Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
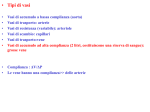
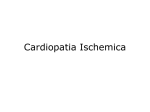
Sezioni UNIVERSITA' DEGLI STUDI - BARI DIPARTIMENTO DELL'EMERGENZA E DEI TRAPIANTI DI ORGANI (D.E.T.O.) DIRETTORE: Prof.Michele Battaglia Segretario Amministrativo: Rag.Vito De Mola Tel+Fax 080 5478627 e-mail: [email protected] Prof Marco Matteo Ciccone Responsabili Anestesia e Rianimazione Cardiochirurgia Chirurgia d’urgenza Chirurgia Generale e Trapianti di Fegato Chirurgia Veterinaria Gastroenterologia Malattie dell’Apparato Cardiovascolare Medicina Interna,Endocrinologia, Andrologia e Malattie Metaboliche Nefrologia, Dialisi e Trapianti Patologia Chirurgica Urologia e Andrologia Urologia, Andrologia e Trapianti di Rene F.Bruno L.De Luca Tupputi N.Palasciano V.Memeo A.Crovace A.Francavilla S.Favale F.Giorgino F.P.Schena F.Prete A.Pagliarulo F.P.Selvaggi Bari, October, 27th 2015 To: Professor Michael Henein Editor-in-chief International Cardiovascular Forum Journal Dear Editor, Please find enclosed an original paper entitled “An unusual case of ST elevation myocardial infarction in a teenager with a coronary artery fistula.””, which we would like to submit for publication in International Cardiovascular Forum Journal. This paper reports a rare case of coronary artery fistula determining ST-elevation myocardial infarction in a young boy. All of the authors declare that this manuscript has not been published previously, it is not under consideration for publication elsewhere, its publication is approved by all authors, and, if accepted, that it will not be published elsewhere. We benefit of the offer to publish for free (code 9-201601). Dr. Francesca Cortese critically reviewed the intellectual content of the manuscript, and finally approved the version to be submitted for publication. Dr. Michele Gesualdo analysed coronary computer tomography angiography images and finally approved the version to be submitted for publication. Dr. Tommaso Acquaviva reviewed the manuscript’s intellectual content, and finally approved the version to be submitted for publication. Dr. Domenico Zanna reviewed the manuscript’s intellectual content, and finally approved the version to be submitted for publication. Dr Emanuela De Cillis performed the angiographic assessment, and finally approved the version to be submitted for publication. Prof. Alessandro Bortone performed the angiographic assessmen, and finally approved the version to be submitted for publication. Prof Marco Matteo Ciccone critically reviewed the intellectual content of the manuscript, and finally approved the version to be submitted for publication. Dr. Francesca Cortese will deal with all pre-publication correspondence. None of the authors have any financial or other relations that could lead to a conflict of interest. We look forward to hearing from you in due course. Yours sincerely, Francesca Cortese Michele Gesualdo Tommaso Acquaviva Domenico Zanna Emanuela De Cillis Alessandro Bortone Marco Matteo Ciccone Address for correspondence: Dr. Francesca Cortese Piazza G. Cesare 11 - 70124 Bari Italy; Tel +39-080-5478791, Fax +39-080-5478796 e-mail: [email protected] An unusual case of ST elevation myocardial infarction in a teenager with a coronary artery fistula. Francesca Cortese1*, Michele Gesualdo1, Tommaso Acquaviva2, Domenico Zanna1, Emanuela De Cillis2, Alessandro Bortone2, Marco Matteo Ciccone1. 1.Department of Cardiology, University of Bari, Italy; 2.Department of Cardiac Surgery, University of Bari, Italy. Corresponding author: Dr. Francesca Cortese Piazza G. Cesare 11 - 70124 Bari Italy; Tel +39-080-5478791, Fax +39-080-5478796 e-mail: [email protected] Conflicts of interest: none. Key words: coronary artery fistula; ST-elevation myocardial infarction; percutaneous closure. Coronary artery fistula (CAF) is an abnormal connection between a coronary artery and any of the 4 chambers of the heart or any of the great vessels (superior vena cava, pulmonary artery, pulmonary veins, or coronary sinus). This abnormality is most often congenital [1] and, although representing the most common coronary arterial malformation, is a rare cardiac anomaly. The incidence is of 0.002% of the general population and of 0.4% of all cardiac malformations [2]. Fistulas originating from the right coronary artery account for 50% to 60% of cases, while those from the left anterior descending artery for 25% to 42% of cases, 18.3% from the circumflex artery, 1.9% from the diagonal branch, and 0.7% from the left main coronary artery or circumflex-marginal branch [3, 4]. The most common are single fistulas, with a prevalence ranging from 74% to 90%, multiple fistulas occur in 10.7% to 16%, while both coronary arteries are involved in only 5% [2]. The right heart is the most frequent site of drainage of fistulas [5]; in particular, the pulmonary artery is the drainage site in 15% to 43% of cases, followed by the right ventricle in 14% to 40%, the right atrium in 19% to 26%, the left ventricle in 2% to 19%, the coronary sinus in 7%, the superior vena cava in 1% and finally the left atrium in 5% to 6% [3, 4]. Moreover literature data show that bilateral fistulas, accounting for 5% of the total, terminate more often into