Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Psychoneuroimmunology wikipedia , lookup
Urinary tract infection wikipedia , lookup
Common cold wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Staphylococcus aureus wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Hepatitis B wikipedia , lookup
Neonatal infection wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
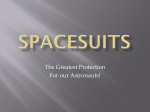
INVITED ARTICLE HEALTHCARE EPIDEMIOLOGY Robert Weinstein, Section Editor Infection Prevention and Control During Prolonged Human Space Travel Leonard A. Mermel Department of Medicine, Warren Alpert Medical School of Brown University, Division of Infectious Diseases, Department of Epidemiology and Infection Control, Rhode Island Hospital, Providence, Rhode Island Prolonged human spaceflight to another planet or an asteroid will introduce unique challenges of mitigating the risk of infection. During space travel, exposure to microgravity, radiation, and stress alter human immunoregulatory responses, which can in turn impact an astronaut’s ability to prevent acquisition of infectious agents or reactivation of latent infection. In addition, microgravity affects virulence, growth kinetics, and biofilm formation of potential microbial pathogens. These interactions occur in a confined space in microgravity, providing ample opportunity for heavy microbial contamination of the environment. In addition, there is the persistence of aerosolized, microbe-containing particles. Any mission involving prolonged human spaceflight must be carefully planned to minimize vulnerabilities and maximize the likelihood of success. Keywords. infection prevention; infection control; space medicine; aviation medicine; astronaut. The US National Aeronautics and Space Administration (NASA) is currently planning for prolonged human spaceflight. It is estimated that a mission to and from Mars will take a minimum of 520 days, the crew will be 360 million kilometers from Earth, there will be a 20-minute one-way communication delay from this distance [24], and there may be no way to return to Earth until the mission is completed. Clearly space travel creates a unique challenge of preventing and controlling infection. In addition to the physiologic effects of microgravity on humans, exposure to solar and cosmic radiation, the stress of being in a confined setting, and the myriad of changes observed in microorganisms in this unique environment all add to the complexity of this endeavor (Figure 1). Crucian and Sams wrote, “it cannot yet be firmly concluded that a clinical risk related to immune Received 16 July 2012; accepted 24 September 2012; electronically published 9 October 2012. Correspondence: Division of Infectious Diseases, Rhode Island Hospital, 593 Eddy Street, Providence, RI 02903 ([email protected]). Clinical Infectious Diseases 2013;56(1):123–30 © The Author 2012. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: [email protected]. DOI: 10.1093/cid/cis861 dysregulation actually exists for exploration-class spaceflight” [1]. Nevertheless, in microgravity, potential microbial pathogens demonstrate enhanced expression of virulence factors [2–5], more rapidly enter into log-phase growth in liquid media [6, 7], and may increase biofilm formation [8]. At the same time, there is dysregulation of the human immune system during space travel, which may increase risk of infection [9– 11], including reactivation of herpesviruses [12]. In addition, anaerobic colonic flora is diminished with a commensurate increase in aerobic bacteria such as Pseudomonas and Staphylococcus aureus [13, 14] and there is a greater abundance of S. aureus, along with Enterobacteriaceae, on the skin [13] and in the upper airway [14]. Numerous conditions that are conducive to the spread of infection exist within the confines of a containment vessel such as the International Space Station. Transmission of microbial flora among astronauts, including some multidrug-resistant pathogens, has been demonstrated [13, 15–20]; microbes survive in free-floating condensate [21]; and symptom-based management of medical conditions [22] may be carried out by individuals who may not have medical or nursing degrees and must confer with earthbound physicians at Mission Control. Based on postflight medical debriefs, there were 29 infectious disease HEALTHCARE EPIDEMIOLOGY • CID 2013:56 (1 January) • 123 anaerobic flora and increased density of aerobic gram-negative bacteria and staphylococci on the skin and in the upper airway and colon [14]. Additionally, stress associated with space travel in a confined environment may induce changes in the intestinal microbiome that are unrelated to microgravity, and this may impact immune function [38, 39]. The Microbe Figure 1. Variables that impact the risk of infectious diseases and their transmission during space travel. incidents (ie, fever/chills [8], fungal infection [5], flu-like illness [3], urinary tract infection [4], aphthous stomatitis [3], viral gastroenteritis [2], subcutaneous skin infection [2], and other viral disease [2]) among approximately 742 crew members who have flown 106 space shuttle flights [23]. This review explores the challenges of preventing and controlling infections and suggests potential countermeasures. The opinions