Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
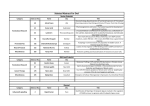
J Med Sci 2006;26(2):065-068 http://jms.ndmctsgh.edu.tw/2602065.pdf Copyright © 2006 JMS Wen-Chiuan Tsai, et al. Primary Neuroendocrine Carcinoma of the Breast Wen-Chiuan Tsai1, Jyh-Cherng Yu2, Lai-Fa Sheu1, and Shin Nieh1* 1 Department of Pathology, 2Division of General Surgery, Department of Surgery, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan, Republic of China Definitions and classifications of primary neuroendocrine (NE) carcinomas of the breast were first proposed by the World Health Organization (WHO) in 2003. Here we present a case of large-cell neuroendocrine carcinoma of the breast with regional nodal metastasis, which was diagnosed using cell morphology and immunohistochemical staining. We also reviewed 32 reported cases of primary breast NE carcinoma to identify prognostic factors associated with classes of this type of breast carcinoma defined according to the most recent WHO classification system. To our knowledge, this is the first study of breast carcinoma prognosis using the new WHO classification system. Key words: breast cancer, carcinoid tumor, neuroendocrine carcinoma, solid growth pattern INTRODUCTION Primary NE carcinoma of the breast is rare, and histological patterns vary between cases1. The World Health Organization (WHO) classifies this type of breast cancer into three histological types according to the morphology of the tumor cells: solid neuroendocrine (NE) carcinoma, small or oat-cell carcinoma, and large-cell NE carcinoma2. Most studies show that prognosis is correlated with the clinical stage of the cancer, as compared with other breast malignant tumors1. However, a report by Sapino and associates revealed that the growth pattern of neuroendocrine differentiation may influence the classification of the tumor when it is classed according to the current grading system3. Until now, prognostic and therapeutic protocols have been controversial. The aim of this study was to provide sufficient clinical data to resolve this issue. CASE REPORT An 83-year-old female patient presented with a firm, nontender mass in the upper, outer quadrant of the left breast without associated symptoms. A mass-lesion of the left breast was identified by laboratory and physical Received: August 1, 2005; Revised: September 15, 2005; Accepted: September 22, 2005. * Corresponding suthor: Shin Nieh, Department of Pathology, Tri-Service General Hospital, 325, Cheng-Gong Road Section 2, Taipei 114, Taiwan, Republic of China. Tel: +886-28792-7155; Fax: +886-2-8792-7159; E-mail: ab95057@ hotmail.com Fig. 1 (A): Nests of tumor cells with hyperchromatic nuclei, granular cytoplasm and abundant extracellular mucin secretion separated by dense collagen bundles (H & E stain, ×200). (B): More than 50% of tumor cells showed diffuse staining for chromogranin A (IHC, ×200). examination. Subsequent mammography and mammary ultrasound both revealed a solitary and poorly demarcated tumor. As we suspected malignancy, we performed a core biopsy and diagnosed infiltrating ductal carcinoma of the breast. We recommended modified radical mastectomy and dissection of the axillary lymph nodes, which were subsequently performed. On gross examination, the resected breast measured 24 cm ×23 cm×9 cm and contained one tumor measuring 1.7 cm×1.5 cm×1 cm and several axillary lymph nodes. Microscopically, median-sized, hyperchromatic tumor cells with faintly granular cytoplasms were separated by dense collagen bundles arranged in solid nest pattern with abundant extracellular mucin production (Fig. 1A). The dissected axillary lymph nodes showed no evidence of tumor metastasis. Immunohistochemical studies revealed that 65 Prognosis of breast neuroendocrine carcinoma the tumor cells were immunoreactive for chromogranin A (Fig. 1B), synaptophysin, neuron-specific enolase (NSE), mucin, estrogen