Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
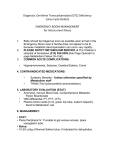
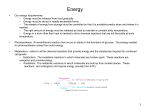
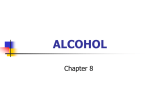
[CANCER RESEARCH 37, 2336-2347, July 1977] Energy Metabolism and Requirements in the Cancer Patient1 Vernon R. Young Department of Nutrition and Food Science, Massachusetts Institute of Technology, Cambridge, Massachusetts 02139 Summary As a basis for assessing energy metabolism and require ments in cancer patients, selected aspects of whole-body energy metabolism are considered, with particular refer ence to basal energy metabolism and factors that affect it. The importance of protein metabolism in relation to whole body energy metabolism is emphasized. The need to con sider the intimate relationships between protein and energy nutrition and metabolism in the comprehensive evaluation of the energy needs of cancer patients also is stressed. Published data on the basal metabolic rate of patients with malignant disease are difficult to evaluate for their meta bolic and nutritional significance. Quantitative estimates of the utilization of major fuel sources in cancer patients are still quite limited, but the available data suggest that there may be a change in the pattern of fuel utilization, with lipid sources predominating, an altered regulation of glucose metabolism, and a reduced efficiency of energy utilization in some, but not all, cancer patients. The best balance of the major exogenous energy sources and level of total energy intake sufficient to meet the energy demands of organs and the whole body cannot be easily predicted and, therefore, only crude guidelines can be suggested. Introduction Investigations of the characteristics of energy metabolism and of the assessment of energy requirements in cancer patients are limited. However, the maintenance of cell and organ function involves decreased entropy, and this implies an increased requirement for energy. Thus, an adequate understanding of the metabolism and utilization of fuel sources and of the regulation of whole-body energy ex penditure is important in considerations of nutritional ther apy for cancer patients. An important question to explore is whether the presence of cancer per se presents a unique set of problems in relation to energy metabolism and requirements, or whether the problems are similar to those of patients with nonmalignant disease. Because cachexia, accompanied by reduced food intake, is often a prominent feature of ad vanced cancer (17, 77, 80), it could be argued that there is a failure to maintain normal regulation and efficient patterns of fuel utilization and, therefore, body protein composition and cell mass. Hence, some selected aspects of energy metabolism and factors that alter basal metabolism and the I Based on a paper presented at the Conference on Nutrition Therapy, November 29 to December 1, 1976, Key Biscayne, Fla. 2336 and utilization and need for energy will be reviewed here as a basis for assessing the status of energy metabolism and requirements in the cancer patient. It is hoped that this brief review will help to identify those aspects of energy metabo lism and nutrition that deserve more critical and extensive investigation, in order to develop more effective and ra tional approaches to the nutritional support of patients with malignant disease. Major emphasis will be given here to data from human studies. Basal and Resting Metabolic Rate Physical activity and basal metabolism are among the major factors that determine total daily energy expenditure. The former will not receive detailed mention here; for the present, it will be assumed that, in energy expenditure due to physical activity, differences between cancer patients and those suffering from other disease states and normal subjects are due to the intensity of physical exercise and time devoted to such activities. The metabolic aspects of energy expenditure and utilization will receive the major focus in this paper. For individuals who spend a large portion of the day ‘ ‘at rest,― the BMR,2 defined as the energy output of an individ ual under standard resting conditions (bodily and mentally at rest, 12 to 18 hr after a meal, in a neutral, thermal environment), accounts for a significant proportion of total daily energy expenditure (16). It is appropriate, therefore, to consider first the biochemical basis of the BMR and some of the factors that affect it. At the outset, it must be noted that a precise determina tion of BMR is not easy to achieve in practice (20), and a more useful measure of metabolic rate may be obtained by measurement of the resting metabolic rate (14). This may be determined in a person at rest, 2 to 4 hr after a light break fast. However, a distinction between basal and resting me tabolism does not require particular emphasis in the discus sion that follows and, forthe present purpose, these param eters of energy metabolism will be used synonymously. Resting energy metabolism represents the combustion of fuel sources needed to provide energy for metabolic proc esses involved in maintaining the function and integrity of cells and body organs and for the mechanical processes involved in keeping the body alive. Synthetic processes, such as protein, nucleic acid and lipid synthesis and gluco neogenesis, transport processes, including the pumping of ions to maintain ion gradients within cells and organelles and, finally, mechanical processes involving muscular ac Cancer 2 The abbreviation used is: BMR, basal metabolic rate. CANCERRESEARCHVOL. 37 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 1977 American Association for Cancer Research. Energy Requirements tivity, require energy inputs. These are obtained from high energy phosphate compounds, usually ATP, generated dur ing the oxidation of the major energy-yielding substrates. Hence, these various processes and their associated energy needs constitute a biochemical basis of the basal rate of energy expenditure. Various factors alter the activities of these processes and the types of substrate used for supply ing energy. The contribution made by the various body organs to BMR in the healthy adult is summarized in Table 1. It has been estimated that the liver accounts for approximately 27% of resting metabolism, with the brain, skeletal muscle, and remainder also being important sites of total body energy expenditure (65). Thus, the proportion ofthese body organs in relation to total body weight will affect values for BMR when expressed per unit body weight or surface area. Because the relative contributions of the body organs to total body weight change with growth and development (53), aging (72), malnutrition (21), and pathological states, interpretation of the metabolic significance of differences in BMR among differing groups of patients must be cautious. It is possible that alterations in the body organ compart ments would bring about differences in BMR without any real change in the status of energy metabolism within the organs themselves. this lactate is more or less quantitatively resynthesized to glucose (45). This cyclic metabolic pathway, involving con version of glucose to lactate and the return of lactate to glucose, is termed the Con cycle. Utilization of lactate for glucose synthesis is an energy-requiring process, and an increased rate of conversion of lactate to glucose has been proposed as a mechanism for the increased energy expend iture of the tumor-bearing patient (17, 25). It is well known that tumors show high rates of anaerobic glycolysis with production of lactic acid (24, 79), and studies in cancer patients show increased lactate production. Holroyde et al. (36) recently reported a series of studies on Con cycle activity in a heterogeneous group of patients with metastatic carcinoma (Table 3). Patients without pro gressive weight loss appeared to have normal glucose me tabolism, but Con cycle activity was increased in patients with progressive weight loss, showing that lactate produc tion rates were higher in these patients. Gold (25) proposed that the increased rate of resynthesis of glucose in the liver from the lactate produced by the tumor acts as a significant energy drain on host tissues. However, from the data shown in Table 3 and from addi tional estimates of the rate of lactate production and recy cling in cancer patients (68, 81), increased Con cycle activ ity does not appear to account for a significant