Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
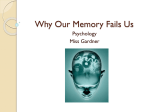
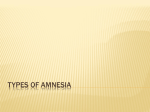
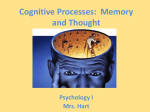
Memory and Anterograde Amnesia Francesca Philips Maths 89S Duke University 6st December 2016 1 Memory and Anterograde Amnesia Patient HM Perhaps the most notable case study in neuroscience is that of ‘Patient H.M.’. Henry Gustav Molaison had suffered from epilepsy from the age of ten onwards, and his condition only continued to worsen with time (Adams, 2013). At the age of 27, he was having up to 11 seizures a week. After determining that the seizures were beginning in his temporal lobes, a neurosurgeon named William Scoville decided to perform what was later seen as essentially experimental surgery in order to control the epilepsy (Pearce, 2006). Scoville performed a bilateral medial temporal lobe resection, Figure 1: Henry Molaison (1986) meaning that he removed most of the temporal lobe on both sides. This can be seen in Figure 2, where HM’s brain can be compared to a normal brain, and the missing hippocampi and surrounding tissue is clear (Pearce, 2006). After the surgery, the seizures were milder and could be controlled by medication. In fact, he suffered no tonic-clonic or ‘grand-mal’ seizures for a year after the surgery. However, Figure 2: Patient HM’s brain vs normal brain 2 the surgery had an unanticipated effect; Henry Molaison could no longer retain any new information for more than a brief time. His old memories remained relatively intact, but this side effect meant that he could not form any new memories. Molaison’s case is one of the most ‘pure’ cases of anterograde amnesia ever recorded, and allowed for new discoveries in neuroscience that have completely revolutionised the way that we discuss and understand memory. Anterograde Amnesia Amnesia is a “severe impairment of memory”, and varies in form, cause, and scope. Anterograde amnesia, which Henry Molaison suffered from, is the inability to form new memories following an event (Watson and Breedlove, 2012). Often, a patient’s can still make very short term memories, but will struggle to recall that information moments later. Previously formed memories usually remain relatively unaffected. For example, Henry was able to remember much of what happened pre-1953, but could not form new memories or recall details about his life post-surgery. For such patients, new information is processed normally, however it is quickly forgotten and not consolidated in long term memories. Mammillary bodies are located on the brain’s underside, and are a pair of small structures. Normally, when a memory is being formed, the neurons (nerve cells) in the mammillary electrical bodies impulses relay to the thalamus, which is a small Figure 3: Anatomy of the brain 3 structure in the centre of the brain (Milner, 2005). Neurons within the thalamus then send signals to the brain’s cortex (the outer layer of neural tissue), and it is in the cortex where long term memories are thought to be ‘stored’. Memories are thought to be passed from a sort of sensory memory, to short term memory, and then committed to long term memory. However, many of our memories seem to never be formed as long-term memories; if we remembered every single aspect of our experiences, just an hour would hold an overwhelming amount of information. It is thought that the depth of processing of the information, motivation, attention all play roles in determining what information is formed into long-term memories. Therefore, anterograde amnesia can be caused by damage to the hypothalamus, thalamus, and the surrounding cortical structures. If such damage occurs, memory storage can be inhibited, as the connections between the key systems utilised in the memory circuit are affected. Anterograde amnesia can also occur as a result of drug abuse, traumatic brain injuries or surgery, or an event such as a heart attack, epileptic attack or oxygen deprivation (Ryback, 1970). One cause of anterograde amnesia that is not often recognised as such is alcohol intoxication; often times this form of amnesia is referred to as a ‘blackout’. The rapid rise in blood alcohol concentration over a short period of time can impair or block the brain’s ability to form long-term memories about events that happen while intoxicated. When alcohol is rapidly consumed, it is at 0.20% BAC that anterograde amnesia usually occurs, although it can occur at blood alcohol concentrations as low as 0.14% (Ryback, 1970). The amount of alcohol consumed correlates positively with the magnitude of the memory loss. However, this form of anterograde amnesia is temporary, and upon reaching sobriety, the ability to create long-term memories returns. It is also important to note that short-term memory 4 function is often unhindered, and so those affected can still remember what happened moments before and can function enough to have conversations or participate in social activities relatively normally. In one of his studies, Ryback writes that the intoxicated subjects could “carry on conversations during the amnesic state, but could not remember what they said or did 5 minutes earlier. Their immediate and remote memory were intact” (Ryback, 1970). Alcohol, if consumed rapidly and in large quantities, can disrupt activity in the hippocampus (a region which is centrally involved in