Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
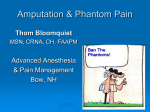
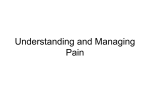
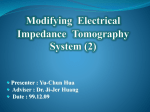
REVIEWS Phantom limb pain: a case of maladaptive CNS plasticity? Herta Flor*, Lone Nikolajsen‡ and Troels Staehelin Jensen§ Abstract | Phantom pain refers to pain in a body part that has been amputated or deafferented. It has often been viewed as a type of mental disorder or has been assumed to stem from pathological alterations in the region of the amputation stump. In the past decade, evidence has accumulated that phantom pain might be a phenomenon of the CNS that is related to plastic changes at several levels of the neuraxis and especially the cortex. Here, we discuss the evidence for putative pathophysiological mechanisms with an emphasis on central, and in particular cortical, changes. We cite both animal and human studies and derive suggestions for innovative interventions aimed at alleviating phantom pain. *Department of Clinical and Cognitive Neuroscience, University of Heidelberg, Central Institute of Mental Health, D-68159 Mannheim, Germany. ‡Department of Anesthesiology and Danish Pain Research Center, § Department of Neurology and Danish Pain Research Center, Aarhus University Hospital, DK-8000 Aarhus C, Denmark. Correspondence to H.F. e-mail: [email protected] doi:10.1038/nrn1991 The amputation or deafferentation of a limb or another body part is usually followed by a global feeling that the missing limb is still present (phantom limb awareness), as well as specific sensory and kinaesthetic sensations (phantom sensations)1. These non-painful phantom phenomena are reported by almost all amputees 2. Phantom limb pain, or phantom pain, belongs to a group of neuropathic pain syndromes that is characterized by pain in the amputated limb or pain that follows partial or complete deafferentation. Phantom pains have also been observed as a consequence of the loss of other body parts such as the breast3, and can occur following spinal cord injury4,5. Residual limb (or stump) pain and non-painful residual limb phenomena are sensations in the still-present body part adjacent to the amputation or deafferentation line. Phantom pain has many features: at one end of the spectrum it is limited to simple, short-lasting and rarely occurring painful shocks in a missing body part; at the other end of the spectrum it can be a constant, excruciatingly painful experience during which the individual has a vivid and intense perception of the missing body part. It seems to be more severe in the distal portions of the phantom and can have a number of characteristics such as stabbing, throbbing, burning or cramping6. Its onset can be immediate, but it may also appear for the first time many years after the amputation2. Several factors can affect the occurrence and extent of phantom pain. Pre- and postoperative pain can influence subsequent phantom limb pain, and it can be difficult to differentiate postoperative, residual limb and phantom limb pain, especially in the early post-amputation phase. Perioperative pain management has improved NATURE REVIEWS | NEUROSCIENCE during the past two decades and now includes both peripheral and central analgesia, but this change in treatment strategy has not resulted in a corresponding reduction of phantom pain2; phantom limb pain still occurs in 50–80% of amputees irrespective of whether the amputation is traumatic or performed for medical reasons, and therefore remains a significant problem7,8. In Western countries, the main reason for amputation is chronic vascular disease. The patients are elderly and have often suffered from long-lasting pre-amputation pain. In other parts of the world, civil wars and landmine explosions result in many unfortunate cases of traumatic amputations in otherwise healthy people9. It is possible that the occurrence and nature of phantom limb pain might differ depending on whether amputation was carried out for chronic or traumatic reasons, although so far there are insufficient data to draw firm conclusions about this7. Interestingly, phantom limb pain is more frequent when the amputation occurs in adulthood, less frequent in child amputees and virtually non-existent in congenital amputees10,11. Phantom limb pain could be related to a certain position or movement of the phantom, and might be elicited or exacerbated by a range of physical factors (for example, changes in the weather or pressure on the residual limb) and psychological factors (for example, emotional stress)12. The long-term course of phantom limb pain is unclear. Whereas some authors report a slight decline in pain prevalence over the course of several years13, others have described high prevalence rates in long-term amputees8. As discussed below, central as well as peripheral factors have been implicated as determinants of phantom limb pain: the clinical characteristics of phantom pain and VOLUME 7 | NOVEMBER 2006 | 873 © 2006 Nature Publishing Group REVIEWS empirical data on central factors, including reports on the effect of brain lesions on phantoms14, suggest that it cannot be completely explained by peripheral mechanisms2. Psychological factors such as anxiety or depression do not seem to be a primary cause, but they might well affect the onset, course and the severity of the pain6,8. Here, we review evidence that has accumulated over the past decade showing that multiple changes along the neuraxis contribute to the experience of phantom limb pain and that cortical changes have a special role. Neuroma When a limb is severed, a terminal swelling or ‘endbulb’ is formed and axonal sprouting occurs. In the case of an amputation, sprouting and endbulb formation lead to a neuroma, a tangled mass that forms when the axons cannot reconnect or can only partially reconnect, as is the case in partial lesions. These neuromas generate abnormal activity that is called ectopic because it does not originate from the nerve endings. Dorsal root ganglion A nodule on a dorsal root that contains cell bodies of afferent spinal neurons, which convey somatosensory input to the CNS. Paraesthesia An abnormal skin sensation such as tingling or itching. Peripheral changes Amputees often report pain and sensitivity to vibration and touch in the nerve that innervated the amputated limb or in the residual limb adjacent to the amputation line. A classic feature following complete or partial nerve injury is the presence of the Tinel sign, which refers to the local or referred pain (pain in the innervation territory of the damaged nerve) that occurs in response to brief mechanical stimulation of an injured nerve. Similarly, tapping of stump neuromas can cause pain in the phantom limb and in the stump2. Following experimental injury to nerves, axotomized afferent neurons show retrograde degeneration and shrinking, primarily involving unmyelinated neurons15. As a consequence of injury, terminal swelling and regenerative sprouting of the injured axon end occurs and neuromas form in the residual limb that display spontaneous and abnormal evoked activity to mechanical and chemical stimuli16. Ectopic discharges from stump neuromas represent a source of abnormal afferent input to the spinal cord and a potential mechanism for spontaneous pain and abnormal evoked pains17. Ectopic discharge from myelinated axons seems to begin earlier and tends to be rhythmic, whereas C-fibres tend to show slow, irregular patterns18. The increased excitability of injured nerves that results in ectopic discharge seems to be due to alterations in the electrical properties of cellular membranes. These alterations involve the