Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
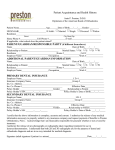
ONLINE ONLY A new concept of mandibular dental arch forms with normal occlusion Tarcila Triviño,a Danilo Furquim Siqueira,b and Marco Antonio Scanavinic São Paulo and Niterói, Brazil Introduction: Because it is important to maintain dental arch dimensions during orthodontic therapy, all possible dental arch forms must be evaluated. Methods: A mathematical method associated with a polynomial function was used to evaluate the dental arch forms of 63 mandibular models of Brazilian adolescents in the permanent dentition with normal occlusion. A bead was glued to each tooth to simulate an orthodontic accessory and help in the measurement of distances between the center of the bead to the x- and y-axes. The dental casts were digitized, and images were plotted on a computer program to obtain the sixth-degree polynomial and the graph of this function. These segments were organized into 8 groups according to the form of the anterior curve of the dental arch; these were named forms A through H. Each group was subdivided into 3 subgroups: small, medium, and large sizes. Results: Form A was the most frequently observed at 22%, whereas form G was observed in only 2% of the total sample. Forms A, B, C, D, E, and F had more curve segments in medium size, and forms G and H had more curves in small size. A mean dental arch curve was calculated; however, this form coincided with form C, which had an incidence of 10%. Conclusions: The mandibular dental arch is represented by 23 forms; thus, a normal dental arch cannot be represented by only 1 simple arch form. (Am J Orthod Dentofacial Orthop 2008;133:10.e15-10.e22) T he dental arch, an important element in orthodontics, is a fundamental principle in orthodontic planning and therapy.1,2 A dental arch form is initially established by the configuration of the bony ridge and then by tooth eruption, perioral muscles, and intraoral functional forces. Even though most patients with a malocclusion have an altered dental arch form, the alterations achieved with mechanics during orthodontic treatment should not affect the balance between bone and dental and muscular structures; the arrangement of these structures adjacent to teeth and jaws should be considered the limit for orthodontic movement.1,3-5 To minimize some of these factors, specialists have investigated the most effective approach for the correct repositioning of teeth to provide esthetics, function, and stability, and to define the size and configuration of the dental arch. Initially, some authors advocated the use of dental casts in which the alveolar ridge form would be the From Methodist University of São Paulo, São Bernardo do Campo, São Paulo, Brazil. a Master degree in orthodontics, Methodist University of São Paulo; specialist in orthodontics, Federal Fluminense University, Niterói, Rio de Janeiro, Brazil. b Professor, postgraduate program in orthodontics. c Professor and coordinator, postgraduate program in orthodontics. Reprint requests to: Tarcila Triviño, Av. Nove de Julho, 5483, conj. 111, Jardim Paulista, São Paulo, SP, Brazil, CEP 01407-200; e-mail, tarcilatrivino@ uol.com.br. Submitted, April 2006; revised and accepted, July 2007. 0889-5406/$34.00 Copyright © 2008 by the American Association of Orthodontists. doi:10.1016/j.ajodo.2007.07.014 reference for the fabrication of archwires, thus avoiding changes in the transverse dental arch dimensions.6,7 Because handling the dental casts might not be practical and fractures often occurred in these diagnostic elements, many authors attempted to find a representation of the dental arch that would allow immediate success, durability, and precision, suggesting the use of prototypes or references to help the professional during orthodontic therapy and provide the parameters for fabricating archwires or selecting preformed ones.2,6,7-11 Basically, the standards established comprised description of the dental arch form by geometric figures such as catenary curve,12,13 parabolic curve,14,15 ellipse,14-17 hyperbola,14 or even a semicircle joined to straight segments.9,18,19 From these representations, diagrams were developed on the basis of measurements of dental arch components that would act as a guide during orthodontic