Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Electrocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
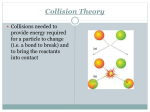
Europace (2012) 14, 99–106 doi:10.1093/europace/eur235 CLINICAL RESEARCH Pacing and Resynchronization Therapy Relationship between endocardial activation sequences defined by high-density mapping to early septal contraction (septal flash) in patients with left bundle branch block undergoing cardiac resynchronization therapy Simon G. Duckett 1,2*, Oscar Camara3,4, Matthew R. Ginks 1,2, Julian Bostock 2, Phani Chinchapatnam 1, Maxime Sermesant1,5, Ali Pashaei 3,4, Pier D. Lambiase 1,2, Jaswinder S. Gill 1,2, Gerry S. Carr-White 2, Alejandro F. Frangi 3,4,6, Reza Razavi 1, Bart H. Bijnens 6, and C. Aldo Rinaldi 1,2 1 Department of Imaging Sciences, The Rayne Institute, Kings College London, UK; 2The Department of Cardiology, Guy’s and St Thomas’ Hospital, London, UK; 3Information & Communication Technologies Department, Centre for Computational Imaging & Simulation Technologies in Biomedicine, Universitat Pompeu Fabra, Barcelona, Spain; 4Networking Research Center on Bioengineering, Biomaterials and Nanomedicine (CIBER-BBN), Barcelona, Spain; 5INRIA, Asclepios Research Project, Sophia Antipolis, France; and 6Institució Catalana de Recerca i Estudis Avançats (ICREA), Barcelona, Spain Received 15 May 2011; accepted after revision 9 June 2011; online publish-ahead-of-print 13 July 2011 Aims Early inward motion and thickening/thinning of the ventricular septum associated with left bundle branch block is known as the septal flash (SF). Correction of SF corresponds to response to cardiac resynchronization therapy (CRT). We hypothesized that SF was associated with a specific left ventricular (LV) activation pattern predicting a favourable response to CRT. We sought to characterize the spatio-temporal relationship between electrical and mechanical events by directly comparing non-contact mapping (NCM), acute haemodynamics, and echocardiography. ..................................................................................................................................................................................... Methods Thirteen patients (63 + 10 years, 10 men) with severe heart failure (ejection fraction 22.8 + 5.8%) awaiting CRT and results underwent echocardiography and NCM pre-implant. Presence and extent of SF defined visually and with M-mode was fused with NCM bull’s eye plots of endocardial activation patterns. LV–dP/dtmax was measured during different pacing modes. Five patients had a large SF, four small SF, and four no SF. Large SF patients had areas of conduction block in non-infarcted regions, whereas those with small or no SF did not. Patients with large SF had greater acute response to LV and biventricular (BIV) pacing vs. those with small/no SF (% increase dP/dt 28 + 14 vs. 11 + 19% for LV pacing and 42 + 28 vs. 22 + 21% for BIV pacing) (P , 0.05). This translated into a more favourable chronic response to CRT. The lines of conduction block disappeared with LV/BIV pacing while remaining with right ventricle pacing. ..................................................................................................................................................................................... Conclusion A strong association exists between electrical activation and mechanical deformation of the septum. Correction of both mechanical synchrony and the functional conduction block by CRT may explain the favourable response in patients with SF. ----------------------------------------------------------------------------------------------------------------------------------------------------------Keywords Cardiac resynchronization therapy † Septal flash † Non-contact mapping † Electro-mechanical † Heart failure * Corresponding author. Simon G. Duckett, Division of Imaging Sciences, The Rayne Institute, 4th Floor, Lambeth Wing, St Thomas’ Hospital London SE1 7EH, UK. Tel: +44 20 7188 7188 8450; fax: +44 207188 5442, Email: [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2011. For permissions please email: [email protected]. 100 Introduction Cardiac resynchronizsation therapy (CRT) is a standard treatment for patients with severe heart failure and conduction delay usually demonstrated by left bundle branch block (LBBB). Although CRT is well established, the non-responder rate is 30%, which poses significant challenges in improving patient selection.1 A favourable response to CRT is known to be associated with a specific ‘U-shape’ activation pattern within the left ventricle (LV), which is not readily apparent from the surface electrocardiogram (ECG).2 – 4 Non-contact mapping (NCM) is able to characterize this endocardial activation pattern5 but is an invasive procedure and not suitable for all CRT candidates. Previous work in our institution demonstrated that NCM