expressed are those of the author. It is hoped that the article will engender greater collaboration among the infection control, infectious diseases, and space science communities. INFECTION PREVENTION CHALLENGES In microgravity, bacteria demonstrate enhanced growth patterns in liquid media [6], reflecting a shortened lag phase and enhanced exponential growth [7]. Additionally, bacteria demonstrate enhanced virulence [2–5]; higher minimal inhibitory concentrations to various classes of antimicrobial agents [40–42], which is at least partly due to thickening of the microbial cell wall [43, 44]; increased conjugal transfer rates [45]; increased production of quorum-sensing molecules such as N-acyl homoserine lactone [46]; enhanced virulence, leading to increased mortality in animal infection models [47]; increased biofilm formation [48]; and increased survival within macrophage [4]. For additional information on the effect of microgravity on microbes, see Horneck et al [49]. The Spacecraft or Space Habitat The internal environment of a spacecraft or space station can become heavily contaminated with microbes [50], and freefloating condensate has been found to harbor numerous bacteria, fungi, and even protozoa [21]. Microgravity affects the aerobiology of the aerosols that are created from a cough or sneeze or during speech. Particles remain airborne until they are inspired, swallowed, contact an otherwise absorbable surface, or are ideally promptly removed by an air filtration system. The presence of these aerosols affects the risk of person-to-person transmission of viruses such as influenza [51–53] and even bacteria such as S. aureus [54, 55]. PREFLIGHT COUNTERMEASURES The Astronaut The immune system undergoes a number of changes during space travel [9, 10], including impaired wound healing [25], inhibition of leukocyte blastogenesis and altered leukocyte distribution [26–28], altered monocyte and granulocyte function [28–30], impaired leukocyte proliferation following activation [31], altered cytokine production patterns [26], abrogated bone marrow responsiveness to colony-stimulating factors [32, 33], altered T-cell intracellular signaling [34], inhibition of natural killer cell activity [35], inhibition of delayed-type hypersensitivity [36, 37], and apparent Th2 potential bias shift [10]. Although the effects of spaceflight on human gut flora have not been studied extensively, changes in the human microbiome have been demonstrated, with reduced density of 124 • CID 2013:56 (1 January) • HEALTHCARE EPIDEMIOLOGY Interventions for mitigating the risk of infection prior to space travel are described in this section (Table 1). The Astronaut A robust vaccination program that includes tetanus/diphtheria/acellular pertussis (Tdap), measles/mumps/rubella (MMR), influenza, pneumococcal, meningococcal, and hepatitis A and B vaccines should be implemented. Because of increased reactivation of herpesviruses, which has been noted in past space missions [12], varicella zoster virus vaccine should be given. In the unlikely event that an astronaut is unknowingly carrying Salmonella, typhoid vaccine should be considered to reduce the risk of transmission. Table 1. Preflight Countermeasures Currently Done by US National Aeronautics and Space Administration Not Done but Recommended Not Done but Consider Astronaut • Medical/dental history and physical • • • • Vaccination ○ Influenza ○ Tetanus, diptheria, acellular pertussis ○ Mumps, measles, rubella ○ Hepatitis A and B Screening, decolonization, and treatment if colonized or infected, respectively ○ Tuberculosis (interferon-gamma release assay) ○ S. aureus (screen nares for MRSA) ○ Human immunodeficiency virus (serology) Isolation from community for a period of time equal to the incubation period for viral respiratory and gastrointestinal pathogens and bacterial pathogens that cause food poisoning Training for aseptic insertion of intravenous and bladder catheters Animals • Vaccination, screening • Pathogen-free animals Plants • Nonsoil-based growth Containment vessel • Potable water storage and distribution systems made of nonleaching material • Point-of-use filters and catalytic oxidation or pasteurization ○ ○ ○ ○ ○ Meningococcus Pneumococcus Varicella-zoster Typhoid • ○ ○ ○ ○ • ○ • • • S. aureus (screen multiple body sites for MRSA and MSSA) Salmonella (screen multiple stools) Strongyloides (serology) Endemic fungi (serology for coccidiomycosis; histoplasmosis) Bioterrorism agents (eg, anthrax) Skin and nares colonization with serine protease Esp-producing Staphylococcus epidermidis that selectively inhibits S. aureus biofilm and nasal colonization Infection control education (eg, hand hygiene, cough etiquette) Infection control protocol for cleaning cages and bedding High-efficiency particulate air filtration system Human factors engineering input regarding location of water outlets and waterless hand-hygiene product dispensers Foot-pedal–operated potable water outlets Reverse osmosis for potable water • Air balancing with living quarters positive (or neutral) pressure to potential docking station and positive (or neutral) pressure to bathroom • Antimicrobial, nonleaching coating of permanent surfaces/structures Other • Selected food is gamma-irradiated, other food undergoes microbial