treatment, because the use of a customized diagram would provide archwires with standardized forms and dimensions.8-10,16-19 However, the use of diagrams describing an average or ideal dental arch form was counterindicated when some authors observed that the dental arch curve was represented or defined not only by a geometric shape, but also by several configurations.15,20-26 The various descriptions of dental arch forms in several studies might be related to the application of algebraic or geometric functions associated with computations that increased the accuracy of the dental arch 10.e15 10.e16 Triviño, Siqueira, and Scanavini representation.15,21,22,25-31 Some authors who observed that polynomial functions could describe the dental arch form in a simple and symmetric manner accepted these mathematical equations as an accurate method for the description of dental arch configurations.26,30,32-38 Because the original mandibular dental arch form and dimensions should be respected during orthodontic therapy and because of controversy about dental arch configuration among authors using various methodologies, in this study, we attempted to establish mandibular dental arch forms with a precise method applied to an adequate sample; this would enhance the construction and use of standardized archwires and, consequently, allow the orthodontist to obtain and maintain ideal results after orthodontic treatment.1,3 MATERIAL AND METHODS Our study sample included 63 subjects (35 female, 28 male) carefully selected from 6118 white Brazilian adolescents between 12 and 21 years old at Methodist University of São Paulo who were in permanent dentition, with all teeth in occlusion except for the third molars, and normal occlusion with at least 4 of the 6 keys to normal occlusion as defined by Andrews.39 Interarch relationship (Andrews’ first key39) should be present in all cases. Mandibular dental casts for the subjects were obtained, and, in each tooth, from the left second molar to the right second molar, a glass bead was glued to simulate the ideal position of an orthodontic brace. All beads were initially measured with a pachymeter (model Zurich; Dentaurum, Ispringen, Germany) to ensure that the diameter was 1.5 mm (⫾ 0.1 mm). Each glass bead was positioned in the center of the clinical crown of the incisors, canines, and premolars, and in the middle third of the mesiobuccal cusps in the first and second molars. After bonding the glass beads, which were red to enhance observation in the grayscale images, dental casts were digitized on a scanner (Scanjet 6100C; Hewlett-Packard, Palo Alto, Calif), and images with 300 dpi resolution in TIFF format were obtained. The position of the dental casts on the scanner was established with millimeter acetate paper, especially designed for this methodology; it was made by photocopying a sheet of millimeter paper on ordinary acetate paper. After making the photocopies, the prepared acetate and millimeter papers were superimposed to verify the lack of distortion in the acetate copy. The customized acetate paper was placed between the scanner glass surface and the occlusal plane of the dental cast, so that the posterior edge of the dental cast would coincide with the abscissa axis (x) and the dental American Journal of Orthodontics and Dentofacial Orthopedics January 2008 Fig 1. Representation of the Cartesian system and the x and y measurements corresponding to the points used to establish dental arch form: 7 and 14, distance between points of the second molars to the x- and y-axes; 6 and 13, distance between points of the first molars to the x- and y-axes; 5 and 12, distance between points of the second premolars to the x- and y-axes; 4 and 11, distance between points of the first premolars to the x- and y-axes; 3 and 10, distance between points of the canines to the x- and y-axes; 2 and 9, distance between points of the lateral incisors to the x- and y-axes; 1 and 8, distance between points of the central incisors to the x- and y-axes. midline with the ordinate axis (y), creating a Cartesian system. The arch images of the 63 mandibular dental casts were divided into right and left sides, and the mirror method was applied to these hemiarches; this resulted in symmetric dental arches, for a total of 126 curve segments.26 The mirror method was