Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
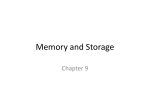
Clinical Chemistry / FIVE CA 19-9 ASSAYS Performance Characteristics of Five Automated CA 19-9 Assays Sonia L. La’ulu,1 and William L. Roberts, MD, PhD2 Key Words: CA 19-9; Automated immunoassay; Method comparison; Imprecision; Linearity DOI: 10.1309/H52VET3M6P7GYWG1 Abstract Serum concentrations of cancer antigen (CA) 19-9 can be useful in monitoring response to therapy in pancreatic cancer. The objective of this study was to evaluate 5 automated CA 19-9 assays: ARCHITECT i2000 (Abbott Diagnostics, Abbott Park, IL), ADVIA Centaur (Bayer Diagnostics, Tarrytown, NY), UniCel DxI 800 (Beckman Coulter, Fullerton, CA), IMMULITE 2000 (Diagnostic Products, Los Angeles, CA), and Elecsys E170 (Roche Diagnostics, Indianapolis, IN). All methods were evaluated for limit of detection, linearity, imprecision, method comparison, and reference intervals. Limit of detection results were all below 2.0 kU/L and met the manufacturers’ claims. Linearity had deviation from target values that ranged from 4.5% to 26.7%. All methods showed acceptable imprecision with total coefficients of variation less than 8%. Method comparison by Passing-Bablok analysis resulted in slopes ranging from 1.00 to 2.06 and correlation coefficients of 0.85 to 0.98. Between 97.6% and 99.2% of results from healthy volunteers were less than 35 kU/L. All methods show acceptable analytic performance. 436 436 Am J Clin Pathol 2007;127:436-440 DOI: 10.1309/H52VET3M6P7GYWG1 Tumor markers are useful in the management of various cancers. Among these, cancer antigen (CA) 19-9 is a marker for pancreatic and colorectal carcinoma.1 However, CA 19-9 has not been shown to be a good screening test for pancreatic cancer in asymptomatic people.2 The primary use of CA 19-9 is in serial monitoring during palliative chemotherapy in conjunction with imaging tests. Serial measurements are also useful for follow-up after potentially curative surgery.3 Measurement of CA 19-9 may also be useful for monitoring other cancers, including gastric, hepatobiliary, hepatocellular, breast, and ovarian cancers.4-6 CA 19-9 is a glycolipid, the sialylated form of the Lewis blood group antigen.4 In serum, it exists as a mucin, a highmolecular-mass (200-1,000 kd) glycoprotein complex.4 CA 19-9 is synthesized by normal human pancreatic and biliary ductular cells and by gastric, colon, endometrial, and salivary epithelia.4 The original monoclonal antibody against CA 199 was developed from a human colon carcinoma cell line, SW-1116.7 Formerly, immunoradiometric assays were used to test for CA 19-9 and have mostly been replaced by automated, nonisotopic immunoassays. Even though imprecision has improved from the use of nonisotopic immunoassays, the agreement of CA 19-9 results has worsened in the last few years when the automated techniques became available.8 The concentration of CA 19-9 in a given specimen, determined with assays from different manufacturers, can vary owing to differences in assay methods, antibodies used, and reagent specificity. Although many quality assessment efforts have been initiated, discrepancies are commonly observed.8,9 We undertook this study to assess the performance characteristics of 5 automated, commercially available CA 19-9 assays. © American Society for Clinical Pathology Clinical Chemistry / ORIGINAL ARTICLE Materials and Methods Limit of detection, linearity, imprecision, method comparison, and reference intervals were determined for the ADVIA Centaur CA 19-9 (Bayer Diagnostics, Tarrytown, NY), ARCHITECT i2000 CA 19-9XR (Abbott Diagnostics, Abbott Park, IL), IMMULITE 2000 GI-MA (Diagnostic Products, Los Angeles, CA), Elecsys E170 CA 19-9 (Roche Diagnostics, Indianapolis, IN), and UniCel DxI 800 GI Monitor (Beckman Coulter, Fullerton, CA). All assays were performed according to manufacturers’ instructions. The limit of detection was determined by averaging 2 separate runs with each run consisting of 10 replicates of zero material and 3 replicates of nonzero material. The following zero and nonzero material was used: on the