Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
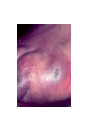
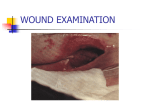
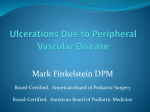
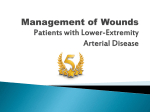
PATIENT PRESENTATION Overview of Lower Extremity Skin Changes Penny Husser BSN RN CWOCN LOWER EXTREMITY WOUNDS • LEAD-Lower-Extremity Arterial Disease • LEVD-Lower-Extremity Venous Disease • LEND- Lower-Extremity Neuropathic Disease LEAD Lower-Extremity Arterial Disease • Commonly referred to as peripheral vascular disease(PVD) • Peripheral arterial occlusive disease (PAOD) • Peripheral arterial disease(PAD) CONCERNS • Cardiovascular disease is the NO. 1 cause of death in the U.S. • LEAD is under-diagnosed, under-appreciated and under-treated in approx. 50% of patients • 50% of patients are asymptomatic or unaware of their condition because of atypical leg symptoms (absence of claudication) CONCERNS • Early diagnosis and preventive care can prevent ischemic events • Diabetes and smoking 1 pack of cigarettes daily are significantly associated with asymptomatic LEAD • Nicotine Replacement Therapy does not affect wound healing ( smoking causes vasoconstriction) RISK FACTORS • Advanced age. • Smoking. • Diabetes. • Hyperlipidemia. • Hypertension. • Hyperhomocysteinemia. • Chronic renal insufficiency. • Family history of cardiovascular disease. • Ethnicity. RISK FACTORS • Cardiovascular disease. • Vascular procedures or surgeries. • Sickle cell anemia. • Obesity. PRESENTATION • • • • • • • • • • • • • Diminished/absent dorsalis pedis/posterior tibial pulses. Cyanosis. Pallor on elevation and dependent rubor. Prolonged capillary/venous refill. Loss of hair on lower limb. Atrophy of skin, subcutaneous tissue, and muscle. Shiny, taut, thin, dry skin. Skin temperature cool to touch. Decreased sensation. Weakness of limb, gait abnormalities. Pain (e.g., intermittent claudication, rest pain, nocturnal pain); pain on elevation. Paresthesias. Dystrophic (i.e., abnormal) nails PRESENTATION • Base: Pale; granulation rarely present; necrosis common; eschar may be present. • Size: Variable; often small. • Depth: May be deep. •Margins: Edges rolled, smooth, undermined; punched-out appearance. • Exudate: Minimal. • Infection: Frequent (signs may be subtle). • Pain: Common. • Non-healing; often precipitated by minor trauma EXAMPLES OF LEAD TESTING • • • • • • Increased Capillary refill Transcutaneous Oxygen (TcPO2) Toe Brachial Index (TBI) Toe systolic pressure (TP) Critical limb ischemia (CLI) Ankle Brachial Index (ABI) TESTING • • • • • • • ABI Perfusion Status > 1.3 Elevated, incompressible vessels > 1.0 Normal < 0.9 LEAD < 0.6 to 0.8 Borderline < 0.5 Severe ischemia < 0.4 Critical ischemia, limb threatened LIMITATIONS • The ABI is an indirect examination that infers the anatomical location of an occlusion or stenosis. The exact location of the stenosis or occlusion cannot be determined by ABI alone • The ABI might be elevated (> 1.3) due to calcification of medial arteries at the ankle in patients with diabetes, renal failure and rheumatoid arthritis; and in such cases, other vascular tests should be performed TREATMENT • Prevent trauma/injury. • Identify/treat infection. • Promote wound healing. • Minimize pain. • Preserve limb. TREATMENT • Referral to a Vascular Surgeon for Further Evaluation/Testing • Urgent Referral to a Vascular Surgeon or Emergency Room – 1. Gangrene. – 2. Wound infection or cellulitis in an ischemic limb. – 3. Sudden onset of 6 Ps (i.e., pain, pulselessness, pallor, parathesia, paralysis, polar[coldness]), which indicates acute limb ischemia associated with a thrombosis. LEVD Lower-Extremity Venous Disease • Commonly referred to as peripheral vascular disease(PVD) • Chronic Venous Disease (CVD’s) • Chronic Venous Insufficiency(CVI) • Chronic Venous Ulcer (CVU) EXAMPLES OF LEVD CONCERNS • Approximately 7 million individuals worldwide have LEVD • Approximately 3 million will develop ulcerations • Account for 80-90% of all leg ulcers • Refractory in nature • Affect quality of life RISK FACTORS • Advanced age. • Obesity. • Pregnancy. • Thrombophilia. • Systemic inflammation. • Anticardiolipin antibody. • Venous thromboembolism (VTE)/phlebitis. • Varicose veins. • Pulmonary embolus RISK FACTORS • Simultaneous insufficiency of two out of three venous systems. • Sedentary lifestyle or occupation; reduced mobility. • Trauma/surgeries/leg fractures. • Impaired calf muscle pump. • Restricted range of motion