Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
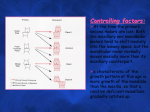
In the name of GOD Periodontal and bone response to normal function Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 8 William R. Proffit, Henry W. Fields, David M.Sarver. 2013. Mosby The principle of orthodontic treatment: if prolonged pressure is applied to a tooth, tooth movement will occur as the bone around the tooth remodels. The tooth moves through the bone carrying its attachment apparatus with it, as the socket of the tooth migrates. Tooth movement is primarily a periodontal ligament phenomenon. The biologic response to the orthodontic therapy includes not only the response of the periodontal ligament but also the response of growing areas distance from the dentition. Pattern of bone apposition and resorption in: sutures of the maxilla bony surfaces of temporomandibular joint Periodontal ligament Normal structure and function Periodontal ligament (PDL) heavy collagenous supporting structure that attached to a tooth and separate it from the adjacent alveolar bone. Approximately 0.5 mm in width around all parts of the root. The major component is a network of parallel collagenous fibers The supporting fibers run in at an angle: attaching farther apically on the tooth (cementum) than on the adjacent alveolar bone (lamina dura) This arrangement resists the displacement of the tooth expected during normal function PDL components: • Collagenous fiber bundles most of the PDL space • Cellular elements mesenchymal cells • Vascular and Neural elements • Tissue fluids All play an important role in normal function and orthodontic tooth movement. The principal cellular elements are undifferentiated mesenchymal cells and their progeny in the forms of fibroblasts and osteoblasts the collagen of the ligament is constantly being remodeled and renewed the stem cells can serve as both fibroblasts and fibroclasts fibroblasts, producing new collagenous matrix materials. fibroclasts, destroying previously produced collagen. remodeling and recontouring of the bony socket and the cementum of the root is constantly carried out, as a response to normal function. fibroblasts in the PDL have properties similar to osteoblasts. new bone probably is formed by osteoblasts that differentiated from the local cellular population. bone and cementum are removed by specialized osteoclasts and cementoclast the origin of these multinucleated giant cells s controversial: most are of hematogenous origin some may be derived from local area stem cells although PDL is not highly vascular, it contains blood vessels and cells from the vascular system nerve endings within the PDL: unmyelinated free ending (pain) more complex receptors (pressure and proprioception) PDL space is full of fluid derived from vascular system the fluid allows the PDL space to play the role of “shock absorber” Response to normal function During masticatory function the teeth and periodontal structures are subjected to intermittent heavy forces: Tooth contacts last for 1 second or less Forces are quite heavy: 1-2 kg to 50 kg Quick displacement of the tooth within the PDL space is prevented by the incompressible tissue fluid The force is transmitted to the alveolar bone, which bends in response bone bending during normal function of the jaws (and other skeletal elements) is often not appreciated. the body of the mandible bends as the mouth is opened and closed upon wide opening, the distance between the mandibular molars decreased by 2 to 3 mm. In heavy function: • individual teeth are slightly displaced as the alveolar bone bends to allow this to occur. • bending stresses are transmitted over considerable distances Bone bending in response to normal function generates piezo-electric currents. An important stimulus to skeletal regeneration and repair First second of pressure very little of the PDL space fluid is squeezed out normal mastication: 1 second or less force application Maintained pressure the fluid s rapidly expressed the tooth displaced within the PDL space compressing the ligament against adjacent bone Pain is normally felt after 3 to 5 seconds of heavy force application PDL Is beautifully adapted to resist forces of short duration It rapidly loses its adaptive capability as the tissue fluid is squeezed out Prolonged force, even of low magnitude, produces a different physiologic response – remodeling of the adjacent bone Orthodontic tooth movement is made possible by the application of prolonged forces. Light prolonged forces in the natural environment- forces from the lips, cheeks, or tongue resting against the teeth- have the same potential as orthodontic forces to cause teeth movement. Physiologic response to heavy pressure against a tooth Time (seconds) Event PDL fluid incompressible <1 Alveolar bone bends Piezoelectric signal generated 1-2 PDL fluid expressed Tooth moves within PDL space PDL fluid squeezed out 3-5 Tissues compressed Immediate pain if pressure is heavy Role of PDL in eruption and stabilization of the teeth Tooth eruption makes it plain that forces generated within the PDL itself can produce tooth movement. The eruption mechanism depends on metabolic events in the PDL, including but perhaps not limited to: formation cross linkage maturational shortening of collagen fibers This process continues, although at a reduced rate, into adult life. Active stabilization of the teeth against prolonged forces of light magnitude light prolonged pressure against the teeth are not in perfect balance In the mandibular anterior , tongue pressure is greater than lip pressure. In the maxillary incisor region, lip pressure is greater The ability of the PDL to generate a force and thereby contribute to the set of forces that determine the equilibrium situation, probably explained this. Active stabilization also implies a threshold for orthodontic force Forces below the stabilization level ineffective The threshold for outside force would vary depending on the extent to which existing soft tissue pressures were already being resisted by the stabilization mechanism. Active stabilization can overcome prolonged forces of a few grams at most, perhaps up to the 5 to 10 gm/cm2 Thanks for your attention