Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
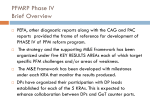
Long-Term Outcomes After Valve Replacement for Low-Gradient Aortic Stenosis Impact of Prosthesis-Patient Mismatch Alexander Kulik, MD; Ian G. Burwash, MD; Varun Kapila, BSc; Thierry G. Mesana, MD, PhD; Marc Ruel, MD, MPH Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Background—The long-term outcomes of patients with low-gradient aortic stenosis (LGAS) after aortic valve replacement (AVR) are poorly defined. The purpose of this study was to define the long-term outcomes of LGAS patients after AVR and to evaluate the potential impact of prosthesis–patient mismatch (PPM) in these patients. Methods and Results—A cohort of 664 patients undergoing AVR for aortic stenosis after 1990 were followed-up prospectively with annual clinical assessment and echocardiography (total follow-up 3447 patient-years; mean follow-up 5.2⫾3.3 years). LGAS was defined as an aortic valve area ⬍1.2 cm2, a mean transvalvular pressure gradient ⬍40 mm Hg, and a left ventricular (LV) ejection fraction ⬍50%, and was present in 79 patients. Rates and correlates of survival, freedom from congestive heart failure (CHF), and LV mass regression after AVR were determined using multivariate regression methods. Ten-year survival and freedom from CHF after AVR were 72.7⫾7.5% and 68.2⫾9.5%, respectively, for patients with LGAS, compared with 89.6⫾1.8% and 84.1⫾4.2% for patients without LGAS (hazard ratio [HR] for death and postoperative CHF, 3.1⫾1.1 and 2.7⫾0.9, respectively; P⬍0.01). In LGAS patients, PPM, defined as an indexed effective orifice area ⱕ0.85 cm2/m2, was independently associated with increased rates of CHF (HR, 3.6⫾2.2; P⫽0.039), impaired LV mass regression (P⫽0.037), and a trend toward increased late mortality (HR, 3.0⫾1.9; P⫽0.084). Conclusions—Patients with LGAS have worse long-term outcomes after AVR compared with patients without LGAS. PPM adversely affects the long-term outcomes of LGAS patients and should be avoided in this population. (Circulation. 2006;114[suppl I]:I-553–I-558.) Key Words: aortic stenosis 䡲 aortic valve replacement 䡲 prosthesis–patient mismatch A ortic valve replacement (AVR) relieves symptoms and improves survival in patients with symptomatic aortic stenosis (AS).1 However, a subset of patients with AS have a low transvalvular pressure gradient as a result of left ventricular (LV) systolic dysfunction and reduced transvalvular flow, a condition known as low-gradient aortic stenosis (LGAS). The ventricular dysfunction in patients with LGAS may result from excessive afterload of long-standing AS, or alternatively relate to concomitant coronary artery disease or a cardiomyopathy.2 Importantly, patients with LGAS undergoing AVR have higher operative mortality rates and reduced medium-term survival compared with patients with high gradient AS.3– 8 However, little is known regarding the long-term outcomes of LGAS patients after AVR and whether they are affected by the presence of prosthesis– patient mismatch (PPM).9 Therefore, the purpose of this study was to compare the long-term results of AVR in patients with and without LGAS with respect to all-cause mortality, freedom from congestive heart failure (CHF), and LV mass regression, and to identify potential factors that affect long-term outcomes. Methods Patient Population and Follow-Up Patients aged 18 years or older were prospectively followed-up after first-time AVR for AS between 1990 and 2002 at the University of Ottawa Heart Institute. Patients were excluded from the study population if they had more than mild (1⫹) aortic insufficiency at the time of operation, another concomitant valve procedure, did not survive the operation, or received a prosthesis that is no longer commercially available. After AVR, patients were assessed 6 months