fraction of daily energy expenditure. Thus, if 6 moles of high-energy Fuel Sources in Relation to Resting Metabolism The major substances used as sources of energy in mam malian tissues are glucose, fatty acids, ketone bodies, amino acids, and lactate (9, 45). Although these are inter changeable sources of energy in the whole organism, mdi vidual organs show some specificity with respect to their use of fuel sources (Table 2). For a well-nourished adult subject in the basal state, glucose is utilized at a rate of 140 g/day, equivalent to 560 kcal. The oxidation of amino acids, liberated during the course of tissue protein breakdown, can be estimated to amount to 75 g/day, or 375 kcal. The rest of the daily energy flux is accounted for largely by the oxidation of 130 g triglyceride, equivalent to 1170 kcal. In the resting human adult, about 20 g lactate are formed daily, mainly by blood cells, and, in the fasting organism, Table 2 Fuels of individual tissues [Modified from Krebs (45).] energyTissueGlucoseEryth Major source of rocytes, leukocytes, re nal medulla, brain, skeletal muscle (exercise), some malignant tumors, fetal tis mucosaFree fatty acids―Liver, sues, intestinal kidney cortex, cardiac muscle,skeletal muscle(ex exercise)Ketone bodies―Cardiac cept in severe muscle, renal cortex, brainOther skeletal muscle, sourcesAmino energy (minor)Lactate acids fromglucose)Ethanol, (derived glycerol, pen toses (minor) Table 1 Distribution of oxygen utilization aresting, among the major body organs in manFor healthy a 65-kg man [from Passmore (65)].Oxygen and Draper con sumption total)LiverOrgan 27splanchnic (including mm) 67 area)Brain 19Kidneys 47 7Heart 10Skeletal 18Remainder muscles 17 26 45 19Total 48 280 (ml/ Resting metabo lism (% of a These amounts sources can be used in quantitatively significant by tissues shown. Table 3 Glucose turnover and Con cycle activity in patients carcinoma Calculatedfrom data of Holrodye et al.(36).Status of body wt turn over rate cycle activity with metastatic glucose oxidation (mg/kg/ lossGlucose (mg/kg/hr)Con(mg/kg/hr)% turnoverGlucose hr)Progressive ±26@ None196 100 110@26b90 a Mean ± S.D. for 8 patients. S Mean ± S.D. for 6 patients. ±21 19±243 ±7 18±262 ±4 48±6 JULY 1977 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 1977 American Association for Cancer Research. 2337 V. R. Young phosphate are consumed for each mole of glucose pro duced from lactate (51), this would involve a substrate en ergy requirement of about 110 kcal. From the data provided by Holroyde et al. (36), it can be estimated that less than 10% of daily energy expenditure can be accounted for by the conventional cost of lactate recycling. Analyzing this problem from a somewhat different perspective, it can be estimated that, if 15% of total lactate production is oxidized to CO2and H2O,and 85% of lactate is converted to glucose, there will be a maintenance of high-energy phosphate bal ance. This assumes, of course, that lactate is the only metabolite being utilized (51). It is difficult to accept, there fore, that changes in Con cycle activity are a significant cause of the marked body wasting in patients with progres sive neoplasia. Nevertheless, it is of interest that Holroyd et al. (36) observed highest Con cycle activity in patients with greatest total energy expenditure. The pattern of fuel sources changes markedly if fasting continues significantly beyond the usual overnight period. For a fast lasting 3 days or longer, glucose oxidation is decreased, in parallel with reduced rates of gluconeogene sis (9, 64) and the oxidation of fatty acids and ketone bodies is increased, with the brain making major use of the latter as its principal fuel source (63). A picture of fuel utilization during short and long-term fasts is shown in Chart 1. This change in the pattern of fuel sources and utilization is accomplished by alterations in substrate availability, in hor monal balance, and by the regulatory effects of ketone bodies on amino acid oxidation in peripheral tissues (71). In terms of energy requirements, glucose and lipid sources are utilized with about the same efficiency, at least when assessed in terms of the potential yield of ATP (44) from isocaloric intakes of glucose and fat. Protein is some POSTABSORPTIVE BRIEF FAST (2-3 what less efficient as a source of energy, depending upon the amino acid composition of the protein and because energy is used for the elimination of nitrogen via urea syn thesis (44). It should be recognized, however, that an estimation of the availability.of utilizable energy from carbohydrate (glu cose) and lipid fuel sources, based on calculation of maxi mum ATP yield, may have limited significance in relation to an assessment of the status of energy metabolism and substrate utilization in the whole organism. Various factors serve to modify the yield of utilizable energy which may be derived from the combustion of these fuel sources. The importance of these factors may vary among individuals and within subjects due to changes in physiological and patho logical states (34). The efficiency of generation of ATP might vary due to changes in the coupling of oxidative phosphorylation, and the efficiency of utilization of ATP does not necessarily remain constant, due to factors such as tissue phosphatase activity and ion concentration. Furthermore, a variable ac tivity of “futile― cycles would result in changes in the amount of energy available for use in energy-requiring processes. These cycles occur when there are 2 opposing metabolic pathways in the cell in which the reactions in the forward and reverse directions are catalyzed by separate enzymes (40, 60). For example, 3 futile cycles in carbohy drate metaboli@mare shown in Chart 2. In one direction, the GLUCOKINASE GLUCOSE CYCLE AlP GLUCOSE ADP GLUCOSE 6P DAYS) GLUCOSE 6P PHOSPIIATASE PHOSPHOFRUCTOKINASE @ FRUCTOSE 6P FRUCTOSE 6P PROLONGED (_v GLUCOSE ,“ diP FAST FRUCTOSE %t-_..-J ‘•@),‘ KETONE FRUCTOSE BODIES •q diP PHOSPHATASE PEP CYCLE ‘ AMINO ACIDS Chart 1. Major patterns of fuel utilization in the postabsorptive state (overnight fast) and after short- and long-term fasts. Glucose utilization is high in the postabsorptive state with depletion of glycogen reserves and gluconeogenesis increasing during the short-term fast. Subsequently gluco neogenosis and flow of amino acids from muscle are reduced with a rise in blood ketone bodies and increased utilization by the brain. Thus, the quantitative contribution of the fuel sources to overall body energy metabo iism depends upon the nutritional state. This picture is based principally on work reviewed in Refs. 9, 63, 64, and 71. FFA, free fatty acids. 2338 ADP AP GOP ATP PEP DECREASED PYRUVATE PEP @“-GTP ADP.*―j PYRUVATE CARBOXYKINASE OAA CARBOXYLASE OAA (CYJ@)(,Mit) Chart 2. Three futile cycles in carbohydrate metabolism: the glucose 6phosphate (glucose 6F), fructose 6-phosphate (fructose 6P), and phospho enolpyruvate (PEP) cycles. The variable activity of these cycles, which do not involve a net change in the levels of reactants (e.g. , glucose, fructose 6phosphate or phosphoenolpyruvate), will result in changes in rates of ATP generation, relative to rates of ATP hydrolysis. Taken from Katz and Rogns tad (40). OAA, oxaloacotic acid; CYTO, cytoplasmic; MIT, mitochondrial. CANCERRESEARCHVOL. 37 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 1977 American Association for Cancer Research. Energy Requirements reaction requires the participation of a high-energy corn pound, such as ATP, while the reaction in the opposite direction is energetically spontaneous. Although there is no net flux of reactants in these cycles, the cycling causes ATP hydrolysis, and thus an energy ‘ ‘wastage.