Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Atrial fibrillation wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
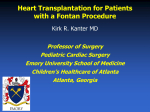
Global Impairment of Cardiac Autonomic Nervous Activity Late After the Fontan Operation Constantinos H. Davos, MD, PhD; Darrel P. Francis, MRCP; Marjolein F.E. Leenarts, MD; Sing-Chien Yap, MD; Wei Li, MD, PhD; Periklis A. Davlouros, MD; Roland Wensel, MD; Andrew J.S. Coats, DM; Massimo Piepoli, MD, PhD; Narayanswami Sreeram, MD; Michael A. Gatzoulis, MD, PhD Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Background—Atrial tachyarrhythmia is a common cause of morbidity and mortality in patients with univentricular physiology undergoing the Fontan operation. We examined cardiac autonomic nervous activity, a predictor of arrhythmia and sudden death in other cardiovascular disease, in patients late after the Fontan operation, employing heart rate variability (HRV) and baroreflex sensitivity. Methods and Results—We measured HRV and baroreflex sensitivity in 22 consecutive patients (8 male, age 26⫾9 years) who had undergone the Fontan operation 13⫾6 years previously, and 22 age- and sex-matched healthy controls. Fontan patients had significantly lower HRV (P⬍0.0001). Baroreflex sensitivity was measured by the ␣-index method (square root of ratio of RR interval spectral power to systolic blood pressure (SBP) spectral power, in the LF and the HF band) and was also significantly depressed in the Fontan group (P⬍0.0001 for both). Both low frequency (LF) and high frequency (HF) components of HRV were reduced in the Fontan patients (P⬍0.0001), but there was interindividual variation so that the LF/(LF⫹HF) ratio may be high, normal, or low, and decreased with increasing right atrial dimensions (r⫽⫺0.62, P⫽0.006). Patients with a history of sustained atrial arrhythmia had a stronger baroreflex than those without (P⫽0.005). Conclusions—Autonomic nervous control of the heart is markedly deranged in patients late after the Fontan operation, with reduced HRV and baroreflex sensitivity. A relative suppression of the sympathetic– compared with the parasympathetic– system was observed in patients with marked right atrial dilation within the Fontan group. Furthermore, stronger baroreflexes were seen in Fontan patients in association with a higher incidence of sustained atrial tachyarrhythmia, implying that sinus node dysfunction is unlikely to be the dominant mechanism. Additional studies are clearly required to examine the prognostic importance of impaired BRS and HRV in these patients. (Circulation. 2003;108[suppl II]:II-180-II-185.) Key Words: fontan procedure 䡲 nervous system autonomic 䡲 baroreceptors 䡲 heart rate/heart rate variability 䡲 arrhythmias P atients with congenital heart disease of univentricular physiology palliated with the Fontan operation frequently suffer late complications, with atrial tachyarrhytmias being prominent among them.1–3 These arrhythmias are difficult to manage, and may significantly compromise cardiac output and lead to increased morbidity and mortality.4 – 8 The pathophysiology of atrial tachyarrhythmia in this setting is not fully understood and may involve the increased right atrial pressure after the Fontan procedure.3,9 –13 Deranged cardiac autonomic nervous activity (CANA) is a well-recognized feature in heart failure patients, without congenital heart disease.14 The degree of derangement is associated with increased burden of cardiovascular morbidity including arrhythmias (and sudden cardiac death) in a variety of clinical settings,15–19 increased mortality, and worse overall prognosis in coronary artery disease and heart failure patients. Limited data exist on CANA in adults with congenital heart disease20,21 after surgical repair of tetralogy of Fallot, and even less in patients with single ventricle physiology after the Fontan operation, mostly in pediatric patients.22 The aim of our prospective study was to assess several aspects of CANA late after the Fontan procedure in older patients (primarily adults) and examine its relationship with cardiac physiology and clinical status. Methods Patients Twenty-two (8 male) patients with previous