Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
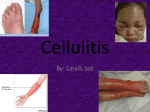
GP Promotional Pack Sunderland Non-complicated Cellulitis Pathway For Patients aged 18 and over (Eron’s Class II) Revised Version following Improvement Event April 2016 1. Project Background Cellulitis is a common painful skin infection, usually bacterial. Patients suffering from cellulitis can be treated with oral antibiotics, although many patients suffering from cellulitis require administration of intravenous (IV) drugs and a hospital admission. The infection most commonly affects the skin of the lower leg but can infect skin in any part of the body, usually following an injury to the skin. Cellulitis can affect people of all ages, including children; rates are thought to be roughly similar in both sexes. Known risk factors for cellulitis include: Having a weakened immune system Lymphoedema Intravenous drug misuse (injecting drugs such as heroin) The development of a primary care cellulitis pathway for Sunderland avoids the need for A&E attendances or hospital admissions for a clearly defined group of patients. As wel l as p at i en ts a tt e nd i ng A & E ha v i n g th e ir f o ll o w u p wit h i n or b y t h e ir l o c a l pr ac t ic e ra th er t h an an em erg enc y c ar e s et t in g. 2. Service Outline This service will target all patients registered with a Sunderland GP who meet the referral criteria for treatment of non complicated cellulitis accordingly to Eron’s Class II in the community. The decision to treat the patient in the community will be made by the referring clinician either GP, GP Out of Hours, GP led WiC or ED. A team of appropriately skilled community based nurses from Community Health Services (Recovery at Home Team) will administer IV medication in patient’s homes to prevent admission to hospital. The service will be available 24 hours a day, 7 days a week. The service aims to: Reduce emergency admissions Reduce the risk of healthcare associated infections Increase the level of care being delivered in the patient’s homes Increase patient independence Increase partnership with patients (through them having involvement in care planning, e.g. timing of administration) Deliver cost savings, by preventing admissions to secondary care 3. Service Description The Recovery at Home Team will provide a community based service to a clearly defined group of patients who are suffering from Eron’s Class II cellulitis, in their own homes. If the patient meets the referral criteria for this service, they are referred to the Recovery at Home Team by the appropriate clinician using the identified referral documentation. Referrals to the Recovery at Home Team should be made by phone to the Recovery at Home Hub, and backed up by the relevant referral documentation, which is to be faxed to the Recovery at Home. The team will accept referrals for adults over the age of 18, the Recovery at Home team will carry out a routine risk assessment and the referring GP should alert the team of any known risk factors upon referral. The Recovery at Home Hub will take all relevant patient information during the initial telephone referral that is required for the Recovery at Home team to visit (Appendix 2). If routine bloods, swabs or investigations are required the Recovery at Home Team will carry out at time of cannulation, which are dependent upon the drug treatment. The GP will flag any anomalies with the blood or swab results for necessary action/treatment to be taken by the Recovery at Home team. During OOH periods (Friday – Sunday) the Recovery at Home team will check patient blood results and liaise with the GP OOH service as necessary to ensure seamless care 24 hours a day, 7 days a week. The GP Receptionist will fax the drug treatment card to the Recovery at Home Team, then give the treatment card to the patient to take home to share with the Recovery at Home Team when they visit. The Receptionist will make the 48hour review appointment, document this on the patient leaflet and give this to the patient (Appendix 4). If this falls on a weekend the appointment will be made with the Recovery at Home GP. Patients should be given their i nformation leaflet and drug treatment card identifying the relevant drug prescribed for the patient; they can then share this with the Recovery at Home Team when they visit. 