used because the geometric figures that would represent the dental arch form, such as parabolic curve, ellipse, hyperbola, and others, are symmetric mathematical representations, and, even though dental casts were obtained from subjects with normal occlusion, there can be asymmetry between the right and left sides of the dental arch. With projection of the cast images on a flat computer screen with the software Corel Photo Paint 10 (Corel Corp, Ottawa, Ontario, Canada) with 100% magnification, the origin of the Cartesian system adapted to the image of the dental cast (point of contact between abscissa x and ordinate y, whose value is zero) was established in the line corresponding to the projection of the interincisal point (dental midline) on axis x. For each image cast, 14 points (x, y) on the dental arch were measured by the distance between the center of glass-bead images to the abscissa axis and ordinate axis, respectively (Fig 1). The centers of the 1.5-mm Triviño, Siqueira, and Scanavini 10.e17 American Journal of Orthodontics and Dentofacial Orthopedics Volume 133, Number 1 Table I. x7, values, class amplitude (CA), and mathematical intervals Form Highest x7 Lowest x7 Difference CA Interval 1 Interval 2 Interval 3 A B C D E F G H 3.10 3.15 3.15 3.15 3.10 3.00 2.90 3.15 2.60 2.50 2.60 2.40 2.60 2.50 2.70 2.45 0.50 0.65 0.55 0.75 0.50 0.50 0.20 0.70 0.15 0.20 0.15 0.25 0.15 0.15 0.05 0.20 2.60-2.75 2.50-2.70 2.60-2.75 2.40-2.65 2.60-2.75 2.50-2.65 2.70-2.75 2.45-2.65 2.80-2.95 2.75-2.95 2.80-2.95 2.70-2.95 2.80-2.95 2.70-2.85 2.80-2.85 2.70-2.90 3.00-3.15 3.00-3.20 3.00-3.15 3.00-3.25 3.00-3.15 2.90-3.05 2.90-2.95 2.95-3.15 diameter beads were used to simulate the distance from the bracket slot base to the buccal aspect of the teeth, which is about 0.75 mm. The computer software Curve Expert (version1.3; http://curveexpert.webhop.biz) was used to choose the polynomial function that would best describe the curve corresponding to the dental arch form. By visual evaluation of graphic representations of various mathematic functions provided by the computer software, the sixth-degree polynomial was selected to establish the dental arch form, because this polynomial function, represented by the equation y ⫽ ax6 ⫹ bx5 ⫹ cx4 ⫹ dx3 ⫹ ex2 ⫹ fx ⫹ g, provided the best description of the curve representing the form of these dental arches. Measurements of coordinates (x, y) of the 14 Cartesian points of the 126 curved segments were then plotted on the software Curve Expert to obtain the sixth-degree polynomial function for each curve segment, ie, the values of ratios a, b, c, d, e, f, and g, as well as the graphic representations. After this, data of the curve segments from the software were printed on white paper (75 g per square millimeter), illustrating the real size of the dental arches in the casts. The papers with the graphic representations of the curve segments were placed on a light box to allow better observation of the characteristics of the intercanine region of each dental arch, enhancing observation of the coincidence of the anterior curve between curve segments. According to the characteristics and similarities of the anterior curves, the 126 curve segments were divided into 8 groups to establish the various dental arch types and configurations. Division into groups allowed observation of the most prevalent dental arch form in the sample; the arithmetic mean applied to the x and y values of the curve segments of each group allowed achievement of mean x and y values for the 14 points of the average curve representing each dental arch form (8 forms, called A through H). Then, small, medium, and large sizes were determined for each group of dental arch forms by division of the curve segments of each group into 3 mathemat- ical intervals, established according to the class amplitude value (used in a distribution of frequencies, it is the difference between upper and lower limits in the same class), which was calculated as the distance from the second molar to the y-axis, because this value— x7—represents the width of the most posterior region in the dental arch. These values were organized in ascending order, and the class amplitude value was obtained by subtraction between the highest and lowest x7 values of each group and divided by 3 for the 3 dental arch