrate concentrations are approximately 10-fold higher R. Allaker, Oral Microbiology Unit, Barts and the London, Queen Mary's School of Medicine and Dentistry, Turner Street, London E1 2AD, UK Telefax: +44–207–2470657 E-mail: [email protected] Key words: dental caries; diet; nitrate; nitric oxide; Streptococcus mutans Accepted for publication June 2004 than those found in plasma (8). This results in a nitrate concentration in saliva of 1500 lm, dependent largely upon dietary nitrate intake. Nitrate concentration varies widely according to the quality and preparation of the food, for example, boiling results in a loss of nitrate from most vegetables. Some typical values of nitrate in foods are shown in Table 1. In mammals, nitrate is considered to be largely an inert material, with no enzymes capable of its reduction. However, in the oral cavity, salivary nitrate will come into contact with bacteria that are capable of rapidly reducing nitrate to nitrite as part of their respiration. Areas of the oral cavity, notably the crypts of the tongue, harbour bacteria in conditions of low oxygen tension (9) that encourage the reduction of nitrate. Such ability of the oral cavity to reduce nitrate is known to vary widely between individuals (10). Nitrate reduction is widespread in nature (11) with highly conserved families of enzymes across genera. The product of nitrate respiration by bacteria is nitrite. Bacteria respiring nitrate rapidly extrude nitrite from their periplasm into the surrounding milieu. Thus, saliva in the oral cavity contains 1500 lm nitrate and 100 lm nitrite, resulting from the bacterial respiration of salivary nitrate. This salivary production of nitrite is reduced following the use of broad-spectrum antibiotics (12) and is absent in germ-free rats (6), thus supporting the role of nitrate-reducing bacteria in its production. Nitrite in the presence of acid will form nitrous acid which, being inherently unstable, dismutates to form a range of nitrogen oxides, most notably nitric oxide (NO). NO, produced in large amounts, is recognized for its antibacterial properties, and is part of the mechanism for Nitrate and caries protection Table 1 Typical values of nitrate in raw and cooked foods (24–27) Nitrate content (mg kg)1) Foodstuff Raw Cooked Apple Asparagus Bacon Banana Beer Beetroot Broccoli Brussel Sprouts Butterhead Lettuce Carrot Celery Corned beef Cos Lettuce French Beans Grapes Ham Orange Parsnip Pear Peas Potato Savoy cabbage Tap water 11 13 101 402 16 1,500 400 12 3,000 170 1,200 19 870 450 46 71 13 81 14 57 154 240 10–20 ND* 0 ND ND ND 1,900 160 8 ND 93 1,000 ND ND 290 ND ND ND 54 ND 17 67 67 ND 425 London, UK. Ethical clearance for the study was obtained from the East London and the City Health Authority (ELCHA). Two saliva samples were taken from each subject using sterile cotton swabs. Microbiological determinations *ND, not determined. killing used by macrophages via the action of the inducible NO synthase enzyme, upregulated by lipopolysaccharide as well as by various proinflammatory cytokines (13). The antimicrobial effects of NO are thought to include modifications of DNA, respiratory complexes, as well as interactions with other reactive species; for example, the highly reactive molecule peroxynitrite is produced upon reaction with superoxide (14). Accordingly, when salivary nitrite comes into contact with the acid environment around the teeth provided by acid-producing bacteria such as S. mutans, a bolus of antimicrobial compounds, including nitric oxide, is formed and results in bacteriostatic and possibly bacteriocidal effects (15). As such, in the presence of large amounts of nitrite in the oral cavity, the growth and possible survival of acidogenic bacteria is limited. Thus, salivary nitrate is a reservoir from which a variety of nitrogen oxides are formed, most notably nitric oxide. After ingesting nitrate-rich food, increases in plasma nitrate, salivary nitrate, salivary nitrite, and oral nitric oxide have been noted (6). To investigate whether salivary nitrate reduction can be preventative against dental caries, we undertook a clinical study with 209 children presenting to the Dental Institute, Barts and The London NHS Trust, London, UK. One swab was placed in a glass vessel containing 20 glass beads and 1 ml of reduced transport fluid (16) and vortexed for 30 s to