― However, the recycling may not be as wasteful as it appears, as pointed out by Katz and Rognstad (40), if these cycles serve a role in metabolic regulation. Although there are no adequate experimental data to estimate the fraction of total ATP formed and used in recy cling, a variation in the activity of futile cycles has been proposed as a basis for adaptation to high-energy intakes (74) and for differences in the propensity of individuals with generous energy intakes to become obese (39). Similarly, it can be speculated that the changes in the availability of to, the sodium pump is relatively small. Cell protein synthesis appears to be of quantitative sign if icance in relation to the utilization of energy substrates under basal conditions, and various observations may be used to support this concept. Thus, the relationship be tween the intensity of whole-body protein metabolism in mammalian species and adult body size is described by the same power of body weight as is basal energy metabolism among these species. Brody (7) showed that the variation in obligatory nitrogen losses, assumed to be an index of the dynamic state of body protein metabolism, among 9 mam malian species, ranging in size from the mouse to the cow, correlated with the 0.72 power of body weight, expressed in kg (Chart 3). This is essentially the same function of body weight that best correlates basal energy metabolism among ATP and in the efficiency of energy utilization might arise as these various species (43). More recently, Munro (58) re a consequence of changes in recycling in disease states viewed this aspect of body protein metabolism and corn and under the varying conditions of therapy. This problem puted the power function of body weight that best corre deserves investigation. lated various parameters of tissue and whole-body protein Another factor that must be mentioned is that, if glucose metabolism, including albumin and ceruloplasm turnover or other carbohydrate sources are converted first to fat for and liver RNA content, among mammals of different body the temporary storage of energy, before being used to meet size. The estimates of Munro (58), together with those of energy requirements, there is a reduction in the amount of Brody (7), demonstrate a close relationship between the utilizable energy obtained from the intake of a given amount intensity of body protein ‘r*ietabolismand rate of energy of carbohydrate. Krebs (45) estimated that this loss of utiliz expenditure in mammals, including man. Estimates of the rate of whole-body protein synthesis in able energy is equivalent to 2 molecules of ATP per C2 adult human subjects provide additional support for the segment of long-chain fatty acid or about 7% of the utiliza ble energy to be stored. Flatt (18) estimates the loss of view that protein turnover (synthesis and breakdown) ac counts for a significant proportion of basal energy expendi utilizable energy to be equivalent to about 20% of the ca ture. Table 4 summarizes some published estimates of rates loric value of the glucose channeled into lipogenic path ways, and this appears to be a significant energy cost. of whole-body protein synthesis in well-nourished adult subjects. Although the estimates vary, depending upon the Whatever the precise value, there is an energy cost associ ated with storage and the later utilization of fuels. Hence method used forthe determination (86), whole-body protein the efficiency of substrate utilization for meeting the basal synthesis approximates 3 to 4 g per kg body per day or 200 to 300 g for a 70-kg subject. Assuming each mole of peptide energy requirement will be determined, in part, by the meta bolic pathways followed before the fuel sources reach the bond requires the equivalent of about 5 moles of ATP and that ATP is formed from glucose at a cost of 18 kcal/mole terminal stage of oxidation. (44), it can be calculated that about 180 kcal of substrate would be required to support this amount of peptide bond Significance of Ion Pumping and Protein Turnover in En synthesis. This would be equivalent to about 10% of basal ergyExpenditure Two processes thought to account for a significant frac tion of the basal energy expenditure are ion pumping and protein turnover (synthesis and breakdown). The mainte nance of electrochemical gradients through the active transport of ions requires energy; it has been suggested that 40 and 52% of the in vitro aerobic energy expenditure of kidney cortex and brain slices, respectively, is linked to sodium-potassium pumping (91). Similarly, the transport of sodium and potassium in liver (15) and tumor cells (48) has been estimated to account for 35 and 85% of energy metab olism in these tissues, respectively. Support for the concept that ion pumping is an important component of basal en ergy metabolism is suggested from the increased metabolic rate in response to thyroid hormone and catecholamines which appears to be due to increased ATP utilization as a consequence of altered activity of sodiurn-potassium-ATP ase (35). However, Himms-Hagen (35) has concluded that, for most normal tissues, the proportion of total cell and organ energy metabolism controlled by, or directly related z z w 0 2 >--- — :@— I0,000 5,000 U) 0 z w 0 0 z w I ,000 500 I 00 50 Ql .0 10 00 500kg BODY WEIGHT (N) Chart 3. Schematic relationship between the obligatory urinary nitrogen loss (urine nitrogen output after initial adaptation to a very low or protein-free intake) and adult body size in mammalian species. As shown, the output of nitrogen is related to the 0.72 power of body weight (expressed in kg) suggesting, as discussed in the text, that nitrogen output or metabolism is closely correlated to energy metabolism. Drawn from the data of Brody (7). JULY 1977 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 1977 American Association for Cancer Research. 2339 V. R. Young energy expenditure. This estimate does not account for the energy costs of amino acid transport, RNA synthesis, turn over of the —CCAterminus of tRNA, synthesis of nonessen tial amino acids, and energy cost of protein breakdown. Furthermore, it is assumed that the oxidation of glucose results in the generation and availability of 36 moles ATP per mole glucose oxidized, but as discussed earlier, this maximum yield of ATP is subject to variation and in all likelihood it will be less. Millward et al. (54) have estimated the energy cost of protein synthesis to be about 1.4 kcal/g protein. On this basis, protein turnover in the adult subject would account for about 25% of the basal metabolic rate. These figures underestimate the quantitative contribution of protein synthesis and breakdown to basal energy metab olism. Thus, it is reasonable to assume that about one-half of resting energy metabolism may be associated with pro tein turnover. For this reason, it would be anticipated that the replenishment of tissue and organ protein content in the initially depleted patient would require an increased energy intake above that required for normal maintenance. Fur thermore, evidence indicating a high energy cost of growth in infants and children (47, 66) supports this view. Finally, resting energy metabolism per unit of body weight declines with progressive growth and development within a mammalian species (43). This fall parallels the reduced intensity of whole-body protein synthesis during this period (e.g., Ref. 88). We (95) have explored the rela tionship between whole-body protein synthesis rates and energy metabolism in human subjects at various ages, and the results of these studies are shown in Table 5. It can be seen that there are marked differences in the intensity of whole-body protein synthesis, expressed per unit of body weight, among the various age groups. However, these differences are not as evident for whole-body protein syn thesis expressed per unit of resting energy metabolism. These observations emphasize further the close and, pre sumably, causal relationship between whole-body protein turnover and resting energy metabolism. Changes in host tissue and total-body protein metabolism due to the presence of a growing tumor (26), physical trauma (19), and surgery (62) and alterationsthat may occur as a result of chemotherapy and radiation treatment would influence also the utilization and requirements for energy. Thus, a critical assessment of energy utilization and re quirements in the cancer patient should take into account these intimate interrelationships energy metabolism. among body protein and Factors Affecting BMR Age, nutritional status, temperature, hormones, and pathologicalstates,includingtrauma and infection, affect the resting metabolic rate. The effects of age have been discussed by others (43, 66, 72). Also, changes in deep body temperature are well established (20). If body temperature is raised by 1°,either by fever or by warming the body, the metabolic rate increases by about 12%. The effect of nutritional state is important in the context of energy metabolism, particularly because body nutrient depletion is common in cancer patients. The effects of starvation and undernutrition on basal metabolism have received considerable