Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
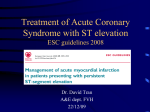
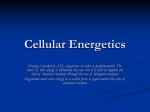
148 Superoxide Dismutase Plus Catalase Improve Contractile Function in the Canine Model of the "Stunned Myocardium" Karin Przyklenk and Robert A. Kloner From the Department of Medicine, Harvard University and Brigham and Women's Hospital, Boston, Massachusetts, and Department of Medicine, Wayne State University and Harper Hospital, Detroit, Michigan Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 SUMMARY. Fifteen minutes of coronary occlusion followed by reperfusion does not result in myocardial necrosis; however, the contractile function and high energy phosphate content of the previously ischemic myocardium remains depressed or 'stunned' for several hours to days after reperfusion. Oxygen-derived free radicals have been implicated in ischemia and reperfusioninduced injury in a variety of tissues. We wished to determine whether administration of free radical scavengers superoxide dismutase plus catalase before and during occlusion, and throughout reperfusion, could attenuate the 'stunning' produced by 15 minutes of left anterior descending coronary artery occlusion in anesthetized, open-chest dogs. Segment shortening in the previously ischemic zone recovered to within only ±10% of preinfusion values in the control group during 3 hours of reperfusion, while, in the treated dogs, segment shortening returned to a maximum of 56 ± 16% of preinfusion at IV2 hours post-reperfusion (P < 0.0003 compared to controls). Similarly, superoxide dismutase + catalase-treated dogs exhibited improved wall thickening during reperfusion (+30% to +70% of preinfusion values), compared to controls (0% to +10%). However, this improvement in contractile function in the treated group was not accompanied by increased adenosine triphosphate stores in the previously ischemic zone (31.8 ± 0.8 vs. 28.2 ± 2.2 nmol/ mg protein for control vs. treated groups). Infusion of superoxide dismutase + catalase did not influence blood flow during occlusion or reperfusion. However, the treated group did exhibit a significant decrease in blood pressure during reperfusion. Hypotension during reperfusion did not appear to be the cause of the improved contractile function, as administration of sodium nitroprusside (an afterload-reducing agent with no free radical scavenging properties) to an additional group of dogs during reperfusion had no significant effect on segment shortening in the previously ischemic tissue. Thus, treatment with free radical scavengers significantly enhanced function, but did not improve high energy phosphate content, in the stunned myocardium. (Circ Res 58:148-156, 1986) BRIEF occlusion of a coronary artery (<20 minutes in duration) followed by reperfusion does not result in myocardial necrosis (Jennings, 1969; Deboer et al, 1980; Kloner et al., 1983); however, the regional contractile function and biochemical properties of the previously ischemic tissue remain depressed for prolonged periods of time following reperfusion (Heyndrickx et al., 1975, 1978; Deboer et al., 1980; Braunwald and Kloner, 1982; Kloner et al., 1983). Whereas the myocardium eventually recovers fully from a brief ischemic episode, the mechanism for this transitory 'stunning* remains unresolved (Braunwald and Kloner, 1982). Recent indirect evidence has suggested that the cytotoxic, oxygen-derived free radicals, Oj (the superoxide ion), 'OH (the hydroxyl radical), and their intermediary, H2O2 (peroxide), are generated at an accelerated rate upon reperfusion (Fig. 1). These radicals are thought to be responsible, at least in part, for ischemia and reperfusion-induced injury in a variety of biological tissues, including the myo- cardium (Parks et al., 1982; McCord, 1984; Jolly et al., 1984; Burton et al., 1984). Specifically, administration of enzymatic free radical scavenging agents significantly reduced the extent of necrosis produced by 60-90 minutes of coronary artery occlusion followed by reperfusion (Chambers et al., 1983; Jolly et al., 1984). Myocytes salvaged by free radical scavengers upon reperfusion had been reversibly injured by the 60-90 minutes of ischemia, and thus may have properties similar to myocytes 'stunned* by brief periods of occlusion followed by reperfusion. That is, the toxic action of free radicals may offer an explanation for the prolonged depression in function and metabolism which follows occlusions of less than 20 minutes. The objective of the current study was to ascertain whether administration of the free radical scavengers superoxide dismutase (SOD: an enzyme catalyzing the conversion of O? to H2O2) and catalase (accelerating the reaction of H2O2 to H2O and O2) could improve contractile function in the post-reperfused, stunned Przyklenk