postoperatively and thereafter on an annual basis by a physician in a dedicated valve clinic. At each visit, patients underwent a medical history focused on the determination of functional status and the occurrence of valve-related complications, a physical examination, ECG, chest radiograph, complete blood count, serum chemistries, and international normalized ratio determinations when applicable. The methods of data collection and analysis of the valve clinic From the Division of Cardiac Surgery (A.K., V.K., T.G.M., M.R.), the Division of Cardiology (I.G.B.), and the Department of Epidemiology (M.R.), University of Ottawa, Ottawa, Ontario, Canada. Presented at the American Heart Association Scientific Sessions, Dallas, Tex, November 13–16, 2005. Correspondence to Marc Ruel, University of Ottawa Heart Institute, 40 Ruskin St, Suite 3403, Ottawa, Ontario, Canada K1Y 4W7. E-mail [email protected] © 2006 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org DOI: 10.1161/CIRCULATIONAHA.105.001180 I-553 I-554 Circulation July 4, 2006 database have been reviewed and approved by the University of Ottawa Heart Institute Human Research Ethics Board. All patients (N⫽664) were followed-up for at least 1 outpatient visit. The total follow-up was 3447 patient-years (mean 5.2⫾3.3 years; maximum 14.0 years). Patients were defined as having LGAS if they fulfilled all of 3 previously published criteria: preoperative aortic valve area ⬍1.2 cm2,5 mean transvalvular pressure gradient ⬍40 mm Hg,8,10 and left ventricular ejection fraction ⬍50%.3,6,11 Of the 664 patients in the study cohort, 79 patients had LGAS. Prostheses Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Prosthesis type and size were recorded in all patients. Prostheses were implanted and oriented according to the manufacturer’s recommendations. The effective orifice area (EOA) for each prosthesis type and size was obtained from the literature of patients with normally functioning prostheses,9,12 and averaged if ⬎1 published value was available. This was supplemented with phase I regulatory data provided by the valve manufacturer if published data were insufficient with respect to a specific prosthesis size. The indexed EOA was obtained by dividing the EOA by the patient’s body surface area at the time of operation, which was available for all patients. PPM was defined a priori as an indexed EOA ⱕ0.85 cm2/m2, because this definition constitutes the most commonly reported description of PPM in the literature.9,13,14 Echocardiograms Patients underwent a complete M-mode, 2-dimensional, and Doppler transthoracic echocardiogram at our institution before AVR. All patients underwent a postoperative echocardiogram, and thereafter as clinically indicated. LV mass was calculated from M-mode recordings as per the recommendations of the American Society of Echocardiography.15 TABLE 1. Characteristics of Patients With and Without LGAS LGAS (N⫽79) No LGAS (N⫽585) Female 17 (21.5%)* 212 (36.2%) Age at operation (years) 67.2⫾11.5 65.2⫾13.7 Body mass index (kg/m2) 26.7⫾3.3 27.5⫾4.6 Cigarette smoking 14 (17.7%) 91 (15.6%) Cerebrovascular accident 0 (0%) 4 (0.7%) 8 (10.1%)* 28 (4.8%) 3 (3.8%) 12 (2.0%) 1 19 (24.3%) 171 (29.3%) 2 18 (22.9%) 181 (30.9%) 3 23 (28.6%) 145 (24.8%) 4 19 (24.3%) 88 (15.1%) 1 0 (0%)* 451 (77.1%) 2 22 (27.8%)* 75 (12.8%) 3 28 (35.4%)* 40 (6.7%) 4 29 (36.7%)* 20 (3.4%) Preoperative mean transvalvular pressure gradient (mm Hg) 29.1⫾7.7* 50.4⫾19.8 Preoperative aortic valve area (cm2) Diabetes mellitus Chronic atrial fibrillation NYHA class LV grade † 0.81⫾0.19 0.72⫾0.45 Preoperative LV end-diastolic diameter (cm) 6.0⫾0.9* 5.3⫾0.9 Preoperative LV end-systolic diameter (cm) 4.5⫾1.0* 3.3⫾1.0 Statistical Analyses Preoperative mitral regurgitation grade 1.2⫾0.8* 0.9⫾0.8 Clinical Outcomes *P⬍0.05 vs patients without LGAS. Grade 1⫽LV