analysis for specific pathogens and fungi Abbreviation: Esp, extracellular serine protease; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-susceptible Staphylococcus aureus. Health screening, including a complete dental exam, should be standard practice. Screening for tuberculosis with an interferon gamma release assay [56] should be conducted. Because S. aureus has been transmitted astronaut-to-astronaut in space [13, 18], robust screening of astronauts for both methicillinsusceptible and methicillin-resistant S. aureus carriage should be done, to include nares, throat, and rectal sampling [57, 58] using techniques with enhanced sensitivity and that involve a molecular method [59]. An algorithm using quantitative nasal cultures may identify those at high risk for persistent S. aureus carriage [60]. S. aureus [61, 62] carriers should be decolonized using serial screening cultures after completion of a decolonization regimen to ensure that carriage has been eradicated [63]. Screening for human immunodeficiency virus (HIV) should be done. Also, screening of astronauts for latent endemic fungal infections such as coccidiomycosis and histoplasmosis should be considered to minimize the risk of reactivation [64]. Screening for Strongyloides and possibly other parasitic infections that may be endemic to the astronauts’ home countries should be considered. Screening multiple stool samples for Salmonella carriage should also be considered [65]. Pretravel infection control education that includes hand hygiene and cough etiquette and a review of the modes of HEALTHCARE EPIDEMIOLOGY • CID 2013:56 (1 January) • 125 microbial transmission and attendant mitigation strategies should be provided. An infection control manual should be reviewed prior to travel and kept on board. The manual should include instructions regarding symptom-based isolation precautions, aseptic technique for insertion and maintenance of inserted medical devices, and similar information. Training for aseptic insertion of intravenous and bladder catheters should also be provided. Additionally, focus groups consisting of astronauts with past space travel experience and human factors engineers should meet to discuss barriers to performing hand hygiene and the ideal location of waterless hand-hygiene product dispensers [66]. As part of the current Health Stabilization program, astronauts are isolated from others in the community for a period of time greater than the incubation period for most common viral upper respiratory tract, gastrointestinal, viral, and bacterial infections. Isolation begins 7 days before launch. It is unclear whether all foodstuffs should be irradiated with gamma radiation for prolonged space missions. Prolonged ingestion of sterile food alters the colonic microbiome, and the microbes in food that become part of the colonic flora likely serve an important homeostatic function for the immune system. On the other hand, irradiation prolongs shelf-life and potential contamination with microbes that cause gastrointestinal illness are a concern. As such, gamma irradiation of selected food should be undertaken as is currently done. Deliverables to the containment vessel should be gamma-irradiated or undergo other sterilizing procedures. The Spacecraft or Space Habitat Ideally, the breathable air within a spacecraft or space habitat is filtered with a high-efficiency particulate air (HEPA) filter and humidity controlled. However, energy requirements for existing filters has made the use of such an air-handling system prohibitive. Consideration should be made for positive or neutral pressure within the containment vessel to reduce the risk of airborne microbes entering the containment vessel after docking if technically feasible. Additionally, consideration should be made for the bathroom to be under negative or neutral pressure compared with that of the living quarters in the containment vessel. The water storage and distribution system should be manufactured using noncorrosive material that has limited organic carbon to minimize biofilm formation. Antibiofouling coatings and materials should be developed to further mitigate propagation of microbes in the water system. Of course, these materials must not introduce any potential toxicity to the astronauts. Potable water should be pasteurized or undergo catalytic oxidation, which is the current method of disinfection. Redundancy for additional protection from waterborne microbes should include point-of-use submicron filters. Foot-pedal–operated potable water outlets will 126 • CID 2013:56 (1 January) • HEALTHCARE EPIDEMIOLOGY minimize the risk of touch contamination and transmission of pathogens [67]. Coating surfaces within the spacecraft should be made of a nonleaching, nonporous antimicrobial material [68], providing these materials do not introduce toxicity to the astronauts despite prolonged exposure through contact or aerosolization. Other design considerations should be reviewed such as temperature and humidity control and waste processing [69]. Alternatively, if a low-power portable ultraviolet light unit is developed and proven effective, it could be used to reduce microbial contamination of environmental surfaces [70]. Other Risks Animals, which pose a risk of zoonotic infection to astronauts [71, 72], should undergo pretravel screening to minimize the risk of disease transmission [73] or, as is currently the case, should be pathogen-free animals. Policies and procedures that are carefully reviewed by veterinary experts in zoonoses should be in place, to include care of animals (eg, glove use when handling animals or when in potential contact with animal waste), handling animal waste, and housing. COUNTERMEASURES DURING SPACE TRAVEL Interventions for mitigating the risk of infection during space travel are described in this section (Table 2) Astronauts with signs or symptoms of respiratory tract infection should wear surgical masks to mitigate risk of transmission to other astronauts [74]. Cough etiquette should be adhered to, especially by those with upper respiratory tract symptoms when unmasked, for example, while eating. Consideration should be made for non-ill astronauts to wear fit-tested N-95 respirators if a companion astronaut has signs or symptoms of a respiratory tract infection and the causative pathogen is known to be transmitted by small aerosol particles [51–53]. Although alcohol-based hand-hygiene products are recommended for most earthbound healthcare settings [66, 75, 76], these products cannot be used in space because the alcohol would contaminate the drinking water supply through the humidity condensate. Therefore, the most effective waterless, nonalcohol-based hand-hygiene product for space travel (ie, potentially harmful vapors from the product can be removed by the air-handling system), such as benzalkonium chloride–based products, should be used. Chlorhexidine-based cloths [77], or possibly other cloth-based, nonalcohol-containing, US Food and Drug Administration–approved products, which are currently used in some school settings, should be considered based on efficacy and safety. The spacecraft or space habitat should be equipped with both nonsterile and sterile gloves, as well as topical (for skin or ocular use), oral, and intravenous antimicrobial agents. In addition, equipment for intravascular or bladder Table 2. Countermeasures during Spaceflight Currently Done by US National Aeronautics and Space Administration Astronaut • Surgical mask and cough etiquette • Fit-tested N95 respirator for other astronauts if respiratory illness caused by a pathogen that can be spread by small aerosol particle • Waterless hand-hygiene product • Germicidal wipes for cleaning high-touch, inanimate objectsb (eg, toileting device) • Gloves and gown for contact with potentially infectious material • Antimicrobial agents (topical [skin and ocular], oral, intravenous) • Intravenous catheter insertion equipment • Cutaneous antiseptic for minor surgeryb • Vitamin D supplementation • Regular exercise program Containment vessel • Intermittent quantitative sampling of air and potable water a Author’s suggestion. b If vapors can be safely removed by air-handling system. Not Done but Recommendeda • • • • • • • Not Done but Considera Source control (ie, surgical mask worn) by astronauts with upper respiratory infection Diagnostic testing capabilities for common viral and bacterial pathogens Glove use handling animals or if potential contact with animal waste Intravenous catheter infection prevention engineering controls (eg, chlorhexidine sponge dressingb) Electric toothbrush use Safety cabinet for sterile preparation of intravenous medications Sensor in bathroom; visual/audio cues if no hand hygiene performed catheterization that includes infection prevention engineering controls should be available [78, 79]. A cutaneous antiseptic to cleanse minor wounds, prep skin prior to insertion of an intravenous catheter, or be used during minor surgeries should be included. Astronauts routinely take a vitamin D supplement, which may enhance immune function [80] and reduce risk of reactivation of herpesviruses [81], and this practice should continue. Use of a powered toothbrush [82], or possibly use of a daily mouth rinse with chlorhexidine, may reduce risk of periodontal disease and should be considered [83]. However, as with daily use of cutaneous antiseptics, the unintended consequences of long-term use must be considered. Germicidal wipes for cleaning high-touch inanimate objects, such as the toileting device, are necessary. Toileting devices that come in contact with an astronaut’s skin should be cleaned after each use. Hand-hygiene compliance is important, particularly after a bowel movement, prior to food preparation, and similar activities. Input from human factors engineers will ensure ease of use of available products, thereby increasing compliance. Consideration could be made for a sensor in the bathroom with visual and/or audio cues to alert an astronaut who did not perform hand hygiene after using the bathroom facility [84]. Routine cleaning of the inanimate environment with a germicidal wipe is important, as outlined in a preflight infection control manual and currently performed on the International Space Station. Intermittent, quantitative air and water sampling should continue to be done to alert crew of defects in mitigation strategies. • • • Chlorhexidine daily mouth rinseb Probiotic ingestion Portable ultraviolet light machine to disinfect surfaces Regular exercise, which has been integrated into