and Kloner/Ettect of Free Radical Scavengers on Stunned Myocardium I ISCHEMIAS Decrease inATP content: degraded into AMP I Adenoane I Inosine Hypoxanth'ne =- Influx of intracelUar Activated protease Xanthine dehydrogenase Xanthine oxidase Xanthine tREFEfffuaONl—-02 Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 2H2O * 0 2 FIGURE 1. Chain of events leading to the production of O2-derived free radicals (02, OH, and H2Ot) upon reperfusion of ischemic myocardium. myocardium following 15 minutes of coronary artery occlusion in the anesthetized, open-chest canine preparation. The effects of SOD + catalase upon regional myocardial blood flow, hemodynamics, and high energy phosphate content were also investigated. As SOD + catalase produced a concomitant reduction in arterial pressure, the question of whether hypotension alone can influence contractile function of the stunned myocardium was further addressed. Methods SOD + Catalase Protocol Twenty-eight mongrel dogs of either sex [27.2 ± 5.3 kg (mean ± SD)] were anesthetized with an intravenous injection of sodium pentobarbital (30 mg/kg), intubated, and ventilated with room air. After cannulas had been inserted into the external jugular vein (for administration of drugs and fluids) and left common carotid artery (for measurement of heart rate and arterial pressures), a left thoracotomy was performed through the 5th intercostal space. The ribs were retracted, the heart was suspended in a pericardial cradle, and the left atrium was cannulated for infusion of either SOD + catalase solution or saline placebo, and injection of radioactive microspheres for measurement of regional myocardial blood flow (RMBF). A Millar pressure transducer was inserted into the left ventricle (LV) through the left atrial appendage for measurement of LV pressure and LV dP/dt. A small segment of the left anterior descending coronary artery (LAD) was isolated, usually distal to the first major diagonal branch. The LAD was then briefly occluded for approximately 5 seconds to delineate the extent of cyanosis. Regional function in the soon-to-be ischemic region was assessed using the transit time technique between ultrasonic crystals implanted in the myocardium, the details of which have been presented previously 149 (Lange et al., 1984). One pair of crystals, used to measure segment shortening (SS), was inserted through small scalpel incisions into the midmyocardium in the center of the area to become ischemic. These crystals were positioned perpendicular to the major axis of the heart, at a separation of 6-12 mm. An additional pair of crystals for measurement of wall thickening (WT) was also placed into the area to become ischemic: one crystal was inserted via a small diagonal incision to the endocardium, while a larger, disc-shaped crystal was sutured to the epicardium at the point at which the ultrasonic transit time between the pair was the shortest. SS, WT, arterial and LV pressures, and LV dP/dt were monitored continuously during the experiment on a Gould recorder. After the initial measurement of SS, WT, heart rate, and arterial pressures under control conditions, dogs recieved either SOD (5 mg/kg per hour) + catalase (5 mg/kg per hour) dissolved in 500 ml of saline, or saline alone (500 ml). Infusion of the saline or SOD + catalase solution was begun 15 minutes before occlusion, and was maintained at a constant rate of approximately 2.4 ml/min for the duration of the experiment. Measurements of hemodynamics, SS, and WT were repeated at 13 minutes postinfusion, before occlusion. After a bolus dose of lidocaine (1.5 mg/kg, iv) had been administered, the LAD was occluded using two Schwartz atraumatic vascular clamps. Hemodynamics and function were monitored at 5, 10, and 14 minutes post-occlusion, and microspheres for measurement of RMBF were injected at 10 minutes post-occlusion. Fifteen minutes after occlusion, the LAD was reperfused by releasing the Schwartz's clamps. Infusion of the control or drug solution was continued for 3 hours following reperfusion, with measurements of function and hemodynamics repeated at 5, 10, 15, 20, 30, 45, 60, 90, 120, 150, and 180 minutes post-reperfusion. A second RMBF measurement was made 2 hours after reperfusion. Immediately prior to sacrifice at 3 hours post-reperfusion, in vivo rransmural needle biopsies were taken from both previously ischemic and normal myocardium, divided into endo- and epicardial segments, and assayed for adenosine triphosphate (ATP) and creatine phosphate (CP) content (Deboer et al., 1980). The LAD then was reoccluded, and monastral blue pigment (1 ml/kg) was injected into the coronary vascularure via the left atrium to delineate the in vivo area at risk (AR). The heart then was arrested with KC1 (20—40 mEq), excised, the positions of the crystals were marked, and