ejection fraction ⱖ50%; grade 2⫽LV ejection fraction of 40%0 – 49%; grade 3⫽ejection fraction of 30%–39%; grade 4⫽ejection fraction ⬍30%. LGAS indicates low-gradient aortic stenosis; LV, left ventricle; NYHA, New York Heart Association. Data were analyzed in Intercooled Stata 8.0 (Stata, College Station, Tex). Non-parametric estimates of freedom from all-cause death and freedom from the composite CHF end-point were determined using the Kaplan-Meier method. For the CHF analysis, a composite CHF end-point was a priori defined as: (1) New York Heart Association (NYHA) functional class 3 or 4 for ⬎4 consecutive weeks; or (2) death in which the primary or main contributing diagnosis was CHF.9 Clinical impressions were corroborated with physical examination, chest radiograph, ECG, and echocardiographic findings. Deaths from an unknown cause were not considered to result from CHF and were treated as a censored event if the patient had not previously experienced NYHA class 3 or 4 symptoms. Survival and freedom from CHF rates after AVR were reported as mean⫾standard error. Multivariate Analyses Possible predictors of death or the CHF composite end-point were individually tested for equality with a log-rank test. Cox proportional hazards models were developed: (1) by forcing into the model risk factors for decreased survival and freedom from CHF after AVR (LV function, age, atrial fibrillation, preoperative heart failure functional class, coronary artery disease, smoking, and insulin-dependent diabetes mellitus) that have been previously identified;9 and (2) by incorporating any other variable that had Pⱕ0.20 on univariate log-rank testing. To account for confounding, no automated model selection procedure was used, and all covariates were used simultaneously unless found to be collinear as determined by a Spearman rank correlation coefficient ⱖ0.30 and P⬍0.005. For all other tests, statistical significance was set at P⬍0.05. Statement of Responsibility The authors had full access to the data and take full responsibility for their integrity. All authors have read and agree to the manuscript as written. † Results Patient Characteristics Preoperative characteristics of patients with and without LGAS are presented in Table 1. Patients with LGAS were more often male, had a higher prevalence of diabetes, and had worse preoperative LV function (all P⬍0.05). The operative procedure and valve prosthesis characteristics are summarized in Table 2. LGAS patients underwent concomitant coronary artery bypass grafting (CABG) more frequently than those without LGAS (P⬍0.05). There was no difference in the types of valves implanted between groups. Survival During the study period, the perioperative mortality of all patients who underwent AVR was 3.5%, whereas that of patients with LGAS was significantly higher at 7.5% (P⫽0.02). Survival (excluding operative mortalities) at 1, 5, and 10 years after AVR for patients with LGAS was 97.3⫾1.9%, 83.8⫾5.1%, and 72.7⫾7.5%, respectively. In contrast, patients without LGAS had 1-year, 5-year, and 10-year survival rates of 98.8⫾0.5%, 93.1⫾1.2%, and 89.6⫾1.8%, respectively, significantly higher than those observed for LGAS patients (HR, 3.1; 95% confidence Kulik et al TABLE 2. Low-Gradient Aortic Stenosis I-555 Operative and Valve Prosthesis Characteristics LGAS (N⫽79) No LGAS (N⫽585) Concomitant CABG 49 (62.0%)* 198 (33.8%) Cardiopulmonary bypass duration (minutes) 125.8⫾34.8 117.6⫾41.0 Aortic cross-clamp duration (minutes) 85.3⫾22.0 79.7⫾27.1 Mechanical valves 39 (49.4%) 272 (46.5%) Medtronic Hall 4 (5.0%) 45 (7.7%) St. Jude 20 (25.3%) 139 (23.8%) Carbomedics 14 (17.7%) 82 (14.0%) 1 (1.3%) 6 (1.0%) 40 (50.6%) 313 (53.5%) MCRI On-X Bioprosthetic valves Homograft Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 2 (2.5%) 42 (7.2%) Medtronic Hancock 35 (44.3%) 230 (39.3%) Edwards Pericardial 3 (3.8%) 32 (5.5%) Edwards Porcine — 4 (0.7%) Stentless Porcine† — 5 (0.9%) *P⬍0.05 vs patients without LGAS. † Denotes either a St. Jude Toronto Stentless or Medtronic Freestyle prosthesis. CABG indicates coronary artery bypass grafting; LGAS, low-gradient aortic stenosis. interval [CI], 1.5, 6.1; P⫽0.001; Figure 1A). Furthermore, LGAS patients had decreased long-term survival when compared with patients without LGAS who had LV dysfunction (HR, 3.0; 95% CI, 1.1, 8.0; P⫽0.027). After adjusting for known confounders,9 late mortality among LGAS patients was independently predicted by a history of atrial fibrillation (HR, 5.1; 95% CI, 1.1, 24.4; P⫽0.04). There was a trend toward increased late mortality among LGAS patients with PPM (HR, 3.0; 95% CI, 0.9, 10.1; P⫽0.084; Figure 2A). Moreover, using indexed EOA as a continuous variable, there was a trend to better long-term survival among LGAS patients with a larger indexed EOA (HR, 0.08 per unit m2/cm2 change; 95% CI, 0.01, 4.3; P⫽0.213). Heart Failure NYHA class improved from the preoperative to postoperative period in patients with LGAS (2.5⫾1.1 to 1.3⫾0.6; P⬍0.001) and patients without LGAS (2.3⫾1.0 to 1.2⫾0.5, P⬍0.001). However, patients with LGAS were more likely to have persistent or recurrent CHF after AVR, with lower freedom from the composite CHF outcome of NYHA 3 to 4 symptoms or CHF-related death (Figure 1B). Freedom from the composite CHF outcome for LGAS patients at 1, 5, and 10 years was 97.2⫾2.0%, 84.4⫾5.3%, and 68.2⫾9.5%, respectively, and significantly worse compared with 99.5⫾0.3%, 94.5⫾1.2%, and 84.1⫾4.2% for patients without LGAS (HR, 2.7; 95% CI, 1.4, 5.2; P⫽0.003). Furthermore, LGAS patients had a significantly lower freedom from the composite CHF outcome when compared with patients without LGAS who had LV dysfunction (HR, 2.6; 95% CI, 1.1, 6.4; P⫽0.028). After adjustment for known confounders,9 the presence of PPM (ⱕ0.85 cm2/m2) was an independent predictor of persistent or recurrent CHF after AVR among LGAS patients (HR, 3.6; 95% CI, 1.1, 11.9; P⫽0.039; Figure Figure 1. Survival (A) and the incidence of persistent or recurrent CHF (B) in patients with and without LGAS after AVR. *Hazard ratio adjusted for left ventricular function, age, atrial fibrillation, preoperative NYHA functional class, coronary artery disease, smoking, and insulin-dependent diabetes mellitus. AVR indicates, aortic valve replacement; CHF, congestive heart failure; CI, confidence interval; LGAS, low-gradient aortic stenosis. 2B). Moreover, using indexed EOA as a continuous variable, a larger indexed EOA was associated with better freedom from CHF among LGAS patients (HR 0.02 per unit m2/cm2 change; 95% CI 0.01, 0.69; P⫽0.03). Postoperative LV Remodeling Patients with LGAS and postoperative PPM had significantly less LV mass regression compared with patients with LGAS and no PPM (PPM 9⫾14 versus no PPM 79⫾31 grams; P⫽0.037) (Figure 3). Similarly, patients with LGAS and PPM had less LV mass regression when indexed for body surface area compared with LGAS patients without PPM (PPM 5⫾7 versus no PPM 45⫾19 g/m2, P⫽0.05). Furthermore, the coefficient for PPM was significantly reduced in a multivariate linear model for LV mass regression that included patient characteristics and the presence of persistent hypertension during postoperative follow-up (coefficient 32; I-556 Circulation July 4, 2006 Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Figure 2. Impact of PPM on survival (A) and the incidence of persistent or recurrent CHF (B) after AVR in patients with LGAS. *Hazard ratio adjusted for LV function, age, atrial fibrillation, preoperative heart failure functional class, coronary artery disease, smoking, and insulin-dependent diabetes mellitus. IEOA indicate indexed effective orifice area; PPM, prosthesis–patient mismatch. 