investigation, and this has been the topic of several reviews (20, 30, 42, 87). Brief fasting does not change total-body oxygen consumption and, thus, heat production, but a longer period of restricted food intake does influence whole-body energy expenditure (31). Chart 4 summarizes results, discussed previously by Oar row (20), of a study by Benedict et al. (2). The major findings of this study are shown here to emphasize a number of points that should be considered in evaluating results of studies of energy metabolism in cancer patients. First, it can be seen that undernutrition reduces BMR to a greater extent than the effect on body weight. Thus, the fall in BMR, under these conditions is due to changes in the metabolic activity of tissue as well as a loss of active tissue mass. On the basis of studies during acute starvation, Grande et a!. inpremature Total daily protein synthesis Table 5 in relation to energy metabolism womenSummarized babies, infants, young male adults, and elderly fromPicou from Young et al. (94). Studies with infants and Taylor-Roberts (67).Total synthesisg/kg/Group g/kcalNewborn body protein Age 0.09Infant day 1-46 days 7Young 0.01Elderly adult 18 0.15 ± 10-20 mos. 20-23 yr 3 0.1 1 ± 69-91 yr 2 0.11 ±0.03 Table 4 Some estimates of the mean rate of whole-body protein synthesis in adult subjects, determined by constant infusion Subjects Author(s)3 No. and sex M Label protein syn thesis (g/kg/ day) 19-50 L-[U-'4CjLysine 2.6 Waterlow (85) 3 M, 1 F― 6 M 5 M 52-75 31-64 31-46 L-[1-14C]Leucine L-[U-14C]Tyrosine L-[a-15N]Lysine 4.1 4.6 3.5 O'Keefe et al. (62) James et al. (38) Halliday and Mc 4 M, 2 F 20-25 [15N]Glycine 3.0 Keran (33) Steffeeet a!. (75) a Preoperative 2340 Age (yr) of labeled acidWhole-body amino patients. Other studies involved healthy subjects. CANCERRESEARCHVOL. 37 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 1977 American Association for Cancer Research. Energy Requirements CHRISTMAS THANKSGIVING 0 I7OO@ 0 U z 0 I600@ IU I 500 P S a. I4 Ui I -i 4 I40O@ U) 4 I300[ @i : @ SEPT OCT NOV DEC JAN FEB 27 27 26 26 25 24 Chart 4. Changes in basal heat production and body weight in 7 healthy subjects studied for the effects of a restricted energy intake. Taken from Benedict et al. (2). The dietary restriction began on October 4, 1917, and finished on February, 3, 1918, but it was interrupted with a free-choice diet between November 29 to December 2, inclusive, and December 20 to January 6, inclusive. refeeding than during initial adaptation to a fast in a healthy subject. In addition to undernutrition, the effects of excessive energy intakes on energy expenditure and BMR have been reviewed recently by others (20, 52, 74). Overfeeding of normal subjects does not always result in the expected weight gain despite unaltered physical activity. Various studies indicate that, over a period of excess energy intake, there is an increase in oxygen consumption in the resting state and that this thermogenic effect of high energy intakes is greater during exercise (52, 74). From these various observations it is difficult to general ize about the effect of nutritional state on basal metabolism. It will depend upon when it is measured, how it is calcu lated, and current as well as previous nutritional history. These points should be kept in mind in the critical evalua tion of energy metabolism in cancer patients. Physical trauma, e.g., due to burns or leg fracture, alters the basal metabolic rate, the degree of change depending upon the severity of trauma (92). The hypermetabolism may cause a marked weight loss if it is not met by substantial increases in energy intake, and Wilmore et al. (93) have proposed that the calorigenic action of catecholamines is the cause of the increased metabolic rate. However, the mechanism of increased heat production in burned patients requires further exploration, and accelerated rates of gluco neogenesis and ureagenesis would account, in part, for this increase in metabolic rate (92). Furthermore, it seems likely that an increased rate of whole-body protein turnover is an important factor. Recent studies (C. L. Kien, J. F. Burke, and V. R. Young, unpublished results) summarized in Table 7, on the effects of thermal injury, have shown that the rates of whole-body protein synthesis and breakdown are higher in children with larger burns. This higher rate correlates with Table6 (31) suggested that the loss of tissue accounts for about 30% of the decrease in metabolism. On the other hand, in long-term undernutrition, the loss of tissue is a major factor determining the reduction in energy expenditure (20). The results shown in Chart 4 also indicate that basal metabolism is rapidly restored to normal levels upon refeed ing. In this case, BMR, expressed per unit of body weight, increases to greater than normal during early refeeding. An increased rate of energy expenditure also occurs after meals in children during early recovery from severe protein calorie malnutrition (1, 8, 46). Brooke and Ashworth (8) propose that this increased energy expenditure with refeed ing is due to the increased rate of protein synthesis which would involve an increased rate of ATP generation and utilization. Of additional interest is that the fall in BMR with continued fasting in obese subjects (5) also appears to be ‘. related constant to a fall [‘5N]glycine in whole-body infusion protein model, synthesis. we (J. Using C. a Changesin breakdownin rates of whole-bodyprotein synthesis and fastFrom 5 moderately obese women after a 1-weektotal V.R. unpublished resultsofJ. C. Winterer, B. R. Bistrian, and withthe Young. Estimatesof protein synthesisand breakdownmade useof the [15N]glycine (67).Protein model of Picou and Taylor-Roberts synthesis (g/kg/day)Control Diet period 1.8Fast 1.8% Protein break down 1 .9 1.4― change a Different (g/ kg/day) —26 from control 0 (p < 0.05). Table7 Effect of extent of synthesisand thermal injury on whole-body protein childrenUnpublishedbreakdown rates in Young.Burn results of C. L. Kien, J. F. Burke, and V. R. controlswere patients ranged in age from 5 to 12years; unburned ages 4 to 18 years.Whole-body Winterer, B. R. Bistrian and V. R. Young, unpublished results) have observed that there is a significant decrease in the overall body protein synthesis rate during a week-long fast in obese women (Table 6). Finally, the results of Benedict et al. (2) suggest that BMR falls more rapidly with fasting after a period of temporary protein Burn size (% surface Breakdown0 area) 3.10.5-25 3.325-60 3.960 No. of obser vations (g/kg/day) Synthesis 11 4 10 3.5 4.0 5.2 10 7.1 6.3 JULY 1977 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 1977 American Association for Cancer Research. 2341 @ —@ V. R. Young the increased basal metabolic rate and energy expenditurefree fatty acid oxidation, as well as carbon dioxide produc which occur in extensive body burns (92).tion, in 5 patients with metastatic malignant disease; stud It must be concluded, therefore, that the basal metabolicies andrate were conducted in patients under basal conditions changes in response to various physiological and path areological during glucose loading. The results of their studies conditions. This makes it difficult to evaluate fullyshown ofthe in Charts 5 and 6. Under basal conditions, rates limited published data obtained in studies of energyglucose andmetabolism and free fatty acid ([1-'4Cjpalmitate) oxidation, in patients with malignant disease, and to de betweentermine total CO2 production did not differ substantially whether cancer has a direct influence on energycancer glucosemetabolism patients and controls. However, when a and, particularly, on energy requirements.load was given, these investigators observed that the oxida patientsResting tion of free fatty acid was suppressed less in cancer that there was a lower rate of ‘ ‘slow― oxidation of Metabolism in Cancer Patientsand 5).In glucose, compared with controls (Chart of the contribution to CO2 production by Table 8, a summary is made of some results of studies nonprotein sources, unlabeled by the administered on the basal metabolic rate in patients with cancer. In view [14C]glucose and [14C)palmitate, indicated that glucose of the various factors that affect metabolic rate, and , in part, loading reduced their oxidation in normal subjects but not because of the limited information supplied in many of the in cancer patients (Chart 6). Waterhouse and