the heart fixed by immersion in 10% neutral buffered formalin. After fixation, the hearts were cut into 7-10 transverse slices, parallel to the atrioventricular groove, approximately 5 mm thick. Correct placement of the ultrasonic crystals was confirmed, and the basal surfaces of the heart slices and margins of the area at risk were traced onto acetate sheets. After the right ventricular tissue had been trimmed off, the heart slices were weighed. For measurement of RMBF, tissue samples from both the center of the previously ischemic region and remote normal myocardium were cut and subdivided into epi-, mid-, and endocardial segments. RMBF then was quantified by the method of Domenech et al. (1969). Extent of the area at risk in each tissue slice was assessed by cutting out and weighing the tracings of the LV and AR and correcting for the weight of the tissue slice. AR weights were summed for each heart and expressed as a percent of the LV (AR/ LV). 150 Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Sodium Nitroprusside Protocol An additional group of 15 dogs (23.4 ± 4.4 kg) were anesthetized and instrumented as described previously. After isolation of the LAD, ultrasonic crystals for measurement of segment shortening were placed within the midmyocardium in the center of the area to become ischemic. Wall thickening was not assessed in this group of dogs. After the initial measurement of SS and hemodynamic parameters and administration of a lidocaine bolus, the LAD was occluded for 15 minutes and then reperfused. At 45 minutes post-reperfusion, sodium nitroprusside (0.75-6.5 jigAg per min, iv) was infused at a dose titrated to reduce systolic and diastolic pressures by approximately 20%, comparable to the hypotension observed in dogs given SOD + catalase. The infusion was maintained for 30 minutes and then discontinued for 30 minutes; this cycle was repeated a total of 3 times. Heart rate, arterial pressures, and SS were monitored continuously throughout the experiment, and were quantified pre-occlusion, 10 minutes post-occlusion, 15, 30, and 45 minutes post-reperfusion, and at 10-minute intervals throughout infusion/discontinuation of sodium nitroprusside. Ten minutes after discontinuation of the final nitroprusside challenge, the in vivo area at risk was delineated by injection of monastral blue dye, and the hearts were arrested with KC1, excised, and immersed in formalin. AR/ LV was quantified as described previously; however, RMBF, ATP, and CP content were not measured in this segment of the study. Analysis and Statistics Values of heart rate and systolic and diastolic blood pressures at each sample time were obtained from a mean of five continuous cardiac cycles. Measurements of WT and SS were timed using LV dP/dt. End-diastolic and endsystolic lengths (EDL, ESL) and wall thicknesses (EDWT, ESWT) were defined as the onset of the rapid rise in LV dP/dt and the peak negative dP/dt, respectively (Lange et al., 1984). ESL, EDL, ESWT, and EDWT were measured from three well-separated cardiac cycles for each sample period, and were averaged. Percent SS during the sample periods was then calculated from the formula: Circulation Research/Vo/. 58, No. 1, January 1986 parisons was applied to the P-values. All data are presented as mean ± SEM, and values were considered to differ significantly if P < 0.05. Results SOD + Catalase Protocol Of the 28 dogs entered into the study, two were excluded because of development of persistent arrhythmias upon cannulation of the left atrium and infusion of saline. In addition, six dogs died of ventricular fibrillation, five within the first 10 minutes of LAD occlusion and one immediately upon reperfusion. Thus, 20 dogs—eight treated and 12 controls—remained. Area at Risk Area at risk of infarction was 23.3 ± 1.0% of the LV for the controls, and 23.1 ± 1.6% for the SOD + catalase-treated group (P = NS), indicating that infusion of oxygen-derived free radical scavengers did not significantly influence in vivo area at risk in this model. Blood Flow RMBF in the center of the area at risk was reduced to 0.12 ± 0.03, 0.25 ± 0.08, and 0.59 ± 0.17 ml/min per g of tissue in the subendo-, mid-, and subepicardium of the saline controls, respectively. Flow in the treated dogs did not differ significantly during occlusion from that of controls [0.14 ± 0.06, 0.37 ± 0.14, 0.81 ± 0.31 (Fig. 2)]. No difference in RMBF during occlusion was observed between the treated and control groups in normal myocardium perfused by the circumflex bed. At 2 hours post-reperfusion, infusion of SOD + catalase did not significantly affect flow in either the previously ischemic area or normal myocardium (Fig. 2). These results indicate that treatment with SOD + catalase did not significantly alter RMBF during occlusion or after 2 hours of reperfusion. Segment