95% CI: 4, 59; P⫽0.02). A detrimental effect of PPM on LV mass regression was also observed in patients without LGAS but was not as pronounced (PPM 44⫾6 versus no PPM 59⫾7 grams; P⫽0.1). Discussion The natural history of patients with LV systolic dysfunction and LGAS is poor with medical management. AVR has the Figure 3. Impact of PPM on LV mass regression after AVR among patients with and without LGAS. LV indicates left ventricle.*P⫽0.037 refers to the comparison of PPM vs no PPM in LGAS patients. †P⫽0.1 refers to the comparison of PPM vs no PPM in no LGAS patients. potential to improve LV function and survival by removing the excessive afterload caused by a severely stenotic aortic valve. However, LV function may not improve after AVR if concomitant coronary artery disease or a cardiomyopathy is responsible for the LV dysfunction.2 Furthermore, high perioperative mortality rates have been observed in LGAS patients undergoing AVR,3– 8 and the long-term outcomes of LGAS patients surviving surgery is unclear. The purpose of this study was to define the long-term outcomes after AVR in LGAS patients and determine whether the presence of PPM impacts on patient outcome. In this cohort followed-up annually after AVR, we observed that: (1) patients with LGAS have worse survival and freedom from CHF after AVR compared with patients without LGAS; (2) PPM is an independent risk factor for CHF and a trend to late mortality in patients with LGAS; and (3) LGAS patients with PPM have less LV mass regression following AVR. Thus, patients with LGAS have a worse long-term prognosis after AVR and tolerate PPM poorly. Patients with LGAS are at substantial risk during AVR, with reported surgical mortality rates ranging from 8% to 33%.3–7 However, the short-term and intermediate-term outcomes with medical management appear worse.7,8 In a propensity matched study, the 1-year and 4-year survival rates of 39 patients with LGAS undergoing AVR were 82% and 78%, respectively, compared with 41% and 15% observed in 56 medically treated patients (P⬍0.0001).7 In our larger cohort of LGAS patients undergoing AVR, we observed a similar 84% 5-year survival rate, and we extended these observations with a 10-year survival rate of 73%. In addition, we have demonstrated that the majority of LGAS patients obtain benefit through the improvement of symptoms following surgery. The principal finding of our study relates to the profoundly negative impact of PPM on the long-term outcomes of LGAS patients undergoing AVR. The concept of PPM was first introduced by Rahimtoola in 1978 to describe the condition in which the prosthetic valve orifice area is less than that of the native human valve.16 Subsequent studies examining the physiological sequelae of PPM have fostered the recommendation that the indexed EOA of an aortic prosthesis should ideally be greater than 0.85 cm2/m2 to minimize postoperative gradients and improve clinical results.12,13 While there remains controversy in the literature as to the relevance of PPM, previous work by our group9,17 and others18 has demonstrated that PPM is a strong and independent predictor of adverse outcomes after AVR, particularly in patients with LV dysfunction. The current study adds to our understanding of the optimal management of LGAS patients. Along with defining the expected long-term survival of LGAS patients undergoing AVR, we have identified a threshold in prosthesis size related to the patient’s body surface area, beyond which survival and cardiac recovery may not reach their maximum potential after valve replacement. No published study to date has described the detrimental effect of PPM (defined as a threshold of ⱕ0.85 cm2/m2) after AVR on the long-term clinical outcomes in LGAS patients. PPM significantly impaired long-term survival, freedom from heart failure, and LV mass