can identify regions of slow conduction and LV pacing outside these areas leads to significant haemodynamic improvement.6,7 Certain heart failure patients demonstrate an early septal contraction and inward motion, stretching the lateral wall, followed by a septal lengthening, while the lateral wall starts to contract.8 This fast inward and outward motion of the septum is within the isovolumic contraction time (IVCT) and is referred to as a septal flash (SF). The presence of a SF is visualized on echocardiography in all views showing the septum and can be appreciated using either (slowed down) grey scale or (anatomical) M-mode. Elimination of the SF has been shown to result in a favourable response to CRT.8 Previous studies have reported the SF as a pathophysiological mechanism underlying heart failure in patients with LBBB.9 – 13 Mechanical deformation changes the electrical properties of myocardial tissues14 with stretching of myocytes decreasing their conductivity15 and computer models have shown that electro-mechanical interaction may play a role in LBBB.16 We hypothesized that SF is associated with a particular (U shaped) LV activation pattern that may predict a favourable response to CRT. We sought to characterize the spatio-temporal relationship between electrical and mechanical events that may explain why patients with SF on echocardiography respond to CRT by directly comparing NCM, acute haemodynamics, and echocardiographic imaging. Methods Study population All patients had severe heart failure fulfilling standard criteria for CRT [New York Heart Association (NYHA) class III– IV, QRS .120 ms, left ventricular ejection fraction (LVEF) ≤35%, and LV end-diastolic diameter ≥55 mm]. The study complied with Declaration of Helsinki and the local ethics committee approved the research. All patients gave written informed consent to undergo the non-routine invasive procedures prior to their CRT implant. Echocardiographic acquisition Standard echocardiograms with tissue Doppler imaging (TDI) were acquired on a GE Vivid 7 scanner (General Electric-Vingmed, Milwaukee, WI, USA). Analysis was performed using EchoPac version 6.0.1 (General Electric-Vingmed). Ejection fraction and LV dimensions were measured using 2D modified biplane Simpson’s method. Transmitral flow velocities were obtained from the apical-4CH view with S.G. Duckett et al. pulsed-wave Doppler positioned at the tip of the leaflets. End diastole (onset of isovolumic contraction) and end systole (aortic valve closure) were determined using transmitral and aortic Doppler profiles. Assessment of dyssynchrony and septal flash The inter-ventricular delay was calculated as the difference between the LV and right ventricle (RV) pre-ejection periods.17 Intraventricular dyssynchrony was measured with TDI.18,19 To determine the presence and extent of the SF, two independent clinical experts, blinded to the electrophysiology studies reviewed all echocardiographic images. Existence of an SF was defined as the presence of early inward and outward motion within the isovolumic contraction period seen both visually from the grey scale SAX and 4CH views as well as on M-mode in the PSLAX, SAX, and 4CH. Bull’s eye plots of the LV indicated the presence and spatial extent (segments involved) of the SF. Patients were categorized according to the SF appearance and extent: a large SF if there was marked fast early septal inward/ outward motion with a prominent displacement involving ≥50% of the septal segments in an American Heart Association model; a small SF if there was early inward/outward motion, but with a very limited displacement; or no SF. Cardiac magnetic resonance imaging Cardiac magnetic resonance was performed on a Philips Achieva 1.5T scanner (Philips, Healthcare, Best, The Netherlands) for delayed enhancement (DE-MR) imaging to assess myocardial scar. Delayed enhancement -MR was performed 15 – 20 min following the administration of 0.1– 0.2 mmol/kg gadopentetate dimeglumine (Magnevistw, Bayer Healthcare, Dublin, Ireland) using conventional inversion recovery techniques.20 Non-contact mapping and acute haemodynamic study Non-contact mapping was performed 11 + 8.6 days prior to CRT implant. Bilateral femoral venous access was used to place 5F Supreme JSN 401443 quadripolar electrode catheters (St Jude Medical, Minnetonka, MN, USA) to the high right atrium and RV apex to perform atrial and RV sensing and pacing, a 5F Supreme CRD-2 401860 quadripolar electrode catheter (St Jude Medical) was positioned at the His bundle. The coronary sinus was intubated using a pre-shaped 8F Fast-Cath SL3 406842 guiding sheath (St Jude Medical) and a multipolar Pathfinder 16 electrode catheter 01-16-1003 (Cardima Inc., Fremont, CA, USA) was passed to a postero-lateral or lateral branch of the coronary sinus to perform epicardial LV pacing to replicate standard CRT. A NCM Ensite Array EC1000 (St Jude