Shortening and, similarly, % WT was determined using: These values were then presented in two ways: (1) normalized to the pre-occlusion measurements of %SS and %WT (Lange et al., 1984), and (2) normalized to the most negative value of %SS and %WT measured during occlusion (i.e., A %SS). In the SOD + catalase protocol, RMBF, ATP, and CP content, and AR/LV between the treated and control groups, were compared by paired t-test. Hemodynamics and function for the control and treated groups were compared by repeat measures analysis. Contrasts between the two groups then were performed for preinfusion values (for hemodynamic variables only), and at 30, 90, and 180 minutes post-reperfusion (for both hemodynamics and function). Bonferroni's correction for multiple corn- Infusion of either SOD + catalase or saline solution did not significantly influence segment shortening during the initial 15 minutes prior to LAD occlusion. In 17 of the 20 animals in the study, segment shortening was replaced by paradoxical systolic bulging in the ischemic region during occlusion (Fig. 3). The remaining three dogs (all controls) demonstrated a marked reduction in segment shortening during LAD occlusion. Mean %SS for the treated gTOup was -74.5 ± 13.4%, -69.8 ± 14.1%, and -98.5 ± 3.8% of the preinfusion value at 5, 10, and 14 minutes post-occlusion, while the control dogs exhibited a mean %SS of -45.3 ± 15.0%, -45.2 ± 17.5%, and -54.7 ± 15.0% of the preinfusion value at comparable times during occlusion (Fig. 3). These data suggest that the severity of ischemia, assessed by regional function, was as bad 151 Przyklenk and Kloner/Effect of Free Radical Scavengers on Stunned Myocardium 0 Treated D Control Area at Risk 10'Post Occlusion Nonjschemic Tissue 2 hr Post Rtperfusion 10'Post Occlusion 2 hr Post Reperfusion 2.4 2.2 2JO LL m cc 1.8 1.6 1.4 1.2 1.0 0.8 0.6 0.4 0.2 Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 0 ENDO MID EPI 10 Post Occlusion FIGURE 2. Regional myocardial blood flow (RMBF: ml/min per g tissue) in the center of the area at risk, and in remote, nonischemic tissue during LAD occlusion and after 2 hours of reperfusion. i MID ENDO 2 hr Post Reperfusion EPI ENDO 10 Post Occlusion if not worse in the treated group as compared to the controls. During the 3 hours of reperfusion, the 12 control dogs demonstrated a mean %SS ranging within approximately ±10% of the preinfusion value (1.9 ± 16.0%, -3.9 ± 16.1%, and -10.1 ± 14.1% at 30 minutes, Vh hours, and 3 hours, respectively). In spite of the severe systolic bulging demonstrated by the treated dogs during occlusion, %SS in the SOD + catalase-treated group returned to 56 ± 16% of the preinfusion value at Vh hours post-reperfusion, and leveled off to 19.8 ± 14.6% at 3 hours postreperfusion (Fig. 3). At both Vh and 3 hours postreperfusion, %SS for the SOD + catalase-treated dogs was significantly greater (P < 0.0003 and P < 0.047, respectively) than that of controls. ENDO MID 2 hr Post Reperfusion When segment shortening data was normalized to the most negative value during occlusion for each dog (i.e., to compensate for variations in the degree of passive bulging during occlusion among the animals), the saline control group showed a A %SS of +39.7 ± 11.7% at 30 minutes, +46.5 ± 11.1% at Vh hours, and +40.3 ± 9.1% at 3 hours post-reperfusion. Dogs treated with SOD + catalase had a A %SS of +103.2 ± 16.0%, +140.5 ± 21.8%, and +104.2 ± 16.7%, respectively. Differences between the two groups were significant (P < 0.0003) at all three time periods (Fig. 4). +160% + 140% Treoted Control + 120% £ +120% + 100% + 80% g1 + 60% £ + 40% I + 100% *P<0.047 - 2 0 80% c 0% Z <" P<0.0003 T * 1 + 60% 1 1 + "0% -40% -60% - 80% -100% 0% Pre \ I Occlusion) Reperfusion 2hr - Post Reperfusion - 3hr FIGURE 3. Segment shortening, expressed as a percent of preinfusion values, for SOD + catalase-treated vs. control groups. I I I 0c,:dmion4 1 Reperfusion 1 1 1 ,1 hr. 1—i 1 1 1 1 2 hr. -Post R«p«rfirtJon- 1 1 3hr., 3 h FIGURE 4. Improvement in percent segment shortening, normalized to the most negative values during occlusion, for SOD + catalasetreated vs. control groups. Circulation Research/Vol. 58, No. 1, January 1986 152 Treoied Control Wall Thickening Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Fifteen minutes of SOD + catalase or saline infusion did not alter pre-occlusion wall thickening in the soon-to-be ischemic tissue. Upon occlusion, both treated and control dogs demonstrated passive thinning, rather than active thickening, during systole (Fig. 5). As was the case with %SS, animals infused with SOD + catalase demonstrated greater values of %WT during reperfusion (+42.8 ± 10.7%, +71.0 ± 15.3%, and +39.6 ± 14.0% at lh, Vh, and 3 hours) than did the controls (+0.2 ± 12.1%, +6.0 ± 12.8%, and +2.4 ± 