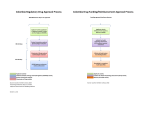
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
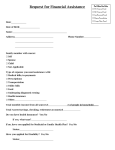
PEMEGANG AMANAH YAYASAN KEBAJIKAN SSL HAEMODIALYSIS 修成林洗肾福利基金 No.9, Jalan 1/5, 46000 Petaling Jaya, Selangor. Tel : 03-7782 2293 / 7782 4092 Fax : 03-7783 5092 APPLICATION FOR HAEMODIALYSIS PROGRAMME (PERMOHONAN MENYERTAI PROGRAM HEMODIALISIS) 1. PERSONAL PARTICULARS Full Name: NRIC No: Address: Tel No. : D.O.B : Marital Status : Age : Sex: Nationality : Race : M / F Type of Accommodation: OWN [ Fully Paid / On Installment : RM __________/month ] Loan payment from _________ until ________ (attach loan agreement) RENT [RM ____________/ month] Low Cost Flat Single Storey Apartment Double Storey Condominium Other __________ 2. EDUCATION BACKGROUND Level / Course Primary Secondary STPM University/College Others Year Name of School 3. DETAILS OF EMPLOYMENT Present Occupation Employer Name : : Income : Address : Tel If unemployed, please state: Since (date): Reason: Name of supporter: [1] : Result PEMEGANG AMANAH YAYASAN KEBAJIKAN SSL HAEMODIALYSIS 修成林洗肾福利基金 No.9, Jalan 1/5, 46000 Petaling Jaya, Selangor. Tel : 03-7782 2293 / 7782 4092 Fax : 03-7783 5092 4. FAMILY INFORMATION List of siblings staying together No. Name Relationship Age Occupation Marital Status No. of Children Monthly Income TOTAL : List of siblings NOT staying together No. Name Relationship Age Occupation Marital Status No. Of Children Monthly Income TOTAL : [2] Contribution To Applicant PEMEGANG AMANAH YAYASAN KEBAJIKAN SSL HAEMODIALYSIS 修成林洗肾福利基金 No.9, Jalan 1/5, 46000 Petaling Jaya, Selangor. Tel : 03-7782 2293 / 7782 4092 Fax : 03-7783 5092 5. TOTAL MONTHLY HOUSEHOLD INCOME AND EXPENDITURE Income RM 1. Personal Income 2. Household Family Income 3. Contributions From Other Children 4. Other Income (Pls specify) TOTAL INCOME Expenditure RM 1. EPF & SOCSO Contribution 2. Food 3. House Rental / Installment 4. Vehicle Installment 5. Utilities (water / electricity / telephone) 6. Schooling Expenses 7. Working Members’ Expenses (petrol / food) 8. Dialysis payment (Dialysis RM_______/month , EPO injection RM_____) 9. Others, pls specify, TOTAL EXPENDITURE BALANCE INCOME (Total Income – Total Expenditure) Description RM Total Income Total Expenditure BALANCE [3] PEMEGANG AMANAH YAYASAN KEBAJIKAN SSL HAEMODIALYSIS 修成林洗肾福利基金 No.9, Jalan 1/5, 46000 Petaling Jaya, Selangor. Tel : 03-7782 2293 / 7782 4092 Fax : 03-7783 5092 6. Every applicant is REQUIRED to attach below listed supporting documents. The admission process will be delayed if the patient fails to submit the complete required documents. a. b. c. d. e. Photocopy of I/C & 2pcs Latest Passport Size Photo (Applicant only) Latest Salary Slip or Certify letter from Employer (Applicant, spouse & children) Income Tax Returns (Form J / EA) (Applicant, spouse & children) Latest EPF Statement, or Proof of EPF withdrawal statement (if any) (Applicant, spouse & children) Photocopy of saving account passbook, current account bank statements or FD slip (Applicant, spouse & children) f. House rental receipt or house installment statement (Applicant, spouse & children) g. Vehicle installment statement, Insurance statement and Credit Card statement(Applicant, spouse & children) h. Photocopy of electricity, water, telephone or hand phone bill (Applicant, spouse & children) i. Medical Report from Nephrologist & ECG Report (if any) j. Blood test report with VDRL (RPR), HIV I & II, Hepatitis A, B, C,Antigen and Antibody (must be within 6 months) ================>>>>>>>>>>>>>>>>>================<<<<<<<<<<<<<<<<<<<============= Checklist (For Office Use Only) Form Date Received