Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
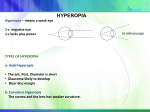
1. Korean J Ophthalmol. 2007 Sep;21(3):159-62. Links Reduction of deviation angle during occlusion therapy: in partially accommodative esotropia with moderate amblyopia. Chun BY, Kwon SJ, Chae SH, Kwon JY. Department of Ophthalmology, Kyungpook National University, School of Medicine, Daegu, Korea. PURPOSE: To evaluate changes in ocular alignment in partially accommodative esotropic children age ranged from 3 to 8 years during occlusion therapy for amblyopia. METHODS: Angle measurements of twenty-two partially accommodative esotropic patients with moderate amblyopia were evaluated before and at 2 years after occlusion therapy. RESULTS: Mean deviation angle with glasses at the start of occlusion treatment was 19.45plusmn;5.97 PD and decreased to 12.14plusmn;12.96 PD at 2 years after occlusion therapy (p<0.01). After occlusion therapy, 9 (41%) cases were indications of surgery for residual deviation but if we had planned surgery before occlusion treatment, 18 (82%) of patients would have had surgery. There was a statistical relationship between increase of visual acuity ratio and decrease of deviation angle (r=-0.479, p=0.024). CONCLUSIONS: There was a significant reduction of deviation angle of partially accommodative esotropic patients at 2 years after occlusion therapy. Our results suggest that occlusion therapy has an influence on ocular alignment in partially accommodative esotropic patients with amblyopia. PMID: 17804922 [PubMed - in process] 2. 1: Ophthalmology. 2007 Jul 28; [Epub ahead of print] Links Prevalence of Hyperopia and Associations with Eye Findings in 6and 12-Year-Olds. Ip JM, Robaei D, Kifley A, Wang JJ, Rose KA, Mitchell P. Department of Ophthalmology (Centre for Vision Research, Westmead Hospital), Westmead Millennium Institute, University of Sydney, and Vision Cooperative Research Centre, Sydney, Australia. PURPOSE: To describe the prevalence of hyperopia and associated factors in a representative sample of Australian schoolchildren 6 and 12 years old. DESIGN: Population-based cross-sectional study. PARTICIPANTS: Schoolchildren ages 6 (n = 1765) and 12 (n = 2353) from 55 randomly selected schools across Sydney. METHODS: Detailed eye examinations included cycloplegic autorefraction, ocular biometry, cover testing, and dilated fundus examination. Information on birth and medical history were obtained from a parent questionnaire. MAIN OUTCOME MEASURES: Moderate hyperopia defined as spherical equivalent (SE) refraction of >/=+2.00 diopters (D), and eye conditions including amblyopia, strabismus, astigmatism, and anisometropia. RESULTS: Prevalences of moderate hyperopia among children ages 6 and 12 were 13.2% and 5.0%, respectively; it was more frequent in children of Caucasian ethnicity (15.7% and 6.8%, respectively) than in children of other ethnic groups. Compared with children without significant ametropia (-0.49 </= SE refraction </= +1.99 D), the prevalence of eye conditions including amblyopia, strabismus, abnormal convergence, and reduced stereoacuity was significantly greater in children with moderate hyperopia (all Ps < 0.01). Maternal smoking was significantly associated with moderate hyperopia among 6-year-olds (P = 0.03), but this association was borderline among 12-year-olds (P = 0.055). Early gestational age (<37 weeks) and low birth weight (<2500 g) were not statistically significant predictors of moderate hyperopia in childhood. CONCLUSIONS: Moderate hyperopia was strongly associated with many common eye conditions, particularly amblyopia and strabismus, in older children. Birth parameters did not predict moderate hyperopia. PMID: 17664011 [PubMed - as supplied by publisher] 3. J Fr Ophtalmol. 