13.1%, respectively). Differences between the two groups proved significant at 30 minutes and Vh hours post-reperfusion (P < 0.0027 and P < 0.0003), but not at the end of the reperfusion phase [P < 0.0546 (Fig. 5)]. When the baseline for wall thickening was taken as the most negative value during occlusion, SOD + catalase-treated dogs exhibited a A %WT of +78.2 ± 19.1%, +102.9 ± 20.1%, and +81.5 ± 20.7% at Vi, Vh, and 3 hours post-reperfusion. In contrast, the saline controls improved by only +27.0 ± 5.7%, +33.0 ± 9.1%, and +29.5 ± 11.2% (Fig. 6). Differences in A %WT between the treated and control dogs were significant at 30 minutes, Vh, and 3 hours post-reperfusion (P < 0.0069, P < 0.0003, and P < 0.0408). Hemodynamics Heart rate measured preinfusion did not differ significantly between the two groups of dogs, and was not influenced significantly, during the course of the experiment, by infusion of SOD + catalase (Fig. 7). Both systolic and diastolic blood pressures were slightly lower prior to infusion in the treated group. Systolic and diastolic pressures were reduced significantly during reperfusion in dogs treated with SOD + catalase [P < 0.0004 at 30 minutes, Vh hours, and 3 hours post-reperfusion (Fig. 7). However, there was no change in arterial pressures in Treated Control 1-1— -1— -1---1-—1 Pre • I Occlusion I Reperfusion lhr. 2hr. -Post Reperfusion- 160% 140% *P<0-0OO3 120% *P<0.0406 *P<0.OO69i ioo% 80% 40% 20% 0% L rOcclusion | Reperfusion 2hr. -Post Reperfusion- 3hr., FIGURE 6. Improvement in percent wall thickening, normalized to the most negative value during occlusion. the control group during the course of the experiment. High Energy Phosphates ATP content in normal myocardium averaged 35 nmol/mg protein in both control and treated groups. In the area previously ischemic, ATP concentration remained somewhat depressed, particularly in the endocardium (i.e., approximately 80% of control) after 3 hours of reperfusion. However, there was no difference in ATP content between control dogs and those infused with SOD + catalase (Fig. 8). Mean CP concentration was 52 nmol/mg protein in normal myocardium. Following 3 hours of reperfusion, CP content in the previously ischemic tissue had returned to (or slightly above) normal, and was not influenced by treatment with SOD + catalase (Fig. 9). Sodium Nitroprusside Protocol Of the 15 dogs entered into this part of the study, two were excluded because no area at risk or evidence of post-ischemic stunning could be detected. Data from one other animal could not be validly analyzed due to electrical interference in the segment shortening signal, and an additional six animals succumbed to ventricular fibrillation (five during occlusion and one immediately upon reperfusion). Results for the remaining six dogs are presented below. 3hr. FIGURE 5. Wall thickening, expressed as a percent of preinfusion values. Area at Risk AR/LV averaged 20.1 ± 1.5% in the six dogs treated with sodium nitroprusside, a value which Przyklenk and K/oner/Effect of Free Radical Scavengers on Stunned Myocardium 153 Treated Control Treated I 1 Control Heart Rate (BPM) 170 160 150 140 130 120 Nonischtmic Truu* 70 -I 60 50 40 30 20 Systolic BP (mm Hq) 160 150 140 130 120 110 100 10 0 #P< 00024 0.0004 *P<00OO4 FIGURE 9. CP content (nmol/mg protein) in the center of the area at risk and in distant, nonischemic tissue at 3 hours post-reperfusion. Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 dogs remained similar to those in the SOD + catalase and saline control groups (Fig. 7). Diastolic BP (mm Hg) Segment Shortening Pre I Infusion' Occlusion All six dogs demonstrated paradoxical systolic bulging in the ischemic zone during occlusion. When segment shortening for each dog was normalized to the value measured during occlusion, A %SS averaged +55.5 ± 8.5%, and +58.4 ± 7.3%, and +56.5 Post Repertusion- 170 Reperfusion Heart Rate (BPM) Infusion 160 FIGURE 7. Heart rate, systolic, and diastolic blood pressures for SOD + catalase-treated and control groups. nfusion Off I Infusion I Off I I Off 150 140 130 does not differ significantly from those of the SOD + catalase or saline control groups. Hemodynamics Both systolic and diastolic pressures were reduced by approximately 20% during infusion of nitroprusside (Fig. 10); thus, the magnitude of the induced hypotension was comparable to that observed in dogs treated with SOD + catalase (Fig. 7). At these doses, nitroprusside infusion was not accompanied by reflex tachycardia (Fig. 10)—heart rates in these 120 160 150 140 130 120 110 100 Systolic BP (mm Hg) WV/\ Treated I | Control NomKhwnic Tltiue 130 Diastolic BP (mm Hq) 120 110 50 100 40 90 30 80 20 70 10 0 Pre + | EN DO Occlusion EPI FIGURE 8. ATP concentration (nmol/mg protein) in the center of the area at risk and in distant, nonischemic tissue at 3 