astronaut activity on the International Space Station, may improve immune function during spaceflight [85]. Ingestion of Lactobacillus reduces the bioburden of aerobic enteric flora [14] and, in addition to immunomodulatory effects [86], may reduce risk of infection [87]. In addition, intravaginal Lactobacillus administration reduces risk of recurrent urinary tract infections [88]. Thus, use of probiotics should be considered if found to be safe during prolonged human exposure to microgravity. Recent research has demonstrated that colonizing the skin and nares with extracellular serine protease (Esp)-producing S. epidermidis selectively inhibits S. aureus nasal colonization and biofilm formation [89]. As such, a somewhat farreaching countermeasure would involve colonizing astronauts’ nares prior to travel with ESP-producing S. epidermidis. An unmet need that is currently being investigated is for astronauts to have access to equipment needed to detect microbial pathogens-causing infections in order to direct appropriate therapeutic interventions and mitigate transmission risk. Challenges include testing for common viruses and bacteria, ease of use, durability of reagents, and output that does not require incubation. UNANSWERED QUESTIONS • Will prolonged spaceflight lead to changes in the risk of infections based on altered human immune function and bacterial physiology that were predicted by preflight studies? HEALTHCARE EPIDEMIOLOGY • CID 2013:56 (1 January) • 127 • What is the best antimicrobial coating for the containment vessel surfaces and water distribution and storage systems? This coating should be broad-spectrum, long-acting, and nonleachable, with a minimal likelihood of resistance developing among exposed microbes and no toxicity to humans despite prolonged exposure. • What is the most effective, acceptable antiseptic agent to be used for hand hygiene during space travel? • Does the benefit of gamma-irradiated food outweigh the potential detrimental effect on colonic microbial diversity and colonization resistance? • What diagnostic testing should be used during space travel? Enhanced diagnostic abilities during prolonged spaceflight, far beyond current symptom-based diagnoses, will be essential. Such testing must be clarified for instances when the above-noted countermeasures did not prevent such illnesses. • Why do microbes become more virulent in microgravity? How and why does the human immune system change under conditions found in space? A better understanding of these changes is of seminal importance and may afford us greater insight into our own evolution and lead us to unique therapeutic interventions not otherwise realized through experimentation on Earth. CONCLUSION Serious infections during space travel have been limited to date; many infections have been superficial skin infections (D. L. Pierson, personal communication). However, plans for human space travel lasting nearly 2 years are currently being discussed at NASA. At the same time, ongoing studies on the International Space Station and elsewhere [90] are attempting to assess the impact of prolonged human spaceflight on the immune system. If clinically significant immune dysfunction is documented, this, along with alterations in bacterial physiology during spaceflight, will create challenges to successful human missions. Attention to basic infection prevention and control practices should help to reduce the risk posed to astronauts. Research funding should be available to address transmission dynamics of microbes in microgravity and other unanswered questions. It is hoped that the present review offers some suggestions to mitigate such potential risk. SEARCH STRATEGY AND SELECTION CRITERIA References for this review were identified through searches of PubMed for articles published from January 1971 to June 2012, by use of the terms “microgravity,” “space travel,” 128 • CID 2013:56 (1 January) • HEALTHCARE EPIDEMIOLOGY “infection control,” “immune function,” “infection prevention,” “Lactobacillus,” “vaccination,” “Staphylococcus aureus screening and decolonization,” “Salmonella detection,” “latent tuberculosis detection,” “hand hygiene,” “zoonoses,” “prevention of gingivitis,” “vitamin D and immune function,” and “prevention of Legionnaires’ disease.” Articles resulting from these searches and relevant references cited in those articles were reviewed. Articles published in English were included. Notes Acknowledgments. This manuscript is based on a lecture given by the author at the NASA Microbiology Workshop, Johnson Space Center, Houston, Texas, 19 April 2011. The author gratefully acknowledges Duane Pierson, PhD, who critically reviewed the manuscript and made insightful suggestions, and Nicole Lundstrom for assistance in manuscript preparation. Potential conflicts of interest. The author has received research funding from Theravance and Pfizer and he has served as a consultant for Angiotech, Bard, Catheter Connections, Fresenius, ICU Medical, Semprus, and Teleflex. The author has submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed. References 1. Crucian B, Sams C. Immune system dysregulation during spaceflight: clinical risk for exploration-class missions. J Leukoc Biol 2009; 86:1017–8. 