2 If the referral is received from secondary care the Recovery at Home Team will visit to administer treatment. The ED/UCC or Recovery at Home Team will contact the surgery to arrange the review appointment for 48hours after commencement of treatment. The Recovery at Home Team will contact the patient within four hours of receipt of referral to confirm with the patient a suitable timescale for first contact and treatment to commence. IV drugs will be prescribed by the referring clinician and administered under an agreed drug protocol. IV Drugs will be supplied by the Recovery at Home service. While the patient is undergoing IV therapy they will remain the clinical responsibility of the referring clinician, but the drugs will be administered by the Recovery at Home Team. The drug protocols will clearly specify the responsibilities towards the patient, of each stakeholder in the service. During treatment the patient will be regularly monitored by the Recovery at Home Team. If RAH are unable to recannulate in community setting the member of staff is to refer to Pallion UCC and only if the patient is house bound to refer to NEAS. The team will liaise with the referring clinician, highlighting if the patient is not responding to treatment; or if the patient has responded and needs to be transferred to oral antibiotics. The decision to move from IV to oral antibiotics will be made by the patient’s referring clinician in liaison with the Recovery at Home Team. Please see the detailed pathway described in Figure 1 overleaf. Figure 1 Emergency Care Directorate Diagnose cellulitis Eron’s Class II Consider sepsis sepsis pathway Prescribe drugs on hospital drug chart IV cannula administer first dose Discharge patient to care of RAH Team Discharge include drugs/ drug chart In hours, review appointment at GP Practice to be made by ED Staff; OOH’s, arrange review appointment with RAH Information leaflet including time of RAH visit GP/GP Led UCC/OOHs Diagnose cellulitis Eron’s Class II Consider sepsis admit to ED Identify suitability for community IV ABx (see exclusion criteria) Discuss community pathway with patient Telephone RAH Team with relevant patient information or to discuss pathway Complete Drug Treatment Record Arrange 48 Hr review appointment Give patient information leaflet Exclusions Exclusion criteria; - IVDU - Facial cellulitis - Pregnancy / breastfeeding - Known or suspected MRSA colonization - Under 18 years of age If bilateral symptoms reconsider diagnosis of cellulitis Telephone RAH Team Co-ordinator RAH Team co-ordinator ensures referral meets criteria for acceptance YES NO Receptionist/GP fax Drug Treatment Record to RAH Team Arrange hospital admission using standard admissions proforma 3 RAH Team contact patient within 4 hours of receipt of referral to discuss time of visit. RAH Nurse will obtain IV antibiotics from stock. First Visit by RAH Team Discuss care to gain consent Cannulate Administer drugs Provide patient information leaflet with contact details Schedule next visit Responsiveness to treatment * Referrer will review after 48 hrs or if over a weekend RAH GP will review. RAH Team to discuss progress. Ongoing review * Deterioration * Planned and unplanned according to patient’s needs Discuss with referrer if appropriate or admit directly to hospital. CONSIDER ambulatory care between 7.30am and 10pm weekdays and 7.30am to 8pm weekends If no improvement after 48 hrs CONSIDER discussion with microbiology If no improvement after 72 hrs MUST liaise with microbiologist Patients who RAH unable to cannulate: Housebound patient contact NEAS (ANP). Discharge 4 4. Diagnosis of Cellulitis GP or medical practitioner will carry out clinical assessment; including risk factors and full patient history to establish diagnosis and Erons classification II cellulitis. Eron’s classification system can be found in Appendix 1. 3 Clinical features of cellulitis are : Acute and progressive onset of red, painful, hot, swollen and tender skin with possible blister or bullae formation, usually unilateral Fever, malaise, shivering and rigors may precede or accompany the skin changes Spreading lymphangitis in severe cases Cause usually identifiable (such as laceration, burn, bite, leg ulceration, eczema). Differential diagnosis are identified in table one. Table One Common Varicose eczema DVT Acute gout • • • • • • • • • • Typical Cellulitis Rare Gangrene Carcinoma Erisipeloides Necrotising fasciitis Acute lipopsclerosis Vasculitis Pyoderma gangrenosum Bilateral Varicose Eczema Patient assessment to include the following, erythematous edges should be marked with indelible ink pen to allow subsequent clinical assessment of progress by the Recovery at Home Intermediate Care Team.: Temperature Blood pressure Heart Rate Respiration Rate Oxygen Saturation on air Patient weight if available Investigations to include the following, initial investigations will be carried out by the Recovery at Home Intermediate Care Team at the patient’s first home visit: FBC/U&E/LFT/CRP/Glucose/INR (if applicable) and routine swab if skin is broken or blistering this is dependent upon patient needs and GP clinical judgement Patients suitable and unsuitable for the pathway are identified in table two. 5 Table Two Suitable Adults with uncomplicated cellulitis (Eron’s Class II) Any patient who, on assessment, can be safely treated at home Unsuitable IV drug users Facial/ periorbital cellulitis Pregnancy/breastfeeding