of the ankle. • Family history of venous disease. • Injection drug user. • Previous wound. RISK FACTORS • Congestive heart failure. • Lymphedema. • Orthopedic procedures PRESENTATION • Base: Ruddy red; granulation tissue present; yellow adherent or loose slough may be present. • Size: Variable; can be large. • Depth: Usually shallow. • Margins: Irregular; undermining or tunneling are uncommon. • Exudate: Moderate to heavy. • Infection: Not common. PRESENTATION • Edema: Pitting or non-pitting; worsens with prolonged standing or sitting with legs dependent. • Scarring from previous wounds. • Venous dermatitis (e.g., erythema, itching, vesicles, weeping, scaling, crusting, afebrile). • Hemosiderosis (i.e., brown staining). • Lipodermatosclerosis. • Maceration. • Temperature: Normally warm to touch. PRESENTATION • Leg pain may be variable: Dull aching, itchy, sore, tender; severe sharp or throbbing. • The pain may be accompanied by complaints of heaviness. • The leg pain worsens with dependency. • Elevation relieves pain. TESTING • Venous Reflux Studies • Vascular studies rule out LEAD: TREATMENT • • • • • • • • • • Refer to Vascular for Intervention, obliterate damaged veins Control edema. Absorb exudate Compression therapy- 30–42 mmHg compression at the ankle Increase exercise Control weight Identify/treat infection. Promote wound healing/maintain moist wound surface. Protect periwound skin. Minimize pain. , LEND- Lower-Extremity Neuropathic Disease • NEUROPATHIC ULCERS • DIABETIC ULCERS PREDISPOSING FACTORS • • • • • Diabetes/impaired glucose tolerance. Smoking Alcoholism Chemotherapy Hypertension, obesity, Raynaud’s disease, scleroderma, hyperthyroidism, hypothyroidism, chronic obstructive pulmonary disease. • Charcot-Marie-Tooth disease. • Spinal cord injury; neuromuscular diseases; abdominal, pelvic and orthopedic procedures. PREDISPOSING FACTORS • Lower-extremity arterial disease. • Kidney disease. APPERANCE • Base: Pale, pink; necrosis/eschar may be present. • Margins: Edges well defined, smooth; undermining may be present. • Callus formation over bony prominences (might cover a wound), and periwound. • Edema: Localized area with erythema may indicate high pressure/inflammation. RISK FACTORS • Musculo-skeletal/foot deformities. Diabetic skin markers: Dermopathy, necrobiosis lipoidica, acanthosis nigricans, bullosis diabeticorum. Infection/Cellulitis. • Arterial ischemia. • Osteomyelitis. • Charcot fracture (e.g., swelling, pain, erythema, localized temperature elevation of 3–7° C). • Gangrene. EXAMPLES OF LEND EXAMPLES OF LEND TESTING • Decreased or altered sensitivity to touch occurs. • Pain may be superficial, deep, aching, stabbing, dull, sharp, burning, or cool. • Altered sensation not described as pain (e.g., numbness, warmth, prickling, tingling, shooting, pins and needles; “stocking-glove pattern”) may be present. • Pain may be worse at night. • Allodynia (i.e., intolerance to normally painless stimuli such as bed sheets touching feet/legs) may occur. LIMITATIONS • Use occlusive dressings cautiously. • Use dressings that maintain a moist surface, absorb exudate and allow easy visualization. TREATMENT • Stop smoking. • Revascularize if ischemic. • Maintain tight glucose/glycemic control; control hypertension. • Engage in exercise that is adapted to prevent injury. • Consider medications, as indicated. TREATMENT • Reduce shear stress and offload wounds • Use assistive devices for support, balance and additional offloading. • Use pressure redistribution for heels, toes, and bony prominences, especially if in bed • routine professional nail/callus care. • Avoid chemical, thermal, mechanical injury (e.g., no bare feet even in the house; no hot soaks or heating pads; no medicated corn pads; wear socks/stockings with shoes). REFERENCES • • • • • • • (Bonham, 2006; Bonham et al., 2007, 2010; Hirsch et al., 2006; WOCN®, 2008). (Bonham, 2006; Bonham et al., 2007; Criqui et al., 1989; Rumwell & McPharlin, 2009). WOCN®, 2008). (Carmel, 2012). Wound, Ostomy and Continence Nurses Society. (2008). Guideline for management of wounds in patients with lowerextremity arterial disease. Mt. Laurel, NJ: Author. Wound, Ostomy and Continence Nurses Society. (2011). Guideline for management of wounds in patients with lowerextremity venous disease. Mt. Laurel, NJ: Author. Wound, Ostomy and Continence Nurses Society. (2012). Guideline for management of wounds in patients with lowerextremity neuropathic disease. Mt. Laurel, NJ: Au