Fontan operations were recruited from the Adult Congenital Heart Clinic of the Royal Brompton Hospital, London, UK following informed consent. Ex- From the Royal Brompton Adult Congenital Heart Programme, and Department of Clinical Cardiology, Royal Brompton Hospital and National Heart and Lung Institute, Imperial College School of Medicine, London, UK, and Department of Cardiology, Wilhelmina Children’s Hospital, Utrecht, The Netherlands Correspondence to Michael A. Gatzoulis, M.D., Ph.D., Royal Brompton Hospital, Sydney Street, London SW3 6NP, UK. Phone: 44-207-351-8602, Fax 44-207-351-8629, E-mail [email protected] © 2003 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org DOI: 10.1161/01.cir.0000087946.47069.cb II-180 Davos et al. TABLE 1. Cardiac Autonomic Nervous Activity and Fontan Operation Heart Rate Variability Indices Assessed in the Study Time Domain Indices SDNN Standard deviation of all normal-to-normal RR intervals RMSSD Square root of the mean squared differences of successive RR intervals pNN50 Per cent of differences of successive RR intervals ⬎50 ms Triangular index Integral of the density distribution dived by the maximum of the density distribution Frequency Domain Indices II-181 Transthoracic Echocardiography Transthoracic echocardiography was performed using a Philips Sonos 5500 (Andover) echocardiograph with a 2.5-MHz tranducer. Subjects were examined at rest in the semilateral decubitus position. Right and left atrial (RA and LA) sizes were measured off-line in 2 planes, transverse and supero-inferior, by a single investigator (WL) blinded to the other data. For patients with a total cavo-pulmonary connection type of Fontan–all of them intracrdiac–right atrial measurements were made on the actual true, native right atrium and not on the intra-atrial baffle. Because of the heterogeneity of cardiac anatomy, we used a qualitative, subjective assessment of systemic ventricular dysfunction from multiview 2-dimentional echocardiography, graded from I to IV: I (absent), II (mild), III (moderate), and IV (severe) as described previously.25 Atrio-ventricular valve regurgitation was also graded on a scale from I (absent) to IV (severe). Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 VLF Very low frequency (0.0033–0.04 Hz) Statistical Analysis LF Low frequency (0.04–0.15 Hz) HF High frequency (0.15–0.4 Hz) Data were expressed as frequency for the nominal variables and as mean ⫾ SD for continuous variables. HRV and BRS indices with skewed distributions were log transformed. Data were analyzed by using Statview 5.0 (Abacus Concepts, SAS Institute). Differences between the control and the patient subgroups were assessed by an unpaired Student t test or by the Mann-Whitney rank-sum for data that failed tests of normality. Variables that did not follow the normal distribution were logarithmically transformed. Univariate and multivariate linear regression was used for determination of independent predictors of the assessed variables. All of the tests were two-sided. A probability value ⬍0.05 was considered significant. clusion criteria included diabetes mellitus, permanent atrial arrhythmia, or ⬎2 ventricular ectopic beats per min during data acquisition, the presence of a permanent pacemaker and clinical instability within the preceding 3 months. Surgical details were obtained from operative notes. The patient symptomatic status was defined according to the New York Heart Association (NYHA) functional classification. Sustained arrhythmia was defined as arrhythmia that was clinically apparent and was documented by ECG, a Holter recording, or ECG strips before electrical cardioversion. Twenty-two age- and sexmatched normal controls, who had no significant past medical history, no abnormalities on examination, and were not taking regular medication, were also studied. Measurements Patients were studied between 13:00 and 17:00 hour under standardized conditions, in a quiet room at a comfortable temperature. All were fasted for at least 2 hours before testing and were not allowed to smoke or drink alcohol- or caffeine-containing beverages for 24 hours before the study. All of the subjects rested supine for 15 minutes