upregulation or novel expression, and altered trafficking, of voltage-sensitive sodium channels and decreased potassium channel expression, as well as altered transduction molecules for mechano-, heat and cold sensitivity in the neuromas19,20. In addition, experimental injury causes the expression of novel receptors in the neuroma that are sensitive to cytokines, amines and so on, which might enhance nociceptive processing18. Non-functional connections between axons (ephapses) might also contribute to the spontaneous activity21. Nyström and Hagbarth22 carried out a classic microneurographic study in which tapping of neuromas in two amputees was associated with increased activity in afferent C-fibres and an increased pain sensation. They also found that anaesthetic blockade of neuromas eliminated spontaneous and stimulation-induced nerve activity related to the stump, but not ongoing phantom limb pain. Moreover, phantom limb pain is often present soon after amputation, before a palpable, swollen neuroma could have formed2. These findings motivated a search for other potential sources of ectopic activity in the PNS that are more proximal to the residual limb. 874 | NOVEMBER 2006 | VOLUME 7 An additional site of ectopic discharge is the dorsal (DRG). Ectopic discharges originating in the DRG can summate with ectopic activity from neuromas in the stump. Indeed, processes such as crossexcitation can lead to the depolarization and activation of neighbouring neurons, significantly amplifying the overall ectopic barrage18. Spontaneous as well as triggered sympathetic discharge can elicit and exacerbate ectopic neuronal activity from neuromas as well as at the level of the DRG23. This could account for the frequent exacerbation of phantom pain at times of emotional distress24. Additional factors such as temperature, oxygenation level and local inflammation in neuromas and associated DRGs might also have a role. In animal studies, nerve injury-induced sensory– sympathetic coupling with sympathetic sprouting into the DRGs has been described, although the role of this phenomenon in phantom limb pain is not clear18. In some patients, the sympathetic maintenance of phantom limb pain is supported by evidence that systemic adrenergic blocking agents sometimes reduce phantom limb pain25. Similarly, injections of adrenaline into stump neuromas have been shown to increase phantom limb pain and paraesthesias in some amputees25. Although sympathetically maintained pain does not necessarily covary with regional sympathetic abnormalities, in some patients sympathetic dysregulation in the residual limb is apparent. For example, a microneurographic study of sympathetic fibres in skin (but not deep somatic) nerves in human lower limb amputees26 showed abnormal sympathetic activity in the lower limb; however, none of these individuals suffered from phantom limb pain. It might be that deep somatic fibres could have a greater role in phantom pain, although these were not studied here. So, damaged and reorganized nerve endings together with an altered activity in the DRG represent a potential source of pain and abnormal evoked activity in nerve injury, including phantom limb pain. root ganglion Central changes: the spinal cord Local anaesthesia of the stump or the plexus, or epidural anaesthesia, do not eliminate ongoing phantom limb pain in all amputees27,28; for example, 50% of the amputees in a study involving anaesthesia of the brachial plexus27 were pain-free, suggesting the involvement of more central factors. Anecdotal evidence in human amputees was the first to indicate that spinal mechanisms might have a role in phantom limb pain. For example, during spinal anaesthesia, phantom pains have been reported to occur in patients who were pain-free at the time of the procedure29. Although direct evidence for spinal changes in human amputees is lacking, experimental data based on animal models of nerve injury are becoming available that point towards an important role for CNS processes in neuropathic pain. Increased activity in peripheral nociceptors related to inflammatory pain leads to an enduring change in the synaptic responsiveness of neurons in the dorsal horn of the spinal cord, a process known as central sensitization30. Central hyperexcitability similar to sensitization might also be triggered by nerve injury, as occurs www.nature.com/reviews/neuro © 2006 Nature Publishing Group REVIEWS Microglia Glial cells are the ‘glue’ of the nervous system, and support and protect the neurons. Microglia are a special form of small glial cells; they have immune functions and can be involved in inflammatory actions. Substance P A neuropeptide that plays an important role in nociception and is released by the primary somatosensory afferents in the spinal cord. C-afferents Unmyelinated fibres, 0.4–1.2 μm in diameter, conducting nerve impulses at a velocity of 0.7–2.3 ms–1. They conduct secondary, delayed pain. Aδ afferents Thinly myelinated nerve fibres with a conduction velocity of 10–30 ms–1 that convey nociceptive information to the spinal cord. These receptors convey first, sharp, pricking pain and are located mainly on hairy skin. Aβ fibres Large-diameter myelinated fibres that have a conduction velocity of ~40 ms–1 and normally carry non-nociceptive information. during amputation. For example, spinal changes associated with nerve injury include increased firing of the dorsal horn neurons, structural changes at the central endings of the primary sensory neurons and reduced spinal cord inhibitory processes31. Inhibitory GABA (γ-aminobutyric acid)-containing and glycinergic interneurons in the spinal cord could be destroyed by rapid ectopic discharge or other effects of axotomy32, or might change from having an inhibitory to an excitatory effect under the influence of brain-derived neurotrophic factor (BDNF) released from microglia33, thereby contributing to a hyperexcitable spinal cord. Another CNS process that might contribute to the hyperexcitability of spinal cord circuitry following major nerve damage is that of the downregulation of opioid receptors, on both primary afferent endings and intrinsic spinal neurons34. This is expected to add to disinhibition due to the reduction of normally inhibitory GABA and glycine activity. In addition, cholecystokinin35, an endogenous inhibitor of the opiate receptor, is upregulated in injured tissue, thereby exacerbating this effect of disinhibition. Changes that might trigger abnormal firing have also been noted in ascending projection neurons from the spinal cord to supraspinal centres. These changes depend on the cascade of biological events that takes place in the spinal cord after peripheral nerve damage. Part of this sensitization is due to, for example, inflammation-induced facilitation of the response of NMDA (N-methyl-d-aspartate) receptors to the primary afferent neurotransmitter glutamate36. A remarkable effect of the spinal changes evoked by nerve injury is that low-threshold afferents can become functionally connected to ascending spinal projection neurons that carry nociceptive information to supraspinal centres. Substance P is normally expressed only by C-afferents and Aδ afferents, most of which are nociceptors. The injury-triggered expression of substance P by Aβ fibres could render them more like nociceptors. For example, it might permit ectopic or normal activity in Aβ fibres to trigger and maintain central sensitization. When this happens, normally innocuous A-fibre input from the periphery, ectopic input and input from residual intact low-threshold afferents might contribute to phantom pain sensation37. Following peripheral nerve