Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
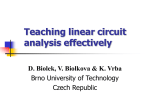
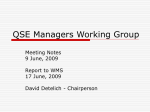
902 Effects of -Adrenergic Receptor Stimulation and Blockade on Rate-Dependent Atrioventricular Nodal Properties Mohsen Nayebpour, Mario Talajic, and Stanley Nattel Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Recent work has shown that alterations in the dynamic atrioventricular (AV) nodal response to changes in heart rate can significantly modify AV nodal function. The present study was designed to evaluate the nature and potential importance of sympathetic regulation of the rate-dependent properties of the AV node. Selective stimulation protocols and mathematical formulations were used to independently quantify AV nodal recovery, facilitation, and fatigue in 12 morphine-chloralose-anesthetized dogs. Vagal effects were prevented by bilateral vagal transection and intravenous atropine, and the sinus node was crushed to allow a broader range of pacing cycle lengths. In seven dogs with sympathetic nerves intact, ,B-adrenergic receptor blockade increased the recovery time constant (i-) for the conduction of premature test beats from 47±2 (mean±SEM) msec (control) to 62±1 msec (p<0.001), whereas to 38-t-1 msec (p<0.001). In addition, 3-blockade increased the maximum isoproterenol decreased amount of rate-dependent AV nodal fatigue from 7±1 msec (at a cycle length of 198±9 msec [control]) to 17±2 msec (p<0.001). In five dogs with decentralized stellate ganglia, ir, was decreased from 71±3 msec (control) to 57±4 msec and 48±2 msec (p<0.001 for each) by left stellate ganglion stimulation at 5 and 10 Hz, respectively. Maximum fatigue was similarly reduced from 16±1 msec (control) to 12±2 msec (p=NS) and 8±1 msec (p<0.01), respectively. Stellate ganglion stimulation, isoproterenol, and 13-blockade did not alter AV nodal facilitation. A mathematical model incorporating quantitative indexes of AV nodal function accurately accounted for tachycardia-dependent increases in the atrial-His activation interval, which were enhanced by S-adrenergic receptor blockade and reduced by isoproterenol. Furthermore, this model showed that 1-adrenergic effects were increased by increasing heart rate, with the majority of the rate-dependent action being due to changes in the time course of AV nodal recovery. We conclude that 1-adrenergic receptor stimulation alters functional properties that govern the AV nodal response to changes in heart rate. These changes in functional properties alter the ability of the AV node to conduct impulses during tachycardia and, as such, could play a major role in the ability of sympathetic stimulation to promote and 13-adrenergic receptor blockade to prevent the occurrence of AV nodal reentrant arrhythmias. (Circulation Research 1992;70:902-911) KEY WoRDs * atrioventricular node * arrhythmias, atrial * electrocardiogram * calcium channels * sympathetic nervous system * isoproterenol trioventricular (AV) nodal function determines the occurrence and consequences of a wide variety of cardiac arrhythmias. The likelihoods of intranodal AV block, AV nodal reentrant tachycardia, and orthodromic tachycardia in association with an accessory pathway, as well as the clinical consequences of atrial fibrillation and flutter, are highly related to AV nodal conduction and refractoriness.12 The ability of A From the Department of Medicine, Montreal Heart Institute; the Departments of Pharmacology and Therapeutics and Medicine, McGill University; and the Department of Medicine, University of Montreal (Canada). Supported by operating grants from the Medical Research Council of Canada, the Quebec Heart Foundation, and the Fonds de Recherche de l'Institut de Cardiologie de Montr6al. M.T. is a Research Scholar of the Canadian Heart Foundation. S.N. is a recipient of the Nordic-Fonds de la Recherche en Sante du Quebec Research Scholarship. Address for reprints: Stanley Nattel, MD, Montreal Heart Institute, 5000 Belanger Street East, Montreal, Quebec H1T 1C8, Canada. Received November 28, 1990; accepted December 10, 1991. the AV node to respond to an atrial input with a propagated response is, in turn, related in a complex fashion to the activation history of the AV node.3-13 A number of discrete properties can be identified that relate activation history to AV nodal conduction. The conduction of extrasystolic impulses through the AV node is slowed increasingly as their prematurity increases.3-10,12-21 This phenomenon, AV nodal recovery, has a time constant in the range of 50-100 msec.8,12,'8-21 On the other hand, an abrupt and sustained increase in atrial activation frequency results in a gradual slowing of AV nodal conduction, called "fatigue," requiring minutes to reach steady state.48,122-25 Single premature AV nodal activations (A2) shift the relation between His bundle-atrial activation time (HA interval) and atrialHis activation time (AH interval) of a subsequent A3 beat to the left on the recovery time axis.4,16,18 This shift decreases the conduction time of premature activations for a given recovery interval and has been called AV nodal "facilitation." The properties of recovery, fatigue, and facilitation can be characterized independently using specific stimulation protocols.13,18,24 Nayebpour et al Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 The degree of sympathetic stimulation is an important regulator of AV nodal function. ,B-Adrenergic stimulation, via direct activation of the sympathetic innervation of the heart26-28 or by the exogenous administration of adrenergic agonists,8'29,30 accelerates AV nodal conduction. Changes in sympathetic input play an important role in baroreflex control of AV conduction.31,32 The autonomic adjustments to upright posture facilitate the induction of sustained AV nodal reentrant tachycardia,33 and in some patients with AV nodal reentrant tachycardia, programmed stimulation fails to induce the tachycardia unless isoproterenol is infused.34-36 ,-Blockade slows AV nodal conduction37 and can prevent the induction3839 and clinical occurrence39-41 of AV nodal reentry. The sympathetic nervous system thus plays an important role in regulating AV nodal function and determining the occurrence and manifestations of supraventricular arrhythmias. The dependence of AV nodal function on heart rate and autonomic tone are well known, but the interactions between the latter two are poorly understood. We have recently shown that changes in the AV nodal response to heart rate change are a potentially important mechanism of vagal action.42 Wallick et a128 showed that heart rate influences the effect of sympathetic nerve stimulation on