and then underwent 1 successive 20-minute recording at rest.23 During this investigation, RR interval and blood pressure (BP) were recorded. BP was measured by a Finapres device (model 2300; Ohmeda), with the cuffed finger resting comfortably at the level of the heart. The Finapres cuff was wrapped around the index finger of the left hand. The subjects underwent several minutes of accustomisation to the Finapres, and the servo-adjust mechanism was turned off before recording. The ECG was acquired from the limb lead with the largest R wave (typically lead II). All of the data were sampled at 1000 Hz on a computer using an analogue-to-digital converter (National Instruments). The readings were saved into floppy disk and analyzed off-line with custom designed software. The program measured RR intervals and beat-to-beat systolic pressure while ectopic beats were corrected by linear interpolation.23 HRV HRV analysis was made on the 20-minute ECG recordings, and time domain and frequency domain indexes were calculated (Table 1) using our laboratory software.24 Baroreceptor Sensitivity For the BRS assessment, we measured the average amplitude of oscillations in RR interval and the average amplitude of oscillations in SBP. Power spectral analysis was performed on the RR interval and SBP data using an autoregressive algorithm. The ␣-index was calculated as the square root of the ratio between RR and SBP spectral power in the low frequency (0.04 – 0.15 Hz, ␣LF) and the high frequency (0.04 – 0.15 Hz, ␣HF) band in the presence of an adequate coherence (⬎0.5) between the RR interval and SBP as assessed by cross-spectral analysis.24 Results Patient Characteristics Patient clinical and surgical characteristics are shown in Table 2, their current medication in Table 3, and their echocardiographic profile in Table 4. Ninety-one percent of patients were in NYHA class I-II, whereas 14 (64%) patients had a prior history of sustained atrial tachyarrhythmia. HRV All of the HRV indices in Fontan patients were significantly reduced, compared with controls (Table 5 and Figure 1). The time domain indices (SDNN, RMSSD, pNN50, and Triangular Index) were all reduced by at least 50%. Both LF and HF were about three-fold reduced in Fontan patients, compared with healthy controls. However, the mean relative balance of LF and HF [expressed as LF/(LF⫹HF)] was not different between Fontan patients and controls. There was a large inter-individual variation so that the ratio of LF/(LF⫹HF) could be high, normal, or low. Furthermore, there was a negative correlation between the LF/(LF⫹HF) ratio and right atrial transverse dimensions (r⫽⫺0.62, P⫽0.007, Figure 2) and a borderline correlation with right atrial supero-inferior dimensions (r⫽⫺0.46, P⫽0.05). BRS BRS in the Fontan patients was also markedly reduced (Table 5 and Figure 3). Fontan patients with a previous history of sustained atrial tacharrhythmia in particular had a stronger baroreflex (n⫽14, log aLF 0.83, log aHF 0.97) than the remainder of Fontan patients (n⫽8, log aLF 0.36, log aHF 0.54, P⫽0.01 and P⫽0.005, respectively). In contrast to HRV, BRS was not related to any of the echocardiographic measurements. There were no correlations between number of pre-Fontan palliations and their type, years from palliation to Fontan completion, age at Fontan completion, years from Fontan completion II-182 Circulation September 9, 2003 TABLE 2. Clinical and surgical characteristics: Fontan Patients and Healthy Controls Fontan Patients Range n Controls Range n Age, years 26.2⫾9.6 12.0–43.5 22 29.5⫾7.8 18.3–48.1 22 Female 26.3⫾10.6 12.0–43.5 14 30.6⫾8.2 18.3–47.1 14 Male 26.2⫾8.2 17.3–38.9 8 27.6⫾7.2 18.7–39.0 8 Variable Tricuspid atresia 12* (54.5%) Double inlet ventricle 5 (22.7%) Atrial isomerism 2 (9.1%) Pulmonary atresia/Intact septum 1 (4.5%) Other 2 (9.1%) Time after Fontan, years 13.1⫾5.7 4.8–24.1 Age at Fontan, years 13.2⫾8.1 1.8–28.9 Previous Palliations 18 (81.8%) Blalock-Taussing shunt(s) 13** (72%) Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Glenn 2 (11%) PA banding 1 (6%) Other arterio-pulmonary shunt(s) 2 (11%) Days from birth to 1st palliation 823⫾1510 1–6345 Years remained palliated 10.2⫾6.0 