Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
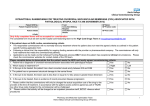
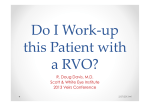
Interactive Grand Rounds Blair Lonsberry, MS, OD, MEd., FAAO Diplomate, American Board of Optometry Clinic Director and Professor Pacific University College of Optometry [email protected] Disclosures and Special Request Paid consultant for: • Alcon Pharmaceuticals, Bausch and Lomb, Carl Zeiss Meditec, NiCox, Sucampo Special Request: Interactive remotes don’t work on your TV, so please don’t take them home! Commitment to change: - write down three things that you “learned” from this presentation that you can incorporate into your practice to improve patient care CASE 1 Case History • 38 black male, complaining that the vision in his right eye is blurry. – Got the current Rx 3 weeks previously, and started out good but in last couple of days OD vision has become blurry • Medical Hx: no current health concerns and no medications Entrance Skills Va’s: OD: 6/7.5 (20/25), OS: 6/6 (20/20) Pupils: PERRL CVF: full to finger count EOM’s: FROM Amsler: central metamorphopsia OD HVF: 10-2 (see VF) Which of the following OCT’s goes with this patient? 1 2 3 4 CASE 2 Case • 55 yr white female complains of fluctuating vision – Worse at near – Spends 8-10 hours/day on the computer • Medical Hx: – Hypertension for 10 years – Joint pain • Medications: – HCTZ for HTN – Celebrex for her joint pain Exam Data • VA (corrected): – 6/7.5 (20/25) OD, OS • • • • PERRL EOM’s: FROM CVF: FTFC SLE: – TBUT 5 sec OD, OS – Positive NaFl staining and Lissamine green staining of conj and cornea – Decreased tear prism Additional Testing/Questions • Schirmer: < 5 mm of wetting in 5 minutes OD, OS • RF and ANA: normal for patients age • SS-A: 2.0 (normal < 1.0), SS-B: 1.9 (normal <1.0) • Additional symptoms reported: – Patient experiences dry mouth and taking Salagen • Diagnosis: Sjogren’s Syndrome Differential Diagnosis of Dry Eye Signs and Symptoms of Dry Eye Signs: – Ocular Surface Damage • • Corneal Staining (Fluorescein and/or Rose Bengal) Conjunctival Staining (Lissamine Green ) – Decreased Tear Quantity • • • Schirmer Score Phenol Red Thread Test Tear Meniscus Height – Decreased Tear Quality • • Tear Break Up Time (TBUT) Tear Osmolarity Symptoms: – – – – – – Grittiness Burning Irritation Stringy discharge Blurring of vision Ocular Surface Disease Index (OSDI) Treatment • We initiated: – Omega-3 supplements (3-4 grams per day) – Recommended warm compresses and lid washes qhs – Testosterone cream 3% applied to upper lid bid • Patient had significant improvement in symptoms with the use of the topical testosterone cream. – However, she was still symptomatic at the end of the day and she still had significant staining on her cornea and conjunctiva – Initiated FML tid for 1 month, restasis bid after 2 weeks • 2 months later patient reported further improvement in her symptoms • No conjunctival staining was noted and only slight SPK • Schirmer values improved to OD: 9 mm, OS: 10 mm Transdermal Testosterone Cream • Recent studies suggest that androgen deficiency may be the main cause of the meibomian gland dysfunction, tear-film instability and evaporative dry eye seen in Sjogren patients • Transdermal testosterone promotes increased tear production and meibomian gland secretion, thereby reducing dry eye symptoms (Dr. Charles Connor). • arGentis and Allergan have conducted trials to see if topical androgens are effective in treating dry eye SJOGREN’S SYNDROME: OLD/NEW CLASSIFICATION • Old: – 1o Sjogrens: occurs when sicca complex manifests by itself • no systemic disease present – 2o Sjogrens: occurs in association with collagen vascular disease such as • RA and SLE • significant ocular/systemic manifestations • New: – The diagnosis of SS should be given to all who fulfill the new criteria while also diagnosing any concurrent organ-specific or multiorgan autoimmune diseases, without distinguishing as primary or secondary. Diagnosis: New Criteria • • Sjogren’s International Collaborative Clinical Alliance (SICCA) was funded by the National Institutes of Health