Applicant Application Form Medical Report Latest Blood Test Report (HHH, HIV & VDRL) Latest 2 pcs Passport Size Photo & photocopy of I/C Latest Salary slip Latest Income Tax Return Latest EPF statement Saving/current account statement House Rental / Installment slip Vehicle Installment slip Utilities bill Others (pls specify), [4] Spouse Parent Children Sibling Others PEMEGANG AMANAH YAYASAN KEBAJIKAN SSL HAEMODIALYSIS 修成林洗肾福利基金 No.9, Jalan 1/5, 46000 Petaling Jaya, Selangor. Tel : 03-7782 2293 / 7782 4092 Fax : 03-7783 5092 7. CONDITIONS FOR SELECTION INTO STAFF NURSE ASSISTANCE HAEMODIALYSIS PROGRAMME a. Applicant is a Malaysian Citizen. b. Applicant is aged 16 years and above. c. Applicant is ambulant (able to move independently). d. Applicant has a suitable functional vascular access. e. Applicant is prepared to have regular blood test to assess the medical condition and quality condition. f. Applicant must be certified medically fit by SSL's appointed Nephrologist. g. Applicant has no other recourse to regular Haemodialysis from charitable organisation. h. Applicant is prepared to meet the SSL Committee Member before being considered for the programme. i. Applicant must agree to a Committee and Social Worker's visit to his/her home with a view to verify all information given. j. Applicant is prepared to pay treatment fee of RM110.00 per dialysis session on admission until the approval of government subsidy of RM50.00 is granted by the Ministry of Health (MOH). SSL will henceforth charge RM60.00 per dialysis session. SSL will apply to MOH for approval of government subsidy on behalf of the patient. k. Applicant is prepared to pay a dialysis deposit of RM300.00 before starting the dialysis with SSL. It will be forfeited if the patient fails to turn up for dialysis during that week. l. Applicant is prepared to pay treatment fee as stated above. This fee is subject to change by the SSL as and when it deems necessary. This amount is payable prior to treatment. m. Applicant who fails to obtain the government subsidy approval from MOH will have to pay RM110.00 or fee set by SSL per dialysis while his appeal is referred to MOH for reconsideration. If the appeal to MOH is rejected, the case will be referred to SSL Committee Member for its final decision to allow the patient to continue dialysis or terminate his dialysis treatment in SSL. n. The selected patient must be willing to undergo dialysis at the Centre at the dates and times fixed by the Centre, three times per week, 4 hours per session. o. Reselection-The patient is reviewed every 6 months with regards to his suitability to continue on the dialysis programme. p. The patient's programme can be terminated if : He/She fails to turn up for more than 3 successive dialysis. He/She is no longer ambulant. [5] PEMEGANG AMANAH YAYASAN KEBAJIKAN SSL HAEMODIALYSIS 修成林洗肾福利基金 No.9, Jalan 1/5, 46000 Petaling Jaya, Selangor. Tel : 03-7782 2293 / 7782 4092 Fax : 03-7783 5092 His/Her condition has deteriorated with complications such as heart disease, infection, stroke etc or need to be transferred to CAPD. He/She is uncooperative and fails to keep within the terms of the contract drawn up. o. The patient must be willing to sign a contract with SSL before commencing the dialysis programme. p. Applicant with HIV positive and Hepatitis B+C positive will not be accepted by SSL. 8. DECLARATION I declare that : a. I have read,understood and agreed to comply with the terms and conditions. b. All the particulars given in this form are true & I have not suppressed any information required. c. I am aware that if my application is successful, I will be accepted for