2007 Mar;30(3):255-9. Links [Management of hyperopia in children] [Article in French] Jeddi Blouza A, Loukil I, Mhenni A, Khayati L, Mallouche N, Zouari B. Service d'Ophtalmologie, Hôpital La Rabta, Tunis, Tunisie. PURPOSE: To study the prevalence of hyperopia in school-aged children and to analyze the factors that increase the risk of squint or amblyopia in a retrospective study. METHODS: Three hundred eyes of 150 children with hyperopia who did not have anisometropia > or =1.5 D were selected. Complete ophthalmological examination was performed for all children. Hyperopia was defined when spherical equivalent was +0.5 D or greater. Amblyopia was screened and treated by patching therapy and then penalisation. Complete spectacle correction was achieved in children with high hyperopia (+3.5 D or greater) or in presence of squint or amblyopia. A statistical analysis compared the results using the Mann-Whitney test and the chi square test. RESULTS: The mean age was 9.5+/-2.7 years. Girls were statistically more represented than boys. The mean sphere measured overall was +2 D (+/-1.65). Severe hyperopia was detected in 19% of the children; it was latent in 35% of children. Strabismus was detected in 7% and was accommodative in 25%. Esotropia was the most prevalent deviation (72.8%). The prevalence of amblyopia was 12%. The mean sphere measured in amblyopic children was 5.66 D (+/-1.64 D). Initial depth of amblyopia was mild to moderate and 98% of the children achieved iso-acuity after patching therapy. The correlation between severe hyperopia, amblyopia, and squint was statistically significant. Indeed, the risk ratios of squint and amblyopia, 5.2 and 3.70, respectively, were significantly high in children with severe hypermetropia. Complete spectacle correction improved final visual acuity and reduced the angle deviation in accommodative esotropia. CONCLUSION: Children with hyperopia of +3.5 D or greater have an increased risk of amblyopia and squint that threatens their visual function. Hyperopic correction should be prescribed even if no strabismus or amblyopia is detected in order to prevent this risk. Screening programs should also be promoted to detect these children at an early age. 4. Survey of German Clinical Prescribing Philosophies for Hyperopia. REITER, CONSTANTIN BS; LEISING, DANIEL PhD; MADSEN, ELLIS M. MS, OD, FAAO [Article] Optometry & Vision Science. 84(2):131-136, February 2007. (Format: HTML, PDF) Purpose. We surveyed a group of German ophthalmologists to evaluate their prescribing philosophies for hyperopic refractive error in symptom-free children and to compare them with the two groups of U.S. pediatric ophthalmologists and U.S. pediatric optometrists as surveyed by Lyons et al. Methods. Practitioners were selected from a list of ophthalmologists on the Internet. They were either in general practice in three cities in northern Bavaria or affiliated with large ophthalmology teaching hospitals in Wuerzburg and Erlangen. The survey questions of Lyons et al. were translated into German and mailed to 103 ophthalmologists. The data received from the German ophthalmologists were compared with those of the U.S. optometrists and ophthalmologists. Results. A total of 45 surveys (44%) were returned to us and analyzed. In cases of asymptomatic bilateral hyperopia, German ophthalmologists did not prescribe significantly differently from U.S. optometrists at all patient age groups (p >= 0.05), but they did differ significantly from U.S. ophthalmologists (p < 0.001). Prescribing fractional amounts of hyperopia or astigmatism was not a popular rule of thumb among the German ophthalmologists, and there was no statistical difference between the German and U.S. practitioners. German ophthalmologists would prescribe for anisometropia for all patient age groups in the same way as both U.S. optometrists and U.S. ophthalmologists. Conclusion. The prescribing philosophies of German ophthalmologists for pediatric patients did not differ from those of U.S. ophthalmologists and U.S. optometrists when prescribing for anisometropia; they did differ from those of U.S. ophthalmologists but not of those of the U.S. optometrists when prescribing for asymptomatic bilateral hyperopia 5. 