hours postreperfusion. I lhr. 2hr. 3hr. -Post Reperfusion- Reperfusion FIGURE 10. Heart rate, systolic and diastolic blood pressures for animals treated with sodium nitroprusside. Circulation Research/Vol. 58, No. 1, January 1986 154 ±9.4% during the three periods of nitroprusside infusion, and +48.1 ± 9.4%, +44.4 ± 10.0%, and +47.2 ± 10.8% while the infusion was discontinued (Fig. 11). Values of A %SS both with and without nitroprusside infusion do not differ from those of the saline control group illustrated in Figure 4, and are clearly less than the maximum A %SS of +140% observed in animals treated with SOD + catalase. Thus, although values of A %SS fluctuated very slightly upon infusion and discontinuation of the afterload-reducing agent, infusion of sodium nitroprusside did not significantly improve the contractile function of the stunned myocardium. Discussion Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Oxygen-derived free radicals (O2, ' OH) and H2O2 are unstable, highly reactive, and cytotoxic variations of the oxygen molecule. These reactive oxygen species have been implicated in ischemia and reperfusion-mediated injury of a variety of tissues, including the brain, intestine, lung, kidney, and heart (Parks et al., 1982; McCord, 1984; Jolly et al., 1984; Burton et al., 1984). Free radicals are produced in vivo by both mitochondria and phagocytes; however, their rate of production is greatly accelerated upon reoxygenation of ischemic tissue (McCord et al., 1984). Free radical scavengers such as superoxide dismutase and catalase are the enzymatic defenses against these cytotoxic agents. SOD acts by catalysing the dismutation of O2 to H2O2 and O2, while catalase accelerates the conversion of H2O2 to H2O and O2 (Fig. 1; Fridovich, 1978; Jolly et al., 1984). However, during reperfusion of ischemic tissue, not only is the rate of free radical production increased, but the damage is exacerbated by the washout of enzymes, including endogenous supplies of SOD in •£ «IOO% 9 i i O 1 L/-| 1- Occlusion Rcpcrfuslon 2hr. -Po»t Repwfutioo- FIGURE 11. Improvement in percent segment shortening, normalized to the value measured during occlusion, for animals treated with sodium nitroprusside. and catalase, from the previously ischemic tissue (McCord, 1984). Thus, reoxygenated tissue becomes even more susceptible to free radical mediated injury. A large body of evidence has been presented to indicate that myocardial necrosis resulting from ischemia followed by reperfusion may be attributed to the formation of oxygen-derived free radicals. Using a canine model of myocardial infarction, Chambers et al. (1983) found that administration of either SOD or allopurinol (a xanthine oxidase inhibitor) during 1 hour of LAD occlusion and 4 hours of reperfusion significantly reduced infarct size, compared to nontreated controls. Similar results were obtained by Jolly et al. (1984): SOD + catalase significantly reduced the extent of necrosis produced by 90 minutes of circumflex occlusion followed by 22V2 hours of reperfusion. Similar results have been obtained with isolated, perfused hearts subjected to global ischemia followed by reperfusion: administration of free radical scavengers SOD, catalase, allopurinol, and/or mannitol improved subcellular and mechanical function, and qualitative morphology of the hearts (Guarnieri et al., 1980; Schlafer et al., 1982a, 1982b; Stewart et al., 1983; Casale et al., 1983; Gauduell and Duvelleroy, 1984). It should be noted that in both the in vivo and in vitro models, the protection afforded by the scavengers was significant only when administered prior to and at the onset of reperfusion, and was not significant when given during reperfusion alone (Casale et al., 1983; Gardner et al., 1983; Guaduell and Duvelleroy, 1984; Jolly et al., 1984). Direct proof of the toxic effects of the O2 and OH radicals on developed tension and myocardial ultrastructure has been demonstrated in isolated, perfused rabbit septa (Burton et al., 1984). These studies indicate that O2 and OH radicals are capable of producing functional and structural alterations in the myocardium, and treatment with free radical scavengers can, at least in part, ameliorate this damage. During coronary artery occlusion, active contraction of the myocardium is almost immediately replaced by passive systolic bulging and wall thinning in the area of ischemia (Heyndrickx et al., 1975; Heyndrickx et al., 1978). For occlusions lasting less than 20 minutes, followed by reperfusion, ischemic damage to the myocytes is reversible and the cells do not become necrotic (Jennings, 1969; Lange et al., 1984). However, the structural, functional, and metabolic properties of the previously ischemic tissue have been shown to remain depressed—or 'stunned*—for prolonged periods of time following