disaggregate bacteria from the swab. Of the resulting solution, 40 ll was then transferred to selective agar using a spiral plater (Don Whitley Instruments, Shipley, UK). Rogosa agar (Oxoid, Basingstoke, UK), selective for Lactobacillus spp., and TYCSB agar (TYC agar, Oxoid, supplemented with 150 g l)1 sucrose and 200 U l)1 bacitracin), selective for S. mutans, were used. Agar plates were incubated in air with 10% CO2 (v/v) at 37C for 72 h. Identification of S. mutans was confirmed on the basis of characteristic colony morphology and standard biochemical tests. Nitrite and nitrate measurements The head was cut off the second swab and placed in a microcentrifuge tube containing 10 glass beads. The tube was then spun at 13,250 g for 5 min, the beads discarded and the saliva sample recovered. Measurement of nitrite. Nitrite concentrations were determined in 96-well plates, in duplicate, using a 50-ll saliva sample volume. To each sample, 50 ll of sulfanilamide solution (1% w/v sulfanilamide in 5% v/v phosphoric acid) was added and incubated for 5 min at room temperature, protected from light. NED solution (0.1% w/v N-1-naphthylethylenediamine dihydrochloride in distilled water; 50 ll) was then added and incubated for 5 min at room temperature, protected from light. The development of a characteristic purple colour was then measured in a plate reader at 540 nm. Values of nitrite were estimated by comparison with a standard curve of nitrite concentrations. Measurement of nitrate. Nitrate concentrations were determined in the following manner. A 50-ll sample of saliva was added to 950 ll of 0.5 m ammonia buffer, pH 9.0, containing 1 g l)1 EDTA. The solution was then exposed to a copperized cadmium column (Nitralyzer; WPI Instruments, Stevenage, UK) for 5 min. This converts all the nitrate in the solution to nitrite. Nitrite in the solution was then measured as described above; starting concentrations of nitrate were calculated by subtracting the values obtained pre- and postreduction using the copperized cadmium column. Caries assessment Caries experience of subjects was determined as the sum of the number of teeth that were diseased as a result of active caries, missing as a result of having been carious and filled owing to carious lesions. Material and methods Dietary nitrate estimation Subjects A dietary questionnaire was used to establish the approximate daily dietary nitrate intake (mg kg)1 body weight) of an individual. This was based upon the National Diet and Nutrition Survey (17). The dietary interview included Consent was sought from patients attending the Dental Institute, Barts and The London Health NHS Trust, 426 Doel et al. questions on the type of vegetables eaten (cooked or raw), frequency of intake and a detailed description of food and fluid intake over the previous 24-h period. Statistics Student’s independent t-tests were employed to analyse data. Results A total of 209 subjects (106 male and 103 female) were recruited to the study from the London Borough of Tower Hamlets, a deprived area with a population of low socio-economic status. Summaries of the values for salivary nitrite and nitrate levels, S. mutans and Lactobacillus spp. counts (CFU) in saliva, caries experience and age are shown in Table 2. To assess the ability of an individual’s oral flora to reduce salivary nitrate to nitrite, the ratio of nitrite in the saliva as a percentage of starting nitrate is given (because nitrate is converted to nitrite) as a nitrate reductase (NR) ratio as follows: Caucasian (33%); 4 Afro-Caribbean (10%); 3 mixed race (8%); and 2 Asian (5%). The control group consisted of 170 subjects; 88 males (52%) and 82 females (48%). Within this group the ethnicity mix comprised: 72 Indian subcontinent (42%); 67 white Caucasian (39%); 21 AfroCaribbean (12%); 4 mixed race (3%), 3 Asian (2%); and 3 Middle-Eastern (2%). In terms of caries experience, a significant decrease (P < 0.05) was observed in subjects in the high salivary nitrate/nitrate reductase group when compared with control subjects. The former group also revealed a lower mean value for counts of S. mutans levels when compared to control subjects. However, this difference was not statistically significant. A dietary survey was also undertaken to identify whether the intake of nitrate within the sample population was within the expected variation. Of 