2. Nickerson CA, Ott CM, Wilson JW, Ramamurthy R, Pierson DL. Microbial response to microgravity and other low-shear environments. Microbiol Mol Biol Rev 2004; 68:345–61. 3. Wilson JW, Ott CM, Höner zu Bentrup K, et al. Spaceflight alters bacterial gene expression and virulence and reveals a role for global regulator Hfq. Proc Natl Acad Sci 2007; 104:16299–304. 4. Rosenzweig JA, Abogunde O, Thomas K, et al. Spaceflight and modeled microgravity effects on microbial growth and virulence. Appl Microbiol Biotechnol 2010; 85:885–91. 5. Crabbé A, Schurr MJ, Monsieurs P, et al. Transcriptional and proteomic responses of Pseudomonas aeruginosa PAO1 to spaceflight conditions involve Hfq regulation and reveal a role for oxygen. Appl Environ Microbiol 2011; 77:1221–30. 6. Kacena MA, Merrell GA, Manfredi B, et al. Bacterial growth in spaceflight: logistic growth curve parameters for Escherichia coli and Bacillus subtilis. Appl Microbiol Biotechnol 1999; 51:229–34. 7. Klaus D, Simske S, Todd P, Stodieck L. Investigation of spaceflight effects on Escherichia coli and a proposed model of underlying physical mechanisms. Microbiology 1997; 143(Pt 2):449–55. 8. Mauclaire L, Egli M. Effect of simulated microgravity on growth and production of exopolymeric substances of Micrococcus luteus space and earth isolates. FEMS Immunol Med Microbiol 2010; 59:350–6. 9. Sonnenfeld G. The immune system in space, including earth-based benefits of space-based research. Curr Pharm Biotechnol 2005; 6:343–9. 10. Crucian BE, Stowe RP, Pierson DL, Sams CF. Immune system dysregulation following short- vs long-duration spaceflight. Aviat Space Environ Med 2008; 79:835–43. 11. Guéguinou N, Huin-Schohn C, Bascove M, et al. Could spaceflightassociated immune system weakening preclude the expansion of human presence beyond Earth’s orbit? J Leukoc Biol 2009; 86:1027–38. 12. Cohrs RJ, Mehta SK, Schmid DS, Gilden DH, Pierson DL. Asymptomatic reactivation and shed of infectious varicella zoster virus in astronauts. J Med Virol 2008; 80:1116–22. 13. Taylor GR. Recovery of medically important microorganisms from Apollo astronauts. Aerosp Med 1974; 45:824–8. 14. Ilyin VK. Microbiological status of cosmonauts during orbital spaceflights on Salyut and Mir orbital stations. Acta Astronaut 2005; 56:839–50. 15. Ilyin VK. Drug resistance of E. coli isolated from cosmonauts. In: Hooke LR, Teeter R, Garshnek V, Rowe J, eds. USSR space life science digest NASA contractor report 3922(29). Washington, DC: NASA Office of Space Science and Applications, 1989:67. 16. Ilyin VK. Study of genetic characteristics and sensitivity to antibiotics of opportunistic microorganisms isolated in sealed environments. In: Stone LR, Rowe J, eds. USSR space life sciences digest NASA contractor report 3922(38). Washington, DC: NASA Office of Space Science and Applications, 1990:48. 17. Pierson DL, Mehta SK, Magee BB, Mishra SK. Person-to-person transfer of Candida albicans in the spacecraft environment. J Med Vet Mycol 1995; 33:145–50. 18. Pierson DL, Chidambarum M, Heath JD, et al. Epidemiology of Staphylococcus aureus in the Space Shuttle. FEMS Immunol Med Microbiol 1996; 16:273–81. 19. Klaus DM, Howard HN. Antibiotic efficacy and microbial virulence during spaceflight. Trends Biotechnol 2006; 24:131–6. 20. Decelle JG, Taylor GR. Autoflora in the upper respiratory tract of Apollo astronauts. Appl Environ Microbiol 1976; 32:659–65. 21. Ott CM, Bruce RJ, Pierson DL. Microbial characterization of free floating condensate aboard the Mir space station. Microb Ecol 2004; 47:133–6. 22. Kirkpatrick AW, Ball CG, Campbell M, et al. Severe traumatic injury during long duration spaceflight: light years beyond ATLS. J Trauma Manag Outcomes 2009; 3:4. 23. Crucian BE, Stowe RP, Ott CM, et al. Risk of crew adverse health event due to altered immune response. Human Research Program. Human health countermeasures element. National Aeronautics and Space Administration (NASA), Johnson Space Center, Houston, TX, 2009. 24. Heppener M. Spaceward ho! The future of humans in space. EMBO Rep 2008; 9(Suppl 1):S4–12. 25. Davidson JM, Aquino AM, Woodward SC, Wilfinger WW. Sustained microgravity reduces intrinsic wound healing and growth factor responses in the rat. FASEB J 1998; 13:325–9. 26. Lesnyak A, Sonnenfeld G, Avery L, et al. Effect of SLS-2 spaceflight on immunologic parameters of rats. J Appl Physiol 1996; 81:178–82. 27. Crucian BE, Cabbages ML, Sams CF. Altered cytokine production by specific human peripheral blood cell subsets immediately following spaceflight. J Interferon Cytokine Res 2000; 20:547–56. 28. Kaur I, Simons ER, Castro VA, Mark Ott C, Pierson DL. Changes in neutrophil functions in astronauts. Brain Behav Immun 2004; 18: 443–50. 29. Kaur I, Simons ER, Castro VA, Ott CM, Pierson DL. Changes in monocyte functions of astronauts. Brain Behav Immun 2005; 19:547–54. 30. Crucian B, Stowe R, Quiriarte H, Pierson D, Sams C. Monocyte phenotype and cytokine production profiles are dysregulated by shortduration spaceflight. Aviat Space Environ Med 2011; 82:857–62. 31. Nash PV, Konstantinova IV, Fuchs BB, Rakhmilevich AL, Lesnyak ATMastro AM. Effect of spaceflight on lymphocyte proliferation and interleukin-2 production. J Appl Physiol 1992; 73(2 Suppl): 186S–90. 32. Sonnenfeld G, Mandel AD, Konstantinova IV, et al. Spaceflight alters immune cell function and distribution. J Appl Physiol 1992; 73(2 Suppl):191S–5. 