the formation of new autobiographical memories) (White, 2004). This theory is based on observations that such alcohol consumption creates a similar amnesiac effect to that produced by damage to the hippocampus. Both impact the brain’s ability to store long-term explicit memories, while leaving short-term memory storage and previously formed long-term memory relatively intact (Milner, 2005). The alcohol has selective effects on neurotransmitter systems which allow for communication between nerve cells. It has been shown that alcohol affects the activity of proteins that bind neurotransmitters, meaning that connections cannot be made between core sections of the memory circuit. It is often only ‘explicit memory’ which is affected by anterograde amnesia. There are two types of long-term memories: explicit memories and implicit memories. Explicit memories are those that we consciously recall and use to explain; they are the kinds of memories we utilise in answering ‘what’ questions (Watson and Breedlove, 2012). Implicit, or procedural memory, is typically not as affected. These types of memories are shown by performance, and do not require conscious recollection. For example, remembering how to ride a bike is an 5 example of an implicit memory, while remembering who the 34th president of the United States is would be an explicit memory (Watson and Breedlove, 2012). Figure 4: Mirror tracing task But why is it that explicit memory is affected, while implicit is not? In the case of HM, a select few tests show this difference in impact. One of these tests was a mirror tracing test. As seen in Figure 4, Henry had to trace a picture of a star, but he could only see this star in a mirror. Henry could never recognise that he had previously performed the task, but his errors per day gradually decreased and demonstrated a long-term implicit memory. Implicit memory does not rely on the hippocampus and surrounding tissues in the same way that explicit memory does, and so often times the memory circuit for implicit memory is left relatively intact. While still in the process of determining exactly what this circuit is, neuroscientists theorise that there is a different memory system being utilised. This is what allowed Henry to learn the new skill of mirror drawing, even though he had forgotten ever having performing the task before. The last time that he performed the test, Henry declared, “Well, this is strange. I thought that that would be difficult. But it seems as though I’ve done it quite well.” (Watson and Breedlove, 2012) 6 Treating Anterograde Amnesia The approaches that are used when treating anterograde amnesia primarily treat the symptoms of the condition rather than the cause itself. Techniques such as diaries and extensive note taking are suggested as ways to cope with the condition, but do not offer long-term solutions. There is no cure for anterograde amnesia, and this is mainly due to the current lack of deep understanding about the way that the mind works and the way that memories are stored. Of course, anterograde amnesia exists on a spectrum, with some patients able to remember some select memories made after an event and have improvements in their long-term memory, while others like Henry Molaison remember nothing. The brain’s ‘neuroplasticity’ offers some explanation for why some patients’ conditions can improve over time. Neuroplasticity refers to the brain’s ability to ‘re-map’ neural pathways and adapt to new situations. It is this characteristic that allows the brain an opportunity to achieve nearly normal memory function after damage to key areas of the memory circuit. However, if the damage is too extensive, this ability is still not sufficient to allow the return of normal memory function (Watson and Breedlove, 2012). Conclusion From our understanding of memory and amnesia, a distinction can be made between learning and memory. Learning is the process of acquiring new information, while memory is the ability to store and retrieve that information. Further research and studies about memory and amnesia may hold clues to ways in which we can better remember, and comprehend the world around us. However, neuroscientists’ current knowledge of human memory remains limited and the knowledge is not sufficient to allow us to ‘map’ the human brain and determine which parts are responsible for different functions. This information may allow us to treat anterograde amnesia and other forms of brain damage more easily. 7 Bibliography Adams, T. (2013, May 4). Henry Molaison. Retrieved December 1, 2016, from The Guardian: https://www.theguardian.com/science/2013/may/05/henry-molaisonamnesiac-corkin-book-feature Milner, B. (2005). The Medial Temporal-Lobe Amnesic Syndrome. Psychiatric Clinics of North America. Pearce, J. M. (2006). Amnesia. European Neurology. Ryback, R. S. (1970). Alcohol amnesia. Observations in seven drinking inpatient alcoholics. Q J Stud Alcohol. Teuber, H. L., Milner, B., & Vaughn, H. G. (1968). Persistent Anterograde Amnesia After Stab Wound of Basal Brain. Neuropsychologia, 6, 267-282. Watson, N. V., & Breedlove, S. M. (2012). The Mind's Machine. Simon and Schuster. White, A. M. (2004, July). What Happened? Alcohol, Memory Blackouts, and the Brain. Retrieved December 2, 2016, from National Institute on Alcohol Abuse and Alcoholism: http://pubs.niaaa.nih.gov/publications/arh27-2/186-196.htm 8