Medical, St Paul, MN, USA) was passed via the femoral artery retrogradely across the aortic valve to the LV cavity. Via the other femoral artery, a decapolar steerable 6F Livewire 401915 electrode catheter (St Jude Medical) was passed to the LV cavity along with a high fidelity pressure wire (Radi Medical Systems, Uppsala, Sweden) with a 5Fr multipurpose catheter. Chamber geometry was reconstructed using a locator signal from the decapolar catheter.21 The following pacing protocol was performed: (100 bpm with consistent capture, AV delay 100 ms, VV simultaneous): atrium sensed and paced (AAI), DDDRV, DDDLV, and DDDBIV (conventional CRT) AAI pacing at 100 bpm was used as baseline to assess LV dP/dtmax measurements and performed prior to each change in pacing mode.22 Ensite data, pacing parameters and percentage rise in LV dP/dtmax for each pacing mode were recorded once steady-state pacing had been achieved for at least 1 min. Capture without fusion was confirmed 101 Electromechanical interaction in LBBB using VVI pacing and examining the paced QRS morphology. Endocardial maps were obtained in sinus rhythm and in each pacing configuration. Electrograms were acquired at 1200 Hz, giving a temporal resolution of 0.83 ms. High-pass filter was set at 8 Hz. Virtual unipolar electrograms recorded from the endocardial surface were analysed to measure the duration of LV activation. Peak negative dv/dt is a universally accepted indicator of the onset of activation in a region of myocardium. Thus, the onset of activation was taken as the time to the first peak negative 8 Hz high-passed unipolar virtual electrogram anywhere in the chamber. The end of LV activation was defined as the time of the latest peak negative 8 Hz unipolar electrogram on the virtual endocardial surface.23 Lines of block were interpreted from patterns of activation observed in isopotential maps and the associated morphological features of electrograms. Bull’s eye activation maps were generated from the NCM data sets by computing the long axis from the manual identification of the ventricular apex and the centre of the mitral valve in at least two views. We estimated the short axis by identifying the ventricular septum, and lateral wall and drawing a perpendicular line through the long axis. We constructed temporal bull’s eye plots representing the percentage of activated tissue (black in the figures) through time. In parallel, we generated bull’s eye plots of the presence and location of mechanical septal motion visually identified with echocardiography as well as the position and extent of scar determined by DE-MR imaging. These visualization tools allowed a multimodal analysis and integration to directly compare different factors involved in the studied pathophysiology, mainly mechanical septal motion, presence and location of scar, and presence and location of lines of conduction blocks. Lines of conduction block where propagation of the activation wavefront is halted is visualized as a stagnation of the black– white transition during several frames in the series of bull’s eyes plots (Figure 1). Acute haemodynamic responders were considered as an increase in LV dP/dtmax of ≥10% from baseline AAI pacing.24 Following the invasive protocol patients subsequently underwent standard CRT implantation. Patients were followed up after 6 months with a repeat echocardiogram and deemed to have remodelled if there was a ≥15% reduction in LV end-systolic volume (ESV). Statistical analysis Statistical analysis was performed using the SPSS software package (IBM, Chicago, IL, USA). Continuous variables were expressed as mean values + standard deviation (SD), where appropriate continuous variables were assessed with a Student’s t-test and one-way analysis of variance. P values of ,0.05 were considered statistically significant. Results Thirteen patients were studied (aged 63 + 10 years, 10 males, NYHA class 3 + 0). All had LBBB (QRS duration 158 + 24 ms). Eight patients had non-ischaemic dilated cardiomyopathy (DCM), and five ischaemic dilated cardiomyopathy (ICM). Mean LV EF 22.8 + 5.8%, inter-ventricular delay 47.8 + 23.6 ms, septal-lateral delay from TDI 79.2 + 40.3 ms, and SD of 12 segments TDI 50.2 + 13.5 ms (Table 1). Five patients had a large SF, four small SF, and four no SF (Table 1). Notably, patients with a large SF had a significantly broader QRS (172.4 + 25.0 ms vs. small 155.5 + 18.0 or no SF 142.8 + 21.0, P , 0.05) and also significantly more inter-venricular mechanical delay but less intraventricular delay. Figure 1 Patient with a large septal flash. (A) Fused activation and echo bull’s eye plots. The black area indicates activation pattern, red segments area with septal flash. There is initial depolarization of the ventricular septum, followed by slowed conduction (20 – 40 ms) both anteriorly and inferiorly. Areas of block indicated with white arrows. There is breakout of activation inferiorly although slowed depicted by the dashed arrows. Block remains anteriorly. Activation continues inferiorly until the anterior wall is retrogradely activated. (B) Unipolar isochronal map. Top row anterior: Bottom row posterior. There is a line of anterior block with activation spreading inferiorly. (C) Left ventricular noncontact mapping unipolar activation map. The activation breaks out in the ventricular septum, instead of spreading uniformly there is an anterior line of block show by white arrows. The activation spreads inferiorly, leading to a U-shaped activation pattern. Ant, anterior; Sep, septum; Inf, inferior; Lat, lateral. 