sizes, represented by the 3 subgroups (Table I, Fig 2). The minimum value of the first subgroup corresponded to the lowest x7 value of the respective dental arch form group, and the maximum value of this interval was obtained by adding the class amplitude value of the respective group to the minimum or lowest x7 value. In the second interval, the minimum value was established by adding 0.05 mm to the maximum value of the previous interval or subgroup 1, and the maximum value of the second interval was established by adding the class amplitude value to its minimum value. The third interval was obtained with the same procedures to establish the second interval or subgroup (Table I). After establishing the subgroups, the curves of each dental arch form group were divided into 3 established sizes according to their x7 values, and, by applying the arithmetic mean to the x and y values of curve segments of each interval, the average curves representing the 3 subgroups (small, medium, and large) were obtained for each group of dental arch forms. To establish the average curve of a normal dental arch, 14 mean x values and 14 mean y values were calculated based on the arithmetic mean of all x and y values of the 126 curve segments organized in a table; this provided the positions of the Cartesian points to establish the possible form of a dental arch with normal occlusion. For the graphic representations of average curves calculated for the groups, subgroups, and normal occlusion, the mean x and y values of each group and the 10.e18 Triviño, Siqueira, and Scanavini American Journal of Orthodontics and Dentofacial Orthopedics January 2008 Figure 2 is a graphic representation of the dental arches in our sample, in small, medium, and large sizes. The medium size of form G is shown as a dotted line because it is a superimposed curve, since in the study sample there was not a curve segment corresponding to subgroup 2. The results of the evaluation of error of the visual classification of the 126 curve segments showed a high index of agreement of our methodology, with a P value of 95.24%; only 6 curve segments were not equally scored in the 2 evaluations by the examiner (T.T.). With regard to the error of measurement of the x and y values, the results of evaluations of systematic error with a paired t test and the casual error measured with the Dahlberg formula40 are given in Table IV, in which no P values were less than .05 and the casual errors were near zero, showing the accuracy of this method. DISCUSSION Fig 2. Graphic representations of the 8 dental arch forms for natural normal occlusion, in small, medium, and large sizes. corresponding subgroup, as well as the possible form representing the dental arch with normal occlusion, were plotted in the software Curve Expert to obtain the corresponding polynomial function and its graphic representation, and to illustrate their forms. RESULTS Table II gives the mean values and corresponding standard deviations of the x and y values of points in curve segments representing dental arch forms A to H and also the mean x and y values of the 14 points representing the teeth and corresponding standard deviations. These values allowed establishment of a possible “ideal” form for a dental arch with natural normal occlusion, illustrated in Figure 3, A. Table III shows the quantitative and percent incidence of thecurve segments according to sex and the quantitative incidence of these curve segments and corresponding percentages in the 3 subgroups of the 8 groups of dental arch forms. In the literature, there is much diversity among authors in the choice of reference points to evaluate dental arch forms and dimensions: cusp tips,2,14,22,27-29,31,33,36,37 contact points,10,20 alveolar bone ridges,6,7 mesiodistal widths of anterior teeth,9,10,18,19 and cranial structures.16,18 However, as in other studies, we selected labial and buccal dental surfaces to determine representations or drawings of curve segments that would simulate the archwires to be inserted into bracket slots or used as a template for archwire fabrication during orthodontic treatment.10-12,17,21,26,30 Some studies have demonstrated the quality of the fourth-degree polynomial to establish the dental arch form,30,32,33,36,37 whereas Hechter35 advocated the use of a simpler