AV nodal conduction in dogs, and Prystowsky and Page43 have provided evidence for a similar interaction in humans. We have developed mathematical approaches to the quantification of individual AV nodal properties44 and have shown that these approaches can account for both the rate-dependent changes in AV nodal conduction time44 and the rate-dependent effects of the vagus nerve on AV conduction.42 The present study was designed to assess the possibility that sympathetic stimulation alters AV nodal conduction by changing the ways in which the AV node adapts to changes in heart rate. Specific goals were 1) to evaluate whether ,B-adrenergic receptor stimulation or blockade alter AV nodal recovery, facilitation, or fatigue and 2) to determine the extent to which changes in these rate-dependent properties account for alterations in AV nodal conduction as a function of heart rate. Materials and Methods General Methods Mongrel dogs of either sex were anesthetized with morphine (2 mg/kg) and a-chloralose (100 mg/kg i.v.). Catheters were inserted into both femoral veins and arteries and were kept patent with heparinized saline solution (0.9%). Dogs were ventilated via an endotracheal tube using an animal respirator (Harvard Apparatus, South Natick, Mass.). Tidal volume and respiratory rate were adjusted to ensure adequate oxygenation (Sao2290%) and physiological arterial pH (7.35-7.45). A thoracotomy was performed through the fourth right intercostal space, and intrathoracic temperature was maintained at 37-38°C by a homeothermic heating blanket. Bipolar Teflon-coated stainless-steel electrodes were inserted into the lateral right atrium, right atrial appendage, and high lateral right ventricle. A bipolar electrode was inserted epicardially to record a His bundle electrogram.45 J3-Adrenergic Effects on Rate Dependence of AV Node 903 The electrodes in the atrial appendage and right ventricle were used to record atrial and ventricular electrograms. The lateral right atrial electrode was used to apply 4-msec square-wave pulses at twice diastolic threshold, with timing controlled by a programmable stimulator (Digital Cardiovascular Instruments Inc., Berkeley, Calif.). Electrogram signals were filtered (30500 Hz) and amplified (Bloom Instruments Ltd., Flying Hills, Pa.), with the amplified output led into a paper recorder and/or a sensing circuit of the stimulator. A Statham P23 1D transducer (Statham Medical Instruments, Los Angeles, Calif.), electrophysiological amplifiers, and a Mingograf T-16 paper recorder (SiemensElema, Ltd., Toronto) were used to record blood pressure; electrocardiographic leads II and aVR; atrial, His bundle, and ventricular electrograms; and stimulus artifacts. Recordings were obtained at a paper speed of 200 mm/sec (measurement accuracy, ±2.5 msec). The sinus node was crushed19 to allow for a wide range of pacing rates. The vagus nerves were isolated in the neck, ligated, and divided. Atropine was given as an initial intravenous bolus of 1 mg, followed by 0.5 mg every 2 hours to produce sustained muscarinic receptor blockade.46 Measurement of Electrophysiological Variables Wenckebach cycle length was determined by decreasing atrial pacing cycle length by 10 msec every 10 beats until second-degree AV block occurred. The effective refractory period of the AV node and atrial effective refractory period were measured with the extrastimulus technique. The effective refractory period of the AV node was defined as the longest atrial (A1A2) interval failing to result in a His bundle deflection, and the atrial effective refractory period was defined as the longest (S1S2) interval failing to result in a propagated atrial response. AV conduction was assessed from the His bundle electrogram, with the AH interval measured from the peak after the most rapid deflection in the atrial electrogram of the His bundle electrode to the peak after the most rapid deflection of the His bundle electrogram. The HV interval was the time from bundle of His depolarization to the onset of ventricular activation in the His signal. The HA interval was the time from the peak after the most rapid deflection in the His electrogram to the peak in the next atrial electrogram in the His recording. Quantitative Assessment of Functional Rate-Dependent Properties of the AV Node Specific stimulation protocols and analysis techniques were used as previously described4244 to quantify selected functional AV nodal properties before and after interventions altering the level of cardiac 13-adrenergic receptor stimulation. A brief summary of these protocols and techniques is given below. AV nodal recovery. The atrium was paced at a basic cycle length (S1S1) of 500 msec, and a single premature or delayed stimulus (S2) was introduced after every 15 basic stimuli. The relation between the A2H2 (AV nodal conduction time of the test impulse) and the H1A2 interval was established and fitted to a single exponential function. 904 Circulation Research Vol 70, No 5 May 1992 TABLE 1. Effects of Isoproterenol and ,-Adrenergic Receptor Blockade Blood pressure (mm Hg) Diastolic Systolic WBCL (msec) 136±7 89±5 132+6 57±5 167±8.8 Control 142±10 69±5t 122±5 146±10* 47±3t Isoproterenol 161±10* 103±7t 73±6t 242±15t 92±6t ,(-Blockade atrial effective refractory period; AH, AH Values are mean±SEM. WBCL, Wenckebach cycle length; AERP, interval. All measurements other than WBCL were obtained at a basic cycle length of 500 msec. *p<0.01, tp<0.05, and tp<0.001 compared with control. AERP (msec) Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 AV nodal facilitation. The atrium was paced at a constant basic cycle length of 500 msec. A premature atrial impulse (S2) was introduced to produce a selected A1A2 facilitation cycle after every 15 basic stimuli. A test impulse (S3) was then applied after each S2, and the AV nodal response to S3 was monitored to generate an H2A3-A3H3 recovery curve. The latter curve was studied at seven values of (A1A2) facilitation cycle length (FCL) between 500 msec and 20 msec greater than the refractory period of the AV conduction system. Each H2A3-A3H3 recovery curve was fitted by a monoexponential model, and the H2A3 value at which the A3H3 interval is 125 msec (to be referred to as the "HA125') was calculated for each curve. The HA125 is an index of the position of the curve on the horizontal axis. Changes in HA125 reflect the magnitude of parallel leftward shift resulting from facilitation and are an exponential function of FCL.42 AV nodal fatigue. A sensing and pacing circuit was used to sense ventricular activation and to pace the right atrium with a given VA delay. Since the HV interval was constant, this caused a