to develop new classification criteria for SS New diagnostic criteria requires at least 2 of the following 3: – 1) positive serum anti-SSA and/or anti-SSB or (positive rheumatoid factor and antinuclear antibody titer >1:320), – 2) ocular staining score >3, or – 3) presence of focal lymphocytic sialadenitis with a focus score >1 focus/4 mm2 in labial salivary gland biopsy samples Ocular Surface Score (OSS) • The ocular surface score (OSS) is the sum of: – 0-6 score for fluorescein staining of the cornea and – 0-3 score for lissamine green staining of both the nasal and temporal bulbar conjunctiva, – yielding a total score ranging from 0-12. Antibodies to SS-A and SS-B • Sjogren’s syndrome A and B • Typically tested by ELISA and immunoblot • Associated Conditions: – Uncommon in the normal population and in patients with rheumatic diseases other than Sjogren’s syndrome and SLE – Present in 75% of patients with “primart” Sjogren’s but only 10-15% of patients with RA and secondary Sjogren’s syndrome Antibodies to SS-A and SS-B • Indications: – Should be measured in patients with a clinical suspicion of Sjogren’s or SLE • Interpretation: – Presence of AB’s is a strong argument for the diagnosis of Sjogren’s Syndrome in a patient with sicca syndrome Dry Eye and Lid Disease? • It is estimated that 67-75% of patients who have dry eye have some form of lid disease – it is often the most overlooked cause for dry eye symptoms • Important to address the lids in any treatment plans for patients with dry eye QUICKIE CHRPE vs Nevus 25 Nevi Trivia • 31% of choroidal nevi show slight enlargement over time without the transformation to a melanoma (Ophthalmology 2011) • The prevalence of choroidal nevi in the white U.S. population ranges from 4.6% to 7.9% – If it is assumed that all choroidal melanomas arise from preexisting nevi, then the published data suggest a low rate (1/8845) of malignant transformation of a choroidal nevus in the U.S. white population. (Ophthalmology 2005) • Choroidal melanoma risk for metastasis, ranging from 16% to 53% (at 5 years of follow-up) depending on the size of the tumor at the time of diagnosis. (Arch Ophthalmol 1992) Nevi Trivia • Studies suggest that the presence of orange pigment is significantly correlated with the risk of subsequent growth – when orange pigment is difficult to clinically discern (especially with the natural coloration of the fundus and in amelanotic nevi), FAF offers the best currently available method to enhance its visibility. (Optometry 2009) • Aggressive surveillance for survivors of ocular melanoma appears to carry a relatively high risk of secondary cancers from the radiation exposure, particularly for young women. (JAMA Ophthalmology 2013). TFSOM—“To Find Small Ocular Melanoma” Thickness: lesions >2mm Fluid: any subretinal fluid (suggestive of serous retinal detachment) Symptoms: photopsia, vision loss Orange pigment overlying the lesion Margin touching optic nerve head • None of these factors = 3% risk of a nevus converting to melanoma in five years. One of these factors = 8% risk of conversion in five years. Two or more factors = 50% risk of conversion in five years. For any changes noted during the course of follow-up, refer the patient to a retinal practice or an ocular oncology service. Case • 65 yr old white male – Notices spot in vision in his left eye – Diabetes for 15 years • Vision:6/6 (20/20) and 6/12 (20/40) • Dilated exam: – Large lesion noted in left eye (not noted in exam 6 months previously – See photo Ocular Tumors Astrocytic Hamartoma Retinoblastoma Amelanotic Melanoma Metastatic Choroidal Tumor Choroidal Melanoma Metastases • 80 to 90% of metastases from uveal melanoma occurred in the liver, less common sites being the skin and lung. – Gragoudas ES, Seddon JM, Egan KM, et al. Longterm results of proton beam irradiated uveal melanomas. Ophthalmology. 