second-degree polynomial. Nevertheless, Ferrario et al36 and Wakabayashi et al37 observed that the higher the degree of the polynomial, the most precise the graphic description of the dental arch. The sixth-degree polynomial equation was the function that best described dental arch configuration, since polynomial functions with lower degrees compromised the descriptions of some important dental arch regions, such as anterior curvature of the mandibular arch, which is determined by intercanine distance, and posterior tooth alignment,8,20,24 whereas polynomials higher than the sixth degree had graphic representations of the curve of the dental arch form with a wavy, rather than smooth, tendency. In our sample of 126 curve segments from 63 dental casts, we identified more than the 3 dental arch forms for Brazilians with natural normal occlusion found by Telles23 and McLaughlin et al.24 Interpretation of the curves provided by the Curve Expert showed that curve morphology in the anterior region has 8 forms, which Triviño, Siqueira, and Scanavini 10.e19 American Journal of Orthodontics and Dentofacial Orthopedics Volume 133, Number 1 Table II. Mean x and y values and corresponding standard deviations of curve segments of the 8 forms and the average curve Form A Measurements Mean x7 and x14 x6 and x13 x5 and x12 x4 and x11 x3 and x10 x2 and x9 x1 and x8 y7 and y14 y6 and y13 y5 and y12 y4 and y11 y3 and y10 y2 and y9 y1 and y8 2.81 2.49 2.24 1.96 1.51 0.88 0.29 1.62 2.67 3.38 4.09 4.73 5.12 5.28 Form B Form C Form D Form E Form F Form G Form H Average curve SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD 0.13 0.10 0.10 0.10 0.07 0.06 0.05 0.28 0.30 0.30 0.32 0.33 0.34 0.35 2.83 2.50 2.26 2.00 1.56 0.88 0.29 1.64 2.71 3.41 4.14 4.80 5.18 5.33 0.17 0.14 0.14 0.13 0.09 0.07 0.05 0.27 0.33 0.31 0.32 0.30 0.32 0.33 2.87 2.58 2.30 2.00 1.53 0.90 0.29 1.59 2.68 3.38 4.08 4.72 5.14 5.30 0.15 0.13 0.10 0.07 0.06 0.03 0.04 0.27 0.28 0.31 0.27 0.25 0.23 0.23 2.83 2.56 2.32 2.05 1.53 0.88 0.28 1.52 2.62 3.28 4.00 4.68 5.05 5.21 0.19 0.14 0.15 0.11 0.08 0.05 0.04 0.21 0.22 0.22 0.22 0.26 0.28 0.28 2.87 2.49 2.16 1.89 1.45 0.86 0.29 1.67 2.75 3.47 4.14 4.76 5.18 5.36 0.11 0.09 0.11 0.08 0.05 0.04 0.03 0.23 0.27 0.25 0.27 0.29 0.29 0.29 2.78 2.51 2.23 1.91 1.48 0.88 0.28 1.56 2.64 3.34 4.02 4.65 5.08 5.26 0.13 0.12 0.12 0.07 0.09 0.06 0.04 0.16 0.19 0.20 0.21 0.23 0.24 0.25 2.77 2.50 2.17 1.83 1.40 0.83 0.32 1.88 2.93 3.58 4.25 4.88 5.27 5.50 0.09 0.07 0.13 0.06 0.11 0.05 0.05 0.27 0.24 0.20 0.18 0.16 0.08 0.07 2.71 2.52 2.28 1.95 1.49 0.87 0.28 1.55 2.65 3.32 4.04 4.67 5.05 5.23 0.17 0.18 0.15 0.11 0.08 0.05 0.03 0.26 0.28 0.27 0.23 0.25 0.26 0.28 2.80 2.52 2.25 1.96 1.50 0.88 0.29 1.60 2.68 3.37 4.08 4.72 5.12 5.29 0.16 0.14 0.14 0.11 0.09 0.06 0.04 0.26 0.28 0.28 0.28 0.28 0.29 0.30 Fig 3. A, Graphic representations of average forms of natural normal occlusion, obtained by the arithmetic means of x and y values of the 126 curve segments; B, superimposition of mean normal form (blue) and form C (black). were organized in groups and named forms A, B, C, D, E, F, G, and H; this agreed with some studies that the application of the sixth-degree polynomial to establish the dental arch form showed that the dental arch cannot be represented by a simple geometric shape such as a parabolic curve, hyperbola, ellipsis, or catenary curve (Fig 2).26,30,34 According to the results, form A has similar characteristics to forms observed by Engel13 and Raberin et al,22 with flattening of the anterior curve region and the origin of the curvature at the distal region of the lateral incisors. In agreement with the incidence of 18.4% observed by Raberin et al,22 form A had 28 curve segments, representing 22% of the total sample, and was the most frequent form in subjects with normal occlusion. The curve representing form B showed a similar configuration as form A—ie, mandibular incisors arranged in a straight line. However, its intercanine distance was slightly wider than in form A. Form B is considered esthetically unpleasant by orthodontic specialists because it causes a tight, narrow smile.41 This form is rarely found in the literature, except for the report of Triviño and Vilella,26 who observed a frequency of 31.2%, which was the predominant form in that study. In our study, form B