tachycardia with a constant HA interval. Tachycardia was initiated abruptly and maintained for 5 minutes, with the atrial cycle length before tachycardia set at 500 msec by using an activationinhibited demand pacemaker at a rate of 120 beats per minute. After 5 minutes of tachycardia, the sense-pace circuit was closed, and 5 minutes at the baseline cycle length (500 msec) was allowed for recovery before initiating tachycardia with a different HA interval. Fatigue was studied at a total of seven HA intervals in each experiment. Experimental Protocol AV nodal recovery, fatigue, and facilitation were characterized under control conditions as described above. Steady-state values for the AH interval were determined at various cycle lengths, with 5 minutes of pacing at each cycle length used to ensure steady-state conditions. Wenckebach cycle length was measured before and after each experimental protocol to confirm the stability of each preparation. Isoproterenol was then infused via an infusion pump (model 848, EDCO Scientific Inc., Chapel Hill, N.C.). The rate of isoproterenol infusion was selected to produce a 20-30-msec decrease in the Wenckebach cycle length, and the infusion rate was then kept constant in a given dog. Three dogs received an infusion of 2 ,g/min, and four others received an infusion of 5 ,ug/min. Thirty minutes after the onset of isoproterenol infusion, the measurements obtained under control conditions were repeated. Isoproterenol was then discontinued, and 20 minutes were allowed for a return to baseline. When the Wencke- AH (msec) bach cycle length had returned to control values, we administered 0.5 mg/kg nadolol, which we have shown causes sustained fl-blockade for over 2 hours. Twenty minutes later, all measurements were repeated. To compare the effects of endogenous sympathetic nerve stimulation with those of exogenous ,B-adrenergic receptor activation and blockade, an additional series of experiments was performed. The left stellate ganglion was decentralized by cutting its connections with the thoracic sympathetic chain and rami communicantes, and outflow from the right stellate ganglion was prevented by cutting both ansae. An insulated bipolar electrode (Dastre Electrode, Ealing Scientific Ltd., St. Laurent, Canada) was attached (anodal pole proximal) to the dorsal and ventral ansae, and stimulation was applied via an SD 9F stimulator (Grass Instrument Co., Quincy, Mass.). Square-wave stimuli of 2-msec duration, 6-10-V intensity, and 5- or 10-Hz frequency were used. AV nodal functional properties were studied in the absence of sympathetic nerve stimulation, and the measurements were repeated during continuous nerve stimulation, first at 5-Hz and then at 10-Hz frequency. Finally, nadolol (0.5 mg/kg i.v.) was given, and the measurements were repeated. Experimental protocols were approved by the animal care committee of the Montreal Heart Institute. Data Analysis Results are reported as mean±SEM. Comparisons between multiple groups were made by two-way analysis of variance with Scheffe contrasts.47 Comparisons between two groups of experimental data only were made with Student's t test. Two-tailed tests were used, and a value of p=0.05 was taken to indicate statistical significance. Nonlinear curve fitting was performed with Marquardt's technique on an IBM AT-compatible computer. The effects of exogenous ,B-adrenergic receptor stimulation with isoproterenol were evaluated in seven dogs, and the effects of sympathetic nerve stimulation were assessed in five dogs. Results General Effects of /B-Adrenergic Receptor Stimulation and Blockade Isoproterenol accelerated AV nodal conduction and decreased the Wenckebach cycle length (Table 1). ,B-Adrenergic receptor blockade had the opposite effects. The effective refractory period of the AV node was not measurable because it was exceeded by the atrial effective refractory period. Isoproterenol reduced diastolic pressure and tended to increase systolic pres- sure, whereas fl-blockade significantly reduced both Nayebpour et al j3-Adrenergic Effects on Rate Dependence of AV Node CONTROL 180140 100 905 0 A1A2 =500 1 a A1A2 =400 ,, A1A2 =250 A1A2 =180 ~~~~~V _ . em 60. ' .w IL _ 180-- ISOPROTEEO E (I to 1 2 3 CONTROL 1 2 3 1 #-BLOCKED C ISO 2 3 re) 100-- 60 20 a Pl-Blocked 180-- Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 FIGURE 1. Bar graph showing Wenckebach cycle length (WBCL) at the beginning (1), middle (2), and end (3) of electrophysiological study protocols under control, isoproterenol (ISO), and ,B-blocked conditions. C represents the value after discontinuation of isoproterenol and before nadolol administration. Results are mean+±SEM. **p<0.0J and ***p<0.00I compared with WBCL under control conditions. systolic and diastolic pressure. The stability of the preparation is indicated by the consistent values of the Wenckebach cycle length obtained at the beginning, midpoint, and end of each experimental protocol (Figure 1). Changes in AV Nodal Recovery Typical recovery curves under control conditions, in the presence of isoproterenol, and after nadolol are shown in Figure 2. (3-Adrenergic receptor blockade resulted in a slower time course of recovery, whereas isoproterenol slightly accelerated recovery. The mean time constant for all recovery curves averaged 47+2 msec under control conditions, compared with 62+1 msec (p<0.001) after (3-blockade and 38±1 msec (p<0.001) in the presence of isoproterenol. AVNodal Facilitation A premature AV nodal activation resulted in a leftward shift of the AV nodal recovery curve for a 200 1 o~~CONTROL z 160() <m ISOPROTERENOL r=62 01 Pl-BLOCKED E 801 '< 40- H1A2 msec FIGURE 2. Recovery curves from a representative experishowing relation between atrioventricular conduction time (AH interval) and recovery time (IIA interval). The best exponential curve fits are shown by the solid lines. The time constants (rs) for each curve are indicated by arrows. ment 100 20 o - 1 oo 200 300 coo 500 H2A3 (msec) FIGURE 3. Recovery curves for a test atrial beat (A3) preceded by a variety of A1A2 (facilitation) cycle lengths in a representative experiment. As the A1A2 decreased, the atrioventricular nodal recovery curve of the A3 beat shifted progressively to the left. The solid lines are best-fit exponentials to the raw data shown. subsequent beat (Figure 3). The magnitude of the leftward shift for a given coupling interval was similar under all three conditions. To analyze changes in facilitation, each AV recovery curve was fitted to the equation (1) AHHA=AH +A. exp(-HA/Trec) where AHHA is the AH interval at a given HA interval, AHl is the AH interval after full recovery, A is a constant, and rrec is a