1.6–27.8 APC 10 (45.5%) AVA 4 (18.2%) TCPC 8 (36.3%) Fontan revisions 4 (18.2%) NYHA class I 45.5% II 45.5% III 9% %O2 saturation at rest 94.9⫾4.1 History of sustained atrial tachyarrhythmia 14 (64%) 84–100 Mean values or frequency and percentages in (). *Including 2 patients with pulmonary atresia. **Including 1 patient with Both Blalock-Taussing and Waterstone shunts. PA: pulmonary artery, APC: Atrio-pulmonary connection, AVA: Atrio-ventricular anastomosis, TCPC: Total cavo-pulmonary connection. to the time of the study, type of Fontan completion and NYHA class, and measured HRV or BRS indices. Discussion This study shows that CANA as measured by HRV and BRS is markedly deranged in patients late after the Fontan operation. Secondly, although LF and HF are overall severely suppressed, there is differential suppression so that patients with the greater degree of right atrial dilation have the most severe suppression of LF (potentially sympathetic modulation), whereas those with lesser degree of right atrial dilation have the most severe suppression of HF (potentially parasympathetic modulation). Thirdly, baroreflexes were significantly more active in Fontan patients with previous history of sustained atrial tachyarrhythmia. Global Suppression of CANA HRV is an index of multiple cyclical components swaying the heart rate around its mean value. Nonspectral or time domain parameters involve computing indices that are not directly related to specific cycle lengths. This method offers a simple means of defining patients with decreased variability in the mean and SDs of R-R intervals. Spectral analysis can provide a more detailed assessment of the modulation of the R-R interval. The HF component of spectral analysis occurs at such a rapid cycle time that only the parasympathetic arm of the autonomic nervous system has sufficiently rapid modulatory capacity to be imputed as the mediating control system. The LF component occurs at a frequency at which the powerful sympathetic nervous system influences are able to contribute importantly. Thus, the LF pattern gives additional information about sympathetic modulation, although of course parasympathetic influences are involved.24 The suppression of HRV was not limited to the HF and LF bands. There also appeared to be diminution of the VLF band, of which the origin is currently incompletely elucidated. This is evidence of global disruption of autonomic regulation. BRS is a more specific measure of the ability of changes in BP Davos et al. TABLE 3. Cardiac Autonomic Nervous Activity and Fontan Operation II-183 Current Medication: Fontan Patients Overall Group (n⫽22) With History of Atrial Arrhythmia (n⫽14) 11 (50.0%) 11 (100%) 0 (0%) Beta blockers 2 (9.1%) 2 (100%) 0 (0%) ACE inhibitors 6 (27.3%) 4 (66.7%) 2 (33.3%) Digoxin 1 (4.5%) 0 (0%) 1 (100%) Calcium channel-blockers 1 (4.5%) 1 (100%) 0 (0%) Drug Amiodarone Without History of Atrial Arrhythmia (n⫽8) Diuretics 6 (27.3%) 5 (83.3%) 1 (16.7) Aspirin 3 (13.6%) 2 (66.7%) 1 (33.3%) Warfarin 18 (81.8%) 12 (66.7%) 6 (33.3%) Nitrates 1 (4.5%) 1 (100%) 0 (0%) Thyroxine 2 (9.1%) 2 (14.3%) 0 (0%) Carbimazole 3 (13.6%) 3 (21.5%) Number of patients and percentages in (). Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 to produce changes in heart rate (which occurs through modulation of cardiac autonomic nervous outflow). We used a well-validated noninvasive method, avoiding possible adverse effects on patients and controls.23 There was markedly suppressed HRV (⬎50% reduction in every measured variable) and BRS (⬇50% reduction) suggesting global disruption of cardiac autonomic nervous control. This was despite many patients being asymptomatic. The disruption of HRV and BRS was unrelated to the age at (or time since) the Fontan operation or previous palliations. Nor did the type of Fontan surgery or the total number of surgical procedures affect the HRV or BRS. These results are consistent with those of Ohuchi et al, who studied a pediatric population of Fontan patients.22 Differential Effects of Sympathetic and Vagal Modulation TABLE 5. Heart Rate Variability and Baroreflex Sensitivity: Fontan Patients and Healthy Controls Fontan Patients (n⫽22) Controls (n⫽22) SDNN (ms) 35.2⫾21.6‡ 74.1⫾23.6 RMSSD (ms) 31.2⫾29.8† 64.6⫾30.3 pNN50 (%) 13.0⫾22.2† 36.1⫾22.4 123.9⫾74.7‡ 290.0⫾85.6 854.8⫾2055.9 846.8⫾496.6 Time domain indices of HRV Triangular index Because global magnitude of HRV varies widely between subjects, evaluation of the balance between sympathetic and TABLE 4. parasympathetic modulation can be helped by addressing a ratio such as LF/(LF⫹HF). This can have a value between almost 1 (indicating LF power much larger than HF power) and 0 (indicating HF power much larger than LF power), with a value of 0.5 indicating an equal balance. In our study we Echocardiographic Characteristics: Fontan Patients Frequency domain indices of HRV VLF (ms2) log VLF 2.2⫾0.8* 2.8⫾0.3 LF (ms2) 254.3⫾400.7‡ 788.0⫾505.8 Mean Standard Deviation Range n Supero-inferior 5.6 1.7 3.2–8.9 18 Transverse 5.4 1.9 3.0–8.8 18 ␣-LF (ms/mmHg) 7.6⫾10.5‡ Supero-inferior 4.9 1.3 3.3–8.0 16 log ␣-LF 0.7⫾0.4‡ 1.1⫾0.2 Transverse 3.1 0.8 2.3–4.7 16 ␣-HF (ms/mmHg) 9.3⫾8.8‡ 29.6⫾16.1 log ␣-HF 0.8⫾0.4‡ 1.4⫾0.2 Variable log LF RA dimension (cm) log HF LA dimension (cm) AVVR Not present 12 (54.5%) Mild 8 (36.4%) Moderate 2 (9.1%) Systemic ventricular dysfunction Absent HF (ms2) 14 (63.7%) Mild 3 (13.6%) Moderate 3 (13.6%) Severe 2 (9.1%) RA: Right atrium, LA: Left atrium, AVVR: Atrio-ventricular valve regurgitation. LF/(LF⫹HF) 1.8⫾0.8‡ 2.8⫾0.4 263.0⫾668.2‡ 852.9⫾682.3 1.9⫾0.7‡ 2.8⫾0.4 0.50⫾0.16 0.50⫾0.21 Baroreflex Sensitivity 14.3⫾5.4 HRV: heart rate variability; RR: mean duration of RR interval; SDNN: standard deviation of all RR intervals; RMSSD: square root of the mean squared differences of successive RR intervals; pNN50: percent of differences of successive RR intervals ⬎50 ms; Triangular index: integral of the density distribution divided by the maximum of the density distribution; VLF: very low frequency; LF: low frequency; HF: high frequency; ␣: alpha index, square root of the ratio between RR and SBP spectral powers in the VLF (␣-VLF), LF (␣-LF) and HF (␣-HF) band in spectral analysis. Values are mean⫾SD. *P⬍0.01. †P⬍0.001. ‡P⬍0.0001 vs controls. II-184 Circulation September 9, 2003 Figure 3. Baroreflex sensitivity: Fontan patients versus healthy controls. P⬍0.001 for all measures. Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 there is a process common to both right atrial dilation and depression of sympathetic modulation. Indeed, the former may cause the latter, although the current observational study would not be able to confirm causality. Clearly, however, there must be other processes depressing CANA, because at least one alternative mechanism must be invoked to explain suppression of HF. Overt or occult damage occurring at or around the time of surgery is a plausible candidate.22 BRS and Atrial Arrhythmia Figure 1. Heart rate variability: Fontan patients versus healthy controls. Upper panel: time domain indices. Lower panel: frequency domain indices. *P⬍0.01, †P⬍0.001, ‡P⬍0.0001. found that the mean value of LF/(LF⫹HF) was not significantly different between the Fontan patients and the controls, although the Fontan patients had a slightly wider dispersion of values (95% CI: 0.08 – 0.93 versus 0.19 – 0.82). This dispersion arose from differential suppression of LF and HF in different individual patients. The individual values of LF/(LF⫹HF) were inversely correlated with right atrial dimensions. This is in contrast to the study by Ohuchi et al, who failed to show any relationship between autonomic nervous dysfunction and underlying heamodynamics in their study of pediatric patients. Longer length of follow-up from the Fontan completion between the 2 studies is almost certainly responsible. We interpret our data as evidence that Figure 2. Correlation between the LF/(LF⫹HF) ratio and right atrial dimension: Fontan patients. Patients from our study with a history of sustained artrial tachyarrhythmia had significantly more sensitive baroreflexes, indicating a greater propensity for modulation of the sinus node rate in response to changes in arterial BP. This is inconsistent with the hypothesis that sinus node damage is a dominant mechanism predisposing to atrial tachyarrhythmia in this population, because any