injury, degeneration of central projection axons occurs. Massive deafferentation is observed when dorsal roots are injured, or cut off from the spinal cord. Deafferentation could act hand-in-hand with the central effects of peripheral denervation to bring about the changes that contribute to spinal hyperexcitability. A mechanism that might be of special relevance to phantom phenomena is the invasion of regions of the spinal cord that are functionally vacated by injured afferents. For example, in the neuroma model in rats and cats, there is an expansion of receptive fields on skin adjacent to the denervated part of the limb, and a shift of activity from these adjacent areas into regions of the spinal cord that previously served the part of the limb that was functionally deafferented by the nerve lesion38. In amputees and patients with severed cervical nerve roots, signs of NATURE REVIEWS | NEUROSCIENCE hyperexcitability can be demonstrated in dermatomes adjacent to the denervated limb part, possibly indicating the spread of spinal hyperexcitability from denervated segments to segments immediately rostral and caudal to the denervated zone (T.S.J. et al., unpublished observations). Such reorganization of the spinal map of the limb, which could be due to the unmasking of previously silent connections, is also reflected in brainstem and cortical remapping (see below). Central changes: brainstem, thalamus, cortex A number of observations in amputees indicate that supraspinal changes could be important. For example, paraplegic individuals with high spinal cord injuries can experience pain in the lower part of the body4, although the relevance of this phenomenon for phantom pain after amputation is not clear. Moreover, spinal anaesthesia does not always eliminate ongoing phantom limb pain28. In primates, the spinal cord forms only 2% of the CNS compared with 15% in rats39, suggesting an important role for supraspinal mechanisms in plastic changes in the primate CNS. It is possible that spinal changes contribute to supraspinal changes, although the extent of the contribution is unclear. Supraspinal changes related to phantom limb pain involve the brainstem, thalamus and cerebral cortex. For example, there is evidence that axonal sprouting in the cortex is involved in the reorganizational changes observed in amputated monkeys40. Thalamic stimulation and recordings in human amputees have revealed that reorganizational changes might also occur at the thalamic level and are closely related to the perception of phantom limbs and phantom limb pain41. Studies in monkeys have shown that changes in the cortex might be relayed from the brainstem and thalamus42–45; however, alterations at the subcortical level could also originate in the cortex, which has strong efferent connections to the thalamus and lower structures 46,47. FIGURE 1 summarizes the putative contributions of peripheral, spinal and supraspinal processes in phantom limb pain. Cortical reorganization. New insights into phantom limb pain have come from studies demonstrating changes in the functional and structural architecture of the primary somatosensory (SI) cortex subsequent to amputation and deafferentation in adult monkeys. In these studies, the amputation of digits in an adult owl monkey led to an invasion of adjacent areas into the representation zone of the deafferented fingers48, as revealed by microelectrode recordings. Pons et al.49 reported an even greater cortical reorganization following deafferentiation of the dorsal root (dorsal rhizotomy), with the representation of the cheek in the SI cortex taking over the cortical arm and hand representation in the range of centimetres. On the basis of these findings, Ramachandran et al.50 suggested that referred sensations in the phantom (that is, painful and non-painful phantom sensations that can be elicited by stimulating body areas adjacent to but also far removed from the amputated limb) are a perceptual correlate of reorganizational processes in VOLUME 7 | NOVEMBER 2006 | 875 © 2006 Nature Publishing Group REVIEWS Normal Reorganized Central changes • Unmasking • Sprouting • General disinhibition • Map remodelling • Loss of neurons and neuronal function • Denervation • Alterations in neuronal and glial activity • Sensory–motor and sensory–sensory incongruence Peripheral changes • Structural changes in neurons and axons • Ectopic impulses • Ephaptic transmission • Sympathetic–afferent coupling • Down- and upregulation of transmitters • Alterations in channels and transduction molecules • Selective loss of unmyelinated fibres Figure 1 | A schematic diagram of the areas involved in the generation of phantom limb pain and the main peripheral and central mechanisms. The peripheral areas include the residual limb and the dorsal root ganglion, and the central areas include the spinal cord and supraspinal centres such as the brainstem, thalamus, cortex and limbic system. The proposed mechanisms associated with phantom pain are listed for the PNS and CNS. the SI cortex (see also Cronholm51). In support of this, they showed a point-to-point correspondence between stimulation sites and areas of sensation from the mouth to the phantom in arm amputees (that is, a “thumb in cheek”52 map of stimulation sites on the face and corresponding sensation in the phantom hand). They called this phenomenon topographical remapping, assuming that it was based on parallel processes in the SI cortex. However, it was shown that referred phantom sensations in arm amputees can be elicited from the toe53, which is far removed from the representation of the arm in the SI cortex, which suggests that other areas could be involved in the generation of referred sensation. It has been reported that topographical referred phantom sensations occur in only a small percentage of amputees54, whereas phantom limb pain is common; this suggests that referred phantom sensation and phantom pain might be related to different central processes. Moreover, Halligan et al.55 showed that topographical remapping can completely change over time. Imaging studies have reported that upper extremity amputees actually show a shift of the mouth into the hand representation in the SI cortex56,57. Another study58 provided evidence that these cortical changes are less related to referred phantom sensations, but rather have a close association with phantom limb pain (FIG. 2). The larger the shift of the mouth representation into the zone that formerly represented the arm, the more pronounced the phantom limb pain. These reorganizational shifts in the SI cortex have been replicated in several studies54,59 and have also been described for the motor cortex60,61, where a similar close association between map reorganization and the magnitude of phantom limb pain was described62–64. Computational models of deafferentation and related phenomena have suggested that peripheral factors can enhance the central reorganization of neuronal networks. Therefore, abnormal noise-like input that might originate 876 | NOVEMBER 2006 | VOLUME 7 from a neuroma in the residual limb could greatly enhance the amount of central map reorganization65. Map reorganization might also be enhanced by the selective loss of C-fibres that occurs after amputation18, as C-fibres seem to have a special role in the maintenance of cortical maps66. The extent of reorganizational changes along the neuraxis might depend greatly on the developmental stage of the CNS. The consequences of limb amputation have been compared in the cortex, brainstem and dorsal horn in adult and juvenile rats, and have shown that amputation in adulthood leads mainly to cortical changes whereas