135 subjects surveyed, the average intake was 3.6 mg kg)1 d)1 (range: 0.2–17.3; median 2.7). The mean value accords closely with the current acceptable daily intake (ADI) of 3.7 mg kg)1 d)1, as published by the World Health Organization (18). The full range of nitrate intake values are shown in Fig. 1. It is of note that 92 (68%) fall below the ADI, with 43 (32%) consuming more than the ADI. 100 ½nitrite=ðnitrite þ nitrateÞ: In order to identify those patients who had both a high concentration of salivary nitrate and a high nitratereducing capacity, the data were further subdivided into two groups. Those patients with levels of salivary nitrate and a nitrite/nitrate ratio above the 50th percentile (986.3 lm and 6.4%, respectively) were considered to have a high nitrate level in saliva and posses a high nitrate-reducing capacity. The two groups are shown in Table 3. This high nitrate-reducing/high salivary nitrate group consisted of 39 subjects: 18 males (46%) and 21 females (54%). Within this group the ethnicity mix comprised: 17 Indian subcontinent (44%); 13 white Table 2 Salivary nitrite and nitrate levels, nitrate reductase (NR) ratio, Streptococcus mutans and Lactobacillus spp. counts, caries experience and age profile of all 209 subjects recruited Variable Salivary nitrite (lm) Salivary nitrate (lm) NR* ratio (%) Streptococcus mutans (CFU ml)1 of saliva) Lactobacillus spp. (CFU ml)1 of saliva) Caries experience Age (yr) Mean 91.0 ± 6.3 (range 0.0–700.9; median 70.2) 1,370.2 ± 93.0 (range 0.0–8,351.2; median 986.3) 9.3 ± 0.8 (range 0.0–100.0; median 6.3) 6.3 · 105 ± 1.5 · 105 (range 0.0–2.5 · 108; median 1.3 · 104) 3.3 · 103 ± 9.4 · 102 (range 0.0–1.4 · 105; median 0.0) 5.0 ± 0.3 (range 0.0–26.0; median 5.0) 7.2 ± 0.3 (range 0.08–16.0; median 7.0) *The NR ratio represents an individual’s capacity to reduce salivary nitrate. Results are expressed as mean ± standard error (range; median). CFU, colony-forming units. Discussion Humans have evolved mechanisms to concentrate nitrate in the oral cavity. As no mammalian enzymes exist to act upon nitrate, this nitrate recycling appears to have no clear function within the human body. However, considering the complex microflora that resides within the specialized niches of the oral cavity, possible reasons for this enteric nitrate recycling become apparent. The oral flora consists of at least 500 different species identified to date (19). Many of these bacteria, such as Veillonella atypica are anaerobes and have an absolute requirement for nitrate as an electron acceptor. Other bacteria, such as Actinomyces odontolyticus, are facultative anaerobes and will respire under conditions of low oxygen tension. Under anaerobic conditions, as found in the deep clefts of the tongue, such bacteria will reduce nitrate, resulting in the production of large quantities of nitrite, which is rapidly extruded from the bacteria. The concentration of nitrate in the oral cavity may thus encourage the survival of bacteria under conditions of low oxygen tension and, in turn, enhance oral immunity via the production of antimicrobial oxides of nitrogen. Accordingly, individuals with a high nitrate intake and an oral flora with the ability to reduce large amounts of nitrate to nitrite in the oral cavity may be protected against cariogenic acidogenic bacteria and, thus, dental caries. Considering acidogenic bacteria, typified by cariogenic S. mutans, the production of acid in the presence of nitrite will result in bacteriostatic and possibly bacteriocidal effects. It is suggested that the antimicrobial nature of acidified nitrite is selective in that only those bacteria in the immediate vicinity will be affected. To test the hypothesis that nitrate recycling and a high nitrate-reductase activity in the oral cavity could be Nitrate and caries protection 427 Table 3 Comparison of salivary nitrite and nitrate levels, nitrate reductase (NR) ratio, Streptococcus mutans and Lactobacillus spp. counts, caries experience and age profile for high nitrate reducers compared with other subjects Salivary nitrite (lm) Salivary nitrate (lm) NR* ratio (%) Streptococcus mutans (CFU ml)1 of saliva) Lactobacillus spp. (CFU ml)1 saliva) Caries experience Age (yr) High nitrate reducers Others 177.8 ± 20.7 (range 74.4–700.9; median 132.5) 1,486.6 ± 98.7 (range 986.3–3,655.5; median 1,294.1) 10.3 ± 0.7 (range 6.5–28.1; median 8.9) 5.2 · 105 ± 2.4 · 105 (range 0.0–9.2 · 106; median 2.3 · 104) 3.6 · 103 ± 1.8 · 103 (range 0.0–6.4 · 104; median 0.0) 4.0 ± 0.7 (range 0.0–14.0; median 3.0) 6.6 ± 0.5 (range 1.0–15.0; median 6.0) 71.1 ± 5.1 (range 0.0–327.4; median 56.2) 1,343.5 ± 112.1 (range 0.0–8,351.2; median 851.6) 9.1 ± 1.0 (range 0.0–100.0; median 4.8) 6.5 · 105 ± 1.8 · 105 (range 0.0–2.5 · 107; median 1.0 · 104) 3.2 · 103 ± 1.1 · 103 (range 0.0–1.4 · 105; median 0.0) 5.3 ± 0.3 (range 0.0–26.0; median 5.0) 7.3 ± 0.3 (range 0.08–16.0; median 7.0) *The NR ratio represents an individual’s capacity to reduce salivary nitrate. ÔHigh nitrate reducersÕ comprise those subjects whose salivary nitrate and NR ratio are above the 50th percentile. Results are expressed as mean ± standard error (range; median). CFU, colony-forming units. Nitrate intake (mg–1 kg–1 day–1) protective against dental caries, we examined the levels of salivary nitrate and nitrite, S. mutans and Lactobacillus spp. counts in saliva, and caries experience in children presenting to the Dental Institute at Barts and The London NHS Trust. We found that those children with high salivary nitrate levels and a high percentage reduction of nitrate to nitrite had significantly less caries experience, providing support to the suggestion that nitrate recycling may be an important part of the innate immune response in the oral cavity. To lend further support, the mean nitrite salivary level of 0.2 mm found in this group reaches the concentration (‡ 0.2 mm) known to kill S. mutans in vitro under acidified conditions (15). Further circumstantial evidence that nitrate reduction could be important as a defence mechanism against 16 12 8 4 0 1 31 61 91 Sample number 121 Fig. 1. Distribution of estimated dietary nitrate intake for 135 subjects (mg kg)1 d)1). The unbroken line represents the acceptable daily intake (World Health Organization guidelines) for nitrate intake (3.7 mg kg)1 d)1). dental caries has been demonstrated (20,21). Such studies found that the incidence of dental caries was much reduced in areas with a high molybdenum content in soil. It is interesting to note in light of this fact that the nitrate reductase enzyme requires molybdenum as a cofactor for activity. Thus, consumption of a higher amount of molybdenum in drinking water and vegetables could lead to a higher level of nitrate reductase activity in such individuals. To conclude, we have found that patients with a high concentration of nitrate in saliva and an oral flora with a high capacity to reduce nitrate to nitrite, have significantly less caries history than those with low amounts of nitrate in saliva and an oral flora with a low capacity to reduce nitrate to nitrite. Dental caries is a particular problem in children, and this is partly explained by a number of salivary factors. Salivary nitrate concentrations are greatly influenced by the amount of nitrate in the diet, which, in industrialized countries, is mainly influenced by the intake of green vegetables (22). In general, many children have a dislike of green vegetables (17), and we hypothesize that increasing nitrate intake in this group may be especially important in establishing nitrate-reducing bacteria in the oral cavity, similar to the effects that are seen in the gut (23). Once established, the nitrate-reducing bacteria may suppress the growth of acid-forming bacteria and thereby protect teeth against caries. The major anaerobic nitrate-reducing bacteria on the human tongue probably include V. dispar and V. atypica. These are thought to be true commensals in the oral cavity as a result of their ability to metabolize lactic acid, the major causative agent of dental caries, into weaker acids. The residency of strictly anaerobic bacteria on the tongue is possibly aided by the presence of secretory glands (von Ebner’s glands) at the base of the circumvallate papillae. These glands release bicarbonate, which could protect and nourish the anaerobic bacteria deep within the clefts. This may be part of a symbiotic adaptation between host and bacteria, adding 428 Doel et al. support to the hypothesis that certain commensal bacteria are encouraged to reside in the oral cavity to enhance mucosal immunity. Therefore, probiotic therapy at an early age to encourage colonization of the oral cavity with micro-organisms such as V. atypica, which contain the nitrate reductase enzyme, may be a potential therapy against dental caries. Acknowledgements – This work was funded by the Royal London Hospital Special Trustees (RAC 399). References 1. Johnson NW. Risk Markers for Oral Diseases, Vol. 1. Dental Caries. Cambridge: Cambridge University Press, 1991. 