ADVIA Centaur, CA 19-9 Diluent (0 kU/L) and Calibrator L (21 kU/L); for the ARCHITECT i2000, Calibrator A (0 kU/L) and Calibrator B (30 kU/L); on the IMMULITE 2000, Multi-Diluent 2 (0 kU/L) and Adjustor Low (200 kU/L); for the Elecsys E170, Diluent Universal (0 kU/L) and Calibrator 1 (24 kU/L); and on the UniCel DxI 800, Calibrator S0 (0 kU/L) and Calibrator S2 (90 kU/L). Specimens used for dilution linearity testing were obtained following completion of clinical testing. Each patient specimen was serially diluted with respective manufacturer assay diluent to yield final concentrations of 0.39%, 0.78%, 1.56%, 3.13%, 6.25%, 12.5%, 25%, 50%, 75%, and 100%. All dilutions were tested in duplicate. Imprecision studies were performed by using commercially available quality control material. Two concentration levels (L1 and L2) of lyophilized Lyphocheck Tumor Marker Controls (Bio-Rad, Hercules, CA) were reconstituted according to the manufacturer’s package insert instructions. Multiple bottles for each level were pooled, divided into aliquots, and stored at 4°C until use. Control experiments were run twice a day for 5 days in replicates of 2, using a fresh aliquot for each run. A minimum of 2 hours separated each run for a total of 20 replicates for each control level. Interference studies were performed as previously described.10 Briefly, a serum pool with a nominal CA 19-9 concentration of 100 kU/L was supplemented with the following: (1) RBC hemolysate to a final hemoglobin concentration of 1.1 g/dL (11 g/L), (2) bilirubin to a final concentration of 38.2 mg/dL (653 µmol/L), and (3) Intralipid to a final triglycerides concentration of 2,360 mg/dL (26.7 mmol/L). A deviation of more than 15% from the target CA 19-9 concentration after correcting for dilution was considered a clinically significant degree of interference. Method comparison was evaluated using 135 specimens that were obtained following completion of clinical testing. Specimens chosen contained CA 19-9 concentrations spanning the range of 1 to 1,500 kU/L as measured by the UniCel DxI 800. Before testing, specimens were thawed, mixed thoroughly, and checked for clots. The ADVIA Centaur was used as the comparison method because it was the first US Food and Drug Administration–approved assay. For each method, specimens with measured concentrations more than the analytic measurement range were diluted on-board according to manufacturers’ instructions. The institutional review board of the University of Utah, Salt Lake City, approved all studies using human samples. To evaluate reference intervals, 127 samples obtained from apparently healthy male and female subjects who were not taking any prescription medications were retrieved from –70°C storage. Each sample was thawed, mixed thoroughly, and analyzed by all methods. EP Evaluator Release 5 software (David G. Rhoads Associates, Kennett Square, PA) was used to calculate limit of detection, linearity, imprecision, diagnostic concordance, and reference intervals. Passing-Bablok and linear regression analysis was performed using Analyse-It, version 1.71 (Analyse-It Software, Leeds, England). Results The limit of detection for each assay was calculated and compared with the manufacturers’ claimed values. The ADVIA Centaur had an average limit of detection of 0.43 kU/L with a manufacturer’s claim of 1.2 kU/L; the ARCHITECT i2000 had an average limit of detection of 0.23 kU/L with a manufacturer’s claim of 2.0 kU/L; the IMMULITE 2000 had an average limit of detection of 0.32 kU/L with a manufacturer’s claim of 1.0 kU/L; the Elecsys E170 had an average limit of detection of 0.07 kU/L with a manufacturer’s claim of 0.6 kU/L; and the UniCel DxI 800 had an average limit of detection of 0.07 kU/L with a manufacturer’s claim of 0.8 kU/L. Linearity for all methods was assessed ❚Table 1❚. The target value for each linearity sample was calculated based on the samples with the lowest and highest concentrations within the analytic measurement range for each method. The maximum average deviation from the target recovery ranged from 4.5% (Elecsys E170) to 26.7% (ADVIA Centaur). Imprecision