Kemperman papers, it cannot be concluded that resting metabolism is (83) interpret this finding to mean that continued intracellu consistently increased in the cancer patient, compared with loading.increased lar oxidation of free fatty acids occurs with glucose healthy controls. Resting energy metabolism appears to beCalculation in many patients with Hodgkin's disease or leuke GLUCOSEPOOL(“aol,/kglNORMAL GLUCOSE OXIDATION FFA OXIDATION BMR'samong mia. There is considerable variation in reported presumably@NCERreflects and within the various studies. This +6 differences in methodological and biological varia bles, as well as possible effects of different cancers and +6 06 severity and stage of disease. In a study of the partition of +6 energy expenditure between host and tumor in tumor-bear I ing rats, Morrison (56) did not find evidence of a consistent change in resting metabolism. Iaaol,/Rg/h,I NORMAL RAPID - @ @ Response of Energy Metabolism to Dietary Intake In the Cancer Patient CANCER SLOW +6 0.5 - 02healthy II fi Potentially of greater nutritional significance is the possi bility that the response of the cancer patient to semistarva tion or nutritional rehabilitation may differ from that of.4 5. Estimates of glucose pool and rates of glucose (“rapid― and subjects or from patients suffering from nonmalig “slow― pools) and free fatty acid (FFA) oxidation in normal and cancer nant diseases. Waterhouse and Kemperman (83) have ex patients studied under basal conditions and during a glucose load (+G). amined this possibility by determining rates of glucose andChart Drawn from tabular data of Waterhouse and Kemperman (83). Table 8 A listing of some published results on thebasal metabolic rate of cancer patientsDescription of popu lationBMRCommentAuthor(s)Leukemia, 16 casesUsually (3)Chronic (89)leukemia, myelocyticLow, >120% detailsBoothby and Sandi ford normalFew normal,Watkin casesincreasedMalignant 4 (82)5 disease,—10% aboveWaterhouse casesnormalMultiple myeloma—14-60% (73)Carcinoma, detailsSilver et a!. (73)izednormalLeukemia, local —6-57%aboveFew detailsSilver et al. (73)and myeloid—12-91% lymphaticnormalMalignant detailsSilver et al. above normalFew (84)plasms, neo 0-30% aboveFew Steinfield4 disease,Low et al. aboveWaterhouse casesnormalLeukemiaIncreasedFew 4 (55)Neoplastic and aboveWatkin detailsMinot and Means and casesnormal(90)Various cancers, 9Usually casesnormalhouse 2342 aboveTerpeka and Water (76) CANCERRESEARCHVOL. 37 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 1977 American Association for Cancer Research. Energy Requirements This suggests that there is a disturbance in normal homeo static mechanisms involving the utilization of glucose and other important fuel sources in patients with malignant disease. In this context, changes in hormonal balance may be of significance, and Goodlad et a!. (28) found reduced insulin production in tumor-bearing male rats. Thus, an alteration in insulin function might account for the abnor mal glucose regulation. The nutritional implications of these findings are more difficult to assess. If glucose is not oxidized directly but is first converted to fat before supplying utilizable energy, this would involve an energy cost and, thus, a relatively higher energy intake to meet the needs of body tissues. Whether gluconeogenesis is inhibited by exogenous glu cose as effectively in the cancerous as in the normal patient does not appear to have received critical investigation. However, sepsis increases gluconeogenesis, and this path , TOTAL —UNLABE LE GLUCOSE RAPID COD PRODUCTION Im moIR/kg/h,I NORMAL CANCER NORMAL NON SLOW CANCER way is not responsive to the administration of glucose dur ing the stress of infection (32). Thus, of possible interest in relation to metabolic regulation by exogenous substrate is the observation that treatment of rats with hepatocarcino gens results in a loss of dietary feedback control of choles terol biosynthesis (70). Additional studies would be desira ble to explore the regulation of carbohydrate and lipid me tabolism and the dynamic interrelationships between glu cose, lipid, and amino acid metabolism in cancer patients. Several investigators (12, 84, 89, 90) have stated that the level of energy intakes needed to maintain body energy balance are higher for cancer patients than for other sub jects. Thus Waterhouse et a!. (84) determined energy bal ance, using the indirect method of Newburgh etal. (59) in a group of 4 patients with leukemia, Hodgkin's disease, and carcinoma of the pancreas. The results obtained with 2 of these patients are summarized in Chart 7, and it may be seen for 1 patient that, even at a liberal energy intake, body energy balance was markedly negative throughout. This implies that, in some but not all cancer patients, dietary energy sources are utilized with relatively low efficiency. However, it must be recognized that the precision of the estimates of energy balance made by Waterhouse et al. (84) is not known and that accurate determinations of energy balance are difficult to undertake. The magnitude of the error in energy balance which could lead to marked body weight loss is quite small compared with the range of en ergy intakes and requirements within a group of subjects (20). Furthermore, Garrow (20) concluded from his review of the literature that rarely is energy balance established over a period of a week or even longer periods in normal subjects, and that an energy imbalance of up to 60,000 kcal is tolerated by the control system in many people. It is not surprising that little is known about the quantitative effects of cancer on energy utilization and body energy balance in human subjects. As reviewed above, continued weight loss and clinical deterioration have been observed in some patients, even when given generous energy and protein intakes. However, the effects of the cancer or treatment conditions may not be NORMAL CANCER - PROTEIN NORMAL CANCER +6 +6 4@G 30 +6 / 2.0 - .0 Ti ‘:___ n Chart 6. Total carbon dioxide production and the contributions from oxi dation of labeled glucose and fatty acids and from unlabeled nonprotein sources in normal subjects and in cancer patients studied under basal conditions and during a glucose load (+G). Drawn from tabular data of Waterhouse and Kemperman (83). CALORIE (Kcols INTAKE @IO'@/6days) M.J. (HODGKINS DISEASE) J. F(ACUTE 15S 14.2 4.2 7.1 14.2 I U Ill iz 6.2 67 S III 6.7 19.5 LEUKEMIA) 14.2 4 a ‘O (0 I,, Chart 7. Estimated body energy bal ance in relation to energy intake during consecutive 6-day experimental periods in 2 cancerpatients.Drawnfromtabulardata of Waterhouse et al. (84). 0 -2 N N, 0 U -4 -6 Ui U 2 -8 4 4 @1 Ui ‘10 12 0 @.1 4 I @Z U @ JULY 1977 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 1977 American Association for Cancer Research. 2343 V. R. Young exerted directly on the yield or availability of utilizable en ergy from energy sources. Changes in energy balance or in the capacity to achieve body energy equilibrium may be secondary to alterations in the status of protein metabolism in body tissues. @ @ Goodlad et a!. (27-29) and Clark and Goodlad (11) have shown that myofibrillar protein synthesis in skeletal muscle of tumor-bearing rats is reduced and they (11) have con cluded that this impairment is due to a defect in the capacity of the 40 S ribosome subunit to promote a postinitiation step in polypeptide synthesis. Lundholm et a!. (50) have examined in vitro protein synthesis in muscle biopsies ob tamed from a heterogeneous group of cancer patients, and the results of these studies are shown in Chart 8. Protein synthetic activity was impaired and the rate of protein breakdown was increased in muscle samples from cancer patients, compared with metabolically healthy controls. However, Lundholm et al. (50) also observed that protein synthesis in muscle from cancer patients, as well as normal subjects, could be stimulated by the addition of high levels of amino acids to the incubation medium (Chart 8). This suggests that in the cancer patient there is a reduced effi ciency of amino acid utilization for muscle protein synthesis at normal levels of amino acid supply, but that this may be overcome by raising the supply of amino acids to muscle. The favorable gains in body weight and nitrogen retention, as well as reduced morbidity and mortality, achieved by i.v. feeding of cancer patients ( e.g., Ref. 13), support this conclusion. Energy Requirements of the Cancer Patient Partly because the effects of cancer on host tissue and whole-body energy metabolism are only partially under stood, it is not possible to be precise about the minimum intake of energy which would be sufficient to meet energy needs and maintain body energy balance in cancer patients. Furthermore, the balance between major exogenous energy SYNTHESIS DEGRADATION P < 0.025 150 U) -I 0 I-@ WITH @ AMINO U ACID SUPPLEMENTATION z — U :, n.s. 100 @ - P<0.05 > @@uUL Chart 8. Rates of in vitro protein synthesis and degradation by muscle fibers from cancer patients, in relation to normal subjects. The relative response of protein synthesis in vitro to high levels of amino acid supplemen tation (10 times normal plasma levels) obtained with muscle samples from cancer patients and control subjects is also shown. Drawn from results of Lundholm 2344 et al. (50). 