such damage would be expected to reduce (rather than increase) the ability of the node to respond to autonomic modulation.11 Why this relationship exists between prior atrial tachyarrhythmia and higher baroreflex gain remains unclear and it would seem counterintuitive, especially when examined in the context of data from patients with myocardial infarction. It is purely speculative, but when baroreflex gain is stronger, disturbances in BP could more easily engender dramatic changes in heart rate, which act as a precursor to atrial ectopy, which in turn may trigger atrial tachyarrhythmia. However, such an explanation is tenuous and would need additional corroboration. Why Fontan patients might be different from others at risk of atrial arrhythmia is unknown. It is certainly far from proven that relatively preserved BRS actually causes atrial arrhythmia. Causation could be in the opposite direction, or there could be a common cause to both. Data on this question is currently lacking. Both ␣LF and ␣HF were markedly depressed in the Fontan patients. ␣LF is a better gauge of BRS than ␣HF, because the response time of the arterial baroreflex corresponds better to the cyclical pattern of LF than to that of HF. Although both ␣ measures were depressed, there seemed to be a trend to greater depression of ␣HF, suggesting a global autonomic abnormality rather than a very specific baroreflex defect Davos et al. Cardiac Autonomic Nervous Activity and Fontan Operation Study Limitations Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 We could not examine direct influence of surgical procedures on CANA, because preoperative and immediate postoperative HRV and BRS data were not available. Trying to keep the study noninvasive and needle-free, we did not assess catecholamine levels or muscle sympathetic nerve activity. Many of our patients were on amiodarone or other anti-arrhythmic medication, which would have been unethical to discontinue in preparation for assessing the CANA. Furthermore, exclusion of patients with previous arrhythmia from the study would have given us a biased population, not representative of the true clinical spectrum of patients late after the Fontan operation. Therefore, we cannot be certain that medication did not contribute to the effects seen and reported here. Additional predictors of CANA dysfunction after the Fontan procedure may exist, and be identified with a larger patient sample and longer period of observation in future studies. Furthermore, the potential effects of atrio-pulmonary to total cavo-pulmonary Fontan conversion and heart transplantation on CANA in patients with univentricular physiology need prospective assessment. Conclusions CANA is markedly depressed in patients late after the Fontan operation, with both HRV and BRS reduced by ⬎50%. Patients with marked right atrial dilation had more marked suppression of their sympathetic compared with the parasympathetic system. Furthermore, stronger baroreflexes seem to be associated with a higher (rather than lower) incidence of sustained atrial tachyarrhythmia, implying that sinus node dysfunction may not be the dominant pathogenetic mechanism involved in late arrhythmogenesis in these patients. Additional studies are clearly required to assess the prognostic value of abnormal CANA in patients with univentricular physiology late after the Fontan procedure. Acknowledgments CD and PD received support both from the Hellenic Society of Cardiology, Athens, Greece and the Clinical Research Committee, Royal Brompton Hospital, London, UK. DF received support from the British Heart Foundation, UK. References 1. Driscoll DJ, Offord KP, Feldt RH, et al. Five- to fifteen-year follow-up after Fotan operation. Circulation. 1992;85:469 – 496. 2. Peters NS, Somerville J. Arrhythmias after the Fontan procedure. Br Heart J. 1992;68:199 –204. 3. Cromme-Dijkhuis AH, Hess J, et al. Specific sequelae after Fontan operation at mid- and long-term follow-up. Arrhythmia, liver dysfunction, and coagulation disorders. J Thorac Cardiovasc Sur. 1993;106:1126–1132. 4. Balaji S, Johnson TB, Sade RM, et al. Management of atrial flutter after the Fontan procedure. J Am Coll Cardiol. 