and progesterone receptors, but negative for thyroid transcription factor-1 (TTF-1) and carcinoembryonic antigen (CEA). These morphological and immunohistochemical findings confirmed the diagnosis of primary large-cell NE carcinoma. The patient was given tamoxifen (20 mg/d) and was healthy and showed no evidence of recurrence at a follow-up visit 6 months after surgery. Table 1 The classification and prognosis of the 32 reported primary breast NE carcinoma cases Paper No. of Cases Zekioglu9 Growth WHO Type classification Solid cohesive Solid NE carcinoma No LNs metastasis MRM and adjuvant C/T Still alive after 48 months follow up 2 Solid papillary Solid NE carcinoma No LNs metastasis MRM and adjuvant C/T Still alive after 54 months follow up 5 Cellular Large cell NE mucinous carcinoma Only one case had LNs meta MRM and adjuvant C/T Still alive after 24 months follow up Yamasaki10 1 Small cell 66 Outcome (Mean follow up time: 26.2 months) 4 DISCUSSION carcinoma of the breast is a specific type of cancer that exhibits a high level of histological Shin11 neuroendocrine marker expression in the majority of tumor cells. In 1963, Ferter and Hartmann first described two breast carcinomas with carcinoid patterns4. The term “primary carcinoid tumor” of the breast was introduced in 1977 by Cubilla and Woodruff to characterize a new group of neoplasms5. They also concluded that primary Our case mammary carcinoid tumor is a neuroendocrine neoplasm derived from argyrophilic cells of neural-crest origin. In most of the early studies, primary breast NE carcinoma was diagnosed using Grimeliu’s stain and electron microscopy6. However, according to some reports, only 5-10% of ordinary breast carcinomas contain tumor cells with dense core granules and are positive for Grimeliu's stain7,8. Together with the 2003 WHO classification, the diagnosis of primary breast NE carcinoma has emphasized the importance of morphological features and immunohistochemical expression2. Our case revealed nested, hyperchromatic tumor cells with extracellular mucin production, which were surrounded by collagenous fibers and exhibited diffuse, positive staining for neuroendocrine markers. We also performed chest Xray, abdominal sonography, and panendoscopy, which revealed no evidence of distal metastasis. The diagnosis of primary solid NE carcinoma of the breast was confirmed by morphological and immunohistochemical findings. The prognosis of primary breast neuroendocrine carcinoma has not been extensively studied and, according to most of the available information, seems to correlate to a greater extent with presentation of clinical stage than with the degree or pattern of neuroendocrine differen-tiation. We reviewed 32 reported cases of primary breast NE carcinoma with long-term follow-up between 2000 and 2004, which were classed into three categories according LN status Treatment Small cell No LNs Lumpectomy and Still alive after 18 NE carcinoma metastasis adjuvant C/T months follow up 10 Small cell Small cell NE carcinoma MRM and adjuvant C/T or R/T 6 cases expired 4 cases still alive (mean follow up time: 19 m) 9 Small cell Small cell NE 6 of 9 cases carcinoma had LNs meta. MRM and adjuvant C/T 6 cases expired 3 cases still alive (mean follow up time 23 m) 1 MRM and adjuvant H/T Still alive after 6 months follow up Alveolar Solid NE carcinoma 6 of 10 cases had LNs meta No LNs metastasis to the most recent WHO classification system (Table 1). Those tumors included seven cases of the solid type of primary carcinoma, five of the large-cell type, and 20 of the small-cell type9-11. All of the subjects with solid and largecell types of breast NE carcinoma survived tumor excision with adjuvant chemotherapy and/or radiotherapy, and only one case had axillary lymph node metastasis. However, 12 of the 20 cases with primary small-cell NE carcinoma of the breast had axillary lymph node metastasis and expired