regression Kulik et al Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 in this patient population. Therefore, PPM at or beyond this threshold should be avoided in patients with LGAS undergoing AVR. Strategies to predict12 and avoid PPM at the time of surgery may lead to improved LGAS outcomes, such as aortic root enlargement. Previous studies in patients with LGAS have demonstrated a negative impact of small prosthesis size on surgical mortality, signifying that failure to effectively reduce afterload can lead to detrimental outcomes.5,19 In contrast, we used the indexed EOA derived from normally functioning valves because this methodology has the advantage of accounting for the large variation in body size in AVR patients, which is an important determinant of the adequacy of a given prosthesis size to relieve outflow obstruction.12 The EOA derived by Doppler-echo continuity equation from individual patients after implantation of the prosthesis may have betterquantified the degree of PPM. However, this methodology has several significant limitations related to difficulties in accurately measuring the LV outflow diameter because of prosthetic valve reverberations, and the presence of large localized transprosthetic gradients or nonuniform transprosthetic spatial velocity profiles, which frequently result in large discrepancies between Doppler-echo and “actual” EOA measurements.20,21 Importantly, EOAs derived from individual patients are not available at the time of surgical decisionmaking. The EOA can only be determined once the prosthesis has been inserted, the patient has been weaned from cardiopulmonary bypass, and the preload, afterload, and contractility have normalized. Therefore, the EOA of an individual patient has little or no role in predicting whether PPM will be avoided or not by a given prosthesis type and size, whether another prosthesis type or size should be selected, or whether aortic root enlargement should be performed before implantation. In patients with severe AS and preoperative LV dysfunction, AVR induces a favorable remodeling of the LV, characterized by normalization of wall stress indices, regression of chamber dilatation, reduction of LV hypertrophy, and an improvement in cardiac performance.22 Similarly, we observed LV mass regression in our patients with and without LGAS after AVR. However, there was a significant impairment in LV mass regression in LGAS patients with PPM after AVR compared with LGAS patients without PPM, and this was associated with a decrease in long-term survival and freedom from CHF. This illustrates the concept that patients with LV dysfunction and LGAS are particularly sensitive to increases in afterload and incomplete relief of LV outflow tract obstruction after AVR. The definition of LGAS used in this study included the previously published criteria of preoperative aortic valve area ⬍1.2 cm2, mean transvalvular pressure gradient ⬍40 mm Hg, and left ventricular ejection fraction ⬍50%.3,5,6,8,10,11 In this regard, some investigators have used even lower gradients and/or ejection fraction criteria; however, a consensus definition of LGAS has not yet been agreed on in the literature.2– 8 The LGAS definition used in this article was decided on for 2 reasons before performing the statistical analyses. First, if PPM was found to have a detrimental effect at our chosen LGAS definition, then it would likely result in at least Low-Gradient Aortic Stenosis I-557 equivalent impact among LGAS patients with even lower transvalvular gradients and more severe LV dysfunction.17 Second, our chosen definition allowed for sufficient sample size to explore the impact of PPM in this relatively rare clinical condition. Potential Limitations All patients in the study cohort had AS and underwent AVR. However, many patients had concomitant coronary