dialysis for only 6 months. Thereafter my application will be reconsidered. d. Upon acceptance, I agree to obey all the rules & regulations set by Pemegang Amanah Yayasan Kebajikan SSL Haemodialysis Berdaftar. e. If I have suppressed or given any incorrect information, Pemegang Amanah Yayasan Kebajikan SSL Haemodialysis Berdaftar reserves the right to discontinue providing treatment to me and I will not take any legal action against the centre. ___________________________ ________________ Applicant's Signature / Right Thumb Print Date WITNESSED BY, Name : I/C No. : Relationship : Tel No. : Address: [6] PEMEGANG AMANAH YAYASAN KEBAJIKAN SSL HAEMODIALYSIS 修成林洗肾福利基金 No.9, Jalan 1/5, 46000 Petaling Jaya, Selangor. Tel : 03-7782 2293 / 7782 4092 Fax : 03-7783 5092 To the Doctor incharge, Kindly complete the questionnaire in full. The report should indicate the period for which the patient was put under care of the referring physician and provide an adequate resume of the patient’s clinical history. If the referring physician has specific reservations about the medical suitability of the patient for the treatment applied for, these should be clearly declared. The referring Nephrologist should undertake to continue to treat the patient jointly with Pemegang Amanah Yayasan Kebajikan SSL Haemodialysis Berdaftar after the patient is accepted for dialysis. Patient’s Name : Physician’s Name : Patient I/C No. : Physician’s Clinic/Hospital : Diagnosis Primary Secondary 1. SUMMARY OF MEDICAL REPORT : 2. SPECIFIC QUESTIONS (SPECIFY) a) Is the patient mentally or educationally normal ? Yes No b) Is the patient ambulant ? Yes No c) Does the patient suffer any vision,hearing or physical disability? Yes No d) Has the patient had any previous surgery (including transplantation) ? Yes No [7] PEMEGANG AMANAH YAYASAN KEBAJIKAN SSL HAEMODIALYSIS 修成林洗肾福利基金 No.9, Jalan 1/5, 46000 Petaling Jaya, Selangor. Tel : 03-7782 2293 / 7782 4092 Fax : 03-7783 5092 e) Does the patient have other significant disease(s) that would Yes No Yes No Yes No h) Is the patient likely to be medically fit to work ? Yes No i) Allergy : Yes No mitigate against response to treatment ? If so, please specify : Coronary artery disease Yes No Cerebrovascular disease Yes No Peripheral vascular disease Yes No Chronic pulmonary disease Yes No Diabetes mellitus Yes No Malignancy Yes No Other systemic disease Yes No f) Has the patient undergone peritoneal dialysis? If yes, please specify : Acute Long Term g) Has the patient been considered for transplantation ? If yes, please specify : Living related Cadaveric j) Other medical illness : 3. VASCULAR ACCESS AV Fistula AV Graft Others,_________________ Date Created : __________________Location : _____________ In Use : Yes 4. CURRENT TREATMENT : Conservative IPD CAPD Haemodialysis Date of first dialysis : __________________________ Place of dialysis : __________________________ [8] No PEMEGANG AMANAH YAYASAN KEBAJIKAN SSL HAEMODIALYSIS 修成林洗肾福利基金 No.9, Jalan 1/5, 46000 Petaling Jaya, Selangor. Tel : 03-7782 2293 / 7782 4092 Fax : 03-7783 5092 5. INVESTIGATIONS (Please attach a copy of latest blood test result) HbsAg : positive negative not done Anti HBS : positive negative not done Anti HCV : positive negative not done HIV : positive negative not done VDRL : positive negative not done MRSA Screen : positive negative not done Creatinine (umol/l) : Urea (mmol/l) : Potassium (mmol/l) : HCO3 (mmol/l) : Calcium (mmol/l) : Phosphate (mmol/l) : ALT (iu/l) : AST (iu/l) : Albumin (g/l) : HB (g/dl) : 6. CURRENT MEDICATIONS : 7. OTHER COMMENTS : _______________________________ Signature of Nephrologist / Physician Date Chop : [9]