0 - @0 — z 20 - Ui U -I0 -I 4 z MEAN ENERGY -20 REQUIRE MENT Ui (9 0 -30 - z 0.5 .0 CALORIE S DELIVE RED BASAL ENERGY 1.5 20 EXPENDITURE Chart 9. Schematic depiction of results of Rutten et al. (69) showing relationship between energy intake (expressed as a fraction of calculated basal energy expenditure) and changes in body nitrogen balance in 13 postoperative patients, including a total of 4 patients with cancer of the lung. bladder, esophagus, and uterus. sources, glucose or other carbohydrates, and lipid, which would promote maximum efficiency of energy utilization, cannot be stated yet. There are no more than a few studies that help to provide only crude guidelines for this purpose. Rutten @t a!. (69) have shown in a group of postsurgical patients, including some with cancer, that hyperalimenta tion with a fluid providing 160 kcal/g nitrogen could support body nitrogen balance when total energy intake approxi mated 1.7 to 2.0 times the calculated basal metabolic rate (Chart 9). Similarly, at nitrogen intakes of 240 mg nitrogen per kg per day, or more than twice the nitrogen allowance for healthy adults (16), Long et al. (49) concluded that energy balance was achieved in a group of septic patients, including 2 with cancer of the bladder, with energy intake being about 1.5 times basal energy expenditure. The studies of Rutten et a!. (69) and Long et al. (49) provide only a partial basis for assessing the adequacy of levels of energy intake, and studies of this kind should be extended , particularly in view of the close interrelationships between energy and protein in nutrition and metabolism. We (22, 23) and others (10, 37) have explored the sensitivity of body nitrogen balance to changes in energy intake in healthy subjects. In these studies it was shown that gener ous intakes of energy result in a sustained increase in nitrogen retention and dietary nitrogen utilization. How ever, the effects of changes in the level of energy intake on protein and energy utilization may be modified by the level of protein intake (57). Hence, the definition of an adequate energy intake for the nutritional therapy of the cancer pa tient is dependent upon a variety of dietary and host factors. These factors, together, will determine the appropriate en ergy intake for the individual patient. Finally, the attending physician and hospital dietitian have little useful informa tion to follow in deciding on the level and sources of energy to provide a particular patient and they must rely upon the clinical progress of the patient, supplemented with some objective biochemical and physiological assessment of the patient's nutritional state. Better knowledge of the interrelationships among energy CANCERRESEARCHVOL. 37 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 1977 American Association for Cancer Research. Energy Requirements and protein metabolism clearly would help to develop better diagnostic aids for the evaluation of nutritional status and lead to the design of improved nutritional therapies for treatment of cancer patients. In addition, this information is necessary for an understanding of the anorexia that is re garded as a major contributory factor to body energy loss and the eventual cachexia in cancer patients (77). Ob viously, energy balance will not be achieved if intake and absorption fail to meet the energy demands of the body. Alterations in intestinal function due to alimentary tract neoplasms or the effects of surgery, chemotherapeutic agents, and radiation may affect energy metabolism by changing the digestive-absorptive phase of nutrient utiliza tion. This topic is discussed elsewhere in this symposium. The regulation of energy intake in normal and cancer patients is beyond the scope of this paper, and the reader is referred to reviews which have discussed this aspect of energy metabolism in normal subjects (e.g., Ref. 61) and in relation to cancer (78). Of particular interest, however, is a review by Bray and Campfield (6) which considers the var might offer an approach to testing hypotheses proposed to explain the actual or relative reduction in food intake and development of negative energy balance which occurs dur ing the onset and development of neoplasia. Of significance in the present context is that the model involves considera tions of important energy-yielding substrates, glucose, and fatty acids, and of the amino acid levels in blood plasma. Changes in glucose, fatty acid metabolism, and in amino acid and protein metabolism in cancer patients have been discussed above. Furthermore, differences in blood amino acid levels of cancer patients, compared with controls, have been described (e.g., Refs. 4, 41). An adequate exploration of energy metabolism and nutri tion should, for these reasons alone, include as many ob servations as possible within a single patient, on the utiliza tion and metabolism of the principal fuel sources (carbohy drate, lipids, and protein). There is also a great need to apply and improve upon modern methods for measurement of whole-body energy expenditure in human subjects in gen eral and in patients with malignant disease in particular. ious metabolic factorsinvolvedin the regulationof food intake. These investigators proposed that body energy stores are the regulated variable and that energy intake or expenditure is altered to maintain a particular level of total caloric storage. The major features of the control system discussed by Bray and Campfield are given in Chart 10. As seen from this chart, the plasma concentrations of amino acids, glucose, glycerol, and free fatty acids, as well as the state of peripheral metabolism, including the quantity of adipose tissue, glycogen, and protein, serve as feedback signals on the ventromedial nucleus, which is assumed to be the long-term monitor of energy balance in the body. This model was proposed to provide a possible framework which might help identify possible changes of system error in relation to obesity, or body energy excess. Similarly, it Conclusion Based on the above, it is clear that various factors affect basal and total daily energy expenditure. This makes it difficult to assess the significance of published data on basal metabolism in cancer patients. Also, there are signifi cant quantitative relationships between whole-body energy and protein metabolism, and these must be considered in assessing energy status and requirements in cancer pa tients who may often be depleted of body protein and re quire vigorous nutritional support to reverse this state and to maintain adequate nutritional status. Although the lim ited data available suggest that the pattern of fuel utilization CONTROLLER I. NEURAL COR T E X SUBCORT ICAL AUTONOMIC NERVOUS SYSTEM CONTROLLER 2. GASTROINTESTINAL STOMACH INTESTINAL CALORIE SYSTEM STORAGE STORED @IEDISTRIBUTION MUCOSA CALORIES 3. HUMORAL CALORIE DISPOSAL PANCREAS P I T U I TA R Y ADRENAL GONAD PLASMA GLUCOSE PLASMA FREE FATTY ACIDS PLASMA GLYCEROL PLASMA AMINO ACIDS PERIPHERAL METABOLIC FEEDBACK STATE ELEMENTS Chart 10. Simplified elements of the system responsible for regulation of body energy stores in human subjects, as proposed by Bray and Campfieid (6). The model consists of a controller, acting upon the controlled system, with effectors including plasma glucose, amino acids, fatty acids, and status of metabolism in peripheral tissues. JULY 1977 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 1977 American Association for Cancer Research. 