102 S.G. Duckett et al. Table 1 Comparison of patients with varying size of septal flash All patients Large SF Small SF Absent SF ............................................................................................................................................................................... Number 13 5 4 4 Age Sex 63.1 + 10.2 10 M:3 F 66 + 7.1 4 M:1F 57 + 13.0 4M 66.5 + 11.8 2 M:2F Aetiology of HF 8 DCM 5 ICM 4 DCM 1 ICM 1 DCM 3 ICM 3 DCM 1 ICM QRS duration (ms) 158 + 24 172.4 + 25.0* 155.5 + 18.0 142.8 + 21.0 Ejection fraction (%) EDV (mL) 22.8 + 5.8 255 + 67 22.4 + 6.5 269.8 + 65.8 22.5 + 4.4 248.0 + 88.9 23.5 + 7.5 245.3 + 61.6 ESV (mL) 198.2 + 59.1 211.2 + 64.7 195.5 + 83.4 184.5 + 29.8 IVMD (ms) Septal/lateral delay TDI (ms) 47.8 + 23.6 79.2 + 40.3 69 + 13.9* 56 + 53.2 40.5 + 17.2 82.5 + 22.2 21.8 + 29.1 105 + 20.8 TDI 12 segment SD (ms) 50.2 + 13.5 50.9 + 16.0 47.4 + 14.0 52.2 + 13.0 TIVT (ms) IVCT (ms) 186 + 128 68 + 63 304 + 72* 133 + 29 222 + 57 59 + 55 125 + 72 38 + 49 IVRT (ms) 118 + 88 171 + 68* 163 + 81 89 + 41 *Significant difference between patients with a large septal flash and small/absent septal flash (P , 0.05). EDV, end-diastolic volume; ESV, end-systolic volume; IVCT, isovolumic contract time; IVMD. interventricular mechanical delay; IVRT, isovolumic relaxation time; TIVT,total isovolumic time. Table 2 Acute haemodynamic response with different pacing modes AAI baseline dP/dtmax DDDLV pacing dP/dtmax % increase DDDBIV pacing dP/dtmax % increase 782 + 214 828 + 240 915 + 219* 1038 + 229* 20 + 18 28 + 14 998 + 254* 1141 + 256* 31 + 24 42 + 28 ............................................................................................................................................................................... All patients Large SF Small SF 713 + 216 876 + 182* 25 + 14 835 + 141 21 + 22 No SF Combined small and no SF 880 + 112 797 + 179 856 + 179 866 + 161 –4 + 9 11 + 19 1063 + 152 949 + 181* 22 + 24 22 + 21 *Significant difference from AAI pacing (P , 0.05). Acute haemodynamic response to cardiac resynchronization therapy Overall, there was a significant increase in acute response to CRT (baseline AAI pacing LV dP/dtmax 782 + 214 mmHg/s, DDDLV pacing 916 + 219 mmHg/s (P , 0.05), and DDDBIV pacing 998 + 254 mmHg/s (P , 0.05)). Patients with a large SF had a larger haemodynamic response than those with a small or no SF (Table 2). All patients with a large SF were acute haemodynamic responders for DDDLV and Biventricular (BIV) pacing. One patient with a small SF did not respond to DDDLV pacing and two did not respond to DDDBIV pacing. No patients without a SF responded to DDDLV pacing and one did not respond to BIV pacing. Clinical response and remodelling At 6 months one patient with no SF had died. All except for one patient (small SF) improved by at least one NYHA class [responder rate 92%, (P , 0.05)]. The SF was no longer present after CRT. With respect to remodelling the overall responder rate was 64% [average decrease in ESV 19.8 + 21.4%, (P , 0.05)]. All patients with a large SF remodelled (decrease in ESV 37.1 + 21.2%), two patients remodelled with a small SF (decrease in ESV 11.5 + 7.4%), and none with no SF (decrease in ESV 1.9 + 13.7%) (Table 3). Comparing patients with a large SF to small or no SF there was a greater improvement in ejection fraction (P , 0.05) and larger decrease in ESV (P , 0.05), and NYHA score (P , 0.05). For isovolumic times (IVTs) patients with a large SF had a greater decrease in both IVT (P , 0.05) and IVCT (P , 0.05), there was no difference in isovolumic relaxation time (P ¼ 0.2). Activation maps Figures 1 and 2 shows examples of the NCM and echo bull’s eye plots from a patient with and without a SF. While the activation spreads homogenously over the endocardial surface when no SF is present, there were definite areas of conduction block in the cases with a large SF (Figure 1). In the large SF patients a specific 103 Electromechanical interaction in LBBB Table 3 New York Heart Association class and echocardiographic parameters pre- and post-cardiac resynchronization therapy All patients Large SF Small SF Absent SF N 5 13 N55 N54 N 5 3a ................................... .................................. .................................. .................................. ............................................................................................................................................................................... Pre-CRT Post-CRT Pre-CRT Post-CRT Pre-CRT Post-CRT Pre-CRT Post-CRT 3+0 1.6 + 0.8b 3+0 1.0 + 0.7 3+0 2.3 + 0.5 3+0 1.7 + 0.6 Ejection fraction (%) EDV (mL) 22.7 + 5.8 255.5 + 67.1 31.6 + 10.5b 227.5 + 71.3b 22.4 + 6.5 269.8 + 65.8 37.2 + 13.1 211.4 + 83 22.5 + 4.4 248.0 + 88.9 30.8 + 4.6 245.3 + 83.1 23.5 + 7.5 245.3 + 61.6 23.3 + 6.7 230.7 + 16.0 ESV (mL) 198.2 + 59.1 157.9 + 55.6b 211.2 + 64.7 137.0 + 61.1 195.5 + 83.4 171.3 + 69.0 184.5 + 29.8 175.0 + 6.6 TIVT(ms) IVCT(ms) 186 + 128 68 + 63 147 + 107 48 + 47 304 + 72 171 + 68 173 + 61 33 + 19 222 + 57 59 + 55 144 + 98 53 + 37 127 + 72 38 + 49 139 + 120 64 + 62 IVRT(ms) 118 + 88 99 + 74 133 + 29 140 + 65 163 + 81 91 + 63 89 + 41 74 + 69 NYHA class a One patient died. Significant difference from pre-cardiac resynchronization therapy measurements. EDV, end-diastolic volume; ESV, end-systolic volume; IVCT, isovolumic contract time; IVRT, isovolumic relaxation time; TIVT, total isovolumic time. b Figure 2 Patient with no septal flash. (A) Fused activation and echo bull’s eye plots. There is uniform activation both anterior and inferiorly with no block. (B) Unipolar isochronal map. Top row anterior: Bottom row posterior. Uniform activation with no block. (C) Left ventricle non-contact mapping unipolar activation map. The activation breaks out in the ventricular septum, and spreads uniformly with no areas of block. Ant, anterior; Sep, septum; Inf, inferior, Lat, lateral. activation pattern was seen with an initial activation of a small septal region followed by a delay of further activation during 2–3 frames on the activation map corresponding to 20 – 40 ms delay. Subsequent activation continued either anteriorly or inferiorly and the opposite area remained blocked until it was activated retrogradely. This resulted in a U-shaped activation pattern with a line of conduction block in either the anterior or inferior region. In patients with a small or no SF there was no conduction block except in one ICM patient with a small SF who had an area of block associated with an anterior-lateral scar. In patients with a large SF the conduction block was present with RV pacing but was seen to disappear with LV and BIV pacing suggesting the lines of block were functional in nature.2 Discussion Our results show that patients with LBBB and a large SF have areas of conduction block with a U-shaped activation pattern on NCM 104 and this is associated with favourable acute and chronic response to CRT. With LV or BIV pacing there was disappearance of the SF which was associated with a more homogenous pattern of electrical activation and improved haemodynamic response. The disappearance of the lines of conduction block during LV and BIV pacing would suggest that the areas of block were functional. Patients without a prominent SF did not exhibit such an abnormal electrical activation pattern and their response to CRT was less marked. Although these results suggest an electro-mechanical interaction during the activation period of the LV we are unable to establish a causal relationship between the presence of a large SF and the presence of conduction block. Our study design does not permit us to ascertain whether the conduction block was produced by the presence of a large SF. In fact the opposite could equally be the case and the presence of conduction block may produce a SF. A likely explanation of the observed activation patterns is the different level of conduction block that may exist within the left bundle conduction system. The surface ECG is inexact in characterizing the location and extent of specific ventricular delays.2 In patients with a large SF there may be block in the proximal left bundle (Figure 1) accordingly the endocardium of the LV would be expected to be activated from the RV with a delay of 40 –50 ms caused by slow muscle-to-muscle trans-septal conduction. Once the impulse reaches the LV endocardium, it enters the subendocardial conduction system and may propagate relatively rapidly within the LV. This has been demonstrated in previous mapping studies2 and would explain the greater degree of echocardiographic inter-ventricular mechanical delay in the large SF patients. In a patient with no SF (Figure 2) the activation pattern in the LV could be explained by preserved activation within the proximal left bundle that causes early activation of the LV endocardium of the septum from where it propagates slowly through the LV myocardium which would correlate more with intra-ventricular delay. The explanation that the difference between activation patterns in patients with and without SF is caused by the type of conduction defect and presence/absence of early