reperfusion (Heyndrickx et al., 1975; Weiner et al., 1976; Heyndrickx et al., 1978; Deboer et al., 1980; Braunwald and Kloner, 1982; Lange et al., 1984; Kloner et al., 1984). In the present study, measurements of function, biochemistry and RMBF for the control group during the 3 hours of reperfusion indicate that the previously ischemic myocardium was 'stunned,* and are in good agreement with Przyklenk and Kloner/Effect of Free Radical Scavengers on Stunned Myocardium Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 previous findings: %SS and %WT remained markedly depressed throughout reperfusion (as was observed by Lange et al., 1984), ATP content was approximately 20% below normal at 2 hours postreperfusion, while CP concentration was restored to control values following 2 hours of reflow (as shown by Deboer et al., 1980, Lange et al., 1984b, and Heyndrickx et al., 1978, respectively). The phenomenon of the stunned myocardium has been well-documented; yet, the explanation for its occurrence remains pending. As the recovery of function has been observed to parallel the restoration of the ATP pool, it has been suggested that these two factors may be causally related (Braunwald and Kloner, 1982). Increased concentrations of intracellular calcium have also been implicated as a possible explanation for 'stunning' (Braunwald and Kloner, 1982). Our current results indicate that treatment with SOD + catalase significantly improves function in the previously ischemic myocardium, implying that OJ and ' OH ions contribute to stunning during reperfusion. As illustrated in Figure 1, free radical formation upon reperfusion is closely related to the degradation of ATP and influx of Ca++ during hypoxia. In fact, it has been postulated that oxygen-derived free radicals contribute to ischemiainduced damage of sarcoplasmic reticulum, and thereby directly affect Ca transport (Hess et al., 1981). Thus, it seems possible that all three factors interact and contribute to depressed function during reperfusion. It is interesting to note that improvement in SS and WT in the SOD + catalase-treated group was effected without a significant change in stores of ATP in the previously ischemic region. This dissociation in recovery of function vs. failure of recovery of ATP concentration suggests that the stunned myocardium is not solely a consequence of a reduced supply of high energy phosphates. However, it should be stressed that normal function was not fully restored in the SOD + catalase-treated group (%SS and %WT returned to a maximum of +60% and +70% of control, respectively), implying that other as yet undefined factors also contribute to the phenomenon of stunning. Improved function also was not accompanied by a decrease in ATP concentration in the treated dogs—that is, the enhanced SS and WT did not appear to drain further the high energy phosphate pool. Both SOD and catalase are highly specific in their roles of Oj and 'OH scavengers (McCord et al., 1984); thus, reduction in infarct size and/or improvement in function upon treatment with these agents has been attributed directly to their enzymatic action. However, in the present study, animals infused with SOD + catalase demonstrated significant reductions in arterial blood pressure during reperfusion. No such response was observed in the saline control group. It is possible that the improved function observed during reperfusion in the present study may be due in part to the concomitant reduc- 155 tion in afterload, rather than the elimination of free radicals alone. To address this question, the timing and magnitude of the hemodynamic changes observed with SOD + catalase were mimicked by infusion of sodium nitroprusside, an afterload-reducing agent with no free radical scavenging ability. Hypotension produced by sodium nitroprusside during reperfusion was clearly not accompanied by a similar improvement in contractile function as occurred in the SOD + catalase group. These findings support our conclusion that the salutory effects of SOD + catalase on contractile function of the stunned myocardium are due to their free radical scavenging action, and not a consequence of afterload reduction. Supported in part by N1H SCOR HL-26215, Bethesda, Maryland. Dr. Przyklenk holds a postdoctoral fellowship from the Medical Research Council of Canada. Dr. Kloner is an established investigator of the American Heart Association. Address for reprints: Dr. Karin Przyklenk, Experimental Myocardial Ischemia Lab, Harper Hospital, 3990 John R, Detroit, Michigan 48201. Received April 29, 2985; accepted for publication October 30, 1985. References Braunwald E, Kloner RA (1982) The stunned myocardium: Prolonged ischemic ventricular dysfunction. Circulation 66: 11461149 Burton KP, McCord JM, Ghai G (1984) Myocardial alterations due to free