the pulmonary artery (56%) than unilateral fistulas (17%) [2]. Pathological manifestations depend on the resistance of the connection and the fistula drainage site. The resistance is determined by the characteristics (size, tortuosity, and length) of the fistula. Flow through fistulas that drain in the right chambers occurs during the whole cardiac cycle loading both ventricles, while when the drain is in the left atrium and pulmonary vein, volume overload affects only the left heart. CAFs are usually asymptomatic at a young age, unless they are of large dimensions. Symptoms can occur with the increase of age: fatigue, dyspnea, palpitations and ischemic chest pain are the most frequent clinical manifestations whereas heart failure, pulmonary hypertension, subacute bacterial endocarditis, rupture or thrombosis the extreme complications [6]. We report a rare case of bilateral CAF draining into the left atrium determining myocardial infarction in a 18 year old boy. A young man of 18 years, with no cardiovascular risk factors and without family history of juvenile sudden death and ischemic heart disease was hospitalized for chest pain radiating to the left arm. Medical history showed right lobar pneumonia at the age of 3 years, and a diagnosis of myopericarditis at 14 years. The patient is not taking medication. At the first medical contact blood pressure was 130/80 mmHg, the general, cardiac and pulmonary examinations where in the normal range. The ECG showed sinus rhythm at the frequency of 68 bpm with ST-segment elevation from V3 to V6 and in D1, D2 and aVL, negative T waves in D3 and aVF. Chest X-ray showed enlargement of the cardiac silhouette, while echocardiogram hypokinesis of the apex and of mid anterior segment with moderate impairment of left ventricular ejection function (EF: 45%). Blood tests showed an increase of troponin value (34.73 ng / ml) and no sign of inflammation. Coronary angiography highlighted the presence of a CAF connecting the right coronary artery and the first tract of the anterior descending artery with the left atrium (figure 1). CT angiography confirmed the angiographic findings CAF was percutaneously closed by using the intracoronary injection of Glubran, an adhesive compound [7]. The coronary angiography performed after 48 hours showed the complete obliteration of CAF (figure 2). The postoperative course was not complicated by clinical and instrumental evidence of new myocardial ischemia. The patient was discharged in clinically stable condition on aspirin and beta blocker therapy. After about one month, the patient was completely asymptomatic with normalization of electrocardiographic abnormalities and left ventricular function To the best of our knowledge, this is the first case of CAF which manifested itself at an early age with myocardial infarction. Myocardial infarction is a rare complication of CAF, accounting for about 5% of overall manifestations [8]. The pathological mechanism involved is the coronary steal phenomena, because the fistula, a low resistance system, in appropriate circumstances, can determine shunting of blood from coronary vessel to the left atrium, leading to myocardial ischemia. The closure with percutaneous approach shows to be an effective method, mini-invasive and safe. Acknowledgements: The authors state that they adhere to the statement of ethical publishing of the International Cardiovascular Forum Journal [9]. Figure 1. The arrows show CAF connecting the first tract of the anterior descending artery (right side of the image) and the right coronary artery (left side of image) to the left atrium. Figure 2. Coronary angiography performed after 48 hours from the closure showing the absence of CAF. REFERENCES. [1] Sommer RJ, Hijazi ZM, Rhodes JF. Pathophysiology of congenital heart disease in the adult. Circulation 2008;117: 1090 –9; [2] C.V. Mangukia, Coronary artery fistula, Ann. Thorac. Surg. 93 (2012) 2084–2092; [3] Dodge-Khatami A, Mavroudis C, Backer CL. Congenital heart surgery nomenclature and database project: anomalies of the coronary arteries. Ann Thorac Surg 2000;69(3 Suppl 1):270 –7; [4] Huang YK, Lei MH, Lu MS, Tseng CN, Chang JP, Chu JJ. Bilateral coronary-to-pulmonary artery fistulas. Ann Thorac Surg 2006;82:1886 – 8; [5] Lowe JE, Oldham HN Jr, Sabiston DC Jr. Surgical management of congenital coronary artery fistulas. Ann Surg 1981;194:373– 80; [6] Zamani H, Meragi M, Arabi Moghadam MY, Alizadeh B, Babazadeh K, Mokhtari-Esbuie F4. Clinical presentation of coronary arteriovenous fistula according to age and anatomic orientation. Caspian J Intern Med. 2015 Spring;6(2):108-12. [7] ASGE Technology Committee, Bhat YM, Banerjee S, Barth BA, Chauhan SS, Gottlieb KT, Konda V, Maple JT, Murad FM, Pfau PR, Pleskow DK, Siddiqui UD, Tokar JL, Wang A, Rodriguez SA. Tissue adhesives: cyanoacrylate glue and fibrin sealant. Gastrointest Endosc. 2013 Aug;78(2):209-15. [8] Ibrahim Halil Kurt Myocardial Infarction Caused by a Fistula between the Left Anterior Descending Coronary Artery and the Left Ventricle. Tex Heart Inst J. 2009; 36(2): 177–179. [9] Shewan LG, Coats AJS, Henein M. Requirements for ethical publishing in biomedical journals. International Cardiovascular Forum Journal 2015;2:2 DOI: 10.17987/icfj.v2i1.4