LV endocardial activation is supported by the fact that the patients with SF had a significantly wider QRS duration at baseline. This may also explains the better acute and chronic response to CRT as the large SF group has primarily a conduction defect that can be rectified by CRT. The placement of the LV lead in the lateral wall opposite to the origin of septal contraction by the activating wavefront compensated for the delay introduced by the U-shaped activation sequence hence creating optimal segmental recruitment of viable myocardium to maximize effective cardiac work. Indeed this activation pattern may demarcate a group of patients most likely to respond to optimally synchronized segmental recruitment. Left bundle branch block: measures of dyssynchrony and the septal flash All patients had LBBB, however, a large SF was only seen in five. Left bundle branch block is a complex electrical disease resulting from conduction delay located at several anatomical levels of the activation sequence2 which may not be apparent from the surface ECG.4 The group with a large SF had a longer QRS S.G. Duckett et al. duration (large SF, 172.4 + 25.0 ms, small SF, 155.5 + 18.0 ms, and no SF, 142.8 + 21.0 ms) (P , 0.05). Looking at interventricular dyssynchrony, patients with a large SF had a larger delay (large SF, 69 + 13.9 ms, small SF, 40.5 + 17.2 ms, and no SF, 21.8 + 29.1 ms). This fits the hypothesis that in the presence of the SF complete LBBB is present. Measuring intra-ventricular dyssynchrony using the septal/lateral delay show the opposite. Patients with a large SF appear to have less intra-ventricular dyssynnchrony. This may be due to patients without SF having less transeptal conduction delay but more delay within the LV. Alternatively, it may be due to the measurement method. First, the peak velocity in patients with an SF is often outside the ejection period (AVO/AVC) and therefore excluded from the measurements. Secondly, since the SF induces stretching/unstretching of the different segments of the LV, this is not necessarily reflected in the velocity of the basal segments. When a 12-segment standard deviation is used there is no difference between the groups, emphasizing that measurements based on velocities are not appropriate ways to assess the intra-ventricular dyssynchrony.25 Comparison with previous studies Auricchio previously demonstrated a heterogeneity of ventricular activation in patients with LBBB.2 Some patients had a specific ‘U-shaped’ activation sequence with a line of block the location and length of which was highly variable and was related to the site and time of LV breakthrough. Prolongation of transseptal time in patients with LBBB would be expected. However, Auricchio found that approximately one-third of patients with LBBB had a normal transseptal time and slightly prolonged or nearnormal LV endocardial activation times. The abrupt change in the transseptal time correlated to a change in the LV breakthrough site suggesting that LV breakthrough at anterior or septobasal was via one or more septal branches of the His–Purkinje system, whereas patients with a significantly prolonged transseptal time had a mid-septal or septoapical breakthrough site likely to indicate a cell-to-cell activation sequence from RV to LV. This is analogous to our findings in patients with and without a large SF. In this study the ability to change the location and length of the line of block with pacing supports a functional basis for the lines of block. The majority of patients with a large SF (80%) had idiopathic cardiomyopathy, thus lacking the presence of ischaemic myocardial scar associated with morphologically based conduction delay and block. Previous haemodynamic data showed that patients with QRS duration ,150 ms have less acute benefit with CRT than patients with a QRS duration .150 ms. Our data support this and that of Auricchio showing evidence of a more homogeneous electrical activation process is less likely to respond to CRT in patients with QRS complex ,150 ms. Our findings build on those of Auricchio with the addition of acute and chronic response to CRT being dependent on the activation pattern which in turn can be recognized from a relatively simple non-invasive demonstration of the SF. Our findings also give insight into the underlying pattern of the LV activation in patients with LBBB. Septal flash and myocardial stretch One speculative hypothesis for the conduction abnormality seen with a large SF is shown in Figure 3. Although this is a potential 105 Electromechanical interaction in LBBB Figure 3 Summary of potential hypothesis with regard to the electrical activation, mechanical events, and their interaction, in patients with left bundle branch block and a septal flash. Shortly, after the onset of the activation (breaking trough at the mid/basal-septum, coming from the right side) (A), the fast and large