had a medium incidence value—15% of the sample, or 19 curve segments. With opposite graphic aspects to the aforementioned forms, in form C, the anterior teeth are roundly arranged, as in an ellipsis, also described by other diagrams.10,13,16,21-24 Even though its incidence reached medium values (10% of the total 10.e20 Triviño, Siqueira, and Scanavini American Journal of Orthodontics and Dentofacial Orthopedics January 2008 Table III. Quantitative distribution of curve segments and corresponding percentages according to sex in the 3 subgroups of the 8 groups of dental arch forms Female Male Subgroup 1 Subgroup 2 Subgroup 3 Form n % n % n % n % n % A B C D E F G H 12 11 8 7 9 9 2 12 43 58 67 64 64 56 67 52 16 8 4 4 5 7 1 11 57 42 33 36 36 44 33 48 4 5 2 2 2 5 2 11 14.3 26.3 16.7 18.2 14.3 31.3 66.7 47.8 13 10 6 7 10 7 0 10 46.4 52.6 50.0 63.6 71.4 43.8 0.0 43.5 11 4 4 2 2 4 1 2 39.3 21.1 33.3 18.2 14.3 25.0 33.3 8.7 Table IV. Arithmetic means and standard deviations of measurements in both evaluations, paired t test, and Dahlberg error analysis Evaluation 1 Evaluation 2 Measurements Mean SD Mean SD P Casual error x7 and x14 x6 and x13 x5 and x12 x4 and x11 x3 and x10 x2 and x9 x1 and x8 y7 and y14 y6 and y13 y5 and y12 y4 and y11 y3 and y10 y2 and y9 y1 and y8 2.76 2.47 2.22 1.93 1.47 0.87 0.28 1.58 2.67 3.36 4.04 4.68 5.08 5.26 0.14 0.12 0.11 0.09 0.08 0.06 0.05 0.23 0.24 0.26 0.26 0.27 0.28 0.29 2.76 2.46 2.22 1.93 1.47 0.86 0.29 1.58 2.67 3.36 4.04 4.68 5.08 5.26 0.14 0.12 0.10 0.09 0.07 0.07 0.06 0.24 0.24 0.26 0.26 0.28 0.28 0.29 .33 .16 1.00 1.00 .33 .33 .33 .33 1.00 .33 1.00 .16 .58 .33 0.007 0.000 0.011 0.000 0.000 0.015 0.007 0.007 0.000 0.007 0.011 0.011 0.011 0.007 sample, or 12 curve segments), form C was the most often observed by Ricketts21 and Telles,23 representing 37.5% and 63.75% of their samples, respectively. The anterior region of form D is analogous with form C, although this form has a greater intercanine distance, and the incisors are positioned nearly in a plane, giving a quadrangular configuration for this form. Some authors observed similar forms in their studies,13,24,26 whereas others developed diagrams that established this dental arch form as ideal.10 In our study, only 9% of the sample, or 11 segments of curve, had this arch form; this agreed with other findings.26 Similar to the morphology of diagrams suggested by Bonwill,18 Hawley,9 and Sved,19 form E has a semicircular arrangement of the anterior teeth; therefore, the posterior region is not strictly straight. This form was observed in 14 curve segments (11% of our sample), differing from the incidence values found by Raberin et al22 (23.7%) and Telles23 (16.25%). Form F was observed in 16 curve segments, or 13% of the total sample; this is an example of a catenary curve described by other authors.10,12,13,20-24,26 The results of studies by Ricketts,21 Telles,23 Raberin et al,22 and Triviño and Vilella26 showed that this form has medium prevalence (15%, 20%, 18.7%, 24.2%, respectively) in the subjects analyzed. The curve segments representing form G illustrate a pointed anterior region like a groin. This was an infrequent dental arch configuration, observed in only 3 curve segments, accounting for 2% of the total sample of normal occlusion. This incidence was different from the results of Raberin et al22 and Triviño and Vilella,26 who found medium values of 19.4% and 12.4%, respectively. Form H was not commonly observed in previous studies, but it is similar to the shape of archwires advocated by Angle,42 Chuck,43 and Boone.44 Form H has a morphology that describes the projection of the Triviño, Siqueira, and Scanavini 10.e21 American Journal of Orthodontics and Dentofacial Orthopedics Volume 133, Number 1 mandibular central incisors and had the second highest frequency in this study, observed in 23 curve segments, or 18% of the sample, an incidence similar to the results of Triviño and Vilella,26 who also observed a significant frequency (23%). Based on Table III, subgroup 2 (medium size) had the most curve segments in forms A (46.4%), B (52.6%), C (50.0%), D (63.6%), E (71.4%), and F (43.8%), whereas forms G (66.7%) and H (47.8%) had a higher incidence of subgroup 1 (small size), even though form G had no segment in subgroup 2 because of our sample size. These results might