33. Sonnenfeld G, Davis S, Taylor GR, et al. Effect of spaceflight on cytokine production and other immunologic parameters of rhesus monkeys. J Interferon Cytokine Res 1996; 16:409–15. 34. Boonyaratanakornkit JB, Cogoli A, Li CF, et al. Key gravity-sensitive signaling pathways drive T cell activation. FASEB J 2005; 19:2020–2. 35. Buravkova LB, Rykova MP, Grigorieva V, Antropova EN. Cell interactions in microgravity: cytotoxic effects of natural killer cells in vitro. J Gravit Physiol 2004; 11:177–80. 36. Taylor GR, Janney RP. In vivo testing confirms a blunting of the human cell-mediated immune mechanism during spaceflight. J Leuk Biol 1992; 51:129–32. 37. Gmünder FK, Konstantinova I, Cogoli A, Lesnyak A, Bogomolov W, Grachov AW. Cellular immunity in cosmonauts during long duration spaceflight on board the orbital MIR station. Aviat Space Environ Med 1994; 65:419–23. 38. Salzman NH. Microbiota-immune system interaction: an uneasy alliance. Curr Opin Microbiol 2011; 14:99–105. 39. Bailey MT, Dowd SE, Galley JD, Hufnagle AR, Allen RG, Lyte M. Exposure to a social stressor alters the structure of the intestinal microbiota: implications for stressor-induced immunomodulation. Brain Behav Immun 2011; 25:397–407. 40. Tixador R, Richoilley G, Gasset G, et al. Preliminary results of Cytos 2 experiment. Acta Astronaut 1985; 12:131–4. 41. Tixador R, Richoilley G, Gasset G, et al. Study of minimal inhibitory concentration of antibiotics on bacteria cultivated in vitro in space (Cytos 2 experiment). Aviat Space Environ Med 1985; 56:748–51. 42. Lapchine L, Moatti N, Gasset G, Richoilley G, Templier J, Tixador R. Antibiotic activity in space. Drugs Exp Clin Res 1986; 12:933–8. 43. Sieradzki K, Tomasz A. Alterations of cell wall structure and metabolism accompany reduced susceptibility to vancomycin in an isogenic series of clinical isolates of Staphylococcus aureus. J Bacteriol 2003; 185:7103–10. 44. Tixador R, Gasset G, Eche B, et al. Behavior of bacteria and antibiotics under space conditions. Aviat Space Environ Med 1994; 65:551–6. 45. Ciferri O, Tiboni O, Di Pasquale G, Orlandoni AM, Marchesi ML. Effects of microgravity on genetic recombination in Escherichia coli. Naturwissenschaften 1986; 73:418–21. 46. Crabbé A, De Boever P, Van Houdt R, Moors H, Mergeay M, Cornelis P. Use of the rotating wall vessel technology to study the effect of shear stress on growth behaviour of Pseudomonas aeruginosa PA01. Environ Microbiol 2008; 10:2098–110. 47. Nickerson CA, Ott CM, Mister SJ, Morrow BJ, Burns-Keliher L, Pierson DL. Microgravity as a novel environmental signal affecting Salmonella enterica serovar Typhimurium virulence. Infect Immun 2000; 68:3147–52. 48. Lynch SV, Mukundakrishnan K, Benoit MR, Ayyaswamy PS, Matin A. Escherichia coli biofilms formed under low-shear modeled microgravity in a ground-based system. Appl Environ Microbiol 2006; 72:7701–10. 49. Horneck G, Klaus DM, Mancinelli RL. Space microbiology. Microbiol Mol Biol R 2010; 74:121–56. 50. Novikova ND. Review of the knowledge of microbial contamination of the Russian manned spacecraft. Microb Ecol 2004; 47:127–32. 51. Weber TP, Stilianakis NI. Inactivation of influenza A viruses in the environment and modes of transmission: a critical review. J Infect 2008; 57:361–73. 52. Lindsley WG, Blachere FM, Thewlis RE, et al. Measurements of airborne influenza virus in aerosol particles from human coughs. PLoS One 2010; 5:e15100. 53. Mermel LA. Preventing the spread of influenza A H1N1 2009 to health-care workers. Lancet Infect Dis 2009; 9:723–4. (Erratum in: Lancet Infect Dis 2010; 10:16). 54. Bassetti S, Bischoff WE, Walter M, et al. Dispersal of Staphylococcus aureus into the air associated with a rhinovirus infection. Infect Control Hosp Epidemiol 2005; 26:196–203. 55. Gehanno JF, Louvel A, Nouvellon M, Caillard JF, Pestel-Caron M. Aerial dispersal of methicillin-resistant Staphylococcus aureus in hospital rooms by infected or colonised patients. J Hosp Infect 2009; 71:256–62. HEALTHCARE EPIDEMIOLOGY • CID 2013:56 (1 January) • 129 56. Diel R, Loddenkemper R, Nienhaus A. Predictive value of interferongamma release assays and tuberculin skin testing for predicting progression from latent TB infection to disease state: a meta-analysis. Chest 2012; 142:63–75. 57. Lauderdale TL, Wang JT, Lee WS, et al. Carriage rates of methicillinresistant Staphylococcus aureus (MRSA) depend on anatomic location, the number of sites cultured, culture methods, and the distribution of clonotypes. Eur J Clin Microbiol Infect Dis 2010; 29:1553–9. 58. Mermel LA, Cartony JM, Covington P, Maxey G, Morse D. Methicillin-resistant Staphylococcus aureus colonization at different body sites: a prospective, quantitative analysis. J Clin Microbiol 2011; 49:1119–21. 59. Peterson LR, Liesenfeld O, Woods CW, et al. Multicentered evaluation of the LightCycler methicillin-resistant Staphylococcus aureus (MRSA) advanced test as a rapid method for detection of MRSA in nasal surveillance swabs. J Clin Microbiol 2010; 48:1161–6. 60. Verhoeven PO, Grattard F, Carricajo A, et al. An algorithm based on one or two nasal samples is accurate to identify persistent nasal carriers of Staphylococcus aureus. Clin Microbiol Infect 2012; 18:551–7. 