1: Optom Vis Sci. 2007 Feb;84(2):115-23. Links The epidemiology of early childhood hyperopia. Tarczy-Hornoch K. Department of Ophthalmology, University of Southern California/Childrens Hospital Los Angeles, Los Angeles, California, USA. [email protected] Hyperopia is present in a small proportion of children aged between 6 and 12 months, with ethnicity likely affecting prevalence, and higher prevalences in certain subgroups, especially those with a family history of hyperopia or accommodative esotropia. Around a fifth of children who are hyperopic in infancy go on to develop strabismus, while an unknown proportion develop bilateral ametropic amblyopia; persistent hyperopia appears to be a harbinger of future pathology. Early prophylactic spectacle correction of hyperopia has failed to prevent strabismus in three of four studies, but showed reduced incidence of strabismus in one study, and yielded improved visual acuity outcomes in two studies by one investigator. Currently our ability to detect or measure refractive error with automated instruments easily adaptable to a screening setting has outpaced our knowledge of how best to identify the subset of hyperopes who are really at risk, and how to manage isolated early hyperopia once it has been identified 6. 1: Optom Vis Sci. 2007 Feb;84(2):103-9. Related Articles, Links Management of childhood hyperopia: a pediatric optometrist's perspective. Cotter SA. Southern California College of Optometry, Fullerton, California, USA. [email protected] PURPOSE: To provide an optometric perspective on the management of hyperopia in children without strabismus or amblyopia. METHODS: Factors that have potentially shaped optometry's viewpoint and influenced its prescribing philosophy for childhood hyperopia, such as optometry school and residency training, professional association clinical guidelines, conferences and continuing education courses, textbooks, scientific studies, opinions of professional leaders, and clinical experiences are discussed. RESULTS: Variations in prescribing patterns for childhood hyperopia occur within optometry and within ophthalmology. There are also differences in prescribing philosophies between the two professions. These differences are probably due to a greater level of concern, more so among optometrists, about associated vision functions such as accommodation, vergence, and stereopsis, as well as concerns about the potential impact of uncorrected hyperopia on reading and school performance. CONCLUSIONS: If indications for prescribing spectacles for children with hyperopia are to be validated, randomized controlled trials need to be performed. Publication Types: • Review PMID: 17299339 [PubMed - indexed for MEDLINE] 2: Optom Vis Sci. 2007 Feb;84(2):97-102. Related Articles, Links To emmetropize or not to emmetropize? The question for hyperopic development. Mutti DO. The Ohio State University College of Optometry, Columbus, Ohio, USA. Emmetropization appears to be a rapid process, occurring in the first year of life. Failure to emmetropize leaves about 2 to 8% of children with potentially clinically significant hyperopia after infancy. Uncorrected hyperopia in childhood has a negative impact on distance acuity and the accuracy of the accommodative response for some unknown number of children. The clinical "gray zone" for these problems as judged by distance refractive error alone might begin somewhere around +2.00 to +3.00 D. Use of a refractive correction seems to improve distance acuity and the accuracy of accommodation. Clinicians' reluctance to prescribe hyperopic corrections to children to improve visual performance might be unwarranted. If emmetropization is largely complete, if defocus has only a minor effect on the development of refractive error in infancy or childhood, and if the hyperopic eye is already growing longer but not moving toward emmetropia, then there may be little reason to either wait or be concerned about interfering with emmetropization that may never happen. The immediate visual benefit may outweigh these concerns. Publication Types: • Research Support, N.I.H., Extramural • Research Support, Non-U.S. Gov't • Review PMID: 17299338 [PubMed - indexed for MEDLINE] 3: Optom Vis Sci. 2007 Feb;84(2):84-96. Related Articles, Links Infant hyperopia: detection, distribution, changes and correlates-outcomes from the cambridge infant screening programs. Atkinson J, Braddick O, Nardini M, Anker S. Visual Development Unit, University College London, London, United Kingdom. [email protected] PURPOSE: To report on two population screening