be related to the anterior curve of each dental arch form. Forms G and H had pointed alignments of the incisors, with a smaller distance between homologous teeth at the canine region, and reduced sizes and more components with small size, as also observed for form F, which had a high incidence in subgroup 1 (31.25%). As stated by some authors, medium-sized dental arches are generally predominant in normal occlusion; according to the results, there were 63 curve segments in subgroup 2, or 50% of the total sample.8,21,26 With regard to the incidence of forms evaluated according to sex, all groups of forms included both sexes. As in the studies of Raberin et al22 and Triviño and Vilella,26 forms A, B, F, and H had homogeneous distributions between the sexes. Our extensive literature review and results suggested the need to inform orthodontic specialists about the representative forms of normal occlusion, in case they believe that there is an ideal form for this type of dental arch. Application of arithmetic means of x and y values of the 126 curve segments showed a possible average form for normal occlusion (blue) that is similar to the curve representing form C (black), as shown in Figure 3, B, which illustrates the superimposition of these 2 arch configurations. However, form C had a low incidence (10%) in our sample of normal occlusion; it was the sixth group of dental arch forms in increasing order. Therefore, establishing the “ideal” form for the normal dental arch no longer needs to be the objective in future studies, since our results show that a normal dental arch cannot be represented by a single form but, rather, by 8 forms with 3 sizes in each. Since form G had no segments in subgroup 2 because of the small sample, we established 23 possible mandibular dental arch forms. The establishment of 8 configurations for the dental arch in 3 sizes allows more accurate individualization of form and dimensions, thus reducing the occurrence of errors in the selection of the best form for a patient.2,8,11,17,26 These configurations also permit the fabrication of preformed archwires with the most common dental arch forms or templates to help in the manual contouring of archwires, eliminating the need to use dental casts during orthodontic treatment and consequently reducing the possibility of fracturing them. CONCLUSIONS According to our results, the mandibular dental arch can be represented by 8 forms. There is not 1 ideal or representative form of normal occlusion. Most arch forms were medium size, and the incidence of the 8 groups of forms according to sex was homogeneous. REFERENCES 1. Strang RHW. Factors of influence in producing a stable result in the treatment of maloclusion. Am J Orthod Oral Surg 1946;32: 313-32. 2. Ricketts RM. A detailed consideration of line of occlusion. Angle Orthod 1978;48:274-82. 3. Strang RHW. The fallacy of denture expansion as a treatment procedure. Angle Orthod 1949;14:12-22. 4. Lear CSC, Moorrees CFA. Bucco-lingual muscle force and dental arch form. Am J Orthod 1969;56:379-93. 5. Vaden JL, Dale JG, Klontz HA. The Tweed-Merrifield edgewise appliance: philosophy, diagnosis and treatment. In: Graber MT, Vanarsdall RLJ. Orthodontics: current principles and techniques. 2nd ed. St. Louis: Mosby; 1994:579-635. 6. Strang RHW. Factors associated with successful orthodontic treatment. Am J Orthod 1952;38:790-800. 7. Andrews LF, Andrews WA. The syllabus of the Andrews® orthodontic philosophy. 9th ed. San Diego: L. F. Andrews Foundation; 2001. p. 7-29. 8. Interlandi S. New method for establishing arch form. J Clin Orthod 1978;12:843-5. 9. Hawley CA. Determination of the normal arch and its application to orthodontia. Dent Cosmos 1905;47:541-52. 10. Monti AE. Textbook of orthodontics. 3rd ed. 1958. Editorial “El Ateneo”; Buenos Aires: p. 221-36. 11. Capelozza L Jr, Capelozza JAZ. OAID: Objective anatomic individual diagram. A proposal for choosing the form of the arches in the straight-wire tecnique, based on both the anatomic individuality and the aims of the treatment. Rev Clin Ortodon Dental Press 2004;3:84-92. 12. Scott JH. The shape of the dental arches. J Dent Res 1957;36: 996-1003. 13. Engel GA. Preformed arch wires: reliability of fit. Am J Orthod 1979;76:497-504. 14. Currier JH. A computerized geometric analysis of human dental arch form. Am J Orthod 1969;56:164-79. 