2345 V. R. Young in neoplastic disease states may differ from that of healthy subjects, with lipid sources predominating, an altered regu lation of glucose metabolism, and less efficient utilization of food energy, further studies are needed to verify and estab lish the nutritional and metabolic significance of this obser vation. Whether particular cancers, other than those di rectly involving the neuroendocrine system, affect energy metabolism and requirements in different ways cannot be determined from the available literature, nor is the role of severity of the disease state, in this regard, adequately understood . Only crude guidelines can be suggested for the levels of energy intake and optimum relationship between protein and energy requirements for the feeding of cancer patients. A better understanding of the characteristics of the utilization and metabolism of the major fuel sources in cancer patients should lead to improved diagnostic tests for assessing body energy balance and needs during the var ious phases of the disease and under the differing condi tions of therapy. In part, this will require much better infor mation on the regulation of energy metabolism and utiliza tion of energy sources at the whole-body level in healthy subjects. References 1. Ashworth, 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. A. Metabolic Rates during Recovery from Protein-Calorie Malnutrition: The Need for a New Concept of Specific Dynamic Action. Nature, 223: 407-409, 1969. Benedict, F. G., Miles, W. R., Roth, P., and Smith, H. M. Human Vitality and Efficiency under Prolonged Restricted Diet. Publication No. 280, p. 701. Washington, D. C.: Carnegie Institute of Washington, 1919. Boothbay, W. M., and Sandiford, I. Summary of the Basal Metabolism Data on 8,614 Subjects with Especial Reference to the Normal Standards for the Estimation of the Basal Metabolic Rate. J. Biol. Chem. , 54: 783803, 1922. Brackenridge, C. J. The Tyrosine and Tryptophan Content of Blood Serum in Malignant Disease. Clin. Chim. Acta, 5: 539-543, 1960. Bray, G. A. Effect of Calorie Restriction on Energy Expenditure in Obese Patients. Lancet, 2: 397-398, 1969. Bray, G. A., and Campfield, L. A. Metabolic Factors in the Control of Energy Stores. Metabolism, 24: 99-117, 1975. Brody, S. Bioenergetics and Growth. New York: Reinhold Publishing Co., 1945. Brooke, 0. G., and Ashworth, A. The Influence of Malnutrition on the Post-prandial Metabolic Rate and Respiratory Quotient. Brit. J. Nutr., 27: 20. Garrow, J. S. Energy Balance and Obesity in Man. Amsterdam, The Netherlands: North-Holland Publishing Co., 1974. 21. Garrow, J. S., Smith, R., and Ward, E. E. Electrolyte Metabolism In Severe Malnutrition, p. 168. New York: Pergamon Press, 1968. 22. Garza, C., Scrimshaw, N. S., and Young, V. R. Human Protein Require ments: The Effect of Variations in Energy Intake within the Maintenance Range. Am. J. Clin. Nutr., 29: 280-287, 1976. 23. Garza, C., Scrimshaw, N. 5., and Young, V. R. Human Protein Require ments. Evaluation of the 1973 FAO/WHO Safe Level of Protein Intake for Young Men at High Energy Intakes. Brit. J. Nutr. , In press. 24. Gold, J. Metabolic Profiles in Human Solid Tumors. I. A New Technique for the Utilization of Human Solid Tumors in Cancer Research and Its Application to the Anaerobic Glycolysis of Isologous Benign and Malig nant Colon Tissues. Cancer Res., 26: 695-705, 1966. 25. Gold, J. Cancer Cachexia and Gluconeogenesis. Ann. N. Y. Acad. Sci., 230: 103-110,1974. 26. Goodlad, G. A. J. Protein Metabolism and Tumor Growth. In: H. N. Munro (ed), Mammalian Protein Metabolism, Vol. 3, Chap. 20, pp. 415444. New York: Academic Press, Inc., 1969. 27. Goodlad, G. A. J., and Clark, C. M. Activity of Gastrocnemius and Soleus Polyribosomes in Rats Bearing the Walker 256 Carcinoma. European J. Cancer, 8: 647-651 , 1972. 28. Goodlad, G. A. J., Mitchell, A. J. H., McPhail, L., and Clark, C. M. Serum Insulin and Somatomedin Levels in the Tumor-bearing Rat. European J. Cancer, 11: 733-737, 1975. 29. Goodlad, G. A. J. . and Raymond, M. J. The Action of the Walker 256 Carcinoma and Toxohormone Incorporation into Diaphragm Protein. European J. Cancer, 9: 139-145, 1973. 30. Grande, F. Man under Caloric Deficiency. In: Handbook of Physiology: Adaptation to the Environment. Sect. 4, Vol. 1, Chap. 59, pp. 911-937. Washington, D. C.: American Physiological Society, 1964. 31. Grande, F., Anderson, J. T. , and Keys, A. Changes of Basal Metabolic Rate in Semistarvation and Refeeding. J. Appi. Physiol., 12: 230-238, 1958. 32. Gump, F. E., Long, C. L.. Geiger, J. W., and Kinney, J. M. The Signifi cance of Altered Gluconeogenesis in Surgical Catabolism. J. Trauma, 15: 704-710, 1975. 33. Halliday, D., and McKeran, A. 0. Measurement of Muscle Protein Syn thetic Role from Serial Muscle Biopsies and Total Body Protein Turnover in Man by Continuous Intravenous Infusion of L-[a-'NjLysine. Clin. Sd., 49: 581-590,1975. 34. Hegsted, D. M. Energy Needs and Energy Utilization. Nutr. Reviews, 32: 33-38, 1974. 35. Himms-Hagen, J. Cellular Thermogenesis. Ann. Rev. Physiol., 38: 315351, 1976. 36. Holroyde, C. P., Gabuzda, T. 6., Putnam, R. C., Paul, P., and Reichard, G. A. AlteredGlucoseMetabolismin MetastaticCarcinoma.cancer Res., 35: 3710-3714, 1975. 37. lnoue, G., Fujita, Y. , and Niiyama, V. Studies on Protein Requirements of Young Men Fed Egg Protein and Rice Protein with Excess and Mainte nance Energy Intakes. J. Nutr. , 103: 1673—1687, 1973. 38. James, W. P. T., Garlick, P. J., Sender, P. M., and Waterlow, J. C. Studies of Amino Acid and Protein Metabolism in Normal Man with L(U―C)TyrOsifle.Clin. Sci., 50: 525-532, 1976. 39. James, W. P. T., and Trayhern, P. An Integrated View of the Metabolic 407-415, 1972. and Genetic Basis for Obesity. Lancet, 2: 770-773, 1976. Cahill, G. F., Jr. Starvation in Man. New Engi. J. Med., 282: 668—675, 40. Katz, J., and Rognstad, R. Futile Cycles in the Metabolism of Glucose. 1970. Current Topics Cellular Regulation, 10: 237-289, 1976. Calloway, D. H. Nitrogen Balance of Men with Marginal Intakes of Pro tein and Energy. J. Nutr., 105: 914-923, 1975. in Leukemic Blood. Blood, 12: 635—643, 1957. Clark, C. M., and Goodlad, G. A. J. Muscle Protein Biosynthesis in the 42. Keys, A., Brozek, J,, Henschel, A., Mickelsen, 0., and Taylor, H. L. Basal Metabolism. In: The Biology of Human Starvation. Vol. 1, Chap. 17, pp. Tumor-bearing Rat. A Defect in the Post-initiation Stage of Translation. Biochem. Biophys. Acta, 378: 230-240, 1975. 303-339. Minneapolis: University of Minnesota Press, 1950. 43, Kleiber, M. The Fire of Life. New York: John Wiley & Sons, 1961. Copeland, E. M., Macfayden, B. V., and Dudrick, S. J. Intravenous Hyperalimentation in Cancer Patients. J. Surg. Res., 16: 241-247, 1974. 44. Krebs, H. A. The Metabolic Fate of Amino Acids. In: H. N. Munro and J. Copeiand, E. M., Macfayden, B. V., Lanzolti, V. J. , and Dudrick, S. J. B. Allison (eds.), Mammalian Protein Metabolism, Vol. 1, Chap. 5, pp. Intravenous Hyperalimentation as an Adjunct to Cancer Chemotherapy. 125-176. New York: Academic Press, Inc., 1964. 45. Krebs, H. A. Some Aspects of the Regulation of Fuel Supply in Omnivo Am. J. Surg., 129: 167-173, 1975. rous Animals. Advan. Enzyme Regulation, 10: 397-420, 1972. Durnin, J. V. G. A., and Passmore, R. Energy, Work and Leisure. Lon don: Heinemann Publishing Co., 1967. 46. Kreiger, I. The Energy Metabolism in Infants with Growth Failure Due to Elshove, A., and van Rossum, G. 0. V. Net Movements of Sodium and Maternal Deprivation, Undernutrition and Causes Unknown. Metabolic Potassium, and Their Relation to Respiration, in Slices of Rat Liver Rate Calculated from Insensible Loss of Weight. Pediatrics, 38: 63-76, Incubated in vitro. J. Physiol., 168: 531-553, 1963. 1966. FAO/WHO. Protein and Energy Requirements. Report of an Ad Hoc 47. Krieger, I., and Chen, Y. C. Calorie Requirements for Weight Gain in Expert Committee. World Health Organization Technical Report Series Infants with Growth Failure due to Maternal Deprivation, Under-nutri No. 522. Geneva, Switzerland: World Health Organization, 1973. tion, and Congenital Heart Disease—ACorrelation Analysis. Pediatrics, 44: 647-654, 1969. Fenninger, L. D., and Mider, G. B. Energy and Nitrogen Metabolism in 48. Levinson, C., and Hempling, H. G. The Role of Ion Transport in the Cancer. Advan. Cancer Res., 2: 229—252, 1954. Flatt, J. P., 1976. Personal communication, cited by Sims, E. A. H. See Regulation of Respiration in the Ehrlich Mouse Ascites-Tumor Cell. Ref. 74. Biochim. Biophys. Acta, 135: 306—318, 1967. 