recovery time constant. The magnitude of the leftward shift of the recovery curve was quantified by calculating the HA125 from Equation 1. The HA125 decreased with decreased FCL under all three conditions (Figure 4). HAl25 was greater in the presence of P3-blockade, indicating that lesser degrees of prematurity were needed to attain an AH of 125 msec than under control conditions. Isoproterenol produced changes in HA125 qualitatively opposite to those resulting from ,3-blockade. However, the differences between HA125 under control compared with isoproterenol conditions were small and not statistically significant. Isoproterenol accelerated basal AV nodal conduction, as shown by AHl, whereas P-blockade had the opposite effect. Decreases in HA125 produced by a premature beat at any FCL relative to the value at the basic cycle length of 500 msec (AHA) are an index of the magnitude of the facilitating effect at that FCL.42,4448 This index of facilitation was not altered by 83-adrenergic stimulation or blockade (Figure 5). Changes in the HA interval can be fitted to an equation of the form AHA=K. exp(-FCL B) (2) where K is a constant equal to the (theoretical) change in the HA interval at an FCL of 0 and B is a rate 906 Circulation Research Vol 70, No 5 May 1992 zuu 0 S 0 . 150¢*-.i .4 4 E in C4 - FIGURE 4. Values of the HA interval corresponding to an AH value of 125 msec (HA125), the AH interval after full recovery (AH.), and the recovery time constant (re,c) as a function of A1A2 (facilitation) cycle length (FCL). Results were obtained by fitting recovery data (of the type shown in Figure 3) at each FCL for an A3 test beat to the equation AHHA =AH. +A * exp(-HA/ r,e), where AHHA is the AH intervalfor a given HA recovery time; AHl, is the AH interval afterfull recovery, and A is a constant. HA,25 was obtained by using the best-fit values of AH,, A, and 7Jec for each curve to solve for the hA corresponding to an AH of 125 msec. *p<0.05, **p<0.01, and ***p<0.001 compared with control at the same FCL. - 100 .. 50- .. i:i * Control 0 l soproterenol I 20 8 I 19 U E U S 80 60 60 o °** 000 a* 20 JII 40-- IDownloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 20 300 200 100 400 soo 600 ^ A1A2 (FCL) msec constant. K and B were unaltered by ,B-adrenergic receptor stimulation and blockade (Table 2), further indicating that they did not alter AV nodal facilitation. AVNodal Fatigue The initiation of a tachycardia with a constant HA interval results in gradual AH prolongation. Figure 6 shows the time course of changes in the AH interval from beat 2 of the tachycardia until a steady state has been achieved in a representative experiment. Since facilitation stabilizes within one cycle6,42 and the recovery variable HA is constant, such changes are due to fatigue alone. Changes in the AH interval were well fitted by an exponential relation of the form AAHn =AAH8s [1 -exp(-n/rfat)] (3) where AAH, is change in the AH interval due to fatigue for the nth beat, is steady-state change in the AH AAHSS .-> 80-- 0 CONTROL E= ISOPROTERENOL SOP-BLOCKED 400 300 250 200 180 160 A1A2 (FCL) mSeC FIGURE 5. Bar graph showing changes in HA125 (the HA value at which the AH interval was 125 msec) from the value at 500 msec (AH4) as a function of A1A2 (facilitation) cycle length (FCL). Values are mean-+SEM for all seven dogs under each condition. Differences in AHIA between conditions were not statistically significant at any FCL. interval due to fatigue, and Tfat is the time constant for fatigue onset. In the experiment illustrated in Figure 6, (3-blockade increased the magnitude of fatigue (AAHSS). This was a general finding in all experiments, as shown by the mean data in Figure 7. mf1t was not affected by 3-adrenergic receptor stimulation and blockade, averaging 65 + 7 beats under control conditions, 84+18 beats in the presence of isoproterenol, and 47±4 beats after ,8-blockade (p=NS). The magnitude of AH change due to fatigue at any steady-state HA interval (AAAH,A) was a function of HA, of the form AAHHA=AAHm.exp(-D * HA)+C (4) where AAHmax, C, and D are constants. The dashed lines in Figure 7 show fits to the mean data using Equation 4 for each condition. Role of Changes in Rate-Dependent Properties The basic AV recovery equation (Equation 1) describes the effect of the coupling interval on AV nodal conduction but does not consider the role of facilitation or fatigue. It fails, therefore, to account for conduction changes when the level of facilitation or fatigue is changing.9"12'48 During sustained rate changes, alterations in both facilitation and fatigue occur. To evaluate the role of modulation of AV nodal properties at different heart rates, it is necessary to analyze the effects of changes in ,B-adrenergic receptor stimulation on all three rate-dependent AV nodal properties. We have shown that the contribution of facilitation and fatigue can be incorporated into Equation 1.48 Facilitation is incorporated by considering HA to be modulated by the preceding cycle length (according to Equation 2), and AH. is adjusted to account for the effect of fatigue (Equation 4). Equation 1 then becomes AHHA=P+A. exp(-Q/rec) (5) Nayebpour et al P-Adrenergic Effects on Rate Dependence of AV Node 907 estimates of the predicted effects of incomplete recovery alone (from Equation 1), of recovery modified by facilitation (Equation 2), of fatigue alone (Equation 4), and of all three processes functioning simultaneously (Equation 5). Values at each cycle length were subtracted from those at a basic cycle length of 500 msec, to estimate rate-dependent slowing at any cycle length due to the influence of each process. The resulting curves are shown in Figure 8. Isoproterenol (middle panel) accelerates recovery, reducing the amount of conduction slowing due to incomplete recovery (dotted line) compared with control (top panel). 