2. Allaker RP, Hardie JM. Oral infections. In: Collier L, Balows A, Sussman M, eds. Topley and Wilson’s Microbiology and Microbial Infections, 9th edn. London: Arnold, 1998; 373– 390. 3. Anderson P, Hector MP, Rampersad MA. Critical pH in resting and stimulated whole saliva in groups of children and adults. Int J Paediatr Dent 2001; 11: 266–273. 4. Knobeloch L, Salna B, Hogan A, Postle J, Anderson H. Blue babies and nitrate-contaminated well water. Environ Health Perspect 2000; 108: 675–678. 5. Benjamin N, O’Driscoll F, Dougall H, Duncan C, Smith L, Golden M, McKenzie H. Stomach NO synthesis. Nature 1994; 368: 502. 6. Duncan C, Dougall H, Johnston P, Green S, Brogan R, Leifert C, Smith L, Golden M, Benjamin N. Chemical generation of nitric oxide in the mouth from the enterosalivary circulation of dietary nitrate. Nat Med 1995; 1: 546–551. 7. Weller R, Price RJ, Ormerod AD, Benjamin N, Leifert C. Antimicrobial effect of acidified nitrite on dermatophyte fungi, Candida and bacterial skin pathogens. J Appl Microbiol 2001; 90: 648–652. 8. Knight TM, Forman D, Al-Dabbagh SA, Doll R. Estimation of dietary intake of nitrate and nitrite in Great Britain. Food Chem Toxicol 1987; 25: 277–285. 9. Li H, Duncan C, Townend J, Killham K, Smith LM, Johnston P, Dykhuizen R, Kelly D, Golden M, Benjamin N, Leifert C. Nitrate-reducing bacteria on rat tongues. Appl Environ Microbiol 1997; 63: 924–930. 10. Xu J, Xu X, Verstraete W. Quantitative measurement of the nitrate reductase activity in the human oral cavity. Food Chem Toxicol 2001; 39: 393–400. 11. Richardson DJ. Bacterial respiration: a flexible process for a changing environment. Microbiology 2000; 146: 551–571. 12. Dougall HT, Smith L, Duncan C, Benjamin N. The effect of amoxycillin on salivary nitrite concentrations: an important mechanism of adverse reactions? Br J Clin Pharmacol 1995; 39: 460–462. 13. MacMicking J, Xie QW, Nathan C. Nitric oxide and macrophage function. Annu Rev Immunol 1997; 15: 323–350. 14. Fang FC. Mechanisms of nitric oxide-related antimicrobial activity. J Clin Invest 2003; 99: 2818–2825. 15. Silva Mendez LS, Allaker RP, Hardie JM, Benjamin N. Antimicrobial effect of acidified nitrite on cariogenic bacteria. Oral Microbiol Immunol 1999; 14: 391–392. 16. Allaker RP, Langlois T, Hardie JM. Prevalence of Eikenella corrodens and Actinobacillus actinomycetemcomitans in the dental plaque of dogs. Vet Rec 1994; 134: 519–520. 17. Gregory JR, Collins DL, Davies PSW, Hughes JM, Clarke PC. National Diet and Nutrition Survey. London: HMSO, 1995. 18. World Health Organization. Toxicological Evaluation of Certain Food Additives with a Review of General Principles and of Specifications. Seventeenth Report of the Joint FAO/WHO, Expert Committee on Food Additives. Geneva: World Health Organization, 1973. 19. Paster BJ, Boches SK, Galvin JL, Ericson RE, Lau CN, Levanos VA, Sahasrabudhe A, Dewhirst FE. Bacterial diversity in human subgingival plaque. J Bacteriol 2001; 183: 3770–3783. 20. Ludwig TG, Healy WB, Losee FL. An association between dental caries and certain soil conditions in New Zealand. Nature 1960; 186: 695–696. 21. Jenkins GN. Molybdenum and dental caries. 3. In vitro experiments on modes of action and possible practical applications. Br Dent J 1967; 122: 545–550. 22. Howe GR, Harrison L, Jain M. A short diet history for assessing dietary exposure to N-nitrosamines in epidemiologic studies. Am J Epidemiol 1986; 124: 595–602. 23. Turek B, Hlavsova D, Tucek J, Waldman J, Cerna J. The fate of nitrates and nitrites in the organism. IARC Sci Publ 1980; 31: 625–632. 24. Meah MN, Harrison N, Davies A. Nitrate and nitrite in foods and the diet. Food Addit Contam 1994; 11: 519–532. 25. Maff UK: 1994 Total Diet Study – Nitrate and Nitrite, Vol. 137. London: Joint Food Safety and Standards Group, 1997. 26. Maff UK: Survey of Nitrate and Nitrite in Bacon and Cured Meat Products, Vol. 142. London: Joint Food Safety and Standards Group, 1998. 27. Maff UK: Nitrate in Vegetables, Vol. 158. London: Joint Food Safety and Standards Group, 1998.