amputation at a younger age causes more comprehensive reorganization along the neuraxis67. Several stages of cortical reorganization can be differentiated68,69. The first relates to the unmasking of normally inhibited connections. Unmasking of latent excitatory synapses can be secondary to the increased release of excitatory neurotransmitters, increased density of postsynaptic receptors, changes in conductance of the neuronal membrane, decreased inhibitory inputs or the removal of inhibition from excitatory inputs70. The data suggest that the excitatory activation could be the result of loss of GABA-mediated inhibition71,72. In fact, several studies have shown enhanced cortical excitability in patients with phantom limb pain73,74. A second stage involves structural changes such as axonal sprouting, as well as alterations in synaptic strength. Finally, use-dependent plasticity might lead to additional changes based on Hebbian learning and long-term potentiation75. Alterations in sensory and motor feedback. Research into illusory perceptions, such as the perception of body ownership of a rubber hand76 (BOX 1) has shown that not only the SI cortex but also frontal and parietal areas are involved in the perception of abnormal somatosensory phenomena, and might also have a role in phantom sensation and phantom pain. It has been suggested that www.nature.com/reviews/neuro © 2006 Nature Publishing Group REVIEWS Phantom limb pain Amputees without pain Healthy controls Figure 2 | Cortical changes related to phantom limb pain. Functional MRI data from seven patients with phantom limb pain, seven amputees without pain and seven healthy controls during a lip pursing task. Activation in primary somatosensory and motor cortices is unaltered in amputees without pain and is similar to that of healthy controls. In the amputees with phantom limb pain the cortical representation of the mouth extends into the region of the hand and arm. Reproduced, with permission, from REF. 64 © (2001) Oxford Univ. Press. abnormal painful sensations might be related to the incongruence of motor intention and sensory feedback and a corresponding activation of frontal and parietal brain areas77. In line with this suggestion, one study used a mirror to create a discrepancy between actual and seen movement (movement seen in the mirror is discrepant from the movement behind the mirror if both arms perform asynchronous movements) 78. The authors reported the presence of painful and non-painful paraesthesias as a consequence of the incongruent movement condition and suggested that sensorimotor incongruence might cause the abnormal sensations seen in many neuropathic pain syndromes. However, it has been pointed out that this was not a controlled study, and that the role of these central disturbances in perceptual and motor processing for phantom pain and phantom phenomena remains to be determined79. Telescoping is another phenomenon that is frequently observed in amputees and refers to perceived changes in the size and length of the phantom, which can even retract into the stump (FIG. 3) . Whereas telescoping was previously thought to be a sign of adaptive plasticity, it is actually related to increased levels of phantom pain54. The research into illusory perceptions and imagery in other sensory domains has shown that the primary cortical areas respond to the perceived and not the actual input into the respective sensory system80. Extended phantoms might therefore provide ongoing motor and sensory feedback to the area that previously represented the amputated limb, whereas telescoped phantoms activate areas remote from the limb representation. So, the continued perception of extended phantoms might reverse maladaptive cortical changes. Functional MRI data from subjects with varying degrees of telescoping show that the cortical representation of the phantom movement actually follows the location of the perceived movement and is not statically fixed in the cortical representation zone of the hand (H.F. et al., unpublished observations) (FIG. 3). These data support the notion that visual, sensory and motor feedback to the cortex might be an important determinant of phantom NATURE REVIEWS | NEUROSCIENCE limb phenomena and pain that needs to be further investigated. These hypotheses might also be important for our understanding of chronic painful and non-painful symptoms in both neuropathic and other types of pain in general. The pain memory hypothesis. Sometimes pain in the phantom is similar to the pain that existed in the limb prior to amputation. The likelihood of this ranges from 10–79% in different reports, and depends on the type and time of assessment81,82. It has been proposed that pain memories established prior to the amputation are powerful elicitors of phantom limb pain83,84. Pain memories might be implicit; the term implicit pain memory refers to central changes related to nociceptive input that lead to subsequent altered processing of the somatosensory system and do not require changes in conscious processing of the pain experience85. In patients with chronic back pain, it was shown that increasing chronicity is correlated with an increase in the representation zone of the back in the SI cortex, and it was also reported that the experience of acute pain alters the map in the SI cortex86. These data indicate that long-lasting noxious input might lead to long-term changes at the central, and especially at the cortical, levels that affect the later processing of somatosensory input. It has long been known that the SI cortex is involved in the processing of pain and that it might be important for the sensory–discriminative aspects of the pain experience87. There have also been reports that phantom limb pain was abolished after the surgical removal of portions of the SI cortex, and that stimulation of this area evoked phantom limb pain88,89. If a somatosensory pain memory has been established with an important neural correlate in spinal and supraspinal structures, such as in the SI cortex, subsequent deafferentation and an invasion of the amputation zone by neighbouring input might preferentially activate neurons that code for pain. As the cortical area that receives input from the periphery seems to stay assigned to the original zone of input, the activation in the cortical zone representing the amputated limb is referred to this limb and could be interpreted as phantom sensation and phantom limb pain90. Several prospective studies82,91 have shown that chronic pain before the amputation predicts later phantom limb pain, therefore supporting the pain memory hypothesis. However, these samples included few traumatic amputees and mainly amputees with long-standing prior pain problems, in whom pain memories can have developed over a long time period. In traumatic amputees, additional factors relating to the surgery, such as type of anaesthesia, and pre- and postoperative pain, could be important. Nevertheless, the pain memory hypothesis is also supported by the relatively modest effects of preemptive analgesia92. On the basis of the idea that the afferent barrage of nociceptive input might not be sufficiently inhibited by central anaesthesia, peripheral anaesthesia is added for some time before and during surgery to prevent central sensitization from occurring93. However, VOLUME 7 | NOVEMBER 2006 | 877 © 2006 Nature Publishing Group REVIEWS Box 1 | Incongruence phenomena, bodily symptoms and illusory perceptions In recent years, the preconditions and neural correlates of a number of illusory somatosensory phenomena have been investigated and might shed light on the understanding of phantom phenomena and