artery disease, and it is therefore difficult to determine with certainty the foremost indication for surgery. Nevertheless, both LGAS and no LGAS patient groups had mean preoperative aortic valve areas within the severe range, indicating that hemodynamically severe AS was present in these patients. Preoperative dobutamine challenge during echocardiography or cardiac catheterization was performed in a minority of our patients and thus could not be incorporated in our outcome models. Unsuspected demographic and selection factors unique to this study cohort may have resulted in overfitted statistical associations. We examined the long-term outcomes of LGAS patients who survived AVR to evaluate the impact of surgery and PPM on heart failure symptoms and LV mass regression. Perioperative outcomes were not examined because surgical decision-making and confounding by indication may particularly bias operative mortality rates in patients with PPM. Furthermore, a threshold of ⱕ0.85 cm2/m2 was chosen a priori as the definition of PPM. Lower thresholds have occasionally been used to quantify the severity of PPM (ie, severe PPM defined as ⱕ0.65 cm2/m2) and higher 30-day mortality rates have been reported in AS patients with severe PPM after AVR.18 Conclusions Patients with LGAS represent a small subset (⬇12%) of AS patients requiring AVR. LGAS patients have a worse longterm survival and decreased freedom from CHF after AVR compared with patients without LGAS. PPM in patients with LGAS results in less LV mass regression after AVR and is an important and potentially preventable independent risk factor for both late mortality and CHF in this challenging subset of AS patients. Disclosures None. References 1. Bonow RO, Carabello B, de Leon AC, Jr., Edmunds LH Jr, Fedderly BJ, Freed MD, Gaasch WH, McKay CR, Nishimura RA, O’Gara PT, O’Rourke RA, Rahimtoola SH, Ritchie JL, Cheitlin MD, Eagle KA, Gardner TJ, Garson A, Jr., Gibbons RJ, Russell RO, Ryan TJ, Smith SC, Jr. Guidelines for the management of patients with valvular heart disease: executive summary. A report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines (Committee on Management of Patients with Valvular Heart Disease). Circulation. 1998;98:1949 –1984. 2. Carabello BA, Green LH, Grossman W, Cohn LH, Koster JK, Collins JJ, Jr. Hemodynamic determinants of prognosis of aortic valve replacement in critical aortic stenosis and advanced congestive heart failure. Circulation. 1980;62:42– 48. 3. Blitz LR, Herrmann HC. Hemodynamic assessment of patients with low-flow, low-gradient valvular aortic stenosis. Am J Cardiol. 1996;78: 657– 661. I-558 Circulation July 4, 2006 Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 4. Connolly HM, Oh JK, Orszulak TA, Osborn SL, Roger VL, Hodge DO, Bailey KR, Seward JB, Tajik AJ. Aortic valve replacement for aortic stenosis with severe left ventricular dysfunction. Prognostic indicators. Circulation. 1997;95:2395–2400. 5. Connolly HM, Oh JK, Schaff HV, Roger VL, Osborn SL, Hodge DO, Tajik AJ. Severe aortic stenosis with low transvalvular gradient and severe left ventricular dysfunction:result of aortic valve replacement in 52 patients. Circulation. 2000;101:1940 –1946. 6. Brogan WC, 3rd, Grayburn PA, Lange RA, Hillis LD. Prognosis after valve replacement in patients with severe aortic stenosis and a low transvalvular pressure gradient. J Am Coll Cardiol. 1993;21:1657–1660. 7. Pereira JJ, Lauer MS, Bashir M, Afridi I, Blackstone EH, Stewart WJ, McCarthy PM, Thomas JD, Asher CR. Survival after aortic valve replacement for severe aortic stenosis with low transvalvular gradients and severe left ventricular dysfunction. J Am Coll Cardiol. 2002;39: 1356 –1363. 8. Monin JL, Quere JP, Monchi M, Petit H, Baleynaud S, Chauvel C, Pop C, Ohlmann P, Lelguen C, Dehant P, Tribouilloy C, Gueret P. Lowgradient aortic stenosis: operative risk stratification and predictors for long-term outcome: a multicenter study using dobutamine stress hemodynamics. Circulation. 