contraction of the septum during the initial phase of the septal flash (B) leads to mechanical stretching of the surrounding tissues, thus changing its conductivity and slowing down or halting further activation. When activation slowly surpasses the stretched region (around half of the total activation time, while only a limited area of the left ventricle is activated at this point), either anterior or inferior of the septal flash region (C/D), it rapidly conducts further over the left ventricle endocardium, activating the rest of the ventricle, and initiating mechanical activity in the free walls, which start to contract and exhibit force on the contracted septum, which in its turn is stretched, resulting in the outward/ lengthening portion of the septal flash. (E/F). A, anterior wall; AVO, aortic valve opening; I, inferior wall; L, lateral wall; MVC, mitral valve closure; RV, right ventricle; S, septum. explanation for the finding of conduction block in SF patients we cannot substantiate this hypothesis as we can only show an association rather than causation. Study limitations Non-contact mapping relies on unipolar signal detection and may not reliably distinguish between signals from the opposite site of the septum since they are very sensitive and reflect electrograms from the entire wall. Non-contact mapping may also be less accurate in enlarged LVs. We studied a small number of patients with only five having a large SF. There are definite trends that patients with a large SF have a greater acute response to LV and BIV pacing and greater remodelling at 6 months. However, due to the small numbers it is not possible to determine whether these differences are clinically significant. The design of the bull’s eye plots was crude. A better method of quantifying the SF is required, including a quantitative analysis of the extent and location of the deformation. We included both ICM and DCM patients. There is evidence that patients with ICM compose a spectrum of different conduction abnormities due to variable locations and extent of scar; however, 80% of our patients with a large SF were nonischaemic. A further factor that is very difficult to control for in such a small mechanistic study is the volume of viable myocardium available for recruitment during pacing. To fully investigate many of these limitations would require a large population and normalization of the haemodynamic/echocardiographic remodelling data; however, given the invasive and complex nature of these clinical measurements this would not be feasible. Clinical implications for cardiac resynchronization therapy This work concurs with previous studies that show correction of the SF by CRT to be associated with significant remodelling.8 The identification that a large SF correlates with a LV activation pattern that is associated with a favourable response to CRT may have important clinical implications. Non-contact mapping has been advocated as a way to determine responders to CRT; however, this is a highly invasive and not practical. If the SF is able to act as a surrogate for a favourable activation pattern this may represents a simple, reproducible, and non-invasive tool to 106 predict CRT response and aid patient selection. If the SF is proven to be indicative of U-shaped activation it may allow better selection of optimal lateral wall LV lead placement in CRT patients. Conclusion In LBBB with a SF there is a strong association between electrical activation and mechanical deformation. This information may be valuable in understanding and predicting response to CRT. Acknowledgements The author would like to thank Dr Tarik Hussain. Conflict of interest: M.G. receives research funding from St. Jude Medical. R.R. receives research funding from Philips Healthcare. G.C.-W. receives support from Medtronic and St. Jude Medical. C.A.R is a consultant to St. Jude Medical. Funding This work was supported by European Community’s Seventh Framework Programme (FP7/2007-2013) under grant agreement n. 224495 (euHeart project) and CENIT Program from Spanish MICINN-CDTI under grant CEN20091044 (cvREMOD project). References 1. Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L et al. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med 2005;352:1539 –49. 2. Auricchio A, Fantoni C, Regoli F, Carbucicchio C, Goette A, Geller C et al. Characterization of left ventricular activation in patients with heart failure and left bundle-branch block. Circulation 2004;109:1133 – 9. 3. Fung JW, Chan JY, Yip GW, Chan HC, Chan WW, Zhang Q et al. Effect of left ventricular endocardial activation pattern on echocardiographic and clinical response to cardiac resynchronization therapy. Heart 2007;93:432 – 7. 4. Rodriguez LM, Timmermans C, Nabar A, Beatty G, Wellens HJ. Variable patterns of septal activation in patients with left bundle branch block and heart failure. J Cardiovasc Electrophysiol 2003;14:135 –41. 