phantom pain. Sensory illusions such as the tactile funnelling illusion80, during which the simultaneous presentation of brief stimuli at multiple points on the skin produces a single focal sensation at the centre of the stimulus pattern even when no physical stimulus occurs at that site, have been shown to have a percept-related and not a stimulation-related representation in the primary somatosensory (SI) cortex. These data not only indicate that the brain processes the perceptual, and not the physical, properties of sensory stimulation but also that these integrative processes occur early in the SI cortex. Illusory phenomena, however, involve additional brain regions when the perception of the body and of individual body parts is involved, as in phantom sensations. Here, bottom-up processes of visuotactile integration and top-down processes that originate from the representation of one’s own body are important in generating illusions of body ownership, such as in the rubber hand illusion. In this illusion, synchronous input from the actual and the rubber hand, related to synchronous stroking of the actual and the fake hand, produce the feeling of ownership of the artificial hand113. If the rubber hand is in an implausible position with respect to the normal body schema, the illusion does not occur. Whereas synchronous stimulation can lead to the illusion of body ownership, asynchronous stimulation in one sensory modality or between the senses can lead to abnormal sensory perception78 and mismatch-related activations in ventral premotor and parietal regions114. The extent to which the restoration of homeostatic processes and of an intact body schema takes part in these perceptual phenomena needs to be determined115. The exploration of the preconditions and neural correlates of such illusory perceptions might shed light on the experience of phantom phenomena and unusual bodily sensations, somatosensory misperceptions and phantom pain. a controlled study in amputees showed that pre-emptive analgesia did not significantly reduce the incidence of phantom limb pain94, although the addition of an NMDA receptor antagonist in the peri-operative phase extending into the postoperative weeks might have beneficial results95. This effect could be due to the erasure of preexisting, and the prevention of postoperatively acquired, somatosensory pain memories. The fact that pre-existing sensitivities in the processing of nociceptive stimulation might be important is also underscored by the finding that pain pressure thresholds before the amputation predict phantom limb pain after the amputation96. To our knowledge, no study has examined the extent to which prior pain experience in general might contribute to phantom limb pain. Research on pain experiences in the perinatal phase has shown that sensitization occurs that could then predispose individuals to chronic pain development97,98. Later life experience and modelling might have similar effects. The role of insufficient postoperative pain management has so far probably been underestimated99, and more longitudinal research is needed to test the pain memory hypothesis. Myoelectric prosthesis A motor-driven prosthesis that can, for example, be used for grip movements and is operated through the use of electromyographic signals from muscles. Affective and motivational aspects of pain. It is likely that reorganization following amputation occurs not only for the areas involved in sensory–discriminative aspects of pain, but also for those brain regions that mediate affective–motivational aspects of pain, such as the insula, anterior cingulate and frontal cortices100. A close relationship has been shown between activation of the anterior cingulate cortex and phantom limb pain after induced phantom pain by hypnotic suggestion101. Another study observed a potentiation of sensory responses in the anterior cingulate cortex of rats following limb amputation102. The role of affective and motivational factors in phantom limb pain is also underscored by the fact that several studies could predict the severity of phantom limb pain from depression and coping-related variables8. These factors need to be explored in greater detail. 878 | NOVEMBER 2006 | VOLUME 7 Implications for the treatment of phantom pain Several studies, including large surveys of amputees, have shown that most currently available treatments for phantom limb pain, which range from analgesic and antidepressant medication to stimulation, are ineffective and fail to consider the mechanisms that underlie production of the pain83. On the basis of the findings on CNS plasticity related to phantom pain, experimental methods that affect neuroplasticity as well as memory formation and maintenance might positively influence phantom limb pain. Work in healthy animals and humans on stimulationinduced plasticity has shown that extensive, behaviourally relevant stimulation of a body part leads to an alteration of its cortical representation zone103,104. In patients with phantom limb pain, intensive use of a myoelectric prosthesis is positively correlated with both reduced phantom limb pain and reduced cortical reorganization105. When cortical reorganization was partialled out, the relationship between prosthesis use and reduced phantom limb pain was no longer significant, suggesting that cortical reorganization mediates this relationship. An alternative approach in patients in whom prosthesis use is not viable is the application of behaviourally relevant stimulation. A 2 week regimen that consisted of daily discrimination training of electrical stimuli to the stump led to significant improvements in phantom limb pain and a significant reversal of cortical reorganization as assessed with neuroelectric source imaging106. A control group of patients who received standard medical treatment and general psychological counselling in this time period did not show similar changes in cortical reorganization and phantom limb pain. The basic idea of the treatment was to provide input into the amputation zone and thereby undo the reorganizational changes that occurred subsequent to the amputation. This effect was replicated by asynchronous stimulation of the mouth and stump in upper extremity amputees107. Similar effects on phantom pain and cortical activation were reported for imagined movement of the phantom108. Mirror treatment (where a mirror is used to trick www.nature.com/reviews/neuro © 2006 Nature Publishing Group REVIEWS Imagined movement 100 Telescoping (%) 75 50 25 r = 0.85 IM 0 EM 0 2 4 6 8 10 12 14 16 Shi of S1 activation towards Cz (mm) Figure 3 | Brain correlates of the telescoping phenomenon. The phenomenon of telescoping refers to the shrinking and retraction of the phantom towards the residual limb (left). The middle panel shows brain activation related to the imagined movement (IM) of telescoped and non-telescoped phantoms. The representation of the movement in the primary somatosensory (SI) cortex (red shading) follows the perceived location of the movement (opening and closing of the hand) and not the actual anatomical location (hand area). Completely telescoped phantoms create activity in the cortical region that represents the shoulder, partially telescoped phantoms in the region of the arm and non-telescoped phantoms in the hand region. EM denotes the cortical activation related to executed movements of the intact hand and Complex regional pain syndrome (CRPS). A chronic neuropathic pain syndrome of two types. CRPS1 occurs most often in the arms or legs after a minor or major injury and is accompanied by severe pain, swelling, oedema, sudomotor abnormalities and increased sensitivity to touch. CRPS2 is related to an identified nerve injury. 