Known or suspected colonisation/infection with MRSA Whether to prescribe oral or intravenous antibiotics will be a matter of clinical judgement. IV antibiotics should be considered for patients with: Marked cellulitis (more than mild localised but not extensive) Mild systemic - features (e.g. Flu-like symptoms, malaise) but not unwell Stable co-morbidity such as peripheral vascular disease, chronic venous insufficiency or morbid obesity which may complicate or delay resolution of their infection Cellulitis not improved on oral therapy 5. Treatment Following diagnosis of Class II cellulitis according to Eron’s classification, patients suitable for the pathway should be referred to the Recovery at Home Team for treatment in the community. The three options of recommended IV treatments depending upon patient risk are outlined in Table 3. Table 3 No particular risk of C.difficile infection No allergies or other contraindications Ceftriaxone IV* 1-2g once daily Under 80kg 1g, over 80kg 2g per day Review the morning after the second dose or next working day to decide whether to orally switch or continue Oral switch after 48/72 hours to Flucloxacillin (Complete 7 day course) Allergic to cephalosporins or anaphylactic to penicillins Clindamycin IV* 600mg 6 hourly CDI within past 12 months or living in nursing home or otherwise deemed at high risk by the prescriber Flucloxacillin IV* 1-2g 6 hourly th th Review with the 7 or 8 dose to decide whether to orally switch or continue Oral switch after 48/72 hours to Flucloxacillin (Complete 7 day course ) Not suitable for the pathway th th Review with the 7 or 8 dose or the next working day to decide whether to orally switch or continue. Oral switch to Clindamycin 300mg qds (Complete 5 day course) ** Doses may need to be modified in light of renal function, liver function or extremes of body weight Drug cards can be found as Appendix 3. Intravenous to oral switch; patients should be reviewed at 48 hours or the next working day if at a weekend and if possible switch to oral preparations, suggested criteria are: Pyrexia settling Erythema settling Falling inflammatory markers if available Any co-morbidities stabilized If the patient has not improved at the time of review hospital referral should be considered 6 6. Management of Healthcare Associated Infections The list below outlines advice for GP and Recovery at Home Team to minimise the risk of C.difficile in the community: Nurse and GP to liaise following patients first symptoms of diarrhoea Test for C difficile and treat according to local guidelines if positive Review all antibiotic treatment if applicable Review and stop gastric acid suppressant therapy if applicable Do not prescribe antimotility medication 7. Evaluation of Pathway The following monitoring arrangements will be put in place to ensure the pathway is operating as planned: Cellulitis activity data will be collected and monitored quarterly at the Project Group Meetings to inform the key metrics below: 8. Number of referrals and from Sunderland GP’s to CHS A&E Number of admissions from Sunderland GP’s to CHS Number of referrals to Recovery at Home Team Number of inappropriate referrals to Recovery at Home Team ie. Class I,111 & IV Number of patients switched to oral medication within 72 hours Number of referrals from CHS A&E department to Recovery at Home Team Any evidence of patients on the pathway who have developed C difficile Number and range of antibiotics prescribed Identify the number of practices operating the pathway Contacts If you have any queries or require any information relating to this project please don’t hesitate to contact: Name Designation Contact Details Natalie McClary Sunderland CCG Dr Tracey Lucas Sunderland CCG 0191 5128456 [email protected] 0191 5128456 [email protected] 7 Appendix 1 Eron’s Severity Classification System 4 Eron LJ (2000) devised this classification system of skin and soft tissue infections to aid the GP/Nurse diagnosis, treatment and admission decisions. Once a diagnosis of lower limb cellulitis has been made a decision should be made as to admission/treatment options according to the following classification system. Please see Figure 2: Class I Patients have no signs of systemic toxicity, have no uncontrolled co-morbidities and can usually be managed with oral antimicrobials. Class II Patients are either systemically ill or systemically well but with a co-morbidity such as peripheral vascular disease, chronic venous insufficiency or morbid obesity which may complicate or delay resolution of their infection. Class III Patients may have a significant systemic upset such as acute confusion, tachycardia, tachypnoea and hypotension or may have unstable co-morbidities that may interfere with a response to therapy or have a limb threatening infection due to vascular compromise. Class IV Patients have sepsis syndrome or severe life threatening