15. Biggerstaff RH. Three variations in dental arch form estimated by a quadratic equation. J Dent Res 1972;51:1509. 16. Izard G. New method for the determination of the normal arch by the function of the face. Int J Orthod Oral Surg Radiog 1927;13: 582-95. 17. Brader AC. Dental arch form related with intraoral forces: PR ⫽ C. Am J Orthod 1972;61:541-61. 18. Bonwill WGA. The scientific articulation on the human teeth as founded on geometrical, mathematical and mechanical laws. Dent Items Interest 1899;21:617-43. 10.e22 Triviño, Siqueira, and Scanavini American Journal of Orthodontics and Dentofacial Orthopedics January 2008 19. Sved A. Mathematics of the normal dental arch. Dent Cosmos 1917;59:1116-24. 20. Savostin-Asling I. The geometric analysis of mandibular dental arch form. Ann Dent 1980;39:3-11. 21. Ricketts RM. Provocations and perceptions in cranio-facial orthopedics. Dental science and facial art— book 1 (part 2). Denver: Rocky Mountain Orthodontics; 1989. p. 686-711. 22. Raberin M, Laumon B, Martin JL, Brunner F. Dimensions and form of dental arches in subjects with normal occlusions. Am J Orthod Dentofacial Orthop 1993;104:67-72. 23. Telles FS. Contour diagrams: presentation of a new contour diagram. Rev Soc Parana Ortodon 1995/96;1:29-36. 24. McLaughlin R, Bennett J, Trevisi H. MBT™ arch form and archwire sequencing—part 2. Rev Dent Press Ortodon Ortopedi Facial 1998;3:39-48. 25. Noroozi H, Nik TH, Saeeda RBS. The dental arch form revisited. Angle Orthod 2001;71:386-9. 26. Triviño T, Vilella OV. Forms and dimensions of the lower dental arch. Rev Soc Bras Ortodon 2005;5:19-28. 27. BeGole EA. Application of the cubic spline function in the description of dental arch form. J Dent Res 1980;59:1549-56. 28. Valenzuela PA, Pardo MA, Yezioro S. Description of dental arch form using the Fourier series. Int J Adult Orthod Orthognath Surg 2002;17:59-65. 29. Taner T, Ciger S, El H, Germeç D, Es A. Evaluation of dental arch width and form changes after orthodontic treatment and retention with a new computerized method. Am J Orthod Dentofacial Orthop 2004;126:464-76. 30. Kageyama T, Domínguez-Rodríguez GC, Vigorito JW, Deguchi T. A morphological study of the relationship between arch dimensions and craniofacial structures in adolescents with Class II Division 1 malocclusions and various facial types. Am J Orthod Dentofacial Orthop 2006;129:368-75. 31. Nie Q, Lin J. A comparison of dental arch forms between Class II Division 1 and normal occlusion assessed by euclidean distance matrix analysis. Am J Orthod Dentofacial Orthop 2006;129:528-35. Lu KH. An orthogonal analysis of the form, symmetry, and asymmetry of the dental arch. Arch Oral Biol 1966;11:1057-69. Sanin C, Savara BS, Thomas DR, Clarkson QD. Arc length of the dental arch estimated by multiple regression. J Dent Res 1970;49:885. Pepe SH. Polynomial and catenary curve fits to human dental arches. J Dent Res 1975;54:1124-32. Hechter FJ. Symmetric and dental arch form of orthodontically treated patients. J Can Dent Assoc 1978;44:173-84. Ferrario VF, Sforza C, Miani AJ, Tartaglia G. Mathematical definition of the shape of dental arches in human permanent healthy dentitions. Eur Orthod Soc 1994;16:287-94. Wakabayashi K, Sohmura T, Takahashi J, Kojima T, Akao T, Nakamura T, et al. Development of the computerized dental cast form analyzing system—three dimensional diagnosis of dental arch form and the investigation of measuring condition. Dent Mater J 1997;16:180-90. Ferrario VF, Sforza C, Dellavia C, Colombo A, Ferrari RP. Three-dimensional hard tissue palatal size and shape: a 10-year longitudinal evaluation in healthy adults. Int J Adult Orthod Orthognath Surg 2002;17:51-8. Andrews LF. The six keys to normal occlusion. Am J Orthod 1972;62:296-309. Houston WJB. The analysis of errors in orthodontic measurements. Am J Orthod 1983;83:382-90. Roden-Johnson D, Gallerano R, English J. The effects of buccal corridor spaces and arch form on smile esthetics. Am J Orthod Dentofacial Orthop 2005;127:343-50. Angle EH. The lastest and best in orthodontic mechanism. Dent Cosmos 1928;52:1143-58. Chuck GC. Ideal arch form. Angle Orthod 1934;4:312-27. Boone GN. Archwires designed for individual patients. Angle Orthod 1963;33:178-85. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44.