8-Adrenergic receptor blockade (bottom panel) slows recovery and increases the effect of fatigue. These changes reduce total rate-dependent conduction slowing (solid line) in the presence of isoproterenol and increase rate-dependent conduction slowing in the presence of /3-blockade. Experimental data (open boxes and error bars) agree well with the theoretical analysis. To further quantify the role of changes in ratedependent properties, we determined the magnitude of AV conduction change attributable to changes in recovery and fatigue resulting from 3-adrenergic receptor activation. AH intervals in the presence of isoproterenol were compared with those in the presence of /3-adrenergic receptor blockade in order to contrast findings associated with a constant, enhanced level of ,3-adrenergic receptor stimulation (isoproterenol) with those associated with the absence of /3-mediated effects. As shown in the top panel of Figure 9, 3-adrenergic receptor stimulation results in a decrease in the AH interval, which becomes more marked as cycle length (or HA interval) decreases. Predicted changes are TABLE 2. Mean Values of Constants Characterizing Atrioventricular Nodal Recovery, Facilitation, and Fatigue in Seven Dogs Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 P3-Blockade Control Isoproterenol 85±7t 45+4* AH' (msec) 54+5 0.6+0.1 1.5±0.3 1.0+0.3 A(sec) 69±4t 43±5 35±2 Trec (msec) 395±128 317±59 425±114 K (msec) B (msec-1) 0.009±0.003 0.009±0.002 0.010±0.002 AAHmax (msec) 12±1 18±4 24±2t -2±1 -1±1 0±1 C (msec) 0.006±0.001 D (msec-') 0.008±0.002 0.014±0.003 Values are mean±SEM. AH', AH interval after full recovery at a cycle length of 500 msec; A, constant; rec, recovery time constant; K, constant equal to the (theoretical) change in the HA interval at a facilitation cycle length of 0; B, rate constant; AAHm., maximum change in the AH interval due to fatigue; C and D, constants. AH', A, and Trree were obtained by fitting recovery data at a cycle length of 500 msec to Equation 1 for each experiment and averaging the values obtained in all seven experiments. K and B were obtained by fitting facilitation data in each experiment to Equation 2. AAHmax, C, and D were obtained by fitting fatigue data from each experiment to Equation 4, as shown for the mean data in Figure 7. *p<0.05, tp<0.001, and tp<0.01 compared with corresponding control value. where P is AH0+AAHHA (AH' is AHr. at a cycle length of 500 msec, and AAHHA is defined as in Equation 4) and Q is HA+ AHA (for AHA as defined in Equation 2). Data in each experiment were used to calculate the constants AH,, A, Trew, K, B, AAHmax, C, and D. The mean constants for all experiments (Table 2) were substituted into the corresponding equations to obtain 41n CONTROL 15- 10.. * d _ *@ *@9* *0 * C.) o ISOPROTERENOL E __e00 10- m 5-. 0 0 o0 _;Q -0 S ~ 0 0 5- 20 0 0 100 200 300 400 BEAT NUMBER 500 600 HA=230 FIGURE 6. Graphs showing changes in the AH interval (AAH) as a function of beat number after the onset of tachy- 20*- U) HA=130 * HA=170 * 5 700 cardia in a representative experiment. Solid lines show best-fit exponential curves. The time HA= 1 20 course of AH prolongation was HA=1 60 under all three condiHA=225 similarbut its magnitude for a tions, given H4 interval was greatest in the presence of 13-blockade, least in the presence of isoproterenol, HA= 1 35 and intermediate under control HA=1 90 conditions. HA=250 .~ _- Circulation Research Vol 70, No 5 May 1992 908 20 1 j,,** **,, n 16 E CONTROL A ISOPROTERENOL ", Af D\ \ `j, 1 2- 11 8. z ",, :^ a[ P-BLOCKED 5* *S** . -1 4. - tm ____ U =S= = == -1 Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 200 300 400 500 VA (msec) FIGURE 7. Graph showing magnitude offatigue (changes in the AH interval at steady state) for tachycardias produced by pacing with the fixed ventriculoatrial (VA) intervals shown. Results (mean ±SEM) were obtained from curve fits to the type of data presented in Figure 6. Dashed curves represent best-fit exponentials to mean data. **p<0.01 and ***p<0.001 compared with control values. 0 100 shown by the solid curve and agree well with experimental data. The mathematical analysis allows us to attribute the observed AH reductions to changes in underlying AV nodal properties. At cycle lengths >500 msec, the AH reduction caused by isoproterenol is attributed to a time-independent (tonic) action. As cycle length is reduced, the acceleration of recovery produced by /3-adrenergic receptor stimulation becomes important and accounts for over half of the consequent acceleration in conduction at cycle lengths between 200 and 300 msec. Whereas a reduction of fatigue may also play a role at very rapid heart rates, it is predominantly the change in AV nodal recovery that accounts for the rate-dependent effects of sympathetic stimulation on AV nodal conduction. 90705030.01 g 9050- T%..A 30- _ I_-1r Ix i pr ISOPROTERENOL 70- E Discussion We have shown that the degree of 3-adrenergic receptor activation can control the processes that govern the AV nodal response to changes in heart rate. Enhanced receptor activation reduces the conduction slowing effect of increases in heart rate, whereas f3-adrenergic receptor blockade enhances the negative dromotropic effect of supraventricular tachycardia. ...RECOVERY -- RECOVERY+FACILITATION --- FATIGUE TOTAL PREDICTED Eo OBSERVED . 10 -10 a) (1) CONTROL Effects of Sympathetic Nerve Stimulation To determine whether graded sympathetic nerve stimulation alters the rate-dependent properties of the AV node, an additional five dogs were studied. The effects of sympathetic nerve stimulation on recovery in a typical experiment are shown in Figure 10. Overall, sympathetic nerve stimulation reduced Tw, from 71+3 msec (control) to 57±4 msec (p<0.001) at a stimulation frequency of 5 Hz and 48±2 msec (p<0.001 versus control) at 10 Hz. In keeping with the decentralization of sympathetic cardiac nervous input, Trec in the presence of ,B-blockade (65±3 msec) was not significantly different from control values. Figure 11 shows results for fatigue-induced conduction slowing in the presence of varying degrees of sympathetic tone. Sympathetic stimulation caused a graded reduction in the magnitude of fatigue, which was statistically significant only for a VA interval of 50 msec during 10-Hz stimulation. In contrast, facilitation was not altered by sympathetic stimulation, with the maximum left shift of the recovery curve averaging 45±9 msec under control conditions, 35±4 msec during 5-Hz sympathetic stimulation, 36+8 msec during 10-Hz stimulation, and 30±3 msec after 83-blockade (no statistically significant differences). .. ~0a a 10 90 .. -ap-BLOCKED 70 5030-10- 100 I 200 I I 3B 0 4(0 BCL (msec) I 500 FIGURE 8. Graphs showing predicted ratedependent changes in theAH interval (AAH) due to incomplete recovery, recovery modified by facilitation, and fatigue as a function of basic cycle length (BCL). Mean characterizing constants determined experimentally (Table 2) were substituted into Equations 1, 2, and 4, respectively (see text), to obtain predictions shown. As BCL decreases, incomplete recovery is expected to increase the AH interval to an extent indicated by the dotted lines. Facilitation attenuates the effects of recovery, and when this action offacilitation is incorporated, the AH slowing is predicted by the dashed lines. Changes due to combined recovery and facilitation were added to those resultingfrom fatigue alone to obtain the total rate-dependent AH prolongation predicted (solid lines). The latter are in close agreement with experimentally observed values (mean ±SEM). Nayebpour et al f-Adrenergic Effects on Rate Dependence of AV Node 909 (CONTROL BCL) 400 300 n U 500 600 . o -2 0 .0 In -4, E _E Ir -61 n0- I..RECOVERY -O- ~FATIGUE --- TONIC -t TOTAL o~~~~~OBSERVED /1 -10 10 10 ._____.w ,.,~ SO z PROPORTION OF TOTAL jB-ADRENERGIC EFFECT 6 iO ,-W0~~ C) ~ ~ Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 -. , .O 200 100 .. 