1987;94:349–53. CASE 3 Case • 23 WM – Eye pain OD – Severe, started 2 days ago – Photophobia and redness • POHx: – Had similar problem and was given drops and felt better • PMHx: – Told to get back into shape and to reduce stress • Meds: – Ibuprofen for lower back pain Assessment • VA: • 6/6 (20/20)-, • 6/6 (20/20)+ • Entrance skills unremarkable • SLE: – OD: • • • • 2+ injection, 2+ cell, Mild flare, Fine deposits – IOP: 18, 14 mm HG • DFE: unremarkable Uveitis • Uveitis frequently is nonspecific but can be associated with: – systemic disease, – occur following trauma, or – be the result of a primary ocular disorder such as: • Fuchs's heterochromic iridocyclitis or • glaucomatocyclitic crisis (ie, Possner-Schlossman syndrome) Helpful Mnemonic • Mnemonic for acute forms of nongranulomatous uveitis: BLAIR G – B: Behcet’s disease – L: Lyme disease – A: Ankylosing spondilitis – I: Irritable bowel syndrome (Crohn’s) – R: Reactive arthritis – G: Glaucomatocyclitic crisis Uveitis: Clinical Features • The clinical features of anterior uveitis are readily recognizable – complaints of: • photophobia, • pain, • blurred or variable vision • A change in the blood-aqueous barrier results in the liberation of protein and cellular matter into the anterior chamber and the vitreous. Uveitis: Clinical Findings • Clinical findings of: – circumlimbal hyperemia, – cells and flare in the aqueous and anterior vitreous, and – keratic and trabecular precipitates Uveitis: Treatment – “Classical treatment”: • Pred forte: every 1-2 hours, ensure taper –Pred forte: prednisolone acetate formulation which allows penetration through cornea to anterior chamber – Newer treatment option: • Durezol Treatment Options • Durezol: – Difluprednate • only difluorinated steroid – Steroid emulsion – BAK free – Increased “potency” so dosing needs to be less than “classical treatment” with Pred Forte • rough recommendation is 1/2 dosing of Pred Forte Cycloplegics • Common cycloplegic agents include: – cyclopentolate 1-2% tid for mild-tomoderate, – homatropine 5% BID – scopolamine 0.25% – atropine 1% bid-tid for moderate-to-severe inflammation • most common is the use of Homatropine 5% bid • be careful using atropine as there is potential for severe systemic side effects – also makes the iris essentially immobile Cycloplegics • Cycloplegia: – used for reduction of pain, – break/prevent the formation of posterior synechiae – also functions in the reduction of inflammation Treatment • Topical administration is most common though periocular injections and systemic meds are useful for posterior uveitis and difficult cases • Dosing is dependent upon severity of the inflammation – typically you want to hit the uveitis hard and fast! • E.g 1 gtt q 2hrs until the inflammation is gone! • If you have a minimal anterior chamber reaction then steroid may not be necessary at all Treatment • NOTE: it is crucial to taper your steroid treatment! – You will have a rebound inflammation if you simply remove your patient from their steroids… – The taper will be dependent upon how long you have had them on the steroid to get rid of the inflammation! – Typically, a slow taper is better in order to prevent rebound inflammation – If the patient has been on the steroid for less than a week a faster taper can be considered. Treatment • NSAIDs: – do not play an important role in the treatment of an acute uveitis Treatment: Additional Therapies • Immunosuppressive agents (cytotoxic) – reserved for sight-threatening uveitis that have not responded to conventional treatment • e.g. cyclophosphamide • Antimetabolites (e.g. methotrexate) have been found useful in JIA related iridocyclitis and scleromalacia • Cyclosporin has a very specific effect on the immune system and has been found useful in posterior and intermediate uveitis Follow-up • Every 1-7 days in acute phase depending upon severity and every 1-6 months when stable. • On each f/u visit the AC reaction and IOP should be evaluated – DFE should be performed for flareups, when VA affected, or every 3-6 months. Follow Up • If AC reaction improving, then steroid drops can be slowly tapered. – cycloplegia can also be tapered as the AC reaction improves. – slow taper recommended for chronic granulomatous uveitis. CASE 4 Case • 65 year old Caucasian patient presents with sudden onset loss/blurring of vision in