radical generation. Am ] Physiol 246: H776-H783 Casale AS, Bulkley GB, Bulkley BH, Flaherty JT, Gott VL, Gardner TJ (1983) Oxygen free radical scavengers protect the arrested, globally ischemic heart upon reperfusion. Surg Forum 34: 313— 316 Chambers DE, Parks DA, Patterson G, Yoshida S, Burton KP, Parmley LF, McCord JM, Downey JM (1983) Role of oxygenderived free radicals in myocardial ischemia (abstr). Fed Proc 47: 1093 Deboer LMV, Ingwall JS, Kloner RA, Braunwald E (1980) Prolonged derangements of canine myocardial purine metabolism after brief coronary artery occlusion not associated with anatomic evidence of necrosis. Proc Natl Acad Sci USA 77: 54715475 Domenech RJ, Hoffman JE, Noble MM, Saunders KB, Henson RJ, Subyanto S (1969) Total and regional coronary blood flow measured by radioactive microspheres in conscious and anesthetized dogs. Ore Res 25: 581-596 Fridovich I (1978) The biology of oxygen radicals. Science 201: 875-880 Gardner TJ, Stewart JR, Casale AS, Downey JM, Chambers DE (1983) Reduction of myocardial ischemic injury with oxygenderived free radical scavengers. Surgery 94: 423-437 Gauduell Y, Duvelleroy MA (1984) Role of oxygen radicals in cardiac injury due to reoxygenation. J Mol Cell Cardiol 16: 459470 Guamieri C, Flamingi F, Caldarera CM (1980) Role of oxygen in the cellular damage induced by reoxygenation of hypoxic heart. J Mol Cell Cardiol 12: 797-808 Hess ML, Okabe E, Kontos HA (1981) Proton and free oxygen radical interaction with the calcium transport system of cardiac sarcoplasmic reticulum. J Mol Cell Cardiol 13: 767-771 Heyndrickx GR, Millard RW, McRitchie RJ, Maroko PR, Vatner SF (1975) Regional myocardial function and electrophysiolog- 156 ical alterations after brief coronary artery occlusion in conscious dogs. J Clin Invest 56: 978-985 Heyndrickx GR, Baig H, Nellens P, Leusen I, Fishbein MC, Vatner SF (1978) Depression of regional flow and wall thickening after brief coronary occlusions. Am J Physiol 234: H653-H659 Jennings RB (1969) Early phase of myocardial ischemic injury and infarction. Am J Cardiol 24: 753-765 Jolly SR, Kane WJ, Bailie MB, Abrams GD, Lucchesi BR (1984) Canine myocardial reperfusion injury: Its reduction by the combined administration of superoxide dismutase and catalase. Circ Res 54: 277-285 Kloner RA, Ellis SG, Lange R, Braunwald E (1983a) Studies of experimental coronary artery reperfusion: Effect on infarct size, myocardial function, biochemistry, ultrastrucrure and microvascular damage. Circulation 68 (suppl I): 8-15 Kloner RA, Ellis SG, Carlson NV, Braunwald E (1983b) Coronary reperfusion for the treatment of acute myocardial infarction: Post ischemic ventricular dysfunction. Cardiology 70: 233-246 Lange R, Ware J, Kloner RA (1984a) Absence of a cumulative deterioration of regional function during three repeated 5 or 15 minute coronary occlusions. Circulation 69: 400-408 Lange R, lngwall J, Hale SL, Alker KJ, Braunwald E, Kloner RA (1984b) Preservation of high energy phosphates by verapamil in reperfused myocardium. Circulation 70: 734-741 Circulation Research/Vo/. 58, No. 1, January 1986 McCord JM (1984) Are free radicals a major culprit? In Therapeutic Approaches to Myocardial Infarct Size Limitation, edited by DJ Hearse, DM Yellon. New York, Raven Press, pp 209-218 Parks DA, Bulkley GB, Granger DN, Hamilton SR, McCord JM (1982) Ischemic injury in the cat small intestine: Role of superoxide radicals. Gastroenterology 82: 9-15 Schlafer M, Kane PF, Kirsch MM (1982a) Superoxide dismutase plus catalase enhances the efficacy of hypothermic cardioplegia to protect the globally ischemic, reperfused heart. J Thorac Cardiovasc Surg 83: 830-839 Schlafer M, Kane PF, Wiggins VY, Kirsch MM (1982b) Possible role for cytotoxic oxygen metabolites in the pathogenesis of cardiac ischemic injury. Circulation 66 (suppl I): 85-92 Stewart JR, Blackwell WH, Crute SL, Loughlin V, Hess ML, Greenfield LJ (1982) Prevention of myocardial ischemic reperfusion injury with oxygen free radical scavengers. Surg Form 33: 317-320 Weiner JM, Apstein CS, Arthur JH, Pirzada FA, Hood WB (1976) Persistance of myocardial injury following brief periods of coronary occlusion. Cardiovasc Res 10: 678-686 INDEX TERMS: Myocardial ischemia • Oxygen-derived free radical scavengers • Regional myocardial function • Sonomicrometry • Coronary reperfusion • Sodium nitroprusside Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Superoxide dismutase plus catalase improve contractile function in the canine model of the "stunned myocardium". K Przyklenk and R A Kloner Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Circ Res. 1986;58:148-156 doi: 10.1161/01.RES.58.1.148 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1986 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/58/1/148 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/