ranged from 2.8% to 8.1% for level 1 and 2.5% to 4.7% for level 2. The Elecsys E170 was the most precise for both control levels and the ARCHITECT i2000 was the least precise for level 1 and the ARCHITECT i2000 and IMMULITE 2000 were the least precise for level 2 ❚Table 2❚. Interference studies were conducted for hemolysis, icterus, and lipemia. The interference detected by the maximum concentration of each substance tested was less than 15% for all methods. Icterus is a relatively common interference in patients with pancreatic cancer owing to metastases to Am J Clin Pathol 2007;127:436-440 © American Society for Clinical Pathology 437 DOI: 10.1309/H52VET3M6P7GYWG1 437 437 La’ulu and Roberts / FIVE CA 19-9 ASSAYS ❚Table 1❚ Summary of Dilution Linearity Data Maximum Deviation for Target Recovery (%) Method* ADVIA Centaur ARCHITECT i2000 IMMULITE 2000 Elecsys E170 UniCel DxI 800 Concentration at Which Maximum Deviation From Target Occurred (kU/L) 26.7 9.8 15.2 4.5 5.0 Measured Range (kU/L) 45.25 707.6 100.7 239.2 371.5 1.4-583.1 4.7-1,045.6 3.7-950.0 5.6-996.1 7.5-1,560.0 * ADVIA Centaur, Bayer Diagnostics, Tarrytown, NY; ARCHITECT i2000, Abbott Diagnostics, Abbott Park, IL; IMMULITE 2000, Diagnostic Products, Los Angeles, CA; Elecsys E170, Roche Diagnostics, Indianapolis, IN; and UniCel DxI 800, Beckman Coulter, Fullerton, CA. ❚Table 2❚ Summary of Imprecision Data Coefficient of Variation (%) Method*/Sample ADVIA Centaur L1 L2 ARCHITECT i2000 L1 L2 IMMULITE 2000 L1 L2 Elecsys E170 L1 L2 UniCel DxI 800 L1 L2 * Mean Concentration (kU/L) Within Run Between Run Between Day Total 16.23 62.50 4.6 2.8 0.0 2.3 4.9 0.0 6.7 3.6 18.38 122.55 8.1 4.1 0.0 2.1 0.0 0.0 8.1 4.7 8.31 34.72 5.6 3.8 0.0 2.8 2.8 0.0 6.3 4.7 11.57 40.04 1.4 1.3 2.2 2.1 0.8 0.0 2.8 2.5 10.65 34.10 5.6 1.3 3.0 2.3 0.7 0.0 6.3 2.6 See Table 1 for manufacturer information. the liver and biliary tract obstruction. It is noteworthy that a total bilirubin concentration of 38.2 mg/dL (653 µmol/L) does not produce a significant interference for any of the methods that were evaluated. Method comparison revealed acceptable agreement when compared with the ADVIA Centaur ❚Figure 1❚. PassingBablok slopes ranged from 1.00 to 2.06 with correlation coefficients ranging from 0.85 to 0.98. Statistical outliers were retested and did not change significantly from the original result. An average of the results from the original and repeated run was used in the final method comparison analysis. Diagnostic concordance was evaluated using the ADVIA Centaur as the comparison method ❚Table 3❚. Results of reference interval studies using samples from healthy volunteers are shown in ❚Table 4❚. Of the 5 methods, 3 use a cutoff of 35 kU/L (ADVIA Centaur, Elecsys E170, and UniCel DxI 800) and 2 use 37 kU/L (ARCHITECT i2000 and IMMULITE 2000). We evaluated reference intervals for 35 and 37 kU/L, and the results were identical. Table 4 shows results evaluated at a cutoff of 35 kU/L because the majority of methods use this cutoff. Reference intervals from healthy volunteers resulted in 97.6% (ADVIA Centaur) to 99.2% 438 438 Am J Clin Pathol 2007;127:436-440 DOI: 10.1309/H52VET3M6P7GYWG1 (IMMULITE 2000, Elecsys E170, and UniCel DxI 800) of specimens tested at less than 35 kU/L. The 97.5% upper reference limit ranged from 17.0 kU/L (IMMULITE 2000) to 37.1 kU/L (ADVIA Centaur). Discussion The limit of detection was lower than the manufacturers’ claimed values for each method and more than adequate for clinical use on serum samples. When evaluating method linearity, if a maximum deviation from the target values of 10% was arbitrarily used as the limit, then the ARCHITECT i2000, Elecsys E170, and UniCel DxI 800 methods would be acceptable. Linearity studies for the ADVIA Centaur and IMMULITE 2000 were also performed using low serum pools as the diluent, and deviations from target values were comparable to those seen using the manufacturers’ diluent (data not shown). Reasons for large deviations from target values, particularly for the ADVIA Centaur method, are unclear. Deviations do not seem to be attributable to a matrix effect from