1994;23:1209 –1215. 5. Garson Ajr, Bink-Boelken M, Hesslein PS, et al. Atrial flutter in the young: A collaborative study of 380 cases. J Am Coll Cardiol. 1985;6:871–878. II-185 6. Rhodes LA, Walsh EP, Gamble WJ, et al. Benefits and potential risks of atrial antitachycardia pacing after repair of congenital heart disease. Pacing Clin.? Electrophysiol. 1995;18:1005–1016. 7. Triedman JK, Bergau DM, Saul JP, et al. Efficacy of radiofrequency ablation for control of intraatrial reentrant tachycardia inpatients with congenital heart disease. J Am Coll Cardiol. 1997;30:1032–1038. 8. Deal BJ, Mavroudis C, Backer CL, et al. Impact of arrhythmia circuit cryoablation during Fontan conversion for refractory atrial tachycardia. Am J Cardiol. 1999;83:563–568. 9. Weber HS, Hellenbrand WE, Kleinman CS, et al. Predictors of rhythm disturbances and subsequent morbidity after the Fontan operation. Am J Cardiol. 1989;64:762–767. 10. Gelatt M, Hamilton RM, McCrindle BW, et al. Risk factors for atrial tachyarrhythmias after the Fontan operation. J Am Coll Cardiol. 1994; 24:1735–1741. 11. Fishberger SB, Wernovsky G, Gentles TL, et al. Factors that influence the development of atrial flutter after the Fontan operation. J Thorac Cardiovasc Surg. 1997;130:80 – 86. 12. Durongpisitkul K, Poerter CJ, Cetta F, et al. Predicators of early- and late-onset supraventricular tachycardias after Fontan operation. Circulation. 1998;98:1099 –1107. 13. Gatzoulis MA, Munk MD, Williams WG, et al. Definitive palliation with cavopulmonary or aortopulmonary shunts for adults with single ventricle physiology. Heart. 2000;83:51–57. 14. Ponikowski P, Anker SD, Chua TP, et al. Depressed heart rate variability as an independent predictor of death in chronic congestive heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol. 1997;79:1645–1650. 15. Schwartz PJ. The autonomic nervous system and sudden death. Eur Heart J. 1998;19 Suppl F:F72– 80. 16. Kleiger RE, Miller JP, Bigger JT, Jr., et al. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am J Cardiol. 1987;59:256 –262. 17. Bigger JT, Jr., Fleiss JL, Steinman RC, et al. Frequency domain measures of heart period variability and mortality after myocardial infarction. Circulation. 1992;85:164 –171. 18. Farrell TG, Paul V, Cripps TR, et al. Baroreflex sensitivity and electrophysiological correlates in patients after acute myocardial infarction. Circulation. 1991;83:945–952. 19. La Rovere MT, Bigger JT, Jr., Marcus FI, et al. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) Investigators. Lancet. 1998;351:478 – 484. 20. Ohuchi H, Suzuki H, Toyohara K, et al. Abnormal cardiac autonomic nervous activity after right ventricular outflow tract reconstruction. Circulation. 2000;102:2732–2738. 21. Davos CH, Davlouros PA, Wensel R, et al. Global impairement of the cardiac autonomic nervous activity late after repair of tetralogy of Fallot. Circulation. 2002;106:I69 –I75. 22. Ohuchi H, Hasegawa S, Yasuda K, et al. Severely impaired cardiac automonic nervous activity after the Fontan operation. Circulation. 2001; 104:1513–1518. 23. Davies LC, Francis D, Jurak P, et al. Reproducibility of methods for assessing baroreflex sensitivity in normal controls and in patients with chronic heart failure. Clin Sci (Colch). 1999;97:515–522. 24. Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North Am Society of Pacing and Electrophysiology. Circulation. 1996;93:1043–1065. 25. Bolger AP, Sharma R, Li W, et al. Neurohormonal activation and the chronic heart failure syndrome in adults with congenital heart disease. Circulation. 2002;106:92–99. Global Impairment of Cardiac Autonomic Nervous Activity Late After the Fontan Operation Constantinos H. Davos, Darrel P. Francis, Marjolein F.E. Leenarts, Sing-Chien Yap, Wei Li, Periklis A. Davlouros, Roland Wensel, Andrew J.S. Coats, Massimo Piepoli, Narayanswami Sreeram and Michael A. Gatzoulis Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017 Circulation. 2003;108:II-180-II-185 doi: 10.1161/01.cir.0000087946.47069.cb Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2003 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/108/10_suppl_1/II-180 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/