after tumor excision and adjuvant therapy. Regional lymph node metastasis may be the most important determinant of a poor prognosis in primary neuroendocrine carcinoma of the breast. Small-cell carcinoma tends to develop metastasis along the lymphatic channel (Table 2). However, the relationship between lymph node metastasis and survival rate was not statistically significant (P>0.05, Pearson product moment correlation) because of the small number of cases studied. More information is required before a definitive conclusion is made regarding primary NE carcinoma of the breast. In conclusion, with exception of the small-cell type, cases of primary breast NE carcinoma displayed satisfactory prognosis after adequate tumor excision and adjuvant therapy. However, it is important to distinguish between Wen-Chiuan Tsai, et al. Table 2 The relationship between lymph node metastasis and survival of 32 reported cases of primary breast NE carcinoma classed according to the 2003 WHO classification system WHO classification Solid NE carcinoma Large cell NE carcinoma Small cell NE carcinoma No. of No. of Cases of LNs Survival cases/ total cases metastasis/ total cases total cases 7 5 20 0/7 1/5 (20%) 12/20 (60%) 7/7 (100%) 5/5 (100%) 8/20 (40%) metastatic carcinoid tumors and primary NE carcinoma of the breast because of differences in the required management and the prognoses. To date, there have been 15 reported cases of metastatic carcinoid tumors of the breast, 12 of which metastasized from the small intestine; the remaining three metastasized from the pancreas, bronchus, and ovary13. In our opinion, further examinations such as panendoscopy, abdominal sonography, and chest X-ray should be performed to prevent incorrect diagnosis and management. REFERENCES 1. Ajisaka H, Maeda K, Miwa A, Yamamoto K. Breast cancer with endocrine differentiation: report of two cases showing different histologic patterns. Surg Today 2003;33:909-912. 2. Tavassoli FA, Devilee P. WHO Classification of Tumors: Tumors of the Breast and Female Genital Organs. Lyon: IARC press, 2003:32-34. 3. Sapino A, Righi L, Cassoni P, Papotti M, Pietribiasi F, Bussolati G. Expression of the neuroendocrine phenotype in carcinomas of the breast. Semin Diagn Pathol 2000;17:127-137. 4. Feyrter F, Hartmann G. On the carcinoid growth from of the carcinoma mammae, especially the carcinoma solidum (gelatinosum) mammae. Frankf Z Pathol 1963; 73:24-39. 5. Cubilla AL, Woodruff JM. Primary carcinoid tumor of the breast: A report of eight patients. Am J Surg Pathol 1997;1:283-292. 6. Clayton F, Sibley RK, Ordonez NG, Hanssen G. Argyrophilic breast carcinomas. evidence of lactational differentiation. Am J Surg Pathol 1982;6:323-333. 7. Azzopardi JG, Muretto P, Goddeeris P, Eusebi V, Lauweryns JM. “Carcinoid” tumor of the breast; the morphological spectrum of argyrophil carcinomas. Histopathology 1982;6:549-569. 8. Toyoshima S. Mammary carcinoma with argyrophil cells. Cancer 1983;52:2129-2138. 9. Zekioglu O, Erhan Y, Ciris M, Bayramoglu H. Neuroendocrine differentiated carcinoma of the breast: a distinct entity. Breast 2003;12:251-257. 10. Yamasaki T, Shimazaki H, Aida S, Tamai S, Tamaki K, Hiraide H, Mochizuki H, Matsubara O. Primary small cell (oat cell) carcinoma of the breast: report of a case and review of the literature. Pathol Int 2000;50: 914-918. 11. Shin SJ, DeLellis RA, Ying L, Rosen PP. Small cell carcinoma of the breast: a clinicopathologic and immunohistochemical study of nine patients. Am J Surg Pathol 2000;24:1231-1238. 12. Rubio IT, Korourian S, Brown H, Cowan C, Klimberg VS. Carcinoid tumor metastatic to the breast. Arch Surg 1998;133:1117-1119. 13. Mosunjac MB, Kochhar R, Mosunjac MI, Lau SK. Primary small bowel carcinoid tumor with bilateral breast metastases: report of two cases with different clinical presentations. Arch Pathol Lab Med 2004;128: 292-297. 67 Prognosis of breast neuroendocrine carcinoma 68