programs designed to detect significant refractive errors in 8308 8- to 9month-old infants, examine the sequelae of infant hyperopia, and test whether early partial spectacle correction improved visual outcome (strabismus and acuity). The second program also examined whether infant hyperopia was associated with developmental differences across various domains such as language, cognition, attention, and visuomotor competences up to age 7 years. Linked programs in six European countries assessed costs of infant refractive screening. METHOD: In the first program, screening included an orthoptic examination and isotropic photorefraction, with cycloplegia. In the second program we carried out the same screening procedure without cycloplegia. Hyperopic infants (> or = +4 D) were followed up alongside an emmetropic control group, with visual and developmental measures up to age 7 years, and entered a controlled trial of partial spectacle correction. RESULTS: The second program showed that accommodative lag during photorefraction with a target at 75 cm (focus > or = +1.5 D) was a marker for significant hyperopia. In each program, prevalence of significant hyperopia at 9 to 11 months was around 5%; manifest strabismus was 0.3% at 9 months and 1.5 to 2.0% by school age. Infant hyperopia was associated with increased strabismus and poor acuity at 4 years. Spectacle wear by infant hyperopes produced better visual outcome than in uncorrected infants, although an improvement in strabismus was found in the first program only. The corrections did not affect emmetropization to 3.5 years; however, both corrected and uncorrected groups remained more hyperopic than controls in the preschool years. The hyperopic group showed poorer overall performance than controls between 1 and 7 years on visuoperceptual, cognitive, motor, and attention tests, but showed no consistent differences in early language or phonological awareness. Relative cost estimates suggest that refractive screening programs can detect visual problems in infancy at lower overall cost than surveillance in primary care. CONCLUSIONS: Photo/videorefraction can successfully screen infants for refractive errors, with visual outcomes improved through early refractive correction. Infant hyperopia is associated with mild delays across many aspects of visuocognitive and visuomotor development. These studies raise the possibility that infant refractive screening can identify not only visual problems, but also potential developmental and learning difficulties. Publication Types: • Research Support, Non-U.S. Gov't • Review PMID: 17299337 [PubMed - indexed for MEDLINE] 4: Optom Vis Sci. 2007 Feb;84(2):80. Related Articles, Links Infant and child hyperopia. Mutti DO, Candy R, Cotter SA, Haegerström-Portnoy G. Publication Types: • Editorial PMID: 17299334 [PubMed - indexed for MEDLINE] 5: Eye. 2007 Feb 2; [Epub ahead of print] Related Articles, Links Ethnic differences in refraction and ocular biometry in a population-based sample of 11-15-year-old Australian children. Ip JM, Huynh SC, Robaei D, Kifley A, Rose KA, Morgan IG, Wang JJ, Mitchell P. 1Department of Ophthalmology and the Westmead Millennium Institute, Centre for Vision Research, University of Sydney, Sydney, Australia. PurposeTo examine the prevalence of refractive error and distribution of ocular biometric parameters among major ethnic groups in a population-based sample of 11-15-year-old Australian children.MethodsThe Sydney Myopia Study examined 2353 students (75.3% response) from a random cluster-sample of 21 secondary schools across Sydney. Examinations included cycloplegic autorefraction, and measures of corneal radius of curvature, anterior chamber depth, and axial length.ResultsParticipants mean age was 12.7 years (range 11.114.4); 49.4% were female. Overall, 60.0% of children had European Caucasian ethnicity, 15.0% East Asian, 7.1% Middle Eastern, and 5.5% South Asian. The most frequent refractive error was mild hyperopia (59.4%, 95% confidence interval (CI), 53.265.6), defined as spherical equivalent (SE) +0.50 to +1.99 D. Myopia (SE-0.50 D or less) was found in 11.9%, 95% (CI 6.617.2), and moderate hyperopia (SE>/=+2.00 D) in 3.5%, 