infection such as necrotizing fasciitis. Clinical findings alone are usually adequate for diagnosing cellulitis, particularly in non-toxic immunocompetent patients. Figure 2 Treatment in the community Eron’s Class I Oral Eron’s Class II Flucloxacillin IV antibiotics Hospital Admissions Eron’s Class III Eron’s Class IV 8 Appendix 2 Telephone Referral Information Patient Demographics Name: Address: Telephone Number: D.O.B. GP Practice Details Name of Referrer: GP Practice: Telephone Number: Reason for Referral Erons classification BP Temp Heart Rate Respiratory Rate Oxygen Sats on air Past Medical History Allergies Routine Investigations required 9 Appendix 3 Drug Therapy Record – Community Nursing Record Patient Name: Date of Birth Address: Patient Telephone Number GP NHS Number: GP Address: GP Telephone Number: Home: Work: Mobile Other cards in use: Allergies All drugs and changes of drug therapy to be recorded before administration by nursing staff Regular Prescriptions Date Drug Name, Strength and Preparation Ceftriaxone injection Dose Route Frequency Additional instructions 1g IV bolus Once daily Ceftriaxone injection 2g IV infusion Once daily Clindamycin injection 600mg IV infusion Every 6 hrs Flucloxacillin injection 1g IV Every 6 hrs Sodium chloride 0.9% 5ml IV Before and after antibiotic Reconstitute the vial with 10ml water for injection according to the IV guide and administer as bolus over 2-4 minutes Reconstitute the vial with 40ml sodium chloride 0.9% and infuse over 30 minutes Prepare the clinidamycin infusion according to the IV guide and administer Infusion over 20-30 minutes foreach 600mg of clindamycin Reconstitute the vial according to the IV guide and administer as bolus over 2-4 minutes Flush the line with 5ml sodium chloride 0.9% before and after administration of antibiotic 10 Prescriber’s Name (PRINT) and Signature Date Discontinued Appendix 4 Cellulitis and Intravenous Antibiotics: Having your Treatment at Home You have been given this leaflet because your doctor/practitioner has seen you and diagnosed cellulitis. The doctor/practitioner has prescribed intravenous antibiotic treatment for you to be given at home. The doctor has referred you to the Recovery at Home Team who will contact you at your home within 4 hours to arrange to visit. Their telephone number is 5616666 fax number 5536928 What is cellulitis? Cellulitis is an infection of the deep layer of skin [dermis] and the layer of fat and tissues just under the skin [the subcutaneous tissues]. It is generally caused by a break in the skin that has allowed bacteria [germs] to get into and under the skin. Various types of bacteria can cause cellulitis. What is the treatment for cellulitis? A course of antibiotic tablets will often clear cellulitis but sometimes, as in this case, more is needed and intravenous antibiotic treatment is needed. This is where the antibiotic is injected into a vein. You will be contacted by the Recovery at Home Team who will visit you at your home. They will bring the intravenous antibiotics with them to administer at each visit. The Recovery at Home Team will visit twice daily to monitor condition and administer your medications. Your doctor will review you after 48 hours of treatment. This has been arranged for you on -------------------------------------- at ---------------------------------You should contact the Recovery at Home Team (or your doctor) sooner however if the area of infection continues to spread or you become worse after you start your antibiotic treatment. The nurse from the Recovery at Home Team will provide you with a full information leaflet so that you can monitor your symptoms and treatment but things you need to know about now are: some patients may develop diarrhoea; this can occur up to 2-3 weeks after finishing treatment, you should tell the Recovery at Home Team nurse or contact your doctor if you develop diarrhoea elevating (raising) the affected body part uses gravity to help prevent excess swelling, which may also ease pain painkillers such as paracetamol or ibuprofen can ease pain and reduce fever and make you feel generally more comfortable using a moisturiser cream and soap substitute on the affected area of skin until it heals to help prevent the skin from becoming dry and damaged drinking plenty of fluids helps prevent dehydration and can make you feel generally more comfortable you may need a tetanus booster vaccination / human tetanus immunoglobulin if you have had dirty cut or wound and your tetanus injections are not up-to-date You should contact your nurse or doctor for advice immediately if you notice any of these symptoms. Pain 'out of proportion' to the look of the skin changes Feeling unwell and becoming ill 'out of proportion' to the look of the skin Symptoms that get worse rapidly - either skin symptoms, or how you feel generally Affected skin that goes dusky, purple or blistering 11