300 ~ RECOVERY --- ~~~~FATIGUE ~~~TONIC 500 400 600 FIGURE 9. Top panel: Graph showing reductions in theAH interval (AH) resulting from 8-adrenergic receptor stimulation at a given hA (recovery) intervaL BCL, basic cycle length. Values in the presence of isoproterenol were compared with values in the absence of i3-adrenergic receptor stimulation (fi-adrenergic receptor blockade). The mathematical modelpresented in the text was used to estimate the reduction in the AH interval due to the acceleration of recovery (dotted line) and attenuation of fatigue (dashed line) caused by P-adrenergic receptor stimulation as a function of steadystate h4 intervaL These were added to the time-independent (tonic, line with dashes and dots) change in the AH interval resulting from isoproterenol in order to predict the total AH interval reductions (solid curve) produced by fB-adrenergic stimulation. The latter are in close agreement with experimental observations. Bottom panel: Graph showingproportion of the overall AH interval reduction caused by f-adrenergic receptor stimulation due to tonic actions and to changes in recovery and fatigue at each M4 intervaL HA INTERVAL (msec) Comparison With Previous Studies of Sympathetic Effects on the AV Node Sympathetic nerve stimulation,26-28 exogenous fl-agonists,8,29,30 and baroreflex-mediated increases in sympathetic tone31,32 all enhance AV nodal conduction by activating 3-adrenergic receptors. Ferrier and Dresel8 showed that basal AV nodal conduction time at rapid heart rates is reduced by epinephrine, suggesting a reduction in AV nodal fatigue. Wallick et aP28 showed that the acceleration of AV conduction caused by sympathetic nerve stimulation is magnified by tachycardia. The AH interval shortening produced by isoproterenol infusion in humans similarly depends on the atrial activation rate.49 Although the processes underlying rate-dependent responses of the AV node have been extensively characterized with selective pacing protocols,5,13,16,18,24,50 their modulation by sympathetic tone has not been analyzed. We found that f3-adrenergic receptor blockade increased the amount of rate-dependent fatigue in dogs with intact sympathetic nerves. In addition, 3-blockade slowed the recovery of AV nodal conduction after preceding activation. 13-Adrenergic receptor stimulation decreased fatigue and accelerated recovery. fB-Adrenergic receptor activation produced qualitatively similar effects whether caused by the intravenous infusion of an exogenous agonist (isoproterenol) or by electrically stimulating the nervous outflow from the left stellate ganglion. The effect of isoproterenol was quantitatively smaller. It is possible that larger doses of isoproterenol might have been more effective, but preliminary studies suggested that the doses used produced near-maximal changes in the AH interval. The lesser effects of isoproterenol were more likely due to the high level of resting sympathetic tone in open-chest dogs with sympathetic nerves intact. 30 E1 CONTROL 2000 o A 150- 7/ 100-- SYMP#1 KM SYMP#2 f -BLOCKED 20-- SYMP#1 0 SYMP/J2 V fl-BLOCKED _ 15 41 E: E 25-E- CONTROL C, 65 LI 10 5-- 50 ..I 0VA=200 H1A2 (msec) FIGURE 10. Typical recovery curves obtained under control conditions, during 5-Hz stimulation of left stellate ganglion ansae (symp #1), during 10-Hz stimulation (symp #2), and in the presence of 13-blockade. The time constant of each curve (in milliseconds) is indicated by an arrow. VA=1 00 VA=50 FIGURE 11. Bar graph showing magnitude of fatigue (mean ±SEM changes in the AH interval [AAH]) resulting from tachycardia with the ventriculoatrial (VA) intervals indicated. Sympathetic stimulation at 5 Hz (symp #1) and 10 Hz (symp #2) tended to reduce fatigue, with statistical significance (**p<0.01 compared with control) occurring with 10-Hz stimulation at the shortest VA interval tested. 910 Circulation Research Vol 70, No 5 May 1992 The effects of ,3-adrenergic receptor blockade support this contention. Nadolol had a large effect on AV nodal conduction in sympathetically intact dogs but a small and statistically nonsignificant effect in dogs with stellate ganglion outflow decentralized. Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Possible Ionic Mechanisms of Adrenergic Effects on AV Nodal Recovery and Fatigue The precise ionic mechanisms of AV nodal recovery and fatigue remain unknown. It is likely that AV nodal recovery is related to the time required for reactivation of L-type calcium channels.424648 ,B-Adrenergic stimulation accelerates the recovery of slow channel action potentials51 and promotes the reactivation of calcium current in single guinea pig ventricular myocytes.52 An acceleration of the recovery of calcium current from inactivation is thus a probable explanation of the more rapid recovery of AV nodal conduction during ,B-adrenergic receptor stimulation. AV nodal fatigue may be related to ion accumulation or depletion, metabolic dysfunction, or electrogenic transport mechanisms. If extracellular potassium accumulation plays a role in AV nodal fatigue, it is possible that the ability of ,B-adrenergic stimulation to stimulate Na+,K+-ATPase activity53,54 accounts for its fatigue-attenuating properties. Potential Limitations of Our Findings We studied several levels of adrenergic tone in our dogs: resting basal tone in an open-chest, anesthetized preparation; a constantly increased level of l3-adrenergic receptor stimulation resulting from either continuous isoproterenol infusion or graded left stellate ganglion stimulation; and the absence of ,B-adrenergic stimulation resulting from 13-blockade with nadolol. We have not examined the complex changes in rate-dependent AV nodal properties that may occur with continuously changing levels of sympathetic activity.55'56 Although such studies would have been interesting, they are beyond the scope of the present article. Direct membrane actions of 1-blockers can be a complicating factor in electrophysiological studies. Nadolol, however, is devoid of any direct membrane actions,57 and all of its effects can be safely attributed to ,B-adrenergic receptor blockade. We used the HA interval as an index of AV nodal recovery time. The relative merits of the HA interval and