1. 2. 3. 4. 5. indicates where the representation of the hand in the SI cortex is located. The right panel shows the correlation coefficient that was computed for the amount of telescoping (0–100%) and the activation related to the perceived movement of the phantom in the SI cortex with the distance of the maximally activated voxels from the central midline position of the cortex (Cz) computed in millimetres. The correlation was significant in the SI, but not in the primary motor cortex (blue shading). This indicates that pain-free amputees might experience reactivation of the deafferented cortical representation zone related to that hand, whereas amputees without pain might not, which could be related to their pain. The data also indicate that this effect might originate directly in the SI cortex, and is not mediated by the motor cortex. the brain into perceiving movement of the phantom when the intact limb is moved) might be effective but has so far been tested only in an anecdotal manner for phantom limb pain109,110, although it effectively reduces pain in complex regional pain syndrome111. Pharmacological interventions that target either neuroplastic changes or memory mechanisms (which have overlapping targets) should also be effective. These might include NMDA receptor antagonists, GABA agonists or anticonvulsive agents, to mention only a few options. Stimulation of cortical areas that are hyperactive by transcranial magnetic stimulation or direct current stimulation might also be viable options112. These approaches are based on the idea that cortical hyperexcitability, which contributes to pain, could be reduced by setting a ‘virtual’ lesion in the overactive cortical representation zone. Hunter, J. P., Katz, J. & Davis, K. D. The effect of tactile and visual sensory inputs on phantom limb awareness. Brain 126, 579–589 (2003). Nikolajsen, L. J. & Jensen, T. S. in Wall and Melzack’s Textbook of Pain (eds Koltzenburg, M. & McMahon, S. B.) 961–971 (Elsevier, Amsterdam, 2005). A comprehensive overview of factors that contribute to phantom limbs, and treatment options. Rothemund, Y., Grüsser, S. M., Liebeskind, U., Schlag, P. M. & Flor, H. Phantom phenomena in mastectomized patients and their relation to chronic and acute pre-mastectomy pain. Pain 107, 140–146 (2004). Melzack, R. & Loeser, J. D. Phantom body pain in paraplegics: evidence for a ‘central pattern generating mechanism’ for pain. Pain 4, 195–210 (1978). Waxman, S. G. & Hains, B. C. Fire and phantoms after spinal cord injury: Na+ channels and central pain. Trends Neurosci. 29, 207–215 (2006). An overview of molecular mechanisms of pain after spinal cord injury. 6. Conclusions and future directions The mechanisms underlying the painful perception of a missing body part are still unclear. Changes at sensitized and reorganized nerve endings feed into the nervous system and trigger secondary alterations in somatosensory processing systems. Reorganization of the cortical body map seems to be an important element in distinguishing painful from non-painful phantom sensations. However, the extent to which these brain-related neuroplastic changes depend on alterations in the periphery, spinal cord or in the genetic constitution is still not clear, and needs to be examined. Nevertheless, these neuroplastic changes related to phantom limb pain might represent a promising therapeutic target and should therefore be explored to improve the prevention and treatment of this phenomenon. Hill, A. Phantom limb pain: a review of the literature on attributes and potential mechanisms. J. Pain Symptom Manage. 17, 125–142 (1999). 7. Houghton, A. D., Nicholls, G., Houghton, A. L., Saadah, E. & McColl, L. Phantom pain: natural history and association with rehabilitation. Ann. R. Coll. Surg. Engl. 76, 22–25 (1994). 8. Ephraim, P. L., Wegener, S. T., MacKenzie, E. J., Dillingham, T. R. & Pezzin, L. E. Phantom pain, residual limb pain, and back pain in amputees: results of a national survey. Arch. Phys. Med. Rehabil. 86, 1910–1919 (2005). 9. Lacoux, P. A., Crombie, I. K. & Macrae, W. A. Pain in traumatic upper limb amputees in Sierra Leone. Pain 99, 309–312 (2002). 10. Wilkins, K. L., McGrath, P. J., Finley, G. A. & Katz, J. Phantom limb sensation and phantom limb pain in child and adolescent amputees. Pain 78, 7–12 (1998). 11. Saadah, E. S. M. & Melzack, R. Phantom limb experiences in congenital limb-deficient adults. Cortex 30, 479–485 (1994). NATURE REVIEWS | NEUROSCIENCE 12. Sherman, R. A., Arena, J. G., Sherman, C. J. & Ernst, J. L. The mystery of phantom limb pain: growing evidence for psychophysiological mechanisms. Biofeedback Self Regul. 14, 267–280 (1989). 13. Jensen, T. S., Krebs, B., Nielsen, J. & Rasmussen, P. Immediate and long-term phantom limb pain in amputees: incidence, clinical characteristics and relationship to pre-amputation limb pain. Pain 21, 267–278 (1985). 14. Yarnitski, D., Barron, S. A. & Bental, E. Disappearance of phantom pain after focal brain infarction. Pain 32, 285–287 (1988). 15. Jänig, W. & McLachlan, E. On the fate of sympathetic and sensory neurons projecting into a neuroma of the superficial peroneal nerve in the cat. J. Comp. Neurol. 225, 302–311 (1984). 16. Fried, K., Govrin-Lippman, R., Rosenthal, F., Ellisman, M. H. & Devor, M. Ultrastructure of afferent axon endings in a neuroma. J. Neurocytol. 20, 682–701 (1991). VOLUME 7 | NOVEMBER 2006 | 879 © 2006 Nature Publishing Group REVIEWS 17. Wall, P. D. & Gutnick, M. Ongoing activity in peripheral nerves: the physiology and pharmacology of impulses originating from a neuroma. Exp. Neurol. 43, 580–593 (1974). 18. Devor, M. in Wall and Melzack’s Textbook of Pain (eds Koltzenburg, M. & McMahon, S. B.) 905–927 (Elsevier, Amsterdam, 2005). 19. Devor, M. Sodium channels and mechanisms of neuropathic pain. J. Pain 7, S3–S12 (2006). 20. Gorodetskaya, N., Constantin, C. & Jänig, W. Ectopic activity in cutaneous regenerating afferent nerve fibers following nerve lesion in the rat. Eur. J. Neurosci. 18, 2487–2497 (2003). 21. Blumberg, H. & Jänig, W. Activation of fibers via experimentally produced stump neuromas of skin nerves: ephaptic transmission or retrograde sprouting? Exp. Neurol. 76, 468–482 (1982). 22. Nyström, B. & Hagbarth, K. E. Microelectrode recordings from transected nerves in amputees with phantom limb pain. Neurosci. Lett. 27, 211–216 (1981). 23. Chen, Y., Michaelis, M., Jänig, W. & Devor, M. Adrenoreceptor subtype mediating sympatheticsensory coupling in injured sensory neurons. J. Neurophysiol. 76, 3721–3730 (1996). 24. Katz, J. Psychophysiological contributions to phantom limbs. Can. J. Psychiatry 37, 282–298 (1992). A comprehensive discussion of psychophysiological factors in phantom pain. 25. Chabal, C., Jacobson, L., Russell, L. C. & Burchiel, K. J. Pain response to perineuromal injection of normal saline, epinephrine, and lidocaine in humans. Pain 49, 9–12 (1992). 26. Fagius, J., Nordin, M. & Wall, M. Sympathetic nerve activity to amputated lower leg in humans. Evidence of altered skin vasoconstrictor discharge. Pain 98, 37–45 (2002). 27. Birbaumer, N. et al. Effects of regional anesthesia on phantom limb pain are mirrored in changes in cortical reorganization. J. Neurosci. 17, 5503–5508 (1997). 28. Baron, R. & Maier, C. Phantom limb pain: are cutaneous nociceptors and spinothalamic neurons involved in the signaling and maintenance of spontaneous and touch-evoked pain? A case report. Pain 60, 223–228. 29. Schmidt, A. P., Takahashi, M. E. & de Paula Posso, I. Phantom limb pain induced by spinal anesthesia. Clinics 60, 263–264 (2005). 