the diluent. © American Society for Clinical Pathology Clinical Chemistry / ORIGINAL ARTICLE 3,000 2,000 1,000 0 0 500 1,000 1,500 1,500 1,000 500 0 0 500 1,000 1,500 1,000 1,500 0 0 500 1,000 1,500 ADVIA Centaur CA 19-9 (kU/L) ADVIA Centaur CA 19-9 (kU/L) ADVIA Centaur CA 19-9 (kU/L) 500 Unicel Dxl 800 CA 19-9 (kU/L) 4,000 D C IMMULITE 2000 CA 19-9 (kU/L) ARCHITECT i 2000 CA 19-9 (kU/L) 5,000 Elecsys E170 CA 19-9 (kU/L) B A 1,500 1,000 500 0 0 500 1,000 1,500 ADVIA Centaur CA 19-9 (kU/L) ❚Figure 1❚ Method comparison of CA 19-9 assays. The ADVIA Centaur was used as the comparison method. The dotted line is the line of identity (x = y). Passing-Bablok analysis is indicated by the solid line. A, Evaluation of the ARCHITECT i2000 method. Passing-Bablok regression analysis gave a slope of 2.06, an intercept of –18.45 kU/L, and r = 0.98. B, Evaluation of the Elecsys E170 method. Passing-Bablok regression analysis gave a slope of 1.18, an intercept of 0.76, and r = 0.85. C, Evaluation of the IMMULITE 2000 method. Passing-Bablok regression analysis gave a slope of 1.00, an intercept of –2.63 kU/L, and r = 0.87. D, Evaluation of the UniCel DxI 800 method. Passing-Bablok regression analysis gave a slope of 1.29, an intercept of 1.41, and r = 0.88. See Table 1 for manufacturer information. Imprecision was acceptable with coefficients of variation of 8% or less for all methods. Our imprecision data agree with what has been described previously for similar methods.11,12 Differences in mean concentrations, especially for level 2, are quite substantial. For the IMMULITE 2000, Elecsys E170, and UniCel DxI 800, level 2 is close to the cutoff; however, this is not the case for the ADVIA Centaur and the ARCHITECT i2000. Even though all methods have similar cutoff values, 35 or 37 kU/L, the level 2 result range is from 34 to 123 kU/L, suggesting a matrix effect with the quality control material. Method comparison achieved acceptable performance, and results are comparable to those of previous studies.11-13 The best correlation was between the ADVIA Centaur and the ARCHITECT i2000. These two assays are more likely to correlate well based on the use of a common antibody. However, the ARCHITECT i2000 slope of 2.06 would suggest differences in calibration. Owing to intermethod differences, confirmation of baseline values is required when changing methods. Diagnostic concordance showed acceptable agreement among the methods, with positive agreement ranging from 91.0% to 97.4% and negative agreement ranging from 68.4% to 93.0%. Again, the ADVIA Centaur and ARCHITECT i2000 methods showed the best overall concordance. This was likely because these 2 methods use a single monoclonal antibody (1116-NS19-9) for the 2-step sandwich immunoassay, whereas the other 3 use one or more different antibodies. ❚Table 3❚ Summary of Diagnostic Concordance* ARCHITECT i2000 Negative (≤37 kU/L) Positive (>37 kU/L) Total IMMULITE 2000 Negative (≤37 kU/L) Positive (>37 kU/L) Total Elecsys E170 Negative (≤35 kU/L) Positive (>35 kU/L) Total UniCel DxI 800 Negative (≤35 kU/L) Positive (>35 kU/L) Total ADVIA Centaur Negative ≤35 kU/L) (≤ ADVIA Centaur Positive (>35 kU/L) Total 53 4 57 4 74 78 57 78 135 47 10 57 7 71 78 54 81 135 41 16 57 4 74 78 45 90 135 39 18 57 2 76 78 41 94 135 Overall Concordance (%) 94.1 (127/135) 87.4 (118/135) 85.2 (115/135) 85.2 (115/135) * See Table 1 for manufacturer information. Am J Clin Pathol 2007;127:436-440 © American Society for Clinical Pathology 439 DOI: 10.1309/H52VET3M6P7GYWG1 439 439 La’ulu and Roberts / FIVE CA 19-9 ASSAYS ❚Table 4❚ Summary of Reference Interval Data Method* Range of Results (kU/L) Median (kU/L) 97.5th Percentile (kU/L) Percentage <35 kU/L 4.3-56.8 2.0-60.3 2.5-38.0 0.6-46.3 1.0-51.0 9.7 4.4 3.3 6.9 7.0 4.7-37.1 2.0-26.4 2.5-17.0 0.6-31.9 1.0-33.2 97.6 98.4 99.2 99.2 99.2 ADVIA Centaur ARCHITECT i2000 IMMULITE 2000 Elecsys E170 UniCel DxI 800 * See Table 1 for manufacturer information. The upper 97.5% reference limit for all methods, except the ADVIA Centaur, was below the manufacturers’ upper limit of expected values for healthy subjects. The ADVIA Centaur