the AA interval as indexes of the AV nodal recovery period have been disputed, and resolution of this issue is beyond the capability of the methods used in this study. Levy et a16 have shown that the HA interval determines AV nodal conduction independent of basic cycle length, and Billette and M6tayer58 have reported that consideration of the HA interval can explain complex properties of AV nodal functional refractoriness. Potential Significance Autonomic tone is well known to regulate AV nodal conduction. The present investigation, along with our previous study of vagal influences,42 indicates that the autonomic nervous system controls processes, particularly AV nodal recovery and fatigue, that determine the AV nodal response to changes in heart rate. Although there are data in the literature suggesting that the magnitude of sympathetic effects on AV nodal function is heart rate dependent,28 our work is the first to establish the changes in functional properties of the AV node that underly this rate-dependent action. Furthermore, we have been able to. demonstrate quantitatively that an increase in the rate of recovery after activation is the most important contributor to the actions of ,B-adrenergic receptor activation on AV nodal conduction at rapid rates. Changes in AV nodal functional properties are potentially important mechanisms of autonomic nervous system action. It is well known, for example, that 1 :1 AV conduction is maintained during exercise at cycle lengths much shorter than the Wenckebach cycle length measured by rapid atrial pacing. Our results suggest that the acceleration of AV nodal recovery and attenuation of fatigue resulting from increases in sympathetic tone and decreases in vagal tone may contribute to the physiological maintenance of 1:1 conduction during exercise. The acceleration of AV nodal recovery and lessening of fatigue caused by 13-adrenergic receptor stimulation may account for the role of sympathetic activation in the occurrence of AV nodal reentry.33,35,36 On the other hand, enhancement of fatigue and slowing of AV nodal recovery may contribute to the salutary effects of f-adrenergic receptor blockers in supraventricular arrhythmias.38-41 Conclusions We have shown that the degree of 83-adrenergic receptor activation modulates discrete rate-dependent properties of the AV node. These actions decrease AV nodal conduction slowing by tachycardia when sympathetic tone is high and increase the negative dromotropic effects of tachycardia in the presence of ,B-adrenergic receptor blockade. The accommodation properties of the AV node to changes in heart rate are under reciprocal control of both limbs of the autonomic nervous system and constitute a heretofore little-recognized target for autonomic regulation of AV nodal function. Further work needs to be done to clarify the underlying mechanisms of dynamic AV nodal properties and of the autonomic effects on them. Acknowledgments The authors thank Lise de Repentigny for typing the manuscript, Nancy Turmel and Christine Villemaire for technical help, and Squibb Pharmaceuticals (Canada) for supplying the nadolol used to produce ,3-blockade. References 1. Zipes DP: Specific arrhythmias: Diagnosis and treatment, in Braunwald E (ed): Heart Disease, ed 3. Philadelphia, Pa, WB Saunders Co, 1988, pp 658-716 2. Josephson ME, Buxton AE, Marchlinksi FE: The tachyarrhythmias, in Braunwald E, Isselbacker KJ, Petersdorff RG, Wilson JD, Martin JB, Fauci AS (eds): Harrison's Principles of Internal Medicine, ed 11. New York, McGraw-Hill Book Co, 1987, pp 923-937 3. Mobitz W: Uber die unvollstandige storung der erregungsuberleitung zwischen vorhof und kammer des menschlichen herzens. Zeit Gesamte Exp Med 1924;41:180-237 4. Lewis T, Master AM: Observations upon conduction in the mammalian heart: AV conduction. Heart 1925;12:209-269 5. Billette J, Janse MJ, Van Capelle FJL: Cycle length-dependent properties of AV nodal activation in rabbit hearts. Am J Physiol 1976;231:1129-1139 6. Levy MN, Martin PH, Zieske H, Adler D: Role of positive feedback in the atrioventricular nodal Wenckebach phenomenon. Circ Res 1974;34:697-710 7. Van Capelle FJL, du Perron JC, Durrer D: Atrioventricular conduction in isolated rat heart. Am J Physiol 1971;221:284-290 Nayebpour et al f-Adrenergic Effects on Rate Dependence of AV Node Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 8. Ferrier GR, Dresel PE: Relationship of the functional refractory period to conduction in the atrioventricular node. Circ Res 1974; 35:204-214 9. Simson MB, Spear JF, Moore EN: Electrophysiological studies in AV nodal Wenckebach cycles. Am J Cardiol 1978;41:244-258 10. Mazgalev T, Dreifus LS, linuma H, Michelson EL: Effects of the site and timing of atrioventricular nodal input on atrioventricular conduction in the isolated perfused rabbit heart. Circulation 1984; 70:748-759 11. Loeb JM, deTarnowsky JM, Whitson CC, Warner MR: Atrioventricular nodal accommodation: Rate- and time-dependent effects. Am J Physiol 1987;252:H578-H584 12. Shrier A, Dubarsky H, Rosengarten M, Guevara MR, Nattel S, Glass L: Prediction of complex atrioventricular conduction rhythms in humans with use of the atrioventricular nodal recovery curve. Circulation 1987;76:1196-1205 13. Billette J, Gossard JP, Lepanto L, Cartier R: Common functional origin for simple and complex responses of atrioventricular node in dogs. Am J Physiol 1986;251:H920-H925 14. Moe GK, Preston JB, Burlington H: Physiologic evidence for a dual A-V transmission system. Circ Res 1956;4:357-375 15. Denes P, Wu D, Dhingra R, Chuquimia R, Rosen KM: Demonstration of dual A-V nodal pathways in patients with paroxysmal supraventricular tachycardia. Circulation 1973;48:549-555 16. Billette J: Preceding His-atrial interval as a determinant of atrioventricular nodal conduction time in the human and rabbit heart. Am J Cardiol 1976;38:889-896 17. Simson MB, Spear JF, Moore EN: Stability of an experimental atrioventricular reentrant tachycardia in dogs. Am J Physiol 1981; 240:H947-H953 18. Billette J: Short time constant for rate-dependent changes of atrioventricular conduction in dogs. Am J Physiol 1981;241: H26-H33 19. Talajic M, Nattel S: Frequency-dependent effects of calcium antagonists on atrioventricular conduction and refractoriness: Demonstration and characterization in anesthetized dogs. Circulation 1986;74:1156-1167 20. Teague S, Collins S, Wu D, Denes P, Rosen K, Arzbaecher R: A quantitative description of normal AV nodal conduction curve in man. JAppl Physiol 1976;40:74-78 21. Chorro FJ, Ruiz-Granell R, Casadan E, Garcia-Civera R, Such L, Lopez-Merino V: Mathematical descriptions of AV nodal function curves in dogs. PACE 1988;11:679-686 