30. Woolf, C. J. & Salter, M. W. in Wall and Melzack’s Textbook of Pain (eds Koltzenburg, M. & McMahon, S. B.) 91–105 (Elsevier, Amsterdam, 2005). 31. Woolf, C. J. Dissecting out mechanisms responsible for peripheral neuropathic pain: implications for diagnosis and therapy. Life Sci. 74, 2605–1510 (2004). 32. Moore, K. A. et al. Partial peripheral nerve injury promotes a selective loss of GABAergic inhibition in the superficial dorsal horn of the spinal cord. J. Neurosci. 22, 6724–6731 (2002). 33. Coull, J. A. et al. BDNF from microglia causes the shift in neuronal anion gradient underlying neuropathic pain. Nature 438, 1017–1021 (2005). 34. Wang, S. et al. A rat model of unilateral hindpaw burn injury: slowly developing rightwards shift of the morphine dose-response curve. Pain 116, 87–95 (2005). 35. Wiesenfeld-Hallin, Z, Xu, X. J. & Hökfelt, T. The role of spinal cholecystokinin in chronic pain states. Pharmacol. Toxicol. 91, 398–403 (2002). 36. Torsney, C. & MacDermott, A. B. Disinhibition opens the gate to pathological pain signaling in superficial neurokinin 1 receptor-expressing neurons in rat spinal cord. J. Neurosci. 26, 1833–1843 (2006). 37. Ueda, H. Molecular mechanisms of neuropathic painphenotypic switch and initiation mechanisms. Pharmacol. Ther. 109, 57–77 (2006). 38. Devor, M. & Wall, P. D. Reorganisation of spinal cord sensory map after peripheral nerve injury. Nature 276, 75–76 (1978). 39. Swanson, L. W. Mapping the human brain: past present, and future. Trends Neurosci. 18, 471–474 (1995). 40. Florence, S. L., Taub, H. B. & Kaas, J. H. Large-scale sprouting of cortical connections after peripheral injury in adult macaque monkeys. Science 282, 1117–1121 (1998). 41. Davis, K. D. et al. Phantom sensations generated by thalamic microstimulation. Nature 391, 385–387 (1998). In this study phantom sensation was elicited by thalamic stimulation in human amputees. 42. Jones, E. G. & Pons, T. P. Thalamic and brainstem contributions to large-scale plasticity of primate somatosensory cortex. Science 282, 1121–1125 (1998). 43. Wu, C. W. & Kaas, J. H. The effects of long-standing limb loss on anatomical reorganization of the somatosensory afferents in the brainstem and spinal cord. Somatosens. Mot. Res. 19, 153–163 (2002). 44. Kaas, J. H., Florence, S. L. & Jain, N. Subcortical contributions to massive cortical reorganization. Neuron 22, 657–660 (1999). 45. Jain, N., Florence, S. L., Qi, H. X. & Kaas, J. H. Growth of new brainstem connections in adult monkeys with massive sensory loss. Proc. Natl Acad. Sci. USA 97, 5546–5550 (2000). 46. Ergenzinger, E. R., Glasier, M. M., Hahm, J. O. & Pons, T. P. Cortically induced thalamic plasticity in the primate somatosensory system. Nature Neurosci. 1, 226–229 (1998). 47. Kaas, J. H. Is most of neural plasticity in the thalamus cortical? Proc. Natl Acad. Sci. USA 96, 7622–7623 (1999). 48. Merzenich, M. M. et al. Somatosensory cortical map changes following digit amputation in adult monkeys. J. Comp. Neurol. 224, 591–605 (1984). 49. Pons, T. P. et al. Massive cortical reorganization after sensory deafferentation in adult macaques. Science 252, 1857–1860 (1991). Revealed massive changes in the cortical map related to dorsal rhizotomies in adult monkeys. 50. Ramachandran, V. S., Rogers-Ramachandran, D. & Stewart, M. Perceptual correlates of massive cortical reorganization. Science 258, 1159–1160 (1992). 51. Cronholm, B. Phantom limbs in amputees. A study of changes in the integration of centripetal impulses with special reference to referred sensations. Acta Psychiatr. Neurol. Scand. Suppl. 72, 1–310 (1951). 52. Halligan, P. W., Marshall, J. C., Wade, D. T., Davey, J. & Morrisson, D. Thumb in cheek? Sensory reorganization and perceptual plasticity after limb amputation. Neuroreport 4, 233–236 (1993). 53. Grüsser, S. M. et al. Remote activation of referred phantom sensation and cortical reorganization in human upper extremity amputees. Exp. Brain Res. 154, 97–102 (2004). 54. Grüsser, S. M. et al. The relationship of perceptual phenomena and cortical reorganization in upper extremity amputees. Neuroscience 102, 263–272 (2001). 55. Halligan, P. W., Marshall, J. C. & Wade, D. T. Sensory disorganization and perceptual plasticity after limb amputation: a follow-up study. Neuroreport 27, 1341–1345 (1994). 56. Yang, T. T. et al. Sensory maps in the human brain. Nature 368, 592–593 (1994). 57. Elbert, T. R. et al. Extensive reorganization of the somatosensory cortex in adult humans after nervous system injury. Neuroreport 5, 2593–2597 (1994). 58. Flor, H. et al. Phantom-limb pain as a perceptual correlate of cortical reorganization following arm amputation. Nature 375, 482–484 (1995). Showed a close association between the magnitude of map changes in the SI cortex and the severity of phantom limb pain. 59. Flor, H. et al. Cortical reorganization and phantom phenomena in congenital and traumatic upper-extremity amputees. Exp. Brain Res. 119, 205–212 (1998). 60. Wu, C. W. & Kaas, J. H. Reorganization in primary motor cortex of primates with long-standing therapeutic amputations. J. Neurosci. 19, 7679–7697 (1999). 61. Cohen, L. G., Bandinelli, S., Findley, T. W. & Hallett, M. Motor reorganization after upper limb amputation in man. A study with focal magnetic stimulation. Brain 114, 615–627 (1991). 62. Karl, A., Birbaumer, N., Lutzenberger, W., Cohen, L. G. & Flor, H. Reorganization of motor and somatosensory cortex in upper extremity amputees with phantom limb pain. J. Neurosci. 21, 3609–3618 (2001). 63. Karl, A., Mühlnickel, W., Kurth, R. & Flor, H. Neuroelectric source imaging of steady-state movement-related cortical potentials in human upper extremity amputees with and without phantom limb pain. Pain 110, 90–102 (2004). 64. Lotze, M., Flor, H., Grodd, W., Larbig, W. & Birbaumer, N. Phantom movements and pain: an fMRI study in upper limb amputees. Brain 124, 2268–2277 (2001). 65. Spitzer, M., Böhler, P., Weisbrod, M. & Kischka, U. A neural network model of phantom limbs. Biol. Cybern. 72, 197–206 (1995). 880 | NOVEMBER 2006 | VOLUME 7 66. Calford, M. B. & Tweedale, R. C-fibres provide a source of masking inhibition to primary somatosensory cortex. Proc. Biol. Sci. 243, 269–275 (1991). 67. Bowlus, T. H. et al. Comparison of reorganization of the somatosensory system in rats that sustained forelimb removal as neonates and as adults. J. Comp. Neurol. 465, 335–348 (2003). 68. Churchill, J. D., Muja, N., Myers, W. A., Besheer, J. & Garraghty, P. E. Somatotopic consolidation: a third phase of reorganization after peripheral nerve injury in adult squirrel monkeys. Exp. Brain Res. 118, 189–196 (1998). 69. Churchill, J. D., Tharp, J. A., Wellman, C. L., Sengelaub, D. R. & Garraghty, P. E. Morphological correlates of injury-induced reorganization in primate somatosensory cortex. BMC Neurosci. 5, 43 (2004). 70. Kaas, J. H. & Florence, S. L. Mechanisms of reorganization in sensory systems of primates after peripheral nerve injury. Adv. Neurol. 73, 147–158 (1997). 71. Levy, L. M., Ziemann, U., Chen, R. & Cohen, L. G. Rapid modulation of GABA in sensorimotor cortex induced by acute deafferentation. Ann. Neurol. 52, 755–761 (2005). 72. Canu, M. H. et al. Concentration of amino acid neurotransmitters in the somatosensory cortex of the rat after surgical or functional deafferentation. Exp. Brain Res. 173, 623–628 (2006). 73. Larbig, W. et al. Evidence for a change in neural processing after amputation. Pain 67 275–283 (1996). 74. Karl, A., Diers, M. & Flor, H. P300-amplitudes in upper limb amputees with and without phantom limb pain in a visual oddball paradigm. Pain 110, 40–46 (2004). 75. Elbert, T. et al. Input-increase and input-decrease types of cortical reorganization after upper extremity amputation in humans. Exp. Brain Res. 117, 161–164 (1997). 