had an upper limit of 37 kU/L with a manufacturers’ defined upper limit of 35 kU/L. For the ARCHITECT i2000 and the IMMULITE 2000, the upper limit was well below the manufacturer’s cutoff. The ARCHITECT i2000 had an upper reference limit of 26 kU/L with a manufacturer’s cutoff of 37 kU/L, and the IMMULITE 2000 had an upper reference limit of 17 with a cutoff of 37 kU/L. The Elecsys E170 and UniCel DxI had upper limits that were only slightly lower (32 kU/L and 33 kU/L, respectively) than the manufacturer’s cutoff value of 35 kU/L. All automated CA 19-9 assays showed acceptable analytic performance. CA 19-9 results are method-dependent, and continuing efforts to harmonize assays are needed. The availability of an international reference material could facilitate this effort. As with many tumor markers used in monitoring cancer, instead of focusing merely on the cutoff values, consideration of the critical differences may be more useful.12 A single method should be used because values obtained with different methods cannot be used interchangeably. If the assay method is changed, measurement by both methods to determine a new baseline is required. From the 1ARUP Institute for Clinical and Experimental Pathology and 2Department of Pathology, University of Utah Health Sciences Center, Salt Lake City. Supported by Abbott Diagnostics and the ARUP Institute for Clinical and Experimental Pathology. Address reprint requests to Dr Roberts: c/o ARUP Laboratories, 500 Chipeta Way, Salt Lake City, UT 84108. Acknowledgments: We gratefully acknowledge Abbott Diagnostics, Diagnostic Products, and Roche Diagnostics for providing instrumentation to perform testing using their methods. References 1. Lamerz R. CA 19-9: GICA (gastrointestinal cancer antigen). In: Sell S, ed. Serological Cancer Markers. Totowa, NJ: Humana Press; 1992:309-339. 440 440 Am J Clin Pathol 2007;127:436-440 DOI: 10.1309/H52VET3M6P7GYWG1 2. Kim JE, Lee KT, Lee JK, et al. Clinical usefulness of carbohydrate antigen 19-9 as a screening test for pancreatic cancer in an asymptomatic population. J Gastroenterol Hepatol. 2004;19:182-186. 3. Goggins M, Koopmann J, Yang D, et al. National Academy of Clinical Biochemistry (NACB) Guidelines for the Use of Tumor Markers in Pancreatic Ductal Adenocarcinoma. Available at http://www.nacb.org/lmpg/tumor/chp3i_pancreatic.pdf. Accessed May 2006. 4. Chan DW, Booth RA, Diamandis EP. Tumor markers. In: Burtis CA, Ashwood ER, Bruns DE, eds. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics. 4th ed. St Louis, MO: Elsevier Saunders; 2006:773. 5. Engelen MJ, de Bruijn HW, Hollema H, et al. Serum CA 125, carcinoembryonic antigen, and CA 19-9 as tumor markers in borderline ovarian tumors. Gynecol Oncol. 2000;78:16-20. 6. Takahashi Y, Takeuchi T, Sakamoto J, et al. The usefulness of CEA and/or CA19-9 in monitoring for recurrence in gastric cancer patients: a prospective clinical study. Gastric Cancer. 2003;6:142-145. 7. Koprowski H, Steplewski Z, Mitchell K, et al. Colorectal carcinoma antigens detected by hybridoma antibodies. Somatic Cell Genet. 1979;5:957-971. 8. Pilo A, Zucchelli GC, Cohen R, et al. Comparison of immunoassays for tumor markers CA 19-9, CA 15-3 and CA 125: data from an international quality assessment scheme. Tumori. 1995;81:117-124. 9. Pilo A, Zucchelli GC, Cohen R, et al. Performance of immunoassays for CA 19-9, CA 15-3 and CA 125 tumour markers evaluated from an international quality assessment survey. Eur J Clin Chem Clin Biochem. 1996;34:145-150. 10. Owen WE, Roberts WL. Performance characteristics of the IMMULITE 2000 erythropoietin assay. Clin Chim Acta. 2004;340:213-217. 11. Romer M, Haeckel R, Brux B, et al. A multicentre evaluation of the CA 15-3 assay, CA 19-9 assay and CA 125 II assay on the Bayer Immuno 1 System. Eur J Clin Chem Clin Biochem. 1997;35:637-644. 12. Stern P, Friedecky B, Bartos V, et al. Comparison of different immunoassays for CA 19-9. Clin Chem Lab Med. 2001;39:1278-1282. 13. van Dalen A. BR-MA, OM-MA, GI-MA and CEA: clinical evaluation using the IMMULITE analyzer. Tumour Biol. 1999;20:117-129. © American Society for Clinical Pathology