61. Buehlmann M, Frei R, Fenner L, Dangel M, Fluckiger U, Widmer AF. Highly effective regimen for decolonization of methicillin-resistant Staphylococcus aureus carriers. Infect Control Hosp Epidemiol 2008; 29:510–6. 62. Simor AE, Daneman N. Staphylococcus aureus decolonization as a prevention strategy. Infect Dis Clin N Am 2009; 23:133–51. 63. Mollema FP, Severin JA, Nouwen JL, Ott A, Verbrugh HA, Vos MC. Successful treatment for carriage of methicillin-resistant Staphylococcus aureus and importance of follow up. Antimicrob Agents Chemother 2010; 54:4020–25. 64. Williams FM, Markides V, Edgeworth J, Williams AJ. Reactivation of coccidioidomycosis in a fit American visitor. Thorax 1998; 53:811–2. 65. McCall CE, Martin WT, Boring JR. Efficiency of cultures of rectal swabs and faecal specimens in detecting Salmonella carriers: correlation with numbers of salmonellas excreted. J Hyg (Lond) 1966; 64:261–9. 66. Pittet D, Allegranzi B, Boyce J, World Health Organization World Alliance for Patient Safety First Global Patient Safety Challenge Core Group of Experts. The World Health Organization guidelines on hand hygiene in health care and their consensus recommendations. Infect Control Hosp Epidemiol 2009; 30:611–22. 67. Mermel LA, Josephson SL, Dempsey J, Parenteau S, Perry C, Magill N. Outbreak of Shigella sonnei in a clinical microbiology laboratory. J Clin Micro 1997; 35:3163–5. 68. Lichter JA, Van Vliet KJ, Rubner MF. Design of antibacterial surfaces and interfaces: polyelectrolyte multilayers as a multifunctional platform. Macromolecules 2009; 42:8573–86. 69. Czupalla M, Aponte V, Chappell S, Klaus D. Analysis of a spacecraft life support system for a Mars mission Acta Astronaut 2004; 55:537–47. 70. Rutala WA, Gergen MF, Weber DJ. Room decontamination with UV radiation. Infect Control Hosp Epidemiol 2010; 31:1025–9. 71. Weber DJ, Rutala WA. Risks and prevention of nosocomial transmission of rare zoonotic diseases. Clin Infect Dis 2001; 32:446–56. 72. Chomel BB, Sun B. Zoonoses in the bedroom. Emerg Infect Dis 2011; 17:167–72. 73. Lefebvre SL, Waltner-Toews D, Peregrine A, Reid-Smith R, Hodge L, Weese JS. Characteristics of programs involving canine visitation of hospitalized people in Ontario. Infect Control Hosp Epidemiol 2006; 27:754–8. 130 • CID 2013:56 (1 January) • HEALTHCARE EPIDEMIOLOGY 74. Johnson DF, Druce JD, Birch C, Grayson ML. A quantitative assessment of the efficacy of surgical and N95 masks to filter influenza virus in patients with acute influenza infection. Clin Infect Dis 2009; 49:275–7. 75. Boyce JM, Pittet D, Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Morb Mortal Wkly Rep 2002; 51(RR-16):1–45. 76. Tschudin-Sutter S, Pargger H, Widmer AF. Hand hygiene in the intensive care unit. Crit Care Med 2010; 38(8 Suppl):S299–305. 77. Kassakian SZ, Mermel LA, Jefferson JA, Parenteau SL, Machan JT. Impact of chlorhexidine bathing on hospital-acquired infections among general medical patients. Infect Control Hosp Epidemiol 2011; 32:238–43. 78. O’Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis 2011; 52:e162–93. 79. Gould CV, Umscheid CA, Agarwal RK, Kuntz G, Pegues DA, Healthcare Infection Control Practices Advisory Committee. Guideline for the prevention of catheter-associated urinary tract infection 2009. Infect Control Hosp Epidemiol 2010; 31:319–26. 80. Martineau AR, Timms PM, Bothamley GH, et al. High-dose vitamin D(3) during intensive-phase antimicrobial treatment of pulmonary tuberculosis: a double-blind randomised controlled trial. Lancet 2011; 377:242–50. 81. Zwart SR, Mehta SK, Ploutz-Snyder R, et al. Response to vitamin D supplementation during Antarctic winter is related to BMI, and supplementation can mitigate Epstein-Barr virus reactivation. J Nutr 2011; 141:692–7. 82. Rosema NA, Timmerman MF, Versteeg PA, et al. Comparison of the use of different modes of mechanical oral hygiene in prevention of plaque and gingivitis. J Periodontol 2008; 79:1386–94. 83. Gunsolley JC. Clinical efficacy of antimicrobial mouthrinses. J Dent 2010; 38:S6–10. 84. Nevo I, Fitzpatrick M, Thomas RE, et al. The efficacy of visual cues to improve hand hygiene compliance. Simul Healthc 2010; 5:325–31. 85. Shearer WT, Ochs HD, Lee BN, et al. Immune responses in adult female volunteers during the bed-rest model of spaceflight: antibodies and cytokines. J Allergy Clin Immunol 2009; 123:900–5. 86. Makino S, Ikegami S, Kano H, et al. Immunomodulatory effects of polysaccharides produced by Lactobacillus delbrueckii ssp. Bulgaricus OLL1073R-1. J Dairy Sci 2006; 89:2873–81. 87. Hojsak I, Snovak N, Abdović S, Szajewska H, Misak Z, Kolacek S. Lactobacillus GG in the prevention of gastrointestinal and respiratory tract infections in children who attend day care centers: a randomized, double-blind, placebo-controlled trial. Clin Nutr 2010; 29:312–6. 88. Stapleton AE, Au-Yeung M, Hooton TM, et al. Randomized, placebocontrolled phase 2 trial of a Lactobacillus crispatus probiotic given intravaginally for prevention of recurrent urinary tract infection. Clin Infect Dis 2011; 52:1212–7. 89. Iwase T, Uehara Y, Shinji H, et al. Staphylococcus epidermidis Esp inhibits Staphylococcus aureus biofilm formation and nasal colonization. Nature 2010; 465:346–9. 90. Frey MA. Protecting astronauts from infectious disease during longduration space missions. Aviat Space Environ Med 2010; 81:433–4.