2003;108:319 –324. 9. Ruel M, Rubens FD, Masters RG, Pipe AL, Bedard P, Hendry PJ, Lam BK, Burwash IG, Goldstein WG, Brais MP, Keon WJ, Mesana TG. Late incidence and predictors of persistent or recurrent heart failure in patients with aortic prosthetic valves. J Thorac Cardiovasc Surg. 2004;127: 149 –159. 10. Nishimura RA, Grantham JA, Connolly HM, Schaff HV, Higano ST, Holmes DR, Jr. Low-output, low-gradient aortic stenosis in patients with depressed left ventricular systolic function: the clinical utility of the dobutamine challenge in the catheterization laboratory. Circulation. 2002;106:809 – 813. 11. deFilippi CR, Willett DL, Brickner ME, Appleton CP, Yancy CW, Eichhorn EJ, Grayburn PA. Usefulness of dobutamine echocardiography in distinguishing severe from nonsevere valvular aortic stenosis in patients with depressed left ventricular function and low transvalvular gradients. Am J Cardiol. 1995;75:191–194. 12. Pibarot P, Dumesnil JG. Hemodynamic and clinical impact of prosthesis-patient mismatch in the aortic valve position and its prevention. J Am Coll Cardiol. 2000;36:1131–1141. 13. Pibarot P, Honos GN, Durand LG, Dumesnil JG. The effect of prosthesis-patient mismatch on aortic bioprosthetic valve hemodynamic performance and patient clinical status. Can J Cardiol. 1996;12:379 –387. 14. Pibarot P, Dumesnil JG, Cartier PC, Metras J, Lemieux MD. Patientprosthesis mismatch can be predicted at the time of operation. Ann Thorac Surg. 2001;71:S265–S268. 15. Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, Reichek N. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol. 1986;57:450 – 458. 16. Rahimtoola SH. The problem of valve prosthesis-patient mismatch. Circulation. 1978;58:20 –24. 17. Ruel M, Al-Faleh H, Kulik A, Chan KL, Mesana TG, Burwash IG. Prosthesis-patient mismatch after aortic valve replacement primarily affects patients with pre-existing left ventricular dysfunction: impact on survival, freedom from heart failure, and left ventricular mass regression. J Thorac Cardiovasc Surg. 2006;131:1036 –1044. 18. Blais C, Dumesnil JG, Baillot R, Simard S, Doyle D, Pibarot P. Impact of valve prosthesis-patient mismatch on short-term mortality after aortic valve replacement. Circulation. 2003;108:983–988. 19. Morris JJ, Schaff HV, Mullany CJ, Rastogi A, McGregor CG, Daly RC, Frye RL, Orszulak TA. Determinants of survival and recovery of left ventricular function after aortic valve replacement. Ann Thorac Surg. 1993;56:22–29; discussion 29 –30. 20. Baumgartner H, Khan S, DeRobertis M, Czer L, Maurer G. Effect of prosthetic aortic valve design on the Doppler-catheter gradient correlation: an in vitro study of normal St. Jude, Medtronic-Hall, StarrEdwards and Hancock valves. J Am Coll Cardiol. 1992;19:324 –332. 21. Henneke KH, Pongratz G, Bachmann K. Limitations of Doppler echocardiography in the assessment of prosthetic valve hemodynamics. J Heart Valve Dis. 1995;4:18 –25. 22. Pela G, La Canna G, Metra M, Ceconi C, Berra Centurini P, Alfieri O, Visioli O. Long-term changes in left ventricular mass, chamber size and function after valve replacement in patients with severe aortic stenosis and depressed ejection fraction. Cardiology. 1997;88:315–322. Long-Term Outcomes After Valve Replacement for Low-Gradient Aortic Stenosis: Impact of Prosthesis-Patient Mismatch Alexander Kulik, Ian G. Burwash, Varun Kapila, Thierry G. Mesana and Marc Ruel Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Circulation. 2006;114:I-553-I-558 doi: 10.1161/CIRCULATIONAHA.105.001180 Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2006 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/114/1_suppl/I-553 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/