76. Ehrsson, H. H., Spence, C. & Passingham, R. E. That’s my hand! Activity in premotor cortex reflects feeling of ownership of a limb. Science 305, 875–877 (2004). 77. Harris, A. J. Cortical origin of pathological pain. Lancet 354, 1464–1466 (1999). 78. McCabe, C. S., Haigh, R. C., Halligan, P. W. & Blake, D. R. Simulating sensory-motor incongruence in healthy volunteers: implications for a cortical model of pain. Rheumatology 44, 509–516 (2005). 79. Moseley, G. L. & Gandevia, S. C. Sensory-motor incongruence and reports of ‘pain’. Rheumatology 44, 1083–1085 (2005). 80. Chen, L. M., Friedman, R. M. & Roe, A. W. Optical imaging of a tactile illusion in area 3b of the primary somatosensory cortex. Science 302, 881–885 (2003). 81. Katz, J. & Melzack, R. Pain ‘memories’ in phantom limbs: review and clinical observations. Pain 43, 319– 336 (1990). These authors were the first to describe the concept of pain memories in phantom limbs. 82. Nikolajsen, L., Ilkjaer, S., Kroner, K., Christensen, J. H. & Jensen, T. S. The influence of preamputation pain on postamputation stump and phantom pain. Pain 72, 393–405 (1997). 83. Flor, H. Phantom-limb pain: characteristics, causes, and treatment. Lancet Neurol. 1, 182–189 (2002). 84. Flor, H. The functional organization of the brain in chronic pain. Prog. Brain Res. 129, 313–322 (2000). 85. Flor, H., Braun, C., Elbert, T. & Birbaumer, N. Extensive reorganization of primary somatosensory cortex in chronic back pain patients. Neurosci. Lett. 224, 5–8 (1997). 86. Soros, P. et al. Functional reorganization of the human primary somatosensory cortex after acute pain demonstrated by magnetoencephalography. Neurosci. Lett. 298, 195–198 (2001). 87. Kenshalo, D. R. & Willis, W. D. in Pain and the Cerebral Cortex (ed. Peters, A.) 153–212 (Plenum, New York, 1991). 88. Head, H. & Holmes, G. Sensory disturbances from cerebral lesions. Brain 34, 102–254 (1911). 89. Appenzeller, O. & Bicknell, J. M. Effects of nervous system lesions on phantom experience in amputees. Neurology 19, 141–146 (1969). 90. Doetsch, G. S. Perceptual significance of somatosensory cortical reorganization following peripheral denervation. NeuroReport 9, 29–35 (1998). 91. Hanley, M. A. et al. Preamputation pain and acute pain predict chronic pain after lower extremity amputation. J. Pain (in the press). www.nature.com/reviews/neuro © 2006 Nature Publishing Group REVIEWS 92. Jensen, T. S. & Nikolajsen, L. Pre-emptive analgesia in postamputation pain: an update. Prog Brain Res. 129, 493–503 (2000). 93. Woolf, C. J. & Chong, M. S. Preemptive analgesia — treating postoperative pain by preventing the establishment of central sensitization. Anesth. Analg. 77, 362–379 (1993). 94. Nikolajsen, L., Ilkjaer, S., Christensen, J. H., Krøner, K. & Jensen, T. S. Randomised trial of epidural bupivacaine and morphine in prevention of stump and phantom pain in lower-limb amputation. Lancet 350, 1353–1357 (1997). This controlled study showed no added effect of pre-emptive analgesia for the prevention of phantom limb pain. 95. Wiech, K. et al. Prevention of phantom limb pain and cortical reorganization in the early phase after amputation in humans. Soc. Neurosci. Abstr. 28, 163.9 (2001). 96. Nikolajsen, L., Ilkjaer, S. & Jensen, T. S. Relationship between mechanical sensitivity and postamputation pain: a prospective study. Eur. J. Pain 4, 327–334 (2000). 97. Ruda, M. A., Ling, Q. D., Hohmann, A. G., Peng, Y. B. & Tachibana, T. Altered nociceptive neuronal circuits after neonatal peripheral inflammation. Science 289, 628–631 (2000). Showed that neonatal pain leads to the alteration of nociceptive circuits, therefore supporting the idea of pain memories. 98. Hermann, C., Hohmeister, J., Demirakca, S., Zohsel, K. & Flor, H. Long-term alteration of sensory perception and pain sensitivity in school-aged children with early pain experiences. Pain (in the press). 99. Wilder-Smith, O. H. & Arendt-Nielsen, L. Postoperative hyperalgesia: its clinical importance and relevance. Anesthesiology 104, 601–607 (2006). 100. Rosen, G. et al. Different brain areas activated during imagery of painful and non-painful ‘finger movements’ 101. 102. 103. 104. 105. 106. 107. 108. 109. 110. 111. in a subject with an amputated arm. Neurocase 7, 255–260 (2001). Willoch, F. et al. Phantom limb pain in the human brain: unraveling neural circuitries of phantom limb sensations using positron emission tomography. Ann. Neurol. 48, 842–849 (2000). Wei, F. & Zhuo, M. Potentiation of sensory responses in the anterior cingulate cortex following digit amputation in the anaesthetised rat. J. Physiol. 532, 823–833 (2001). Recanzone, G. H., Merzenich, M. M., Jenkins, W. M., Grajski, K. A. & Dinse, H. R. Topographic reorganization of the hand representation in cortical area 3b owl monkeys trained in a frequencydiscrimination task. J. Neurophysiol. 67, 1031–1056 (1992). Elbert, T., Pantev, C., Wienbruch, C., Rockstroh, B. & Taub, E. Increased cortical representation of the fingers of the left hand in string players. Science 270, 305–307 (1995). Lotze, M. et al. Does use of a myoelectric prosthesis reduce cortical reorganization and phantom limb pain? Nature Neurosci. 2, 501–502 (1999). Flor, H., Denke, C., Schaefer, M. & Grüsser, S. Effect of sensory discrimination training on cortical reorganisation and phantom limb pain. Lancet 357, 1763–1764 (2001). Huse, E., Preissl, H., Larbig, W. & Birbaumer, N. Phantom limb pain. Lancet 358, 1015 (2001). Giraux, P. & Sirigu, A. Illusory movements of the paralyzed limb restore motor cortex activity. Neuroimage 20, 107–111 (2003). Ramachandran, V. S. & Rogers-Ramachandran, D. Synesthesia in phantom limbs induced with mirrors. Proc. R. Soc. Lond. B Biol. Sci. 263, 377–386 (1996). MacLachlan, M., McDonald, D. & Waloch, J. Mirror treatment of lower limb phantom pain: a case study. Disabil. Rehabil. 26, 901–904 (2004). Moseley, G. L. Is successful rehabilitation of complex regional pain syndrome due to sustained attention to NATURE REVIEWS | NEUROSCIENCE 112. 113. 114. 115. the affected limb? A randomised clinical trial. Pain 114, 54–61 (2005). Showed specific effects on pain related to hand laterality recognition, imagined movement and mirror training in complex regional pain syndrome. Fregni, F. et al. A sham-controlled, phase II trial of transcranial direct current stimulation for the treatment of central pain in traumatic spinal cord injury. Pain 122, 197–209 (2006). Ehrsson, H. H., Holmes, N. P. & Passingham, R. E. Touching a rubber hand: feeling of body ownership is associated with activity in multisensory brain areas. J. Neurosci. 25, 10564–10573 (2005). Fink, G. R. et al. The neural consequences of conflict between intention and the senses. Brain 122, 497–512 (1999). Craig, A. D. How do you feel? Interoception: the sense of the physiological condition of the body. Nature Rev. Neurosci. 3, 655–666 (2002). Acknowledgements This article is dedicated to the memory of T. Pons, whose work inspired many of the findings reported here. This work was supported by the Deutsche Forschungsgemeinschaft, the Bundesministerium für Bildung und Forschung (German Neuropathic Pain Network) and the Lundbeck Foundation, Denmark. The authors would like to thank W. Jänig for helpful comments on an earlier version of this article and M. Lotze for help with the figures. Competing interests statement The authors declare no competing financial interests. FURTHER INFORMATION Flor’s laboratory: http://www.zi-mannheim.de/herta_flor0. html Access to this links box is available online. VOLUME 7 | NOVEMBER 2006 | 881 © 2006 Nature Publishing Group