49. Long, C. L. , Crosby, F., Geiger, J. W., and Kinney, J. M. Parenteral Fleck, A. Protein Metabolism after Injury. Proc. Nutr. Soc. EngI. Scot., Nutrition in the Septic Patient; Nitrogen Balance, Limiting Plasma Amino 30: 152-157,1971. 2346 41 . Kelley, J.J.,and Waisman, H.A.Quantitative Plasma Amino Acid Values CANCERRESEARCHVOL. 37 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 1977 American Association for Cancer Research. Energy Requirements Acids and Calorie to Nitrogen Ratios. Am. J. Clin, Nutr., 29: 380-391, 1976. 50.Lundholm, K.,Bylund, A.C.,Hoim,J.,andScherstén, T.Skeletal Muscle 51, 52. 53. 54. 55. 56. 57. 58. 59. 60. Metabolism in Patients with Malignant Tumor. European J. Cancer, 12: 465—473, 1976. McGilvery, R. W. In: Biochemistry, a Functional Approach, pp. 280-281. Philadelphia: W. B. Saunders Co., 1970. Miller, D. S., and Mumford, P. An Experimental Study of Overeating Low and High-Protein Diets. Am. J. Clin. Nutr., 20: 1212—1222, 1967. Miller, S. Protein Metabolism during Growth and Development. In: H. N. Munro (ed), Mammalian Protein Metabolism Chap. 26, pp. 183-233. New York: Academic Press, Inc., 1969. Millward, D. J., Garlick, P. J. , James, W. P. T., Sender, P. M., and Waterlow, J. C. Protein Turnover. In: D. J. A. Cole, K. N. Boorman, P. J. Buttery, D. Lewis, R. J. Neele, and H. Swan (eds.), Protein Metabolism and Nutrition, pp. 49-69. London: Butterworth & Co. , Ltd., 1976. Minot, G. R., and Means, J. H. The Metabolism-Pulse Ratio in Exophthal mic Goiter and Leukemia. Arch. Internal Med., 32: 576-580, 1924. Morrison, S. D. Partition of Energy Expenditure between Host and Tu mor. Cancer Res., 31: 98—107, 1971. Munro, H. N. General Aspects of the Regulation of Protein Metabolism by Diet and Hormones, In: H. N. Munro and J. B. Allison (eds.), Mamma han Protein Metabolism, Vol. 1, Chapt. 10, pp. 381-481 . New York: Academic Press, Inc., 1969. Munro, H. N. Evolution of Protein Metabolism in Mammals. In: H. N. Munro (ed), Mammalian Protein Metabolism, Vol. 3, Chap. 25, pp. 133182. New York: Academic Press, Inc., 1969. Newburgh, L. H., Johnston, M. W.. Lashmet, F. H., and Sheldon, J. M, Further Experiences with the Measurement of Heat Production from Insensible Loss of Weight. J. Nutr., 13: 203-221 . 1937. Newsholme, E. A,, and Start, C. Regulation in Metabolism. New York: J. Wiley & Sons, Inc.,1973. 61. Novik, D., Wyrwicka, W., and Bray, G. A. (eds.). Hunger: Basic Mechanisms and Clinical Implications. New York: Raven Press, 1976. 62. O'Keefe, 5, J. D., Sender, P. M., and James, W, P. T. Catabolic Loss of Body Nitrogen in Response to Surgery. Lancet, 2: 1035-1038, 1974. 63. Owen, 0. E., Morgan, A. P., Kemp, H. G., Sullivan, J. M., Herrera, M. G., and Cahill, G. F., Jr. Brain Metabolism during Fasting. J. Clin. Invest., 46: 1589-1595,1967. 64. Owen, 0. E., Patel, M. S., Block, B. S. B., Kreulen, T. H., Reichle, F. A., and Mozzoli, M. A. Gluconeogenesis In Normal, Cirrhotic and Diabetic Humans. In: R. W. Hanson and M. Mehlman (eds.), Gluconeogenesis, Chap. 15, pp. 533-559. New York: John Wiley & Sons, 1976. 65. Passmore, R., and Draper, M. H. The Chemical Anatomy of the Human Body. In: R. H. S. Thompson and E. J, King (eds.), Biochemical Disor ders in Human Disease, pp. 1-19. London: J. & A. Churchill, Ltd., 1964. 66. Payne, P. R., and Waterlow, J. C. Relative Requirements for Mainte nance, Growth and Physical Activity. Lancet, 2: 210-21 1, 1971, 67. Picou, D,, and Taylor-Roberts, T. The Measurement of Total Protein Synthesis and Catabolism and Nitrogen Turnover in Infants in Different Nutritional States and Receiving Different Amounts of Dietary Protein. Clin. Sci., 36:283-296, 1969. 68. Reichard, G. A., Jr., Mowry, N. F., Hochella, N. J., Putnam, R. C., and Weinhouse, S. Metabolism of Neoplastic Tissue. xVll. Blood Glucose Replacement Rates in Human Cancer Patients. Cancer Res., 24: 71-76, 1964. 69. Rutten, P., Blackburn, G. L., Flatt, J. P., Hallowell, E., and Cochran, D. Determination of Optimal Hyperalimentation Infusion Rate. J. Surg. Res., 18:477-483, 1975. 70. Sabine, J. R. Metabolic Controls in Precancerous Liver. VII. Time Course of Loss of Dietary Feedback Control of Cholesterol Synthesis during Carcinogen Treatment. European J. Cancer, 12: 299-303, 1976. 71. Saudek, C. D,, and Felig, P. The Metabolic Events of Starvation. Am. J. Med.,60:117-126, 1976. 72. Shock, N. Energy Metabolism, Caloric Intake and Physical Activity of the Aging. In: L. A. Carlson (ed), Nutrition and Old Age, pp. 12-21 . Uppsala, Sweden: Swedish Nutrition Foundation, 1972. 73. Silver, 5. , Poroto, P., and Crohn, E, B. Hypermetabolic States without Hyperthyroidism (Nonthyrogenous Hypermetabolism). Arch . Internal Med.,85:479-482,1950. 74. Sims, E. A. H. Experimental Obesity, Dietary Induced Thermogenesis and Their Clinical Implications. Clin. Endocrinol. Metab., 5: 377-395, 1976. 75. Steffee, W. P., Goldsmith, R. S., Pencharz, P. B., Scrimshaw, N. S., and Young, V. A. Dietary Protein Intake and Dynamic Aspects of Whole Body Nitrogen Metabolism in Adult Humans. Metabolism,25: 281-297, 1976. 76.Terpeka, A, A., andWaterhouse, C. Metabolic Observations during Forced Feeding of Patients with Cancer. Am. J. Med., 20: 225-238, 1956, 77. Theologides, A. The Anorexia-Cachexia Syndrome: A New Hypothesis. Ann. N. Y. Acad. Sci., 230: 14-22, 1974, 78. Theologides, A. Anorexia-producing Intermediary Metabolites. Am. J. Ciin. Nutr., 29: 552-558, 1976. 79. Warburg, 0. Metabolism of Tumors. London: Constable and Co. , 1930. 80. Warren, S. The Immediate Causes of Death in Cancer. Am. J. Med . Sci., 184:610—615, 1932. 81. Waterhouse, C. Lactate Metabolism in Patients with Cancer. Cancer, 33: 66-71, 1974. 82. Waterhouse, C. How Tumors Affect Host Metabolism. Ann. N.Y. Acad. Sci., 230: 86-93, 1974. 83. Waterhouse, C., and Kemperman, J. H. Carbohydrate Metabolism in Subjects with Cancer, Cancer Res., 31: 1273-1278, 1971. 84. Waterhouse, C. L. , Fenninger, L. D. , and Keutmann, E. H. Nitrogen Exchange and Caloric Expenditure in Patients with Malignant Neoplasm. Cancer,4: 500-514, 1951. 85. Waterlow, J. C. Lysine Turnover in Man Measured by Intravenous Infu sion of L-[u-'[email protected]. Sci., 33: 507—515, 1967. 86. Waterlow, J. C. The Assessment of Protein Nutrition and Metabolism in the Whole Animal. In: H. N. Munro (ed), Mammalian Protein Metabo lism, Vol. 3, Chap. 28, pp. 325-390. New York: Academic Press, Inc., 1969. 87. Waterlow, J. C., and Alleyne, G. A. 0. Protein Malnutrition in Children: Advances in Knowledge in the Last Ten Years. Adv. Prot. Chem. 25: 117- 241,1971. 88. Waterlow, J. C., and Stephen, J. M. L. The Measurement of Total Lysine Turnover in the Rat by Intravenous Infusion of L-(U-―CjLysine.Clin. Sci. 33: 489-506,1967. 89. Watkin, D. M. Nitrogen Balance as Affected by Neoplastic Disease and Its Therapy. Am. J. Clin. Nutr., 9: 446-460, 1961. 90. Watkin, D. M., and Steinfield, J. L. Nutrient and Energy Metabolism In Patients with and without Cancer during Hyperalimentation with Fat Administered Intravenously. Am. J. Clin. Nutr., 16: 182-212, 1965. 91. Whittam, R. J. F. Hoffman (ed.), The Cellular Functions of Membrane Transport. Englewood Cliffs, N. J.: Prentice-Hall, 1964. 92. Wilmore, D. W. Nutrition and Metabolism following Thermal Injury. Clin. Plastic Surg., 1: 603—619,1974. 93. Wilmore,D. W., Lang,J. M., Mason,A.D.,Skreen, R.W.,and Pruitt, B. A. Catecholamines: Mediator of the Hypermetabolic Response to Ther mal Injury. Ann. Surg., 180: 663-668, 1974. 94. Young, V. R., Steffee, W. P., Pencharz, P. B., Winterer, J. C., and Scrimshaw, N. S. Total Human Body Protein Synthesis in Relation to Protein Requirements at Various Ages. Nature, 253: 192-194, 1975. 95. Young, V. A., Winterer, J. C., Munro, H. N., and Scrimshaw, N. S. Muscle and Whole Body Protein Metabolism, with Special Reference to Man. In: M. F. Elias, B. E. Eieftheriou, and P. K. Elias (eds.), Special Review of Experimental Aging Research: Progress on Biology, pp. 217-252. Bar Harbor, Maine: EAR, Inc., 1976. JULY 1977 Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 1977 American Association for Cancer Research. 2347 Energy Metabolism and Requirements in the Cancer Patient Vernon R. Young Cancer Res 1977;37:2336-2347. Updated version E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cancerres.aacrjournals.org/content/37/7_Part_2/2336 Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cancerres.aacrjournals.org on June 15, 2017. © 1977 American Association for Cancer Research.