22. Meredith BJ, Mendez C, Mueller WJ, Moe GK: Electrical excitability of atrioventricular nodal cells. Circ Res 1968;23:69-85 23. Narula OS, Runge M: Accommodation of A-V nodal conduction and fatigue phenomenon in the His-Purkinje system, in Wellens HJJ, Lie KI, Janse MJ (eds): The Conduction System of the Heart. Philadelphia, Pa, Lea & Febiger, 1976 24. Billette J, Metayer R, St-Vincent M: Selective functional characteristics of rate-induced fatigue in rabbit atrioventricular node. Circ Res 1988;62:790-799 25. Jenkins JR, Belardinelli L: Atrioventricular nodal accommodation in isolated guinea pig hearts: Physiological significance and role of adenosine. Circ Res 1988;63:97-116 26. Rothberger DJ, Winterberg H: Ueber die Beziehung der Herznerven zur Automatischen Reizerzeugung und zum Ploetzlechen Herztode. Arch Ges Physiol 1911;141:343-377 27. Spear JF, Moore EN: Influence of brief vagal and stellate nerve stimulation on pacemaker activity and conduction within the atrioventricular conduction system of the dog. Circ Res 1973;32:27-41 28. Wallick DW, Martin PJ, Masuda Y, Levy MN: Effects of autonomic activity and changes in heart rate on atrioventricular conduction. Am J Physiol 1982;243:H523-H527 29. Lister JW, Stein E, Kosowsky BD, Lau SH, Damato AN: Atrioventricular conduction in man. Am J Cardiol 1965;16:516-523 30. Wallace AG, Troyer WG, Lesage MA, Zotti EF: Electrophysiologic effects of isoproterenol and ,3-blocking agents in awake dogs. Circ Res 1966;18:140-148 31. O'Toole MF, Wurster RD, Phillips JG, Randall WC: Parallel baroreceptor control of sinoatrial rate and atrioventricular conduction. Am J Physiol 1984;246:H149-H153 32. Warner MR, Loeb JM: Reflex regulation of atrioventricular conduction. Am J Physiol 1987;252:H1077-H1085 33. Mann DE, Reiter MJ: Effects of upright posture on atrioventricular nodal reentry and dual atrioventricular nodal pathways. Am J Cardiol 1988;62:408-412 911 34. Hariman RJ, Gomes JAC, El-Sherif N: Catecholamine-dependent atrioventricular nodal reentrant tachycardia. Circulation 1983;67: 681-686 35. Brownstein SL, Hopson RC, Martins JB, Aschoff AM, Olshansky B, Constantin L, Kienzle MG: Usefulness of isoproterenol in facilitating atrioventricular nodal reentry tachycardia during electrophysiologic testing. Am J Cardiol 1988;61:1037-1041 36. Huycke EC, Lai WT, Nguyen NX, Keung EC, Sung RJ: Role of intravenous isoproterenol in the electrophysiologic induction of atrioventricular node reentrant tachycardia in patients with dual atrioventricular node pathways. Am J Cardiol 1989;64:1131-1137 37. Priola DV: Effects of beta receptor stimulation and blockade on A-V nodal and bundle branch conduction in the canine heart. Am J Cardiol 1973;31:35-40 38. Wu D, Denes P, Dhingra R, Khan A, Rosen KM: The effects of propranolol on induction of A-V nodal reentrant paroxysmal tachycardia. Circulation 1974;50:665-677 39. Bauernfeind RA, Wyndham CR, Dhingra RC, Swiryn SP, Palileo E, Strasberg B, Rosen KM: Serial electrophysiologic testing of multiple drugs in patients with atrioventricular nodal reentrant paroxysmal tachycardia. Circulation 1980;62:1341-1349 40. Sung RJ, Tai DY, Svinarich JT: Beta-adrenoceptor blockade: Electrophysiology and antiarrhythmic mechanisms. Am Heart J 1984;108:1115-1120 41. Seides SF, Josephson ME, Batsford WP, Weisfogel GM, Lau SH, Damato AN: The electrophysiology of propranolol in man. Am Heart J 1974;88:733-741 42. Nayebpour M, Talajic M, Villemaire C, Nattel S: Vagal modulation of the rate-dependent properties of the atrioventricular node. Circ Res 1990;67:1152-1166 43. Prystowsky EN, Page RL: Electrophysiology and autonomic influences of the human atrioventricular node. Prog Clin Biol Res 1988;275:259-277 44. Nayebpour M, Talajic M, Nattel S: Quantitation of dynamic AV nodal properties and application to predict rate-dependent AV conduction. Am J Physiol 1991;261:H292-H300 45. Karpawich PP, Gillette PC, Lewis RM, Zinner A, McNamara DG: Chronic epicardial His bundle recordings in awake nonsedated dogs: A new method. Am Heart J 1983;105:16-21 46. Nayebpour M, Talajic M, Jing W, Nattel S: Autonomic modulation of the frequency-dependent actions of diltiazem on the atrioventricular node in anesthetized dogs. J Pharmacol Exp Ther 1990; 253:353-361 47. Sachs L: Applied Statistics. New York, Springer-Verlag New York, Inc, 1984 48. Talajic M, Papadatos D, Villemaire C, Glass L, Nattel S: A unified model of atrioventricular nodal conduction predicts dynamic changes in Wenckebach periodicity. Circ Res 1991;68:1280-1293 49. Kammerling JM, Miles WM, Prystowsky EN: Effects of graded isoproterenol infusions on human cardiac electrophysiologic properties (abstract). Circulation 1985;72(suppl III):III-252 50. Billette J, St-Vincent M: Functional origin of rate-induced changes in atrioventricular nodal conduction time of premature beats in the rabbit. Can J Physiol 1987;65:2329-2337 51. Tsuji Y, Inoue D, Pappano AJ: ,-Adrenoceptor agonist accelerates recovery from inactivation of calcium-dependent action potentials. J Mol Cell Cardiol 1985;17:517-521 52. Shimoni Y, Spindler AJ, Noble D: The control of calcium current reactivation by catecholamines and acetylcholine in single guineapig ventricular myocytes. Proc R Soc Lond 1987;230:267-278 53. Chae SW, Wang DY, Gong QY, Lee CO: Effect of norepinephrine on Na+-K+ pump and Na+ influx in sheep cardiac Purkinje fibers. Am J Physiol 1990;258:C713-C722 54. Diacono J, Dietrich J, Lajoix H: Opposite effects of adrenaline and ouabain on the resting potential of rat atrial cells. Life Sci 1986;39:2541-2550 55. Warner MR, Loeb JM: Beat-by-beat modulation of AV conduction: I. Heart rate and respiratory influences. Am J Physiol 1986;251:H1126-H1133 56. Warner MR, deTarnowsky JM, Whitson CC, Loeb JM: Beat-bybeat modulation of AV conduction: II. Autonomic neural mechanisms. Am J Physiol 1986;251:H1134-H1142 57. Weiner N: Drugs that inhibit adrenergic nerves and block adrenergic receptors, in Goodman Gilman A, Goodman LS, Rall TW, Murad F (eds): The Pharmacologic Basis of Therapeutics, ed 7. New York, The Macmillan Co, 1985, p 194 58. Billette J, M6tayer R: Origin, domain, and dynamics of rateinduced variations of functional refractory period in rabbit atrioventricular node. Circ Res 1989;65:164-175 Effects of beta-adrenergic receptor stimulation and blockade on rate-dependent atrioventricular nodal properties. M Nayebpour, M Talajic and S Nattel Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Circ Res. 1992;70:902-911 doi: 10.1161/01.RES.70.5.902 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1992 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/70/5/902 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/