the right eye • PMHx: HTN for 15 years, takes “water pill” • VA’s: 6/18 (20/60) OD, 6/7.5 (20/25) OS • Pupils: PERRL –APD • CVF: Inferior defect right eye, no defects noted in the left eye Vision Loss Without Pain: Diabetes/Diabetic Retinopathy Microvascular complications resulting in capillary closure & abnormal permeability S&S include; ◦ blurring of vision (maculopathy and refractive error shifts), ◦ sudden drop in vision (vitreous heme), ◦ dot and blot hemes, ◦ exudate, ◦ cotton wool spots, ◦ neovascularization (iris, retina and disc) VEGF and DME Aug. 10, 2012: FDA approves Lucentis to treat diabetic macular edema • The drug’s safety and effectiveness to treat DME were established in two clinical studies involving 759 patients who were treated and followed for three years. – patients were randomly assigned to receive monthly injections of Lucentis at 0.3 milligrams (mg) or 0.5 mg, or no injections during the first 24 months of the studies – after 24 months, all patients received monthly Lucentis either at 0.3 mg or 0.5 mg • Results: – 34-45% of those treated with monthly Lucentis 0.3 mg gained at least three lines of vision compared with 1218% of those who did not receive an injection. Vision Loss Without Pain: Vein Occlusion • Associated with: – – – – hypertension, coronary artery disease, DM and peripheral vascular disease. • Usually seen in elderly patients (60-70), slight male and hyperopic predilection. • Second most common vascular disease after diabetic retinopathy. Branch Retinal Vein Occlusion: Signs/Symptoms BRVO: sudden, painless, visual field defect. ◦ patients may have normal vision. ◦ quadrantic VF defect, ◦ dilated tortuous retinal veins with superficial hemes and CWS ◦ typically occurs at A/V crossing (sup/temp) BRVO BRVO more common than CRVO and has more favorable prognosis ◦ Overall 50-60% of BRVO patients will maintain VA of 6/12 (20/40) or better Visual loss results from: ◦ ◦ ◦ ◦ ◦ ◦ ◦ Macular edema Foveal hemorrhage Vitreous heme Epiretinal membrane RD Macular ischemia Neovascularization complications Study Design (n=397) BRVO BRAnch retinal Vein Occlusion study safety/efficacy Macular Edema Secondary to BRVO 1:1:1 Randomization Sham (n=132) Ranibizumab 0.3 mg (n=134) Ranibizumab 0.5 mg (n=131) Monthly Injections (last at 5M) Rescue Laser (if eligible beginning at Month 3) 12M PRN ranibizumab for all patients Rescue Laser (if eligible beginning at Month 9) Ranibizumab 0.5 mg Ranibizumab 0.3 mg Ranibizumab 0.5 mg Month 6 Primary Endpoint Mean Change from Baseline BCVA BRVO Mean Change from Baseline BCVA (ETDRS Letters) Sham/0.5 mg (n=132) 0.3 mg Ranibizumab (n=134) 0.5 mg Ranibizumab (n=131) +18.3* 20 +18.3 18 +16.4 16 14 +16.6* +11.6 +12.1 12 10 +10.2 8 +7.3 6 +3.1 4 2 0 07 2 4 Day 0–Month 5 Monthly Treatment 6 Month 8 10 Months 6–11 PRN Treatment The gain of additional 3 lines occurred at a rate of 61% of 0.5 AVT grp, 55% for 0.3 AVT & 29% placebo 12 Central Retinal Vein Occlusion: Signs/Symptoms CRVO: thrombus occurring at lamina is classical theory but new evidence indicates that the occlusion is typically in the optic nerve posterior to the lamina cribrosa ◦ decreased VA ranging from near normal to hand motion with majority 6/60 (20/200) range ◦ dilated tortuous vessels, with numerous retinal hemes and CWS Central Retinal Vein Occlusion • Visual morbidity and blindness are primarily from: – persistent macular edema, – macular ischemia and – neovascular glaucoma • CRVO’s can be ischemic or non. – Classical definition of ischemic is 10-disc area of nonperfusion found on angiography – RAPD and ERG maybe better predictor – VA’s typically worse in ischemic – Increased number of cotton wool spots with decreased VA maybe predictive Central Retinal Vein Occlusion Ischemic CRVO may lead to iris neovascularization and neovascular glaucoma ◦ Estimated apprx 20% of CRVO’s are ischemic with 45% of those developing neo Regular examinations (1-2 wks) to monitor for ischemia or neo development ◦ should include gonio as angle neo can precede iris rubeosis Study Design CRUISE (n=392) CRVO Central Retinal vein occlUsIon Study: Efficacy & safety Macular Edema Secondary to CRVO 1:1:1 Randomization Sham (n=130) Ranibizumab 0.3 mg (n=132) Ranibizumab 0.5 mg (n= 130) Monthly Injections (last at 5M): 6M tx period 12M trial PRN Lucentis available for for all patients: 6M tx period 0.5 mg Ranibizumab 0.3 mg Ranibizumab 0.5 mg Month 6 Primary Endpoint Mean Change from Baseline BCVA CRVO 0.3 mg Ranibizumab (n=132) Mean Change from Baseline BCVA (ETDRS Letters) Sham/0.5 mg (n=130) 0.5 mg Ranibizumab (n=130) 18 16 +14.9* +13.9 +13.9 14 12 +12.7* 10 8 +7.3 6 4 +0.8 2 0 -2 07 2 4 Day 0–Month 5 Monthly Treatment 6 8 10 Months 6–11 PRN Treatment 12 Month Pts with >/= 3 line improvement was noted in 48% of .5 AVT, 26 of .3 AVT & 17% of sham Vision Loss Without Pain: Artery Occlusion • Primarily embolic in nature from cholesterol, calcifications, plaques. • Usually occurs in elderly associated with: – hypertension (67%), – carotid occlusive disease (25%), – DM (33%) and – cardiac valvular disease. • Sudden loss of unilateral, painless vision – defect dependent upon location of occlusion Vision Loss Without Pain: Artery Occlusion • BRAO typically located in temporal retinal bifurcations. CRAO • CRAO has profound vision loss with history of amaurosis fugax. – Vision is usually CF (count fingers) to LP (light perception) with positive APD. – Diffuse retinal whitening with arteriole constriction, cherry red macula. Ophthalmic Emergency Treatment is controversial due to poor prognosis and questionable benefit. Treat immediately before workup, if patient presents within 24 hours of visual loss: ◦ ◦ ◦ ◦ ◦ Digital ocular massage, systemic acetozolamide (500 mg IV or po), topical ocular hypertensive drops (Iopidine, B-blocker), anterior chamber paracentesis, consider admission to hospital for carbogen Tx (high carbon dioxide) CASE 5 Case • 30 WM presents with 2 weeks worsening vision OS – Was seen by neurologist 2 years previously for flashes, head CT was normal – Flashes continued for the two years – History of color blindness – Patient presents with pressure behind the eye and tightness with left eye movement for the past week – No vision changes with activity or movement – Denies history of trauma, redness, discharge or headache • VA: 6/6 (20/20) and 6/9 (20/30) • External exam reveals no ptosis or resistance to retropulsion Case • PERRL with a left APD • Hertel: Base of 102 and measurements of 19 and 18 • EOM: FROM though notes tight feeling in OS abduction • IOP: 15 OU • DFE: normal ONH appearance and fundus unremarkable • HVF: inferior altitudinal defect OS Case • One week f/u: • Reports continued decreasing vision OS – Now 6/120 (20/400) • Increased left APD • Increased visual field defect • ONH swelling OS Question Which of the following MRI scans goes with this patient’s diagnosis? 1 2 3 4 Optic Neuritis • Optic neuritis typically presents with a triad of symptoms: – loss of vision, dyschromatopsia and eye pain. • The initial attack is unilateral in 70% of adult patients and bilateral in 30%. • Associated visual symptoms are reduced perception of light intensity and Uhthoff's symptom (visual deficit induced by exercise or increased body temperature) • The mean age of onset of optic neuritis is in the third decade of life Optic Neuritis Treatment • The ONTT showed that intravenous methylprednisolone followed by oral prednisone speeds the recovery of visual loss • Oral prednisone was found to increase the risk of recurrent optic neuritis. – Thus, treatment with oral prednisone in standard doses is no longer advised. Case 6 Case History/Entrance Skills • • • • • • • 31 YR HM CC: referred from PCP for a possible uveitis LEE: 3 years ago PMHx: unremarkable Meds: Omega-3 supplements Entrance VA: 6/9 (20/30) OD, OS Refraction: – +0.75 -2.50 x 003 6/7.5+ (20/25+) – +0.25 -2.75 x 004 6/7.5+ (20/25+) • All other entrance skills unremarkable except for difficulty doing confrontation visual fields 76 Health Assessment • SLE: – 1+ conjunctival injection in the right eye – Anterior chamber: deep and quiet (no cells or flare noted in either eye) • IOP: 12 and 11 OD, OS • DFE: see photos 77 OS OD 78 OS OD 79 OS OD 80 81