Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
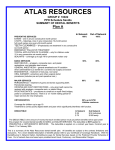
ATLAS RESOURCES GROUP # 10023 PPO Schedule Sandia SUMMARY OF DENTAL BENEFITS Plan B In Network Out of Network PREVENTIVE SERVICES EXAMS – one in any six consecutive month period X-RAYS – bitewings, once in any consecutive 12-month period, full mouth series once every 60-month period TEETH CLEANINGS – (Prophylaxis) one treatment in any consecutive six-month period EMERGENCY PALLIATIVE TREATMENT TOPICAL APPLICATION OF FLUORIDE – only for children under 15 in any consecutive six-month period SEALANTS – coverage up to age 16 for permanent molars only 100% 100% BASIC SERVICES RESTORATIVE – amalgam, composite resin, and plastic restorations, and stainless steel crowns GENERAL ANESTHESIA – general anesthesia and IV sedation when administered by a dentist for a covered oral surgery procedure ENDODONTICS – treatment of root pulp, root canal ORAL SURGERY- extractions and other surgical dental procedures (includes pre and post operative care.) 90% 80% MAJOR SERVICES PERIODONTICS – treatment of gums and bones supporting teeth. Periodontal cleaning. CROWNS AND CAST RESTORATIONS – only when teeth cannot be restored with amalgam, composite resin, or plastic fillings PROSTHODONTICS – procedures to construct or repair fixed bridges, partial or complete dentures. There is a 12- month waiting period for major services for new employees. 60% 50% ORTHODONTICS 50% up to $375 Lifetime maximum Coverage for children up to age 19 Treatment to correct poorly aligned teeth and jaws which significantly interferes with function. DEDUCTIBLE In Network $0 $0 Out Network $ 25 individual $ 75 family The DEDUCTIBLE is the amount of money that each enrolled person must pay before benefits will be paid under this program for covered dental benefits for BASIC and MAJOR SERVICES. The deductible is NOT applied to PREVENTIVE or ORTHODONTIC SERVICES. The deductible is applied on a contract year basis. Contract year is March 1st to February 28th. This is a summary of the Atlas Resources dental benefit plan. All benefits are subject to the contract limitations and exclusions. For a more detailed description of benefits please refer to your Certificate of Coverage Handbook. With the DentalSource In Network Option, DentalSource pays for Dental Services based on the Preferred Provider Schedule of Fees. Out of network fees are based upon predetermined Usual, Customary, and Reasonable Charges. MAXIMUM $ 500.00 PER ENROLLED PERSON – (non-orthodontic) $ 375.00 lifetime for orthodontic services The MAXIMUM is the total dollar amount that will be paid by this program toward covered dental benefits for enrolled persons. The MAXIMUM is applied on a contract year basis. Contract Year is March 1st to February 28th. FREEDOM OF CHOICE You choose the dentist – worldwide. You may visit a specialist without referrals. You may change your dentist without notifying DentalSource Administrators. Participating Dentists: DentalSource contracted dentists will: 1. File claim forms for you. Members are responsible for signing the claim form and verifying accuracy of patient/member information. 2. Accept payment directly from DentalSource. DentalSource will pay the benefit coverage portion directly to the dentist. The non-covered portion is the responsibility of the member. 3. Participating dentists have approved fees that provide maximum dental savings. The dentist will not bill more than the allowable contracted charges. This means the procedures will be paid at the percentage coverage stated on this benefit sheet. Non-Participating Dentists: Non-contracted dentists: 1. Member will receive reimbursement for the allowable amount as determined by DentalSource Inc. 2. Member is responsible for any charge over the allowable amount paid by DentalSource. 3. Member may use any licensed Dentist. PRE-EXISTING CONDITIONS – The plan will not pay for initial prosthetic placement for congenitally missing teeth or for a tooth that has been removed before the patient is covered under the Atlas Resources program. OPTIONAL SERVICES – DentalSource allows the least expensive American Dental Association (ADA) accepted treatment. For example: DentalSource allows and pays for silver (amalgam) fillings on posterior teeth. If you choose a composite resin, you will pay for the difference in price. PRE-TREATMENT ESTIMATE (PRE-DETERMINATION) It is STRONGLY suggested that you get a pre-treatment estimate of benefits for all MAJOR SERVICES or services amounting to $200 or more. A pre-treatment estimate will ensure that you know the procedure you are contemplating having done is covered under this benefit plan as well as what your financial responsibility will be. A pretreatment estimate is not a determination of the need for treatment, only a determination of contracted coverage. ELIGIBILITY – You, your spouse and your unmarried dependent children to age 25 are eligible as defined by your Group Contract. WAITING PERIOD – New employees under the Atlas Resources group dental plan have a 12-month waiting period for major services unless this plan is replacing another dental plan that has been in force for 12 or more months. LIMITATIONS & EXCLUSIONS Prophylaxis limited to one in any six-month period. Fluoride limited to persons under 14 years of age. Sealants limited to the un-restored permanent molars of covered persons under age 16. No coverage for precision attachments, appliance or prosthetic device less than 10 years old or if lost or stolen. TMJ and cosmetic procedures are not covered. MAIL CLAIMS TO: Dental Administrators, PO Box 11569,Albuquerque NM 87192 Albuquerque Number 237-1501 Outside Albuquerque 1-888-862-8659 Web Site: dentalsource.com This summary of the group dental program is subject to the provisions of the group dental contract and cannot modify or affect the group dental contract in any way, nor shall you accrue any rights because of any statement in or omission from this summary.