95% (CI 2.8-4.1). Myopia prevalence was lower among European Caucasian children (4.6%, 95% CI 3.1-6.1) and Middle Eastern children (6.1%, 95% CI 1.3-11.0) than among East Asian (39.5%, 95%, CI 25.6-53.5) and South Asian (31.5%, 95%, CI 21.6-41.4) children. European Caucasian children had the most hyperopic mean SE (+0.82 D) and shortest mean axial length (23.23 mm). East Asian children had the most myopic mean SE (-0.69 D) and greatest mean axial length (23.86 mm).ConclusionThe overall myopia prevalence in this sample was lower than in recent similaraged European Caucasian population samples. East Asian children in our sample had both a higher prevalence of myopia and longer mean axial length.Eye advance online publication, 2 February 2007; doi:10.1038/sj.eye.6702701. PMID: 17277756 [PubMed - as supplied by publisher] 1: J Zhejiang Univ Sci B. 2006 Nov;7(11):884-6. Links Spectacle correction of heterophoria in hyperopic amblyopic children. Liu X, Li YM, Li Y. Ophthalmic Center, the First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou 310003, China. OBJECTIVE: To test the effects of corrective spectacles in hyperopic amblyopic children with heterophoria. METHODS: Visual acuity, refraction and the amount of heterophoria on near (33 cm) fixation were measured before and after 3 weeks of spectacle-wearing in 30 hyperopic amblyopic children with heterophoria. The control group consisted of 20 emmetropic children age-matched to the patients. RESULTS: Uncorrected eyes displayed hyperopic amblyopia accompanied by heterophoria. Corrective spectacles not only attenuated the hyperopia and amblyopia, but also changed the heterophoria to orthophoria. The amount of heterophoria before wearing spectacles was significantly different from that in emmetropic children; but after correction with spectacles, it was the same as that in the emmetropic controls. CONCLUSION: Correction with spectacles is effective for the treatment of heterophoria in hyperopic children with amblyopia. 1: Ophthalmology. 2007 Feb;114(2):374-82. Epub 2006 Nov 21. Links Refractive error and visual impairment in school children in rural southern China. He M, Huang W, Zheng Y, Huang L, Ellwein LB. Key Laboratory of Ophthalmology and Zhongshan Ophthalmic Center, Sun Yat-Sen University, Guangzhou, China. PURPOSE: To assess the prevalence of refractive error and visual impairment in school children in a rural area of southern China. DESIGN: Prospective cross-sectional survey. PARTICIPANTS: Two thousand four hundred children from junior high schools in Yangxi County. METHODS: Random selection of classes from the 3 junior high school grade levels was used to identify the study sample. Children from 36 classes in 13 schools were examined in April 2005. The examination included visual acuity (VA) testing; ocular motility evaluation; cycloplegic autorefraction; and examination of the external eye, anterior segment, media, and fundus. MAIN OUTCOME MEASURES: Distance VA and cycloplegic refraction. RESULTS: Among 2515 enumerated children, 2454 (97.6%) were examined. The study population consisted of the 2400 children between 13 and 17 years old. Prevalences of uncorrected, presenting, and best-corrected VA < or = 20/40 in the better eye were 27.0%, 16.6%, and 0.46%, respectively. Sixty percent of those who could achieve acuity > or =20/32 in at least one eye with best correction were without the necessary spectacles. Refractive error was the cause in 97.1% of eyes with reduced vision; amblyopia, 0.81%; other causes, 0.67%; and unexplained causes, 1.4%. Myopia (spherical equivalent, -0.50 diopters [D] or more in either eye) affected 36.8% of 13-yearolds, increasing to 53.9% of 17-year-olds. Myopia was associated with higher grade level, female gender, schooling in the county urban center, and higher parental education. Hyperopia (+2.00 D or more) affected approximately 1.0% in all age groups. Astigmatism (> or =0.75 D) was present in 25.3% of all children. CONCLUSIONS: Reduced vision because of uncorrected myopia is a public health problem among school-age children in rural China. Effective VA screening strategies are needed to eliminate this easily treated cause of visual impairment