5. Gornick CC, Adler SW, Pederson B, Hauck J, Budd J, Schweitzer J. Validation of a new noncontact catheter system for electroanatomic mapping of left ventricular endocardium. Circulation 1999;99:829 –35. 6. Lambiase PD, Rinaldi A, Hauck J, Mobb M, Elliott D, Mohammad S et al. Noncontact left ventricular endocardial mapping in cardiac resynchronisation therapy. Heart 2004;90:44–51. 7. Ginks MR, Lambiase PD, Duckett SG, Bostock J, Chinchapatnam P, Rhode KS et al. Simultaneous X-MRI and Non Contact Mapping Study of the Acute Hemodynamic Effect of Left Ventricular Endocardial and Epicardial Cardiac Resynchronization Therapy in Humans. Circ Heart Fail 2011 1;4:170 –9. 8. Cikes M, Bijnens B, Durić Z, Bencic ML, Gosev I, Velagić V et al. Detecting volume responders prior to implantation of a cardiac resynchronization therapy device via minithoracotomy: the septal flash as a predictor of immediate left ventricular reverse remodeling. Heart Surg Forum 2009;12:E362 – 7. S.G. Duckett et al. 9. Parsai C, Bijnens B, Sutherland GR, Baltabaeva A, Claus P, Marciniak M et al. Toward understanding response to cardiac resynchronization therapy: left ventricular dyssynchrony is only one of multiple mechanisms. Eur Heart J 2009;30: 940 –9. 10. De Boeck BW, Teske AJ, Meine M, Leenders GE, Cramer MJ, Prinzen FW et al. Septal rebound stretch reflects the functional substrate to cardiac resynchronization therapy and predicts volumetric and neurohormonal response. Eur J Heart Fail 2009;11:863 – 71. 11. Kirn B, Jansen A, Bracke F, van Gelder B, Arts T, Prinzen FW. Mechanical discoordination rather than dyssynchrony predicts reverse remodeling upon cardiac resynchronization. Am J Physiol Heart Circ Physiol 2008;295:H640 –6. 12. Voigt JU, Schneider TM, Korder S, Szulik M, Gürel E, Daniel WG et al. Apical transverse motion as surrogate parameter to determine regional left ventricular function inhomogeneities: a new, integrative approach to left ventricular asynchrony assessment. Eur Heart J 2009;30:959 –68. 13. Kerckhoffs RC, Faris OP, Bovendeerd PH, Prinzen FW, Smits K, McVeigh ER et al. Electromechanics of paced left ventricle simulated by straightforward mathematical model: comparison with experiments. Am J Physiol Heart Circ Physiol 2005;289: H1889 –97. 14. Lab MJ. Mechanosensitive-mediated interaction, integration, and cardiac control. Ann NY Acad Sci 2006;1080:282 – 300. 15. Kuijpers NH, ten Eikelder HM, Bovendeerd PH, Verheule S, Arts T, Hilbers PA. Mechanoelectric feedback leads to conduction slowing and block in acutely dilated atria: a modeling study of cardiac electromechanics. Am J Physiol Heart Circ Physiol 2007;292:H2832 –53. 16. Kerckhoffs RC, Lumens J, Vernooy K, Omens JH, Mulligan LJ, Delhaas T et al. Cardiac resynchronization: insight from experimental and computational models. Prog Biophys Mol Biol 2008;97:543 –61. 17. Ghio S, Constantin C, Klersy C, Serio A, Fontana A, Campana C et al. Interventricular and intraventricular dyssynchrony are common in heart failure patients, regardless of QRS duration. Eur Heart J 2004;25:571 – 8. 18. Bax JJ, Bleeker GB, Marwick TH, Molhoek SG, Boersma E, Steendijk P et al. Left ventricular dyssynchrony predicts response and prognosis after cardiac resynchronization therapy. J Am Coll Cardiol 2004;44:1834 –40. 19. Yu C-M, Fung W-H, Lin H, Zhang Q, Sanderson JE, Lau C-P. Predictors of left ventricular reverse remodeling after cardiac resynchronization therapy for heart failure secondary to idiopathic dilated or ischemic cardiomyopathy. Am J Cardiol 2003;91:684 –8. 20. Lima JAC, Judd RM, Bazille A, Schulman SP, Atalar E, Zerhouni EA. Regional heterogeneity of human myocardial infarcts demonstrated by contrast-enhanced MRI: potential mechanisms. Circulation 1995;92:1117 –25. 21. Schilling RJ, Peters NS, Davies DW. Simultaneous endocardial mapping in the human left ventricle using a noncontact catheter : comparison of contact and reconstructed electrograms during sinus rhythm. Circulation 1998; 98:887 – 98. 22. Derval N, Steendijk P, Gula LJ, Deplagne A, Laborderie J, Sacher F et al. Optimizing hemodynamics in heart failure patients by systematic screening of left ventricular pacing sites: the lateral left ventricular wall and the coronary sinus are rarely the best sites. J Am Coll Cardiol 2010;55:566 – 75. 23. Bleeker GB, Kaandorp TA, Lamb HJ, Boersma E, Steendijk P, de Roos A et al. Effect of posterolateral scar tissue on clinical and echocardiographic improvement after cardiac resynchronization therapy. Circulation 2006;113:969 –76. 24. van Gelder BM, Bracke FA, Meijer A, Pijls NHJ. The hemodynamic effect of intrinsic conduction during left ventricular pacing as compared to biventricular pacing. J Am Coll Cardiol 2005;46:2305 –10. 25. Chung ES, Leon